Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Sequence of events in hemostasis
Sequence of events in hemostasis. The hemostatic process can be divided into four steps: vasoconstriction, primary hemostasis, secondary hemostasis, and resolution. A. vascular injury causes vascular denudation. Endothelin, released by activated endothelium,and neurohumoral factor(s) induce transient vasoconstriction. B. Injury-induced exposure of the subendothelial matrix (1) provides a substrate for platelet adhesion and activation (2). In the granule release reaction, Activated plateles secrete Thromboxane A2 (TxA2) and ADP (3. TxA2 and ADP released by activated platelets caunearby platelets to become activated; these newly activated platelets undergo shape change (4) and are recruited to the site of injury (5). The aggregation of activated platelets at the site of injury form a hemostatic plug (6). C. Tissue factor expressed on activated endothelial cells together with acidic phospholipids expressed on activated platelets and activated endothelial cells (2), initiate the steps of the coagulation cascade, culminating in the activation of thrombin (3). Thrombin proteolytically activates fibrinogen to form fibrin, which polymerizes around the site of injury, resulting in the formation of a definitive (secondary) hemostatic plug (4). D. Natural anticoagulant and thrombolytic factors limit the hemostatic process to the site of vascular injury. These factors include tissue plasminogen activator t-PA, which activates the fibrinolytic system (1); thrombomodulin, which activates inhibitors of the coagulation cascade (2); prostacyclin, which inhibits both platelet activation and vasoconstriction (3); and surface heparin-like molecules, which catalyze the inactivation of coagulation factors.
 induce transient vasoconstriction. B. Injury-induced exposure of the subendothelial matrix (1) provides a substrate for platelet adhesion and activation (2). In the granule release reaction, Activated plateles secrete Thromboxane A2 (TxA2) and ADP (3. TxA2 and ADP released by activated platelets caunearby platelets to become activated; these newly activated platelets undergo shape change (4) and are recruited to the site of injury (5). The aggregation of activated platelets at the site of injury form a hemostatic plug (6). C. Tissue factor expressed on activated endothelial cells together with acidic phospholipids expressed on activated platelets and activated endothelial cells (2), initiate the steps of the coagulation cascade, culminating in the activation of thrombin (3). Thrombin proteolytically activates fibrinogen to form fibrin, which polymerizes around the site of injury, resulting in the formation of a definitive (secondary) hemostatic plug (4). D. Natural anticoagulant and thrombolytic factors limit the hemostatic process to the site of vascular injury. These factors include tissue plasminogen activator t-PA, which activates the fibrinolytic system (1); thrombomodulin, which activates inhibitors of the coagulation cascade (2); prostacyclin, which inhibits both platelet activation and vasoconstriction (3); and surface heparin-like molecules, which catalyze the inactivation of coagulation factors.")
2
The role of platelets in thrombus formation
The role of platelets in thrombus formation. a | Circulating platelets are usually kept in an inactive state by prostacyclin and nitric oxide (NO) released by the endothelial cells that line the walls of blood vessels. Endothelial cells also express CD39 on their surface, which inhibits platelet activation by converting adenosine diphosphate (ADP), a potent inducer of platelet activation, into adenosine monophosphate (AMP). b, c | At sites where the blood vessel wall has been injured, the platelets adhere to the exposed subendothelium through interactions between collagen, von Willebrand factor and fibronectin and their receptors on the platelets, integrin 2 1, glycoprotein Ib-IX (GP Ib-IX) and integrin 5 1, respectively. Both thrombin and ADP cause platelets to change into an active conformation. d | Activated platelets secrete ADP, platelet-derived growth factor, and fibrinogen from storage granules in the platelet, and thromboxane A2 (TXA2), produced by immediate biosynthesis. ADP and TXA2 cause circulating platelets to change shape and become activated. e | Glycoprotein IIb/IIIa receptors on the surface of activated platelets bind fibrinogen, leading to the formation of fibrinogen bridges between the platelets, resulting in platelet aggregation. This, and the simultaneous formation of a fibrin mesh (not shown), lead to the formation of a platelet thrombus. f | Clot retraction then leads to formation of a stable thrombus
 released by the endothelial cells that line the walls of blood vessels. Endothelial cells also express CD39 on their surface, which inhibits platelet activation by converting adenosine diphosphate (ADP), a potent inducer of platelet activation, into adenosine monophosphate (AMP). b, c | At sites where the blood vessel wall has been injured, the platelets adhere to the exposed subendothelium through interactions between collagen, von Willebrand factor and fibronectin and their receptors on the platelets, integrin 2 1, glycoprotein Ib-IX (GP Ib-IX) and integrin 5 1, respectively. Both thrombin and ADP cause platelets to change into an active conformation. d | Activated platelets secrete ADP, platelet-derived growth factor, and fibrinogen from storage granules in the platelet, and thromboxane A2 (TXA2), produced by immediate biosynthesis. ADP and TXA2 cause circulating platelets to change shape and become activated. e | Glycoprotein IIb/IIIa receptors on the surface of activated platelets bind fibrinogen, leading to the formation of fibrinogen bridges between the platelets, resulting in platelet aggregation. This, and the simultaneous formation of a fibrin mesh (not shown), lead to the formation of a platelet thrombus. f | Clot retraction then leads to formation of a stable thrombus.")
