Scaricare la presentazione
1
“Non servono gli antiaritmici?”
Prof Luigi Padeletti Università di Firenze Heart Failure & Co. Caserta, aprile 2011

2
Sommario degli studi sul trattamento farmacologico
Studio Pazienti Disegno dello studio Risultato CAST-I1 1498 Encainide, flecainide/ placebo Sospeso per numero eccessivo di decessi nel braccio di studio CHF-STAT2 674 Amiodarone/Placebo Nessuna variazione rispetto alla mortalità globale SWORD3 546 d-sotalolo/Placebo Sospeso per numero eccessivo di decessi nel braccio di studio ESVEM4 486 EPS-guidato/Holter-guidato Mortalità elevata in ambedue i bracci EMIAT5 1500 Amiodarone/Placebo Nessuna variazione rispetto alla mortalità globale CAMIAT6 1200 Amiodarone/Placebo Nessuna variazione rispetto alla mortalità globale 4 Mason J.W. N Engl J Med. 1993;329(7):452–8. (Supported by Bristol-Myers Squibb, Knoll Pharmaceutical, Boehringer-Ingelheim, Parke-Davis, and Ciba-Geigy). 5 Julian D.G. The Lancet. 1997;349:667–74.(Supported by Sanofi) 6 Cairns J.A. The Lancet. 1997;349:675–82. 1 Echt, et al. N Engl J Med. 1991;324:781–8. 2 Singh, et al. N Engl J Med. 1995;333:77–82 (supported by Sanofi & Wyeth). 3 Waldo A.L. The Lancet; 1996;348:7–12. (supported by Bristol-Myers Squibb).
:452–8. (Supported by Bristol-Myers Squibb, Knoll Pharmaceutical, Boehringer-Ingelheim, Parke-Davis, and Ciba-Geigy). 5 Julian D.G. The Lancet. 1997;349:667–74.(Supported by Sanofi) 6 Cairns J.A. The Lancet. 1997;349:675–82. 1 Echt, et al. N Engl J Med. 1991;324:781–8. 2 Singh, et al. N Engl J Med. 1995;333:77–82 (supported by Sanofi & Wyeth). 3 Waldo A.L. The Lancet; 1996;348:7–12. (supported by Bristol-Myers Squibb).")
3
Implanted Standby Defibrillators
“ In fact, the implanted defibrillator system represents an imperfect solution in search of a plausible and practical application.” Bernard Lown and Paul Axelrod Circulation, Volume XLVI, October 1972

5
% Mortality Reduction w/ ICD Rx
Secondary Prevention Trials: Reduction in Overall Mortality with ICD Therapy % Mortality Reduction w/ ICD Rx 31% 28% 20% Overall Mortality Reduction results are based on: AVID –was 31% based on survival curve results for ICD and AA drug therapy at three years. CASH – was 28% based survival curve results for ICD and drug therapy at three years. CIDS –was 20% based on the hazard ratio for risk of death results over the time period of the study, with an average follow-up of three years. 1 2 3 3 Years 3 Years 3 Years 1 The AVID Investigators. N Engl J Med. 1997;337: 2 Kuck K. Circ.2000;102: 3 Connolly S. Circ. 2000;101: 5

