Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
LA DIETA NEI PAZIENTI AFFETTI DA CALCOLOSI OGGI
Milano, 9 maggio 2015 LA VALUTAZIONE METABOLICA Prof. Pasquale Strazzullo – Dr. Domenico Rendina Dipartimento di Medicina Clinica e Chirurgia Centro per le Malattie del Metabolismo Minerale Università di Napoli Federico II

2
PREVALENCE OF KIDNEY STONE DISEASE IN DIFFERENT COUNTRIES IN THE THIRD MILLENIUM (first decade)
Romero V et al, Reviews in Urology 2010

3
TIME TREND IN THE PREVALENCE OF KIDNEY STONE DISEASE
Scales CD Jr. et al, European Urology 2012

4
RECURRENCE OF NEPHROLITHIASIS IN UNTREATED PATIENTS
Bushinsky DA, JASN 1998

7
PRIMARY PREVENTION SECONDARY PREVENTION
…. means to prevent a first episode ever of kidney stones; ….should be based on the knowledge of the most frequent causal factors of KSD; …should be implemented at the population level by supporting life styles and dietary habits known to be effective on most KSD risk factors. SECONDARY PREVENTION ….targets those who have suffered at least one KS event; …. takes advantage of the assessment of the risk factors operating in the individual patient; …. tries to overcome the problem in a case-specific fashion.

8
Rendina D et al, NDT 2012

9
CHANGING PROFILE OF PATIENTS WITH KIDNEY STONE DISEASE:
a comparison of two patient series observed 25 years apart Ca-nephrolithiasis 50 70 90 60 80 (n=180) (n=226) 6 12 3 9 Urate stones * Rendina D et al, Nephrol Dial Transplant 2013
 (n=226) Urate stones. * Rendina D et al, Nephrol Dial Transplant")
10
Dammi il tuo calcolo: ti dirò chi sei!
L’ANALISI DEL CALCOLO Dammi il tuo calcolo: ti dirò chi sei! Cloutier J et al, World J Urol 2015

11
Dammi il tuo calcolo: ti dirò chi sei!
L’ANALISI DEL CALCOLO Dammi il tuo calcolo: ti dirò chi sei! METODI CHIMICI meno costosi ma più spesso inadeguati METODI FISICI (Infrared spectroscopy) più costosi ma più efficaci: - identificazione di componenti meno comuni - rilevamento accurato di componenti multipli - possibilità di ricostruire il processo patogenetico - matching tra l’analisi del calcolo e la biochimica urinaria Cloutier J et al, World J Urol 2015
 più costosi ma più efficaci: - identificazione di componenti meno comuni. - rilevamento accurato di componenti multipli. - possibilità di ricostruire il processo patogenetico. - matching tra l’analisi del calcolo e la biochimica urinaria. Cloutier J et al, World J Urol")
14
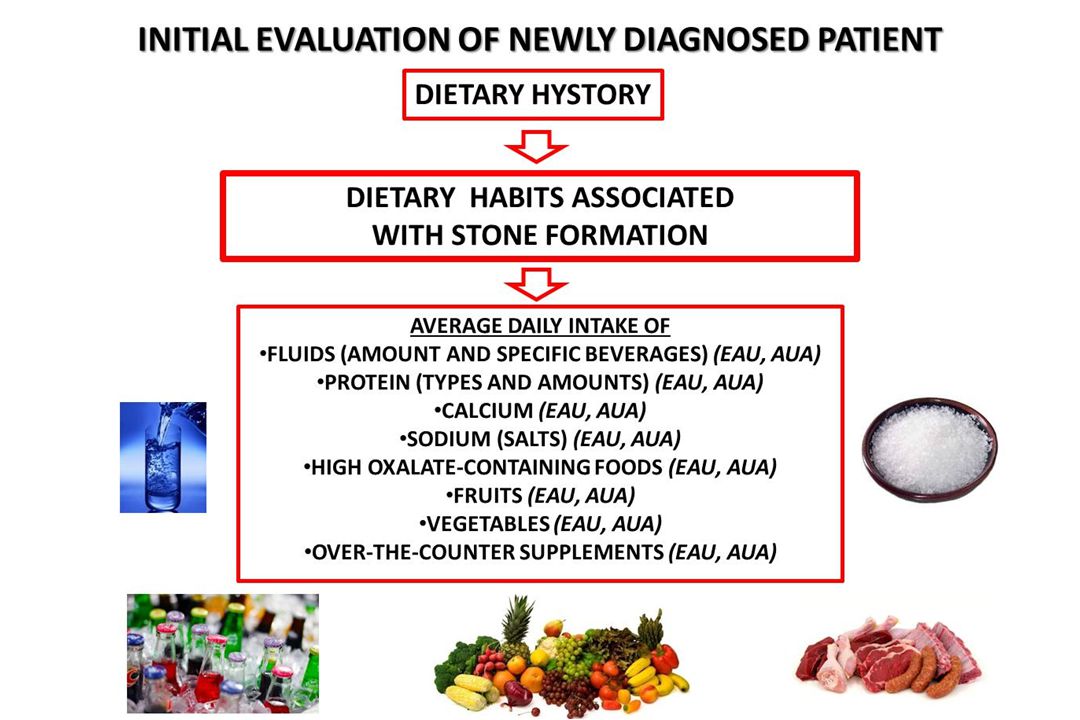
Initial evaluation of newly diagnosed patient
EAU Guideline & AUA Guidelines 2014 Medical hystory Dietary hystory Serum chemistry Urine chemistry

