Scaricare la presentazione

12
EVOLUZIONE DELL’INFEZIONE DA HIV
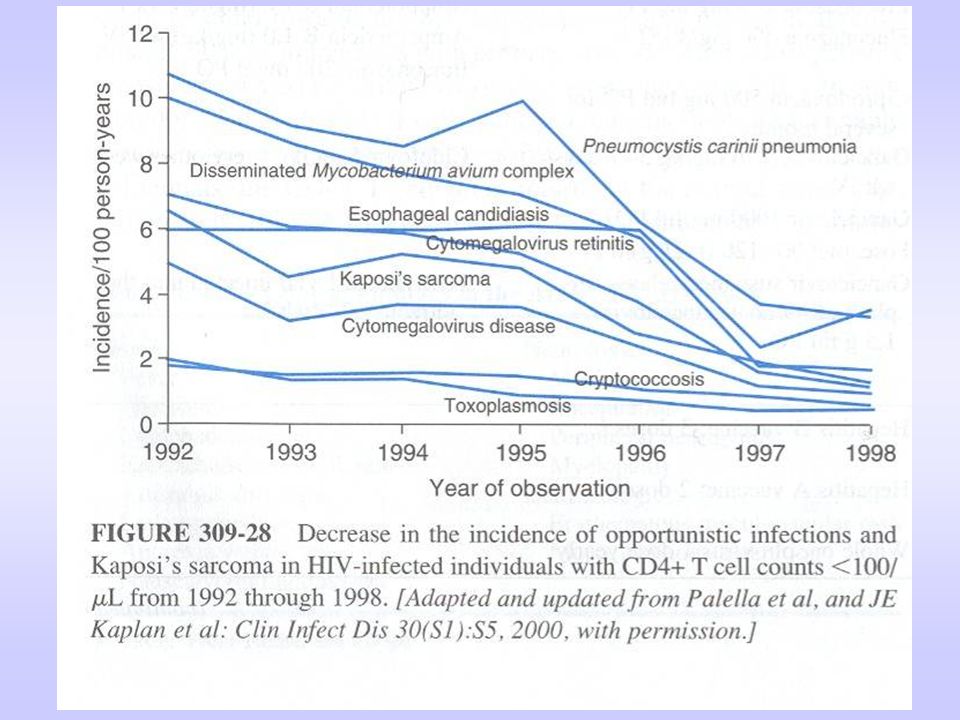
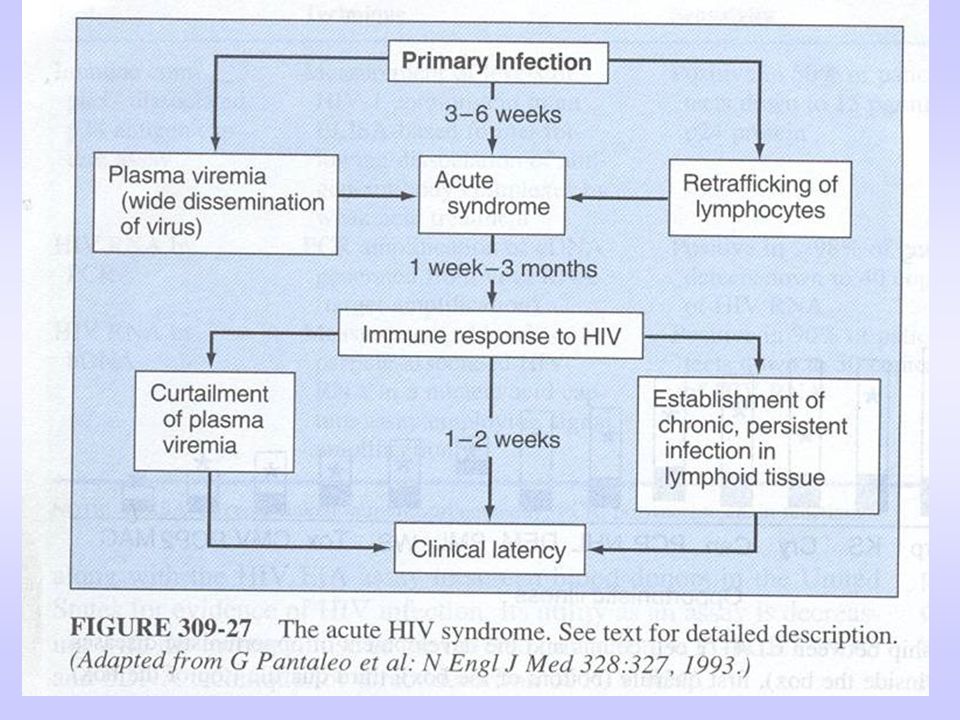
The natural course of HIV-1 infection on the basis of the longitudinal evolution of the two key surrogate markers — plasma viraemia and CD4+ T-lymphocyte count54. The phase of primary HIV-1 infection is generally associated with clinical symptoms of the acute retroviral syndrome. After the first months of infection, plasma viraemia stabilizes at an individual level and the CD4+ T-lymphocyte number normalizes. The protracted chronic phase of infection is clinically silent despite the fact that HIV-1 replicates continuously at high levels. AIDS is defined by the occurrence of opportunistic infections or HIV-1-associated malignancies as defined by the Centers for Disease Control and Prevention (CDC) classification of 1993 (Ref. 118). The risk of opportunistic infections increases significantly when the number of CD4+ T lymphocytes falls to below 200 per mm3. Viral diversity increases over the course of infection in accordance with the continuously high level of viral replication and the error-prone nature of HIV-1 reverse transcription.
 classification of 1993 (Ref. 118). The risk of opportunistic infections increases significantly when the number of CD4+ T lymphocytes falls to below 200 per mm3. Viral diversity increases over the course of infection in accordance with the continuously high level of viral replication and the error-prone nature of HIV-1 reverse transcription.")
15
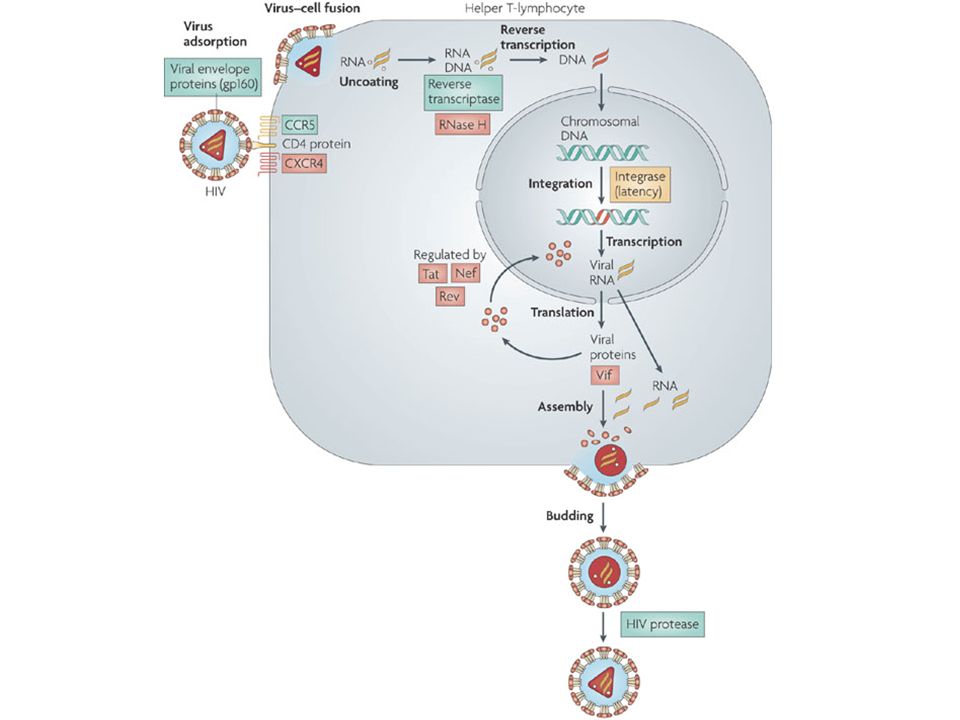