6
Secondary Prevention Trials: Reduction in Mortality with ICD Therapy
59% 56% % Mortality Reduction w/ ICD Rx 31% 33% 28% 20% Overall Mortality Reduction results are based on: AVID –was 31% based on survival curve results for ICD and AA drug therapy at three years. CASH – was 28% based survival curve results for ICD and drug therapy at three years. CIDS –was 20% based on the hazard ratio for risk of death results over the time period of the study, with an average follow-up of three years. Arrhythmic Death results: AVID: Was calculated to be 56%- based on the difference between the percent of arrhythmia deaths for the conventional therapy (10.8%) and the percent of arrhythmia deaths for ICD therapy (4.7%) over the time period of the study, with an average follow-up of 18 months. CASH: Was 59% at three years - based on the year 3 comparisons of cardiac arrest percentage rates between the ICD and AA drug arm. CIDS:Was calculated to be 33% based on the relative risk reduction results, over the time period of the study, with an average follow-up of 3 years. 1 2 3 3 Years 3 Years 3 Years 1 The AVID Investigators. N Engl J Med. 1997;337: 2 Kuck K. Circ.2000;102: 3 Connolly S. Circ. 2000;101: 6
 and the percent of arrhythmia deaths for ICD therapy (4.7%) over the time period of the study, with an average follow-up of 18 months. CASH: Was 59% at three years - based on the year 3 comparisons of cardiac arrest percentage rates between the ICD and AA drug arm. CIDS:Was calculated to be 33% based on the relative risk reduction results, over the time period of the study, with an average follow-up of 3 years Years. 3 Years. 3 Years. 1 The AVID Investigators. N Engl J Med. 1997;337: Kuck K. Circ.2000;102: Connolly S. Circ. 2000;101:")
7
% Mortality Reduction w/ ICD Rx
Primary Prevention Post-MI Trials: Reduction in Overall Mortality with ICD Therapy 55% 54% % Mortality Reduction w/ ICD Rx 31% Overall mortality reductions for the three studies were based on the hazard ratio for risk of death results for the time period of the study, with the average follow-up time of the patients enrolled in the study noted on the graph. 1 2 3 27 Months 39 Months 20 Months 1 Moss AJ. N Engl J Med. 1996;335: 2 Buxton AE. N Engl J Med. 1999;341: 3 Moss AF. N Engl J Med. 2002;346: 7

8
% Mortality Reduction w/ ICD Rx
Primary Prevention Post-MI Trials: Reduction in Mortality with ICD Therapy 75% 73% 61% 55% 54% % Mortality Reduction w/ ICD Rx 31% Overall mortality reductions for the three studies were based on the hazard ratio for risk of death results for the time period of the study with the average follow-up time of the patients noted on the graph. Arrhythmic Death results: MADIT: Was calculated to be 75% based on the difference between the percent of arrhythmia deaths for the conventional therapy (12.9%) and the percent of arrhythmia deaths for ICD therapy (3.15%) over the time period of the study, with an average follow-up of 27 months. MUSTT: Was 73% - based on the relative risk of event of defibrillator therapy as compared with no arrhythmic therapy for the time period of the study with the average follow-up of 39 months. MADIT-II:Was calculated to be 62% based on the difference between the percent of arrhythmia deaths for the conventional therapy (9.39%) and the percent of arrhythmia deaths for ICD therapy (3.63%) over the time period of the study, with an average follow-up of 20 months. These arrhythmic death numbers were presented at by Dr. Moss before the ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19, 2002, but have not been published. 1 2 3, 4 27 Months 39 Months 20 Months 1 Moss AJ. N Engl J Med. 1996;335: 2 Buxton AE. N Engl J Med. 1999;341: 3 Moss AF. N Engl J Med. 2002;346: 4 Moss AJ. Presented before ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19, 2002. 8
 and the percent of arrhythmia deaths for ICD therapy (3.15%) over the time period of the study, with an average follow-up of 27 months. MUSTT: Was 73% - based on the relative risk of event of defibrillator therapy as compared with no arrhythmic therapy for the time period of the study with the average follow-up of 39 months. MADIT-II:Was calculated to be 62% based on the difference between the percent of arrhythmia deaths for the conventional therapy (9.39%) and the percent of arrhythmia deaths for ICD therapy (3.63%) over the time period of the study, with an average follow-up of 20 months. These arrhythmic death numbers were presented at by Dr. Moss before the ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19, 2002, but have not been published , Months. 39 Months. 20 Months. 1 Moss AJ. N Engl J Med. 1996;335: Buxton AE. N Engl J Med. 1999;341: Moss AF. N Engl J Med. 2002;346: Moss AJ. Presented before ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19,")
9
Reductions in Overall Mortality with ICD Therapy
54% 55% % Mortality Reduction w/ ICD Rx 31% ICD mortality reductions in primary prevention trials are equal to or greater than those in secondary prevention trials. 1 2 3 27 months 39 months 20 months % Mortality Reduction w/ ICD Rx 31% 28% 20% 1 Moss AJ. N Engl J Med. 1996;335: 2 Buxton AE. N Engl J Med. 1999;341: 3 Moss AJ. N Engl J Med. 2002;346:877-83 4 The AVID Investigators. N Engl J Med. 1997;337: 5 Kuck K. Circ. 2000;102: 6 Connolly S. Circ. 2000:101: 4 5 6 3 Years 3 Years 3 Years 9