15
Initial evaluation of newly diagnosed patient
Serum and urine chemistry Blood - Serum blood sample Sodium (EAU, auA) Potassium (EAU, auA) Chloride (EAU, auA) bicarbonate (Eau, auA) Calcium (if ↑: PTH, 25OHd3) (EAU, auA) creatinine (EAU, auA) uric acid (EAU, auA) Urine - Dipstick test red cells (EAU, auA) white cells (EAU, auA) nitrite (EAU, auA) urine pH (EAU, auA) Urine - microscopy (EAU, auA) Urine - culture (EAU, auA)
 Potassium (EAU, auA) Chloride (EAU, auA) bicarbonate (Eau, auA) Calcium (if ↑: PTH, 25OHd3) (EAU, auA) creatinine (EAU, auA) uric acid (EAU, auA) Urine - Dipstick test. red cells (EAU, auA) white cells (EAU, auA) nitrite (EAU, auA) urine pH (EAU, auA) Urine - microscopy (EAU, auA) Urine - culture (EAU, auA)")
17
identification of high-risk patient
Recurrent stone formers Multiple stones at initial presentation Family history of stone disease medical conditions predispoSing to stone disease Patients with a solitary kidney additional evaluation One (AUA) or two (eau, Aua) consecutive 24-h urine samples Total volume pH Calcium Oxalate Uric acid Citrate Sodium Potassium Creatinine Cystine Sulphate
 or two (eau, Aua) consecutive 24-h urine samples. Total volume pH. Calcium Oxalate. Uric acid Citrate. Sodium Potassium. Creatinine Cystine. Sulphate.")
18
ESTIMATE OF THE URINE SUPERSATURATION FOR Ca-OXALATE AND Ca-PHOSPHATE
A x calcium0.84 x oxalate Citrate0.22 x magnesium0.12 x volume1.03 CaP B x calcium1.07 x phosphate0.70 x (pH-4.5)6.8 Citrate0.20 x volume1.31
6.8. Citrate0.20 x volume1.31.")
19
Initial evaluation of newly diagnosed patient
medical conditions PREDISPOSING TO stone formation (EAU,AUA) Obesity Metabolic syndrome diabetes mellitus type 2 Gout hyperthyroidism bone disease primary hyperparathyroidism malabsorptive gastrointestinal states Sarcoidosis renal tubular acidosis type 1 Genetically determined stone formation Drugs associated with stone formation Anatomical abnormalities associated with stone formation
 Obesity. Metabolic syndrome. diabetes mellitus type 2. Gout. hyperthyroidism. bone disease. primary hyperparathyroidism. malabsorptive gastrointestinal states. Sarcoidosis. renal tubular acidosis type 1. Genetically determined stone formation. Drugs associated with stone formation. Anatomical abnormalities associated with stone formation.")
20
Rendina D et al, NDT 2012