The human immunodeficiency virus (HIV) provirus is approximately 9
The human immunodeficiency virus (HIV) provirus is approximately 9.8 kb in length and encodes at least nine proteins. The genes encode proteins that can be divided into three classes: structural — Gag, Pol (polymerase) and Env (envelope); regulatory — Tat (transactivator of transcription) and Rev (regulatory for expression of viral proteins); and accessory — Vpu (viral protein u), Vpr (viral protein r), Vif (viral infectivity factor) and Nef (negative factor). HIV proteins released from infected cells can have direct effects on cells of the CNS. iNOS, inducible nitric oxide synthase; LTR, long terminal repeat; gp, glycoprotein, TNF , tumour necrosis factor- . Ellis et al. Nature Reviews Neuroscience 8, 33–44 (January 2007) | doi: /nrn2040
 provirus is approximately 9.8 kb in length and encodes at least nine proteins. The genes encode proteins that can be divided into three classes: structural — Gag, Pol (polymerase) and Env (envelope); regulatory — Tat (transactivator of transcription) and Rev (regulatory for expression of viral proteins); and accessory — Vpu (viral protein u), Vpr (viral protein r), Vif (viral infectivity factor) and Nef (negative factor). HIV proteins released from infected cells can have direct effects on cells of the CNS. iNOS, inducible nitric oxide synthase; LTR, long terminal repeat; gp, glycoprotein, TNF , tumour necrosis factor- . Ellis et al. Nature Reviews Neuroscience 8, 33–44 (January 2007) | doi: /nrn2040.")
16
CICLO VITALE DEL HIV