10
Reductions in Mortality with ICD Therapy
75% 76% 55% 61% 54% % Mortality Reduction w/ ICD Rx 31% ICD mortality reductions in primary prevention trials are equal to or greater than those in secondary prevention trials. 1 2 3, 4 27 months 39 months 20 months 59% 56% % Mortality Reduction w/ ICD Rx 31% 33% 28% 20% 1 Moss AJ. N Engl J Med. 1996;335: 2 Buxton AE. N Engl J Med. 1999;341: 3 Moss AJ. N Engl J Med. 2002;346:877-83 4 Moss AJ. Presented before ACC 51st Annual Scientific Sessions, Late Breaking Clinical Trials, March 19, 2002. 5 The AVID Investigators. N Engl J Med. 1997;337: 6 Kuck K. Circ. 2000;102: 7 Connolly S. Circ. 2000:101: 5 6 7 3 Years 3 Years 3 Years 10

11
MADIT II

15
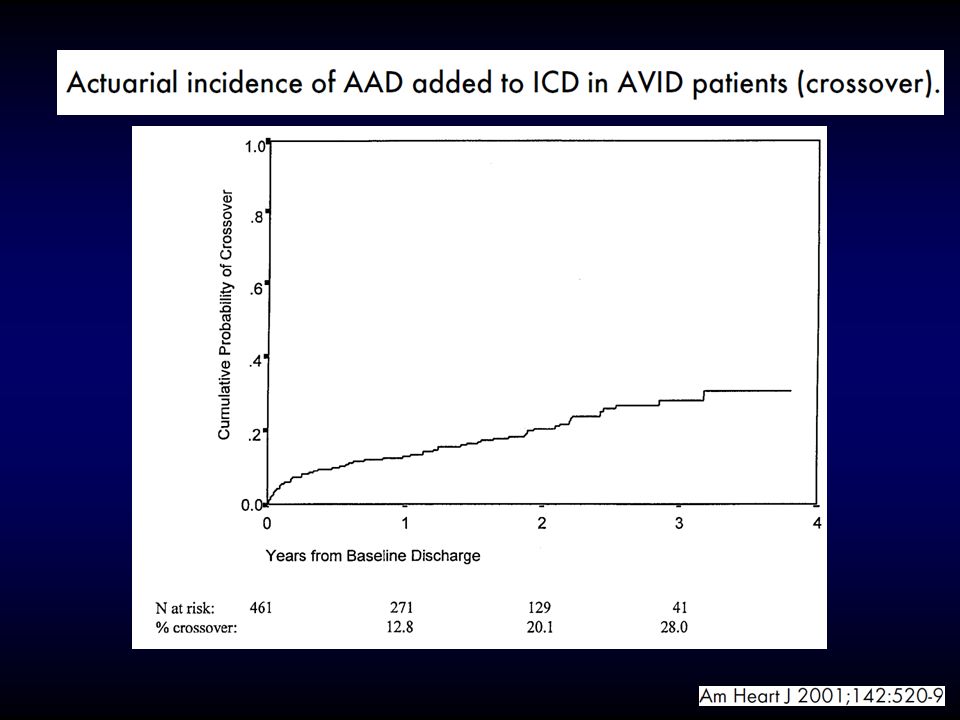
Reason for treatment with AADs in ICD recipients