3
Platelet adhesion and aggregation
Platelet adhesion and aggregation. Von Willebrand factor mediates platelet adhesion to the subendothelium by binding both to the platelet membrane gkycoprotein GPIb and to exposed subendothelial collagen. During platelet aggregation, fibrinogen crosslinks platelets to one another by binding to GPIIb-IIIa receptors on platelet membranes.

4
Platelet activation. Platelet activation is initiated at the site of vascular injury when circulatin platelets adhere to exposed subendothelial collagen and are activated by locally generated mediators. Activated platelets undergo shape change and granule release, and plkatelet aggregates are formed ad additional platelets are recruited and activated. Platelet recruitment is mediated by release of soluble platelet factors, including ADP and TxA2. Tissue factor, expresed on activated endothelium is a critical initiating component in the coagulation cascade. The membranes of activated platelets provide a surface for a number of critical reactions in the coagulation cascade, including the conversion of prothrombin to thrombin.

5
The fibrinolytic system
The fibrinolytic system. Plasmin is formed by theproteolytic cleavage of plasminogen by tissue-type or urokinase-type plasminogen activator. Plasmin formation can be inhibited by plasminogen activator inhibitor 1 or 2, which binds to and inactivates plasminogena ctivators. In the fbrinolytic reaction plasmin cleaves crosslinked fibrin polymers into fibrin degradation products. Alpha2 antiplasmin which circulates in the bloodstream, neutralizes free plasmin in the circulation.

6
COAGULOPATIE

7
EMOFILIA A B è dovuta a un deficit è dovuta a un deficit
congenito di Fattore VIII B è dovuta a un deficit congenito di Fattore IX

8
LA “TRIADE DI VIRCHOW” Virchow’s triad. Endothelial injury, abnormal blood flow and hypercoagulability are thr and hypercoagulability, while abnormal blood flow can cause bothe endothelial injury and hypercoagulabilityee factors that predispose to thrombus formation. These three factors are interrelated; endothelial injury predisposes to abnormal blood flow

9
FATTORI CHE PREDISPONGONO ALLA FORMAZIONE DI TROMBI
1) Lesioni della parete vascolare ipertensione flusso turbolento iperlipidemia diabete mellito traumi alcune infezioni
 Lesioni della parete vascolare. ipertensione. flusso turbolento. iperlipidemia. diabete mellito. traumi. alcune infezioni.")
10
FATTORI CHE PREDISPONGONO ALLA FORMAZIONE DI TROMBI
2) Alterazioni del flusso ematico Immobilità prolungata Promuovono la formazione di trombi causando attivazione dell’endotelio facilitando il contatto tra piastrine e parete vascolare evitando la diluizione dei fattori pro-coagulanti
 Alterazioni del flusso ematico. Immobilità prolungata. Promuovono la formazione di trombi. causando attivazione dell’endotelio. facilitando il contatto tra piastrine e parete vascolare. evitando la diluizione dei fattori pro-coagulanti.")