18
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs)
")
19
INIBITORI NUCLEOSIDICI DELLA TRANSCRITTASI INVERSA

20
TERMINAZIONE DELLA CATENA DA PARTE DI ANALOGHI NUCLEOSIDICI

21
Zidovudina Timidina chinasi Timidilato chinasi Nucleoside difosfato chinasi Didanosina Carrier nucleobasi 5’nucleotidasi Adenilosuccinato sintetasi Adenilosuccinato liasi Stavudina Diffusione Pirimidina difosfato chinasi Zalcitabina Carrier e diffusione Desossicitidina chinasi dCMP chinasi Lamivudina Abacavir Adenosina fosfotransferasi

22
INIBITORI NUCLEOTIDICI DELLA TRANSCRITTASI INVERSA

23
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs)
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs)")
24
INIBITORI NON-NUCLEOSIDICI DELLA TRANSCRITTASI INVERSA (NNRTI)
")
25
a | Three-dimensional structure of HIV-1 reverse transcriptase, with the fingers, palm, thumb, connection and RNase H domains, belonging to the p66 subunit, and the p51 subunit, based on Ref. 9. b | HIV-1 reverse transcriptase complexed with the DNA template primer. The reverse transcriptase heterodimer consists of the p66 subunit (dark blue) and the p51 subunit (light blue). The two magnesium ions in the active site are shown as purple balls. The side-chains of active-site amino acids Y183, M184, D185, D186 and D10 are represented as green-coloured van der Waals spheres. Residues of the non-nucleoside reverse transcriptase inhibitor binding site (L100, K101, K103, V106, V108, V179, Y181, Y188, P225, F227, W229, L234, P236 and Y318) are represented as yellow-coloured van der Waals spheres
 and the p51 subunit (light blue). The two magnesium ions in the active site are shown as purple balls. The side-chains of active-site amino acids Y183, M184, D185, D186 and D10 are represented as green-coloured van der Waals spheres. Residues of the non-nucleoside reverse transcriptase inhibitor binding site (L100, K101, K103, V106, V108, V179, Y181, Y188, P225, F227, W229, L234, P236 and Y318) are represented as yellow-coloured van der Waals spheres.")
26
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI)
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI)")
27
a | Except for tipranavir, all other HIV protease inhibitors can be considered as peptidomimetic in that they contain the non-scissile hydroxyethylene [-CH2-CHOH-] bond instead of the readily hydrolysable peptide [-CO-NH-] bond
![a | Except for tipranavir, all other HIV protease inhibitors can be considered as peptidomimetic in that they contain the non-scissile hydroxyethylene [-CH2-CHOH-] bond instead of the readily hydrolysable peptide [-CO-NH-] bond](http://slideplayer.it/slide/579108/2/images/27/a+%7C+Except+for+tipranavir%2C+all+other+HIV+protease+inhibitors+can+be+considered+as+peptidomimetic+in+that+they+contain+the+non-scissile+hydroxyethylene+%5B-CH2-CHOH-%5D+bond+instead+of+the+readily+hydrolysable+peptide+%5B-CO-NH-%5D+bond.jpg "a | Except for tipranavir, all other HIV protease inhibitors can be considered as peptidomimetic in that they contain the non-scissile hydroxyethylene [-CH2-CHOH-] bond instead of the readily hydrolysable peptide [-CO-NH-] bond")
28
ANTI-PROTEASICI PEPTIDICI

29
ANTI-PROTEASICI NON PEPTIDICI
FDA approval: June 2005

30
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite.")
31
INGRESSO DI HIV NELLA CELLULA OSPITE

32
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite Inibitori della fusione
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite. Inibitori della fusione.")
33
INIBITORI DELLA FUSIONE