16
Prognostic importance of defibrillator shocks in patients with heart failure

17
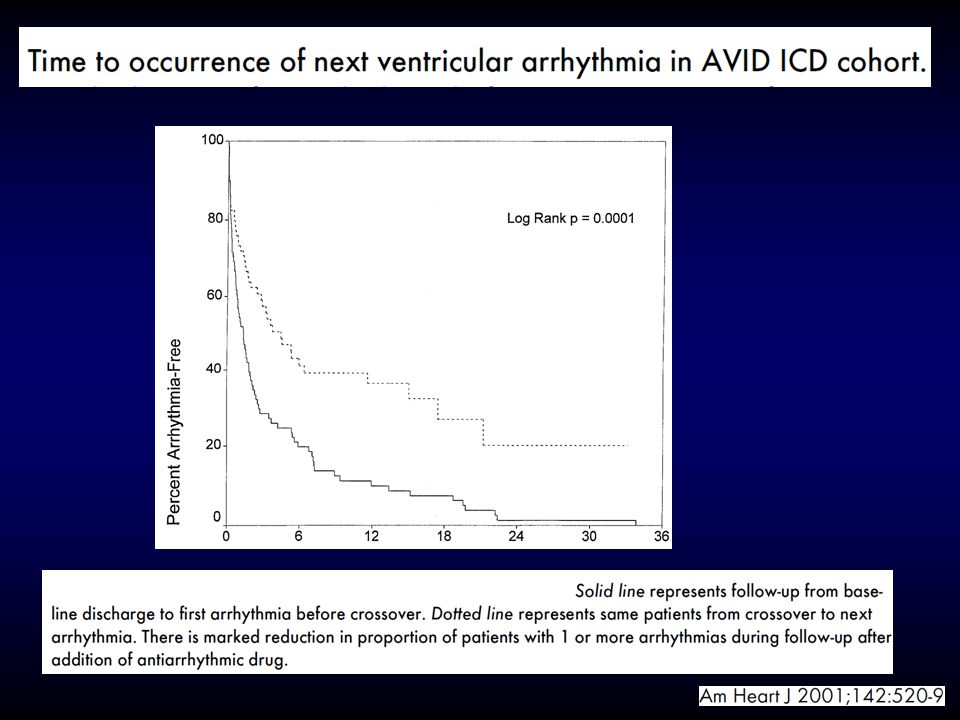
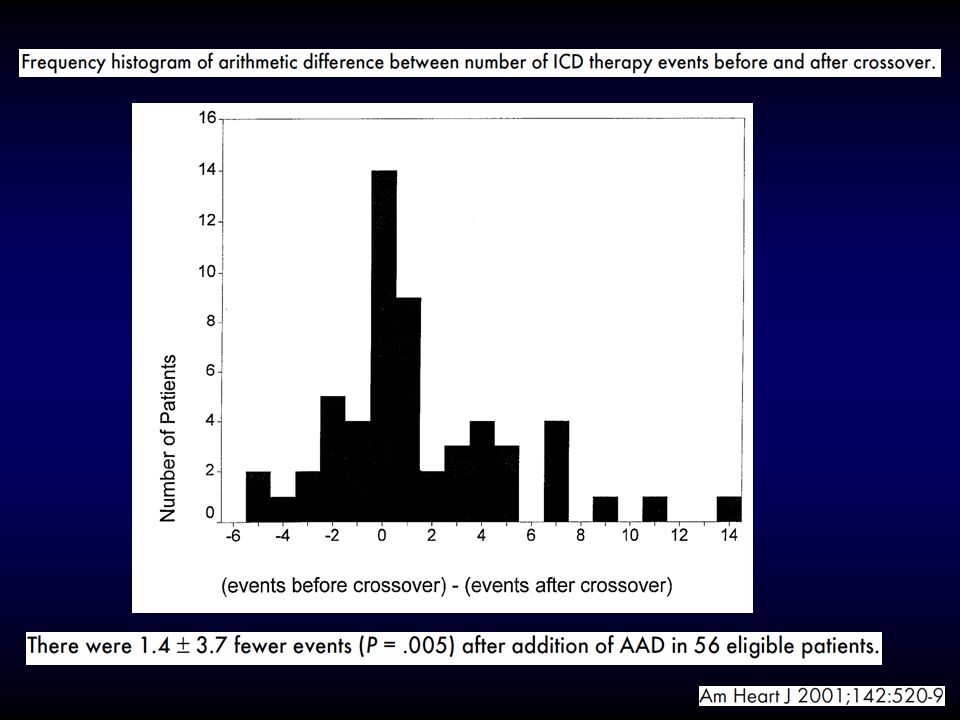
Benefits of adjuvant AADs in ICD patients