11
FATTORI CHE PREDISPONGONO ALLA FORMAZIONE DI TROMBI
3) Anormale coagulabilità del sangue
 Anormale coagulabilità del sangue.")
12
ANTIAGGREGANTI PIASTRINICI
Farmaci attivi sulla cascata dell’acido arachidonico

13
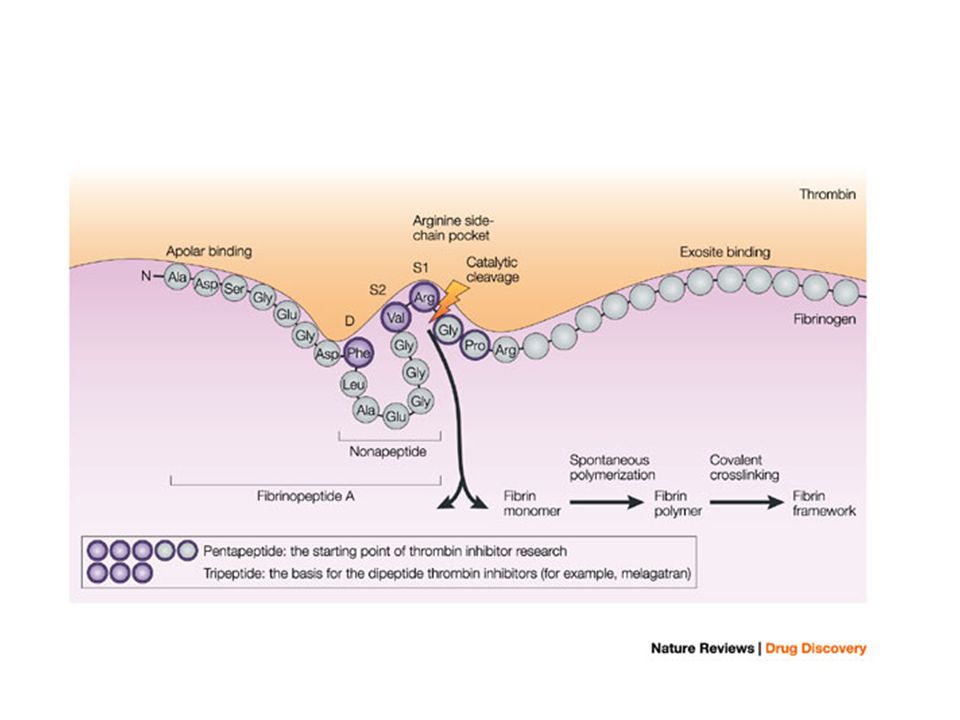
Molecular targets of current antithrombotic drugs
Molecular targets of current antithrombotic drugs. The principal factor regulating the adhesiveness of platelets is the activation state of GPIIb–IIIa. The affinity status of this receptor is strictly regulated by a balance of activating (+ve; ADP, thrombin, TXA2) and inhibitory signals (-ve; prostacyclin, NO). A number of these regulatory pathways have been successfully targeted therapeutically, leading to the development of a diverse range of antithrombotic approaches. These include various surface-receptor antagonists (ADP P2Y12 receptor: ticlopidine and clopidogrel; GPIIb–IIIa: abciximab, tirofiban and eptifibatide), inhibitors of platelet signalling enzymes (COX: aspirin; cAMP PDE: cilostazol; cGMP PDE: dipyridamole), receptor agonists (prostacyclin: iloprost) and soluble agonist inhibitors (thrombin: heparins, direct thrombin inhibitors or vitamin K antagonists). *Note: the antithrombotic effects of thrombin antagonists are primarily due to the inhibition of fibrin generation, although they can also indirectly dampen platelet activation. Also, it should be noted that although dipyridamole is primarily a cGMP PDE inhibitor, it also indirectly affects cAMP levels and inhibits cellular uptake and metabolism of adenosine, leading to further inhibition of platelet function. The efficacy of individual drug therapies (see Box 1) is influenced by a number of factors, including the clinical indication for antithrombotic therapy, patient responsiveness to the therapeutic agent as well as drug pharmacokinetics and pharmacodynamics. For example, although aspirin and ADP-receptor antagonists inhibit two important pathways for platelet activation, other alternative pathways — that is, downstream of thrombin receptors — can bypass the effects of these drugs and induce GPIIb–IIIa activation and thrombosis. Direct GPIIb–IIIa antagonists overcome this limitation, producing potent antithrombotic effects. AA, arachidonic acid; COX, cyclooxygenase; NO, nitric oxide; PDE, phosphodiesterase; TXA2, thromboxane A2.