34
INIBITORI DELLA FUSIONE
ENFUVIRTIDE

35
Fig. 1. The HIV-1 fusion process
Fig. 1. The HIV-1 fusion process. (a) HIV-1 gp120 (shown as a trimer) initially interacts with CD4 (only one CD4 molecule is shown). (b) This interaction uncovers a co-receptor-binding site and is followed by interaction with the co-receptor, usually CCR5 or CXCR4. (c) The gp41 trimer then undergoes profound conformational changes resulting in insertion of the fusion peptides into the target membrane, the N-terminal heptad repeats (in green) forming a coiled-coil (gp120 molecules are shown only in the first two frames). (d) The C-terminal heptad repeats (in yellow) then become arranged about the N-terminal repeats to form the six-helix bundle. This brings the membranes together and results in fusion. HIV entry inhibitors in clinical development, Pages Bryan M. O'Hara and William C. Olson
 HIV-1 gp120 (shown as a trimer) initially interacts with CD4 (only one CD4 molecule is shown). (b) This interaction uncovers a co-receptor-binding site and is followed by interaction with the co-receptor, usually CCR5 or CXCR4. (c) The gp41 trimer then undergoes profound conformational changes resulting in insertion of the fusion peptides into the target membrane, the N-terminal heptad repeats (in green) forming a coiled-coil (gp120 molecules are shown only in the first two frames). (d) The C-terminal heptad repeats (in yellow) then become arranged about the N-terminal repeats to form the six-helix bundle. This brings the membranes together and results in fusion. HIV entry inhibitors in clinical development, Pages Bryan M. O Hara and William C. Olson.")
36
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite Inibitori della fusione Inibitori dell’interazione con i co-recettori
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite. Inibitori della fusione. Inibitori dell’interazione con i co-recettori.")
37
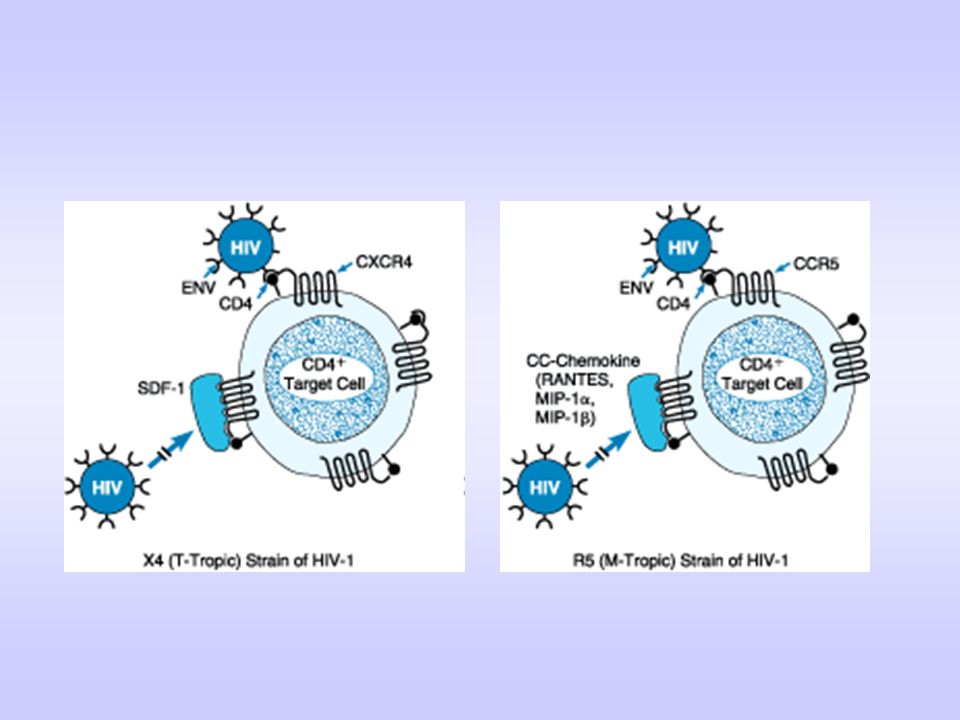
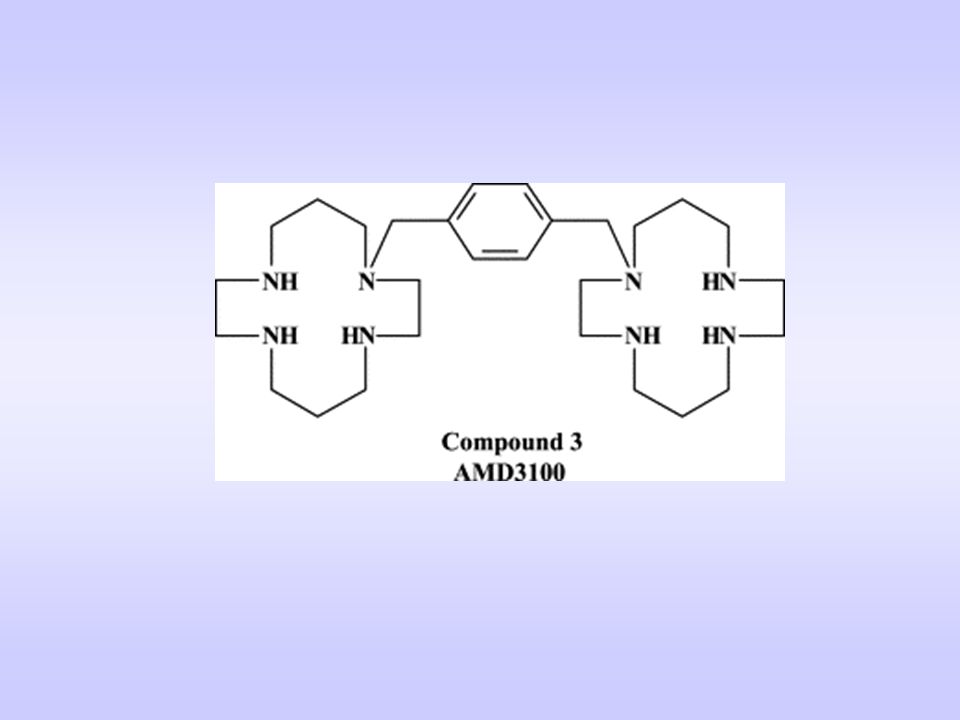
INIBIZIONE DEI CO-RECETTORI

38
Mechanism of action of bicyclams: inhibiting viral entry by blocking the CXCR4 receptor. During the viral adsorption process, a | the viral envelope glycoprotein gp120 interacts with the CD4 receptor at the cell membrane. b | Subsequently, gp120 interacts with the co-receptor CXCR4 for T-tropic (X4) HIV strains, whereupon c | the viral glycoprotein gp41 anchors into the cell membrane. The bicyclams block the interaction between gp120 and CXCR4. CCR, CC chemokine receptor; CXCR, CXC chemokine receptor; gp, glycoprotein.
 HIV strains, whereupon c | the viral glycoprotein gp41 anchors into the cell membrane. The bicyclams block the interaction between gp120 and CXCR4. CCR, CC chemokine receptor; CXCR, CXC chemokine receptor; gp, glycoprotein..")
40
BLOCCO DI CCR5