21
MEDICAL MANAGEMENT OF KIDNEY STONES:
AUA GUIDELINE Guideline Statement 8. All stone formers: fluid intake to achieve a urine volume of ≥ 2.5 liters daily (Standard; Evidence Strength: Grade B) Guideline Statement 9. Patients with calcium stones and ↑ urinary calcium: limit sodium intake and consume 1,000-1,200 mg per day of dietary calcium (Standard; Evidence Strength Grade: B) Guideline Statement 10. Patients with calcium oxalate stones and ↑ urinary oxalate: limit intake of oxalate-rich foods and maintain normal calcium consumption (Expert Opinion)
 Guideline Statement 9. Patients with calcium stones and ↑ urinary calcium: limit sodium intake. and consume 1,000-1,200 mg per day of dietary calcium. (Standard; Evidence Strength Grade: B) Guideline Statement 10. Patients with calcium oxalate stones and ↑ urinary oxalate: limit intake of. oxalate-rich foods and maintain normal calcium consumption. (Expert Opinion)")
22
Guideline Statement 11. Patients with calcium stones and urinary citrate: increase intake of fruits and vegetables and limit non-dairy animal protein (Expert Opinion) Guideline Statement 12. Patients with uric acid stones or calcium stones and ↑ urinary uric acid : limitation of intake of non-dairy animal protein may help reduce stone recurrence Guideline Statement 13. Patients with cystine stones: limit sodium and protein intake
 Guideline Statement 12. Patients with uric acid stones or calcium stones and ↑ urinary uric acid : limitation of intake of non-dairy animal protein may help reduce stone. recurrence. Guideline Statement 13. Patients with cystine stones: limit sodium and protein intake.")
23
General preventive measures

24
ADHERENCE TO DASH-STYLE LOW SODIUM DIET
AND RISK OF SYMPTOMATIC NEPHROLITHIASIS HPFS (45,821 M), NHS I (94,108 older W) and NHS II (101,837 younger W) yr follow-up RR p for trend<0.001 1.0 0.8 0.6 0.4 0.2 Q 1 Q 2 Q 3 Q 4 Q 5 DASH score quintile Adjusted for age, BMI, fluids, alcohol, caffeine, thiazides, hypertension and diabetes status Taylor EN et al, JASN 2009
, NHS I (94,108 older W) and NHS II (101,837 younger W) yr follow-up. RR. p for trend< Q 1. Q 2. Q 3. Q 4. Q 5. DASH score quintile. Adjusted for age, BMI, fluids, alcohol, caffeine, thiazides, hypertension and diabetes status. Taylor EN et al, JASN")
25
DOTTORE : Se dovesse avere una colica renale, mi chiami e le darò qualcosa di efficace.
PAZIENTE : Non potrebbe darmi quel qualcosa già da adesso?

26
PREVENZIONE PRIMARIA …. Vuol dire prevenire già un primo episodio di calcolosi renale; …. E’ basata sulla conoscenza dei principali fattori causali della calcolosi; …. Deve essere realizzata a livello di popolazione, aumentando la consapevolezza e sostenendo stili di vita e abitudini alimentari efficaci su questi fattori.

27
PRIMARY PREVENTION …. means to prevent a first episode ever of kidney stones; ….should be based on the knowledge of the most frequent causal factors of KSD; …should be implemented at the population level by supporting life styles and dietary habits known to be effective on most KSD risk factors.

Presentazioni simili















 Consigliere Onorario della FADOI Emilia Romagna.>")