 and inhibitory signals (-ve; prostacyclin, NO). A number of these regulatory pathways have been successfully targeted therapeutically, leading to the development of a diverse range of antithrombotic approaches. These include various surface-receptor antagonists (ADP P2Y12 receptor: ticlopidine and clopidogrel; GPIIb–IIIa: abciximab, tirofiban and eptifibatide), inhibitors of platelet signalling enzymes (COX: aspirin; cAMP PDE: cilostazol; cGMP PDE: dipyridamole), receptor agonists (prostacyclin: iloprost) and soluble agonist inhibitors (thrombin: heparins, direct thrombin inhibitors or vitamin K antagonists). *Note: the antithrombotic effects of thrombin antagonists are primarily due to the inhibition of fibrin generation, although they can also indirectly dampen platelet activation. Also, it should be noted that although dipyridamole is primarily a cGMP PDE inhibitor, it also indirectly affects cAMP levels and inhibits cellular uptake and metabolism of adenosine, leading to further inhibition of platelet function. The efficacy of individual drug therapies (see Box 1) is influenced by a number of factors, including the clinical indication for antithrombotic therapy, patient responsiveness to the therapeutic agent as well as drug pharmacokinetics and pharmacodynamics. For example, although aspirin and ADP-receptor antagonists inhibit two important pathways for platelet activation, other alternative pathways — that is, downstream of thrombin receptors — can bypass the effects of these drugs and induce GPIIb–IIIa activation and thrombosis. Direct GPIIb–IIIa antagonists overcome this limitation, producing potent antithrombotic effects. AA, arachidonic acid; COX, cyclooxygenase; NO, nitric oxide; PDE, phosphodiesterase; TXA2, thromboxane A2.")
14
ANTIAGGREGANTI PIASTRINICI
Farmaci attivi sulla cascata dell’acido arachidonico acido acetilsalicilico

15
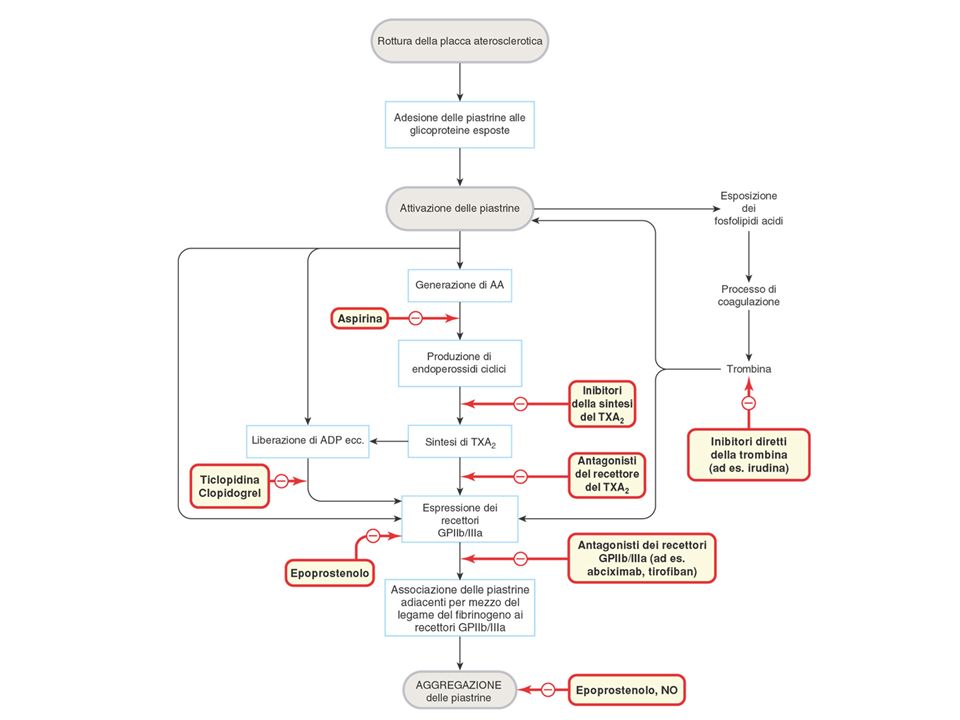
Effetti di agenti antipiastrinici sull’attivazione piastrinica
Effetti di agenti antipiastrinici sull’attivazione piastrinica. Il trombossano A2 (TXA2) attiva, mentre la prostaciclina (PGI2) inibisce l’attivazione piastrinica. L’effetto dell’aspirina sulla produzione di PGI2 in cellule endoteliali è di durata relativamente breve rispetto ai suoi effetti sulla produzione di TXA2-
 attiva, mentre la prostaciclina (PGI2) inibisce l’attivazione piastrinica. L’effetto dell’aspirina sulla produzione di PGI2 in cellule endoteliali è di durata relativamente breve rispetto ai suoi effetti sulla produzione di TXA2-")
16
ANTIAGGREGANTI PIASTRINICI
Farmaci attivi sulla cascata dell’acido arachidonico acido acetisalicilico inibitori della trombossano A2 (TXA2) sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2 inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP
 sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2. inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP.")
17
Different subtypes of ADP receptors. There are three main ADP receptors. Through various second messenger systems, these receptors contribute to platelet activation, shape change, secretion and aggregation. P2Y12 is the target of action of the active metabolite of clopidogrel; the experimental compound AR-C69931MX also binds to this receptor. Adenosine 3',5'-diphosphate (A3P5P) binds to the P2Y1 receptor. ATP activates the P2X1 ion channel, mediating a rapid influx of calcium, leading to platelet shape change and aggregation (not shown). P2Y1 and P2Y12 are G-protein coupled receptors (GPCRs). The P2Y12 receptor leads to inhibition of adenylyl cyclase (AC) and a decrease in cyclic AMP (cAMP), resulting in platelet secretion of thrombotic mediators and in platelet aggregation. The P2Y1 receptor leads to increased calcium influx, resulting in platelet shape change.
 binds to the P2Y1 receptor. ATP activates the P2X1 ion channel, mediating a rapid influx of calcium, leading to platelet shape change and aggregation (not shown). P2Y1 and P2Y12 are G-protein coupled receptors (GPCRs). The P2Y12 receptor leads to inhibition of adenylyl cyclase (AC) and a decrease in cyclic AMP (cAMP), resulting in platelet secretion of thrombotic mediators and in platelet aggregation. The P2Y1 receptor leads to increased calcium influx, resulting in platelet shape change..")
18
ANTI-AGGREGANTI PIASTRINICI

19
ANTIAGGREGANTI PIASTRINICI
Farmaci attivi sulla cascata dell’acido arachidonico acido acetilsalicilico inibitori della trombossano A2 (TXA2) sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2 inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP inibitori delle fosfodiesterasi
 sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2. inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP. inibitori delle fosfodiesterasi.")
20
ANTIAGGREGANTI PIASTRINICI
Farmaci attivi sulla cascata dell’acido arachidonico acido acetilsalicilico inibitori della trombossano A2 (TXA2) sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2 inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP inibitori delle fosfodiesterasi agenti attivi sulla glicoproteina IIb/IIIa
 sintetasi (p.e. dazoxiben) antagonisti del recettore per TXA2. inibitori della trombossano A2 (TXA2) sintetasi e antagonisti del recettore per TXA2 (p.e. ridogrel) analoghi stabili della prostaciclina (iloprost) antagonisti dei recettori per ADP. inibitori delle fosfodiesterasi. agenti attivi sulla glicoproteina IIb/IIIa.")