42
PRINCIPALI CLASSI DI FARMACI ANTI-HIV
Inibitori nucleosidici/nucleotidici della trascrittasi inversa (NRTIs) Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite Inibitori della integrasi
 Inibitori non nucleosidici della trascrittasi inversa (NNRTIs) Inibitori della proteasi (PI) Inibitori dell’ingresso nella cellula ospite. Inibitori della integrasi.")
43
Figure 2 | The two integrase catalytic reactions (3'-processing and strand transfer). The figure shows the viral DNA recombination (att) sites. 3'-processing takes place in the cytoplasm following reverse transcription (Fig. 1). It is a water-mediated endonucleolytic cleavage (green arrow in a and Box 1, figure part a) of the viral DNA immediately 3' from the conserved CA dinucleotide (Box 1, figure part a). 3'-processing generates reactive 3'-hydroxyls at both ends of the viral DNA (red circles (b); other 3'-hydroxyl ends and 5'-phosphate ends are shown as red and green dots, respectively). Integrase multimers (not shown) remain bound to the ends of the viral DNA as the pre-integration complexes (PICs) translocate to the nucleus. The second reaction (c to d) catalysed by integrase is strand transfer (3'-end joining), which inserts both viral DNA ends into a host-cell chromosome (acceptor DNA in blue). Strand transfer is coordinated in such a way that each of the two 3'-hydroxyl viral DNA ends (red circles) attacks a DNA phosphodiester bond on each strand of the host DNA acceptor with a five-base-pair stagger across the DNA major groove (d). Strand transfer leaves a five-base, single-stranded gap at each junction between the integrated viral DNA and the host acceptor DNA, and a two-base flap at the 5'-ends of the viral DNA (d and e). Gap filling and release of the unpaired 5'-ends of the viral DNA (arrows in e) are carried out in coordination with cellular repair enzymes.
 sites. 3 -processing takes place in the cytoplasm following reverse transcription (Fig. 1). It is a water-mediated endonucleolytic cleavage (green arrow in a and Box 1, figure part a) of the viral DNA immediately 3 from the conserved CA dinucleotide (Box 1, figure part a). 3 -processing generates reactive 3 -hydroxyls at both ends of the viral DNA (red circles (b); other 3 -hydroxyl ends and 5 -phosphate ends are shown as red and green dots, respectively). Integrase multimers (not shown) remain bound to the ends of the viral DNA as the pre-integration complexes (PICs) translocate to the nucleus. The second reaction (c to d) catalysed by integrase is strand transfer (3 -end joining), which inserts both viral DNA ends into a host-cell chromosome (acceptor DNA in blue). Strand transfer is coordinated in such a way that each of the two 3 -hydroxyl viral DNA ends (red circles) attacks a DNA phosphodiester bond on each strand of the host DNA acceptor with a five-base-pair stagger across the DNA major groove (d). Strand transfer leaves a five-base, single-stranded gap at each junction between the integrated viral DNA and the host acceptor DNA, and a two-base flap at the 5 -ends of the viral DNA (d and e). Gap filling and release of the unpaired 5 -ends of the viral DNA (arrows in e) are carried out in coordination with cellular repair enzymes..")
45
Formulazioni combinate
Atripla Efavirenz (NNRTI) + Tenofovir (NtRTI) + Emtricitabina (NRTI) Triomune Nevirapina (NNRTI) + Lamivudina (NRTI) + Stavudina (NRTI) Kaletra Lopinavir (PI) + Ritonavir (PI)
 + Tenofovir (NtRTI) + Emtricitabina (NRTI) Triomune. Nevirapina (NNRTI) + Lamivudina (NRTI) + Stavudina (NRTI) Kaletra. Lopinavir (PI) + Ritonavir (PI)")
46
HAART

47
DELLE TERAPIE ANTIRETROVIRALI
EFFETTI COLLATERALI DELLE TERAPIE ANTIRETROVIRALI Tossicità mitocondriale (NRTI)
")
48
EFFETTI MITOCONDRIALI DEI NRTI
Mitochondrial effects of NRTIs. The structure of the mitochondrion is indicated. On the right side of the diagram, the nucleoside reverse transcriptase inhibitor (NRTI) is phosphorylated by thymidine kinase 2 (TK2), the mitochondrial isoform, in the first step towards the formation of the pharmacologically and toxicologically active form. DNA pol- , the mitochondrial DNA polymerase, is inhibited by NRTI triphosphates to deplete mitochondrial DNA (mtDNA). mtDNA is necessary for many oxidative phosphorylation complex I proteins. mtDNA depletion causes a deficiency in complex I and an over-utilization of complex II, resulting in elevated superoxide levels (centre, top). The increase in superoxide levels that results increases oxidative stress to cellular macromolecules including aconitase, which on inactivation liberates ferrous iron and hydrogen peroxide. This, in turn, can provide substrates that can lead to the generation of hydroxyl radicals (which are highly reactive) and readily damage cellular macromolecules. AZT, zidovudine; TCA, tricarboxylic acid cycle.
 is phosphorylated by thymidine kinase 2 (TK2), the mitochondrial isoform, in the first step towards the formation of the pharmacologically and toxicologically active form. DNA pol- , the mitochondrial DNA polymerase, is inhibited by NRTI triphosphates to deplete mitochondrial DNA (mtDNA). mtDNA is necessary for many oxidative phosphorylation complex I proteins. mtDNA depletion causes a deficiency in complex I and an over-utilization of complex II, resulting in elevated superoxide levels (centre, top). The increase in superoxide levels that results increases oxidative stress to cellular macromolecules including aconitase, which on inactivation liberates ferrous iron and hydrogen peroxide. This, in turn, can provide substrates that can lead to the generation of hydroxyl radicals (which are highly reactive) and readily damage cellular macromolecules. AZT, zidovudine; TCA, tricarboxylic acid cycle.")
49
MODALITÀ DI INIBIZIONE DELLA DNA POL-
DA PARTE DEI NRTI Modes of inhibition of DNA pol- by NRTIs. a | Nucleoside reverse transcriptase inhibitors (NRTIs), such as AZT, are competitive inhibitors and compete with the normal nucleotide triphosphates for incorporation into growing DNA chains by DNA pol-γ
, such as AZT, are competitive inhibitors and compete with the normal nucleotide triphosphates for incorporation into growing DNA chains by DNA pol-γ.")
50
MODALITÀ DI INIBIZIONE DELLA DNA POL-
DA PARTE DEI NRTI Modes of inhibition of DNA pol- by NRTIs. b | The anti-HIV NRTIs are chain terminators; once incorporated into a growing strand, DNA replication is abruptly halted.