18
Betabloccanti: Effetti sulla mortalità
26 trials > pts Post-infarto BETABLOCCANTI PLACEBO RIDUZIONE 934/12438 (7.5%) 288/8115 (3.5%) 1124/11860 (9.5%) 401/7706 (5.2%) - 21% - 33% Mortalità Totale Morte Improvvisa As classicaly showed by Yusuf in this metanalysis regarding twenty-six trials for more than twenty-four thousands people, they are able to reduce both sudden death and total mortality by 33% and 21%, respectively, in postinfarction period. YUSUF S. et al. Prog Cardiovas Dis, 1985; 17:
 288/8115. (3.5%) 1124/ (9.5%) 401/7706. (5.2%) - 21% - 33% Mortalità Totale. Morte Improvvisa. As classicaly showed by Yusuf in this metanalysis regarding twenty-six trials for more than twenty-four thousands people, they are able to reduce both sudden death and total mortality by 33% and 21%, respectively, in postinfarction period. YUSUF S. et al. Prog Cardiovas Dis, 1985; 17:")
20
Clinical Trial summarizing Benefits of AADs

21
Clinical Trial summarizing Benefits of AADs

22
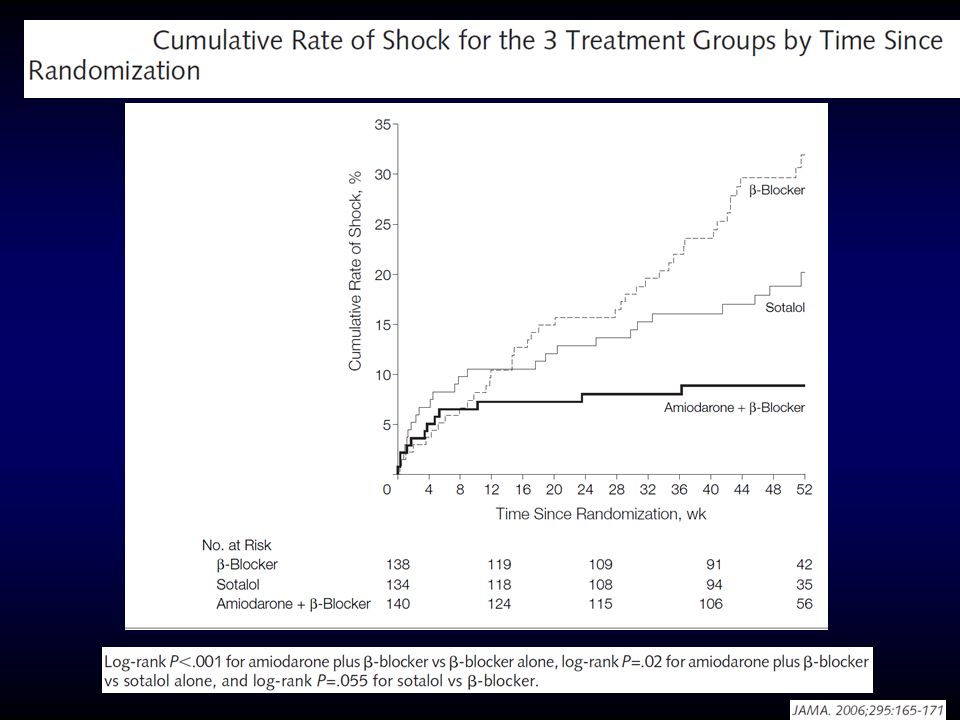
OPTIC Trial

27
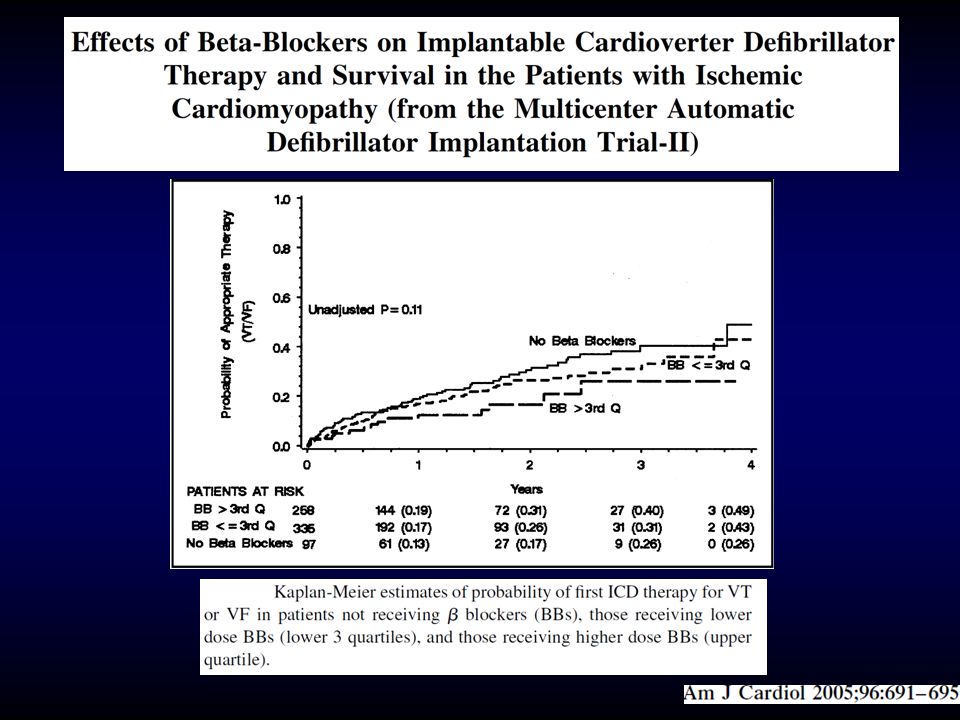
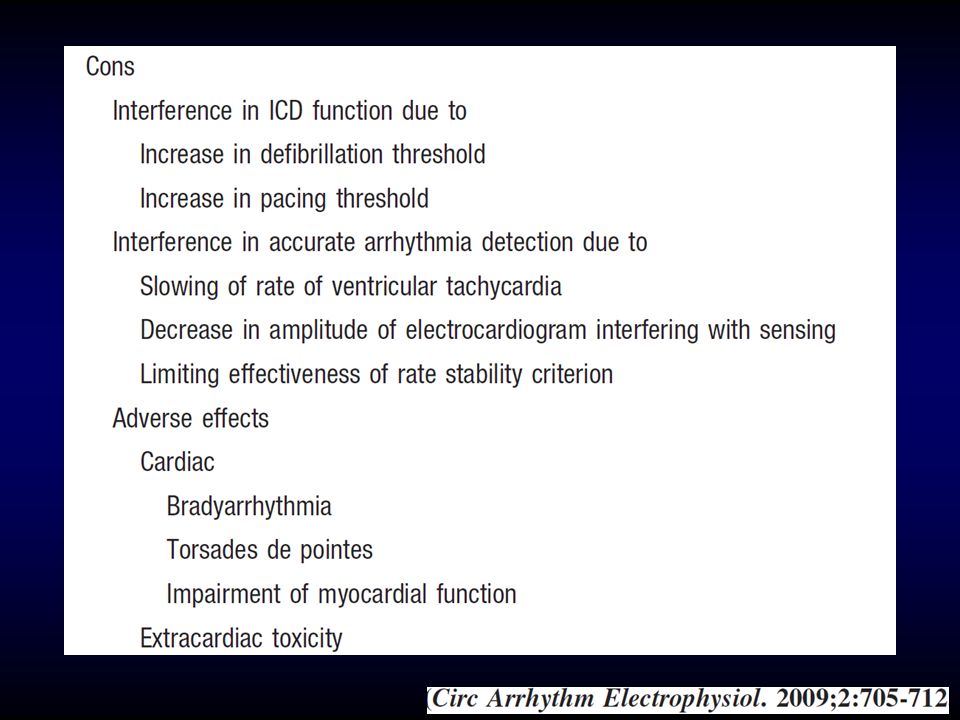
Side Effects of Beta-Blockers could be Beneficial

28
Conclusions Adjunctive AAD therapy often is necessary in many patients with ICDs for control of recurrent ventricular tachyarrhythmias and prevention of ICD shocks.

29
Conclusions Given the scarsity of safe and effective AADs for this indication, the decision of when to start an AAD in the patient with an ICD must be individualized.

30
Conclusions If AAD therapy is initiated, the potential for drug-related toxicities and device interactions must be recognized and anticipated.


















>")