51
MODALITÀ DI INIBIZIONE DELLA DNA POL-
DA PARTE DEI NRTI Modes of inhibition of DNA pol- by NRTIs. c | The terminally incorporated NRTI persists in DNA because it is resistant to exonucleolytic removal by the exonuclease activity of DNA pol-γ due to the lack of a 3' OH group. With native nucleosides, it forms a hydrogen bond to a conserved Glu residue in the active site of the exonuclease. This facilitates an ionic bond to the catalytic Mg2+ and a hydroxide anion which allows efficient removal of the terminal nucleotide monophosphate.

52
MODALITÀ DI INIBIZIONE DELLA DNA POL-
DA PARTE DEI NRTI Modes of inhibition of DNA pol- by NRTIs. . d | The intermediate monophosphorylated forms of some NRTIs are known to accumulate to millimolar concentrations in the cell, owing to the inefficient conversion to diphosphate and triphosphate forms. High concentrations of monophosphorylated NRTIs can inhibit the exonucleolytic proofreading function of DNA pol-γ and therefore lower the fidelity of mtDNA replication.

53
DELLE TERAPIE ANTIRETROVIRALI
EFFETTI COLLATERALI DELLE TERAPIE ANTIRETROVIRALI Tossicità mitocondriale (NRTI) Lipodistrofia (NRTI e inibitori delle proteasi) Dislipidemie, resistenza all’insulina e malattie CV
 Lipodistrofia (NRTI e inibitori delle proteasi) Dislipidemie, resistenza all’insulina e malattie CV.")
54
Pathogenesis of HIV lipodystrophy, dyslipidaemia and insulin resistance. Protease inhibitors can perform a number of functions: inhibit the hepatocyte proteasome, thereby stimulating synthesis of triglyceride; inhibit GLUT-4 in skeletal muscle and adipocytes, so inhibiting glucose uptake; and inhibit SREBP-1 nuclear localization within adipocytes, and so decreasing adipocyte differentiation. Nucleoside analogues deplete mitochondrial DNA within peripheral adipocytes, accelerating apoptosis and decreasing lipid storage capacity. Insulin resistance results from the combination of GLUT-4 inhibition, hyperlipidaemia, peripheral lipoatrophy (possibly via reduced secretion of adiponectin and leptin, and increased production of TNF- ), and possibly visceral fat accumulation. The pathogenesis of visceral fat accumulation is unclear, and may relate to a direct effect of protease inhibitors, or indirect effects of hyperlipidaemia, insulin resistance, lipoatrophy (that is, inability to store fat peripherally with redistribution to functional visceral adipocytes) or functional growth hormone deficiency. Efavirenz and lipoatrophy also contribute to dyslipidaemia. Pre-morbid states such as syndrome X and increasing age probably exacerbate several features. EFV, efavirenz; GH, growth hormone; GLUT-4, facilitated glucose transporter-4; mtDNA, mitochondrial DNA; NRTI, nucleoside reverse transcriptase inhibitor; SREBP-1; sterol regulatory enhancer binding protein-1; TNF, tumour-necrosis factor.
, and possibly visceral fat accumulation. The pathogenesis of visceral fat accumulation is unclear, and may relate to a direct effect of protease inhibitors, or indirect effects of hyperlipidaemia, insulin resistance, lipoatrophy (that is, inability to store fat peripherally with redistribution to functional visceral adipocytes) or functional growth hormone deficiency. Efavirenz and lipoatrophy also contribute to dyslipidaemia. Pre-morbid states such as syndrome X and increasing age probably exacerbate several features. EFV, efavirenz; GH, growth hormone; GLUT-4, facilitated glucose transporter-4; mtDNA, mitochondrial DNA; NRTI, nucleoside reverse transcriptase inhibitor; SREBP-1; sterol regulatory enhancer binding protein-1; TNF, tumour-necrosis factor..")
55
DELLE TERAPIE ANTIRETROVIRALI
EFFETTI COLLATERALI DELLE TERAPIE ANTIRETROVIRALI Tossicità mitocondriale (NRTI) Lipodistrofia (NRTI e inibitori delle proteasi) Dislipidemie, resistenza all’insulina e malattie CV Reazioni di ipersensibilità Disfunzione epatica
 Lipodistrofia (NRTI e inibitori delle proteasi) Dislipidemie, resistenza all’insulina e malattie CV. Reazioni di ipersensibilità. Disfunzione epatica.")
56
EFFETTI COLLATERALI DELLA TERAPIA CON INIBITORI DELLA FUSIONE
Reazioni a livello del sito di iniezione Aumento dell’incidenza di polmonite batterica Reazione sistemica di ipersensibilità

57
The predominant transition since the introduction of potent combination antiretroviral therapies (cART) has been a replacement of human immunodeficiency virus (HIV)-associated dementia (HAD) and mild neurocognitive disorder (MND) by a milder, chronic asymptomatic neurocognitive impairment (ANI), with which individuals can live for many years1, 142. The impact of a neurocognitive disorder that is severe in a patient who lives for a relatively short period of time might actually be less than the impact of a milder cognitive disorder in an individual who lives for decades. Question marks denote uncertainty as to the longevity of cART-treated individuals.

58
Ellis et al. Nature Reviews Neuroscience 8, 33–44 (January 2007) | doi:10.1038/nrn2040
Neuronal dendrites and postsynaptic structures are damaged in human immunodeficiency virus (HIV) encephalitis28. Similar damage is induced in uninfected transgenic mice that express the HIV gp120 envelope protein68, and in neuronal cultures exposed to exogenous gp120 (Ref. 66). a | Confocal microscope image of post-mortem prefrontal cerebral cortex tissue from an HIV-seronegative human control, immunostained and double-labelled for MAP2 (microtubule-associated protein 2, an important structural and functional component of dendrites; green), and synaptophysin (red), a key presynaptic protein. Inset is a normal dendrite and spines stained by the Golgi impregnation method. b | Similarly labelled prefrontal cortex tissue from a patient who died with HIV encephalitis. Inset is a dendrite and spines from the patient stained by the Golgi impregnation method. Arrows indicate dendritic beading and damage. c | Prefrontal cortex tissue from a non-transgenic control mouse, illustrating normal dendrites and cell bodies. d | Prefrontal cortex tissue from a mouse expressing a gp120 transgene in brain tissue, illustrating abnormal cell bodies and dendrites (arrows). There is atrophy and vacuolization of dendrites. e | A control primary fetal cortical human neuron in culture, illustrating normal dendrites and cell bodies. f | Primary human neuron in culture exposed to gp120 for 3 days, illustrating abnormal dendrites with atrophy and beading (arrows).
 encephalitis28. Similar damage is induced in uninfected transgenic mice that express the HIV gp120 envelope protein68, and in neuronal cultures exposed to exogenous gp120 (Ref. 66). a | Confocal microscope image of post-mortem prefrontal cerebral cortex tissue from an HIV-seronegative human control, immunostained and double-labelled for MAP2 (microtubule-associated protein 2, an important structural and functional component of dendrites; green), and synaptophysin (red), a key presynaptic protein. Inset is a normal dendrite and spines stained by the Golgi impregnation method. b | Similarly labelled prefrontal cortex tissue from a patient who died with HIV encephalitis. Inset is a dendrite and spines from the patient stained by the Golgi impregnation method. Arrows indicate dendritic beading and damage. c | Prefrontal cortex tissue from a non-transgenic control mouse, illustrating normal dendrites and cell bodies. d | Prefrontal cortex tissue from a mouse expressing a gp120 transgene in brain tissue, illustrating abnormal cell bodies and dendrites (arrows). There is atrophy and vacuolization of dendrites. e | A control primary fetal cortical human neuron in culture, illustrating normal dendrites and cell bodies. f | Primary human neuron in culture exposed to gp120 for 3 days, illustrating abnormal dendrites with atrophy and beading (arrows).")
59
The progression of cognitive impairment in patients with human immunodeficiency virus (HIV) is unpredictable, waxing and waning over time, but does vary depending on treatment. The figure illustrates a hypothetical course of neurocognitive disorder in three patients with HIV. The red line represents an individual taking no or ineffective antiretroviral therapy. Both viral and host factors contribute to cumulative injury and a reduction in the capacity for repair of the synaptodendritic network. The green line represents an individual who has undergone successful systemic treatment of HIV, but with only partial CNS efficacy due to limited penetration of antiretroviral drugs into brain tissue. The blue line represents an individual who has undergone successful treatment of both systemic and CNS HIV infection by using combined antiretroviral therapy (cART) with good CNS penetration. Normal neurocognitive status, no neurocognitive impairment. Asymptomatic neurocognitive impairment (ANI), mild neurocognitive impairment, not clearly affecting daily activities. Mild neurocognitive disorder (MND; also known as minor cognitive motor disorder, MCMD), mild–moderate neurocognitive impairment with early functional loss. HIV associated dementia (HAD), moderate–severe neurocognitive impairment with obvious deficits in activities of daily living. Unlike in many neurodegenerative disorders such as Alzheimer's disease, the various degrees of HIV neurocognitive dysfunction depicted here are not true stages, in that more severe degrees of impairment do not necessarily follow milder ones in a predictable order. In fact, some investigators believe that these types of neurocognitive dysfunction are qualitatively as well as quantitatively different.
 with good CNS penetration. Normal neurocognitive status, no neurocognitive impairment. Asymptomatic neurocognitive impairment (ANI), mild neurocognitive impairment, not clearly affecting daily activities. Mild neurocognitive disorder (MND; also known as minor cognitive motor disorder, MCMD), mild–moderate neurocognitive impairment with early functional loss. HIV associated dementia (HAD), moderate–severe neurocognitive impairment with obvious deficits in activities of daily living. Unlike in many neurodegenerative disorders such as Alzheimer s disease, the various degrees of HIV neurocognitive dysfunction depicted here are not true stages, in that more severe degrees of impairment do not necessarily follow milder ones in a predictable order. In fact, some investigators believe that these types of neurocognitive dysfunction are qualitatively as well as quantitatively different..")
60
Probabilità/rapporto
Probabilità di trasmissione sessuale di HIV-1 Trasmissione Probabilità/rapporto Maschio maschio 1/10 – 1/1,600 Maschio femmina 1/200 – 1/2,000 Femmina maschio 1/200 – 1/10,000

61
INIBIZIONE DELL’ADESIONE

62
a | Direct infection of epithelial cells
a | Direct infection of epithelial cells. b | Transcytosis through epithelial cells and/or specialized microfold (M) cells. c | Epithelial transmigration of infected donor cells. d | Uptake by intra-epithelial Langerhans cells. e | Circumvention of the epithelial barrier through physical breaches11. Successful transfer of virus across epithelial barriers would result in HIV-1 uptake by migratory dendritic cells (by DC-SIGN or another mannose C-type lectin receptor) and subsequent dissemination to draining lymph nodes115 and/or localized mucosal HIV-1 infection, leading to recruitment of additional susceptible c
 cells. c | Epithelial transmigration of infected donor cells. d | Uptake by intra-epithelial Langerhans cells. e | Circumvention of the epithelial barrier through physical breaches11. Successful transfer of virus across epithelial barriers would result in HIV-1 uptake by migratory dendritic cells (by DC-SIGN or another mannose C-type lectin receptor) and subsequent dissemination to draining lymph nodes115 and/or localized mucosal HIV-1 infection, leading to recruitment of additional susceptible c.")
63
Potential mechanisms of action for microbicide compounds
Potential mechanisms of action for microbicide compounds. Microbicides that act as a lubricant coat the epithelial surface, which might reduce the risk of trauma and provide a physical barrier against infection. Prevention (or treatment) of other sexually transmitted diseases (STDs) can reduce the risk of HIV-1 transmission by reducing the risk of epithelial inflammation and ulceration. In the vagina, maintaining the normal flora — and therefore maintaining the vaginal pH at virucidal levels (pH less than 4.5) — could also reduce the risk of transmission. Once the virus has crossed the epithelial barrier, potential microbicidal strategies include targeting HIV-1 uptake by dendritic cells; targeting reverse transcriptase and targeting HIV-1 fusion and/or absorption.
 of other sexually transmitted diseases (STDs) can reduce the risk of HIV-1 transmission by reducing the risk of epithelial inflammation and ulceration. In the vagina, maintaining the normal flora — and therefore maintaining the vaginal pH at virucidal levels (pH less than 4.5) — could also reduce the risk of transmission. Once the virus has crossed the epithelial barrier, potential microbicidal strategies include targeting HIV-1 uptake by dendritic cells; targeting reverse transcriptase and targeting HIV-1 fusion and/or absorption.")
64
Potential viral targets for microbicide compounds
Potential viral targets for microbicide compounds. Successful microbicide candidates must target conserved features of HIV-1. Although some candidates, such as the detergent nonoxynol-9, target the viral membrane, most are directed towards either the gp120 or gp41 components of the HIV-1 Env protein complex (Box 3). Microbicide candidates can interfere with various stages of the fusion process, for example, cyanovirin-N (CV-N), CD4-IgG2 and anti-Env mAbs b12 and 2G12 all impede the binding of gp120 to CD4 and/or a co-receptor. Ig, immunoglobulin; LFA-1, lymphocyte-function-associated molecule-1; mAbs, monoclonal antibodies; MHC, major histocompatibility complex; SAMMA, mandelic acid condensation product.
. Microbicide candidates can interfere with various stages of the fusion process, for example, cyanovirin-N (CV-N), CD4-IgG2 and anti-Env mAbs b12 and 2G12 all impede the binding of gp120 to CD4 and/or a co-receptor. Ig, immunoglobulin; LFA-1, lymphocyte-function-associated molecule-1; mAbs, monoclonal antibodies; MHC, major histocompatibility complex; SAMMA, mandelic acid condensation product.")
65
Farmaci anti-retrovirali attualmente (2007) approvati
 approvati")
66
Farmaci anti-retrovirali attualmente (2007) approvati
 approvati")
67
Farmaci anti-retrovirali attualmente (2007) approvati
 approvati")
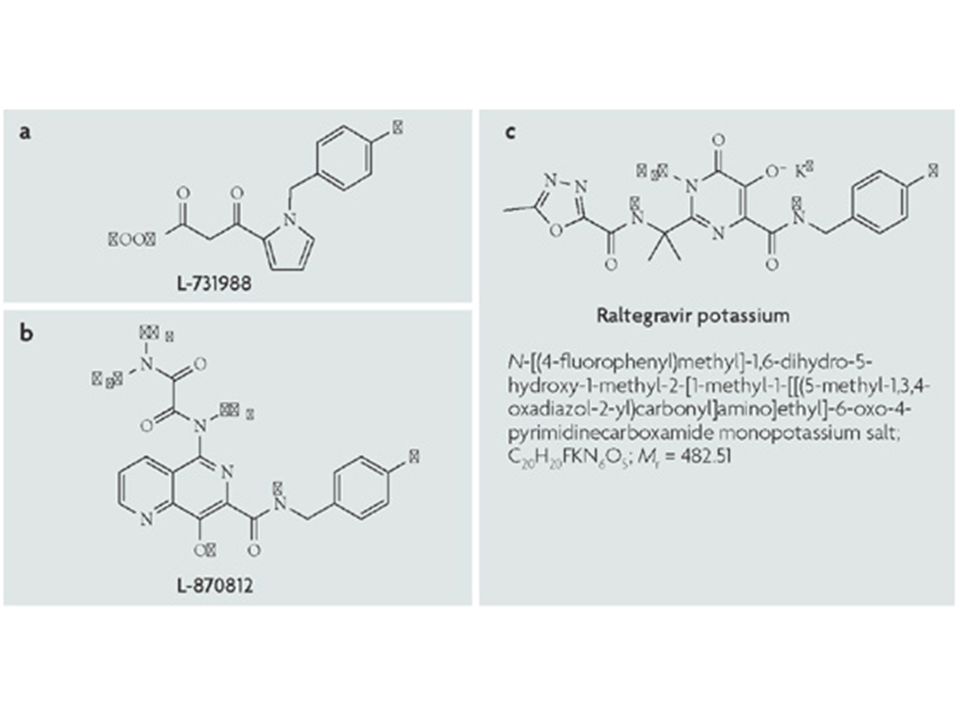
68
Farmaci anti-retrovirali attualmente (2007) approvati
Integrase inhibitors Raltegravir Isentress Merck & Co