21
ANTI-AGGREGANTI PIASTRINICI
Inibitori della glicoproteina IIb/IIIa (IIb3) Abciximab Eptifibatide Tirofiban Blocco del sito di legame RGD
 Abciximab. Eptifibatide. Tirofiban. Blocco del sito di legame RGD.")
23
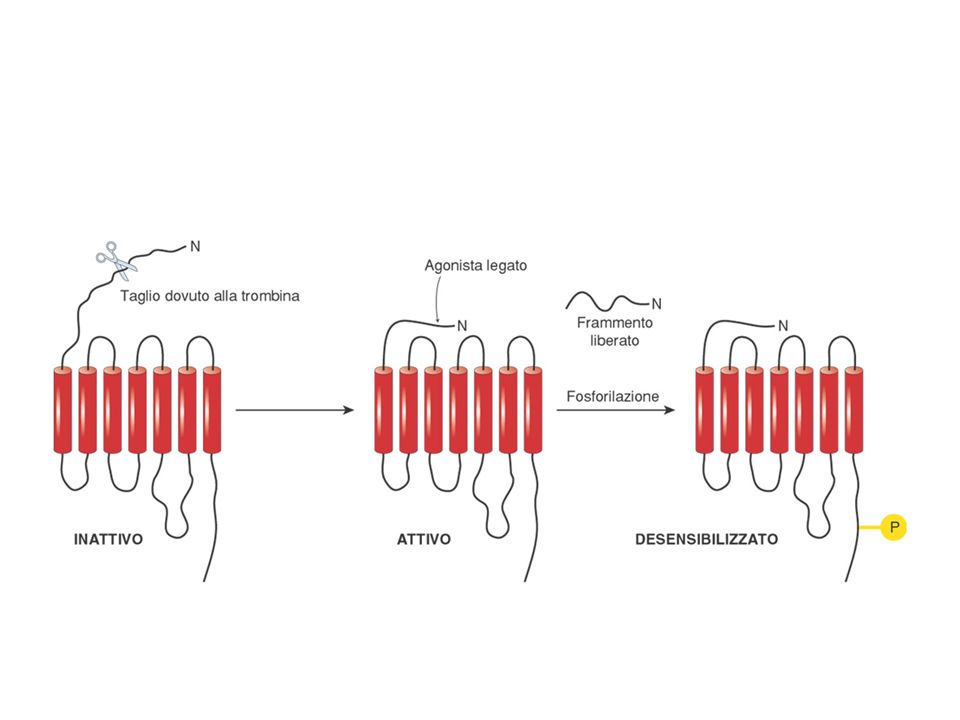
The connection between G-protein-coupled protease-activated receptors and ADP. Protease-activated receptor 1 (PAR1) is the principal receptor responsible for the effects of thrombin, although PAR4 also has a role in response to thrombin. Thrombin binds to PAR1, which leads to PAR cleavage and secretion of ADP, which can then bind to the P2Y receptors. Pepducins are peptides that are able to penetrate cell membranes and disrupt PAR signalling to G proteins, thus inhibiting thrombin-mediated platelet aggregation.
 is the principal receptor responsible for the effects of thrombin, although PAR4 also has a role in response to thrombin. Thrombin binds to PAR1, which leads to PAR cleavage and secretion of ADP, which can then bind to the P2Y receptors. Pepducins are peptides that are able to penetrate cell membranes and disrupt PAR signalling to G proteins, thus inhibiting thrombin-mediated platelet aggregation..")
24
Coagulation cascade. The coagulation cascade is arbitrarily dividedw into the intrinsic pathway, the extrinsic pathway and the common pathway. The extrinsic AND INTRINSIC PATHWAYS CONVERGE AT THE LEVEL OF FACTOR X ACTIVATION. The intrinsic pathway is largely an in vitro pathway, while the extrinsic pathway accounts for the majority of in vivo coagulation. The extrinsic pathway is initiated at sites of vascular injury by the expression of the tissue factor on several different cell types, including activated endothelial cells, activated leukocytes, subendothelial vascular smooth muscle cells and subendothelial fibroblasts. Note that Ca2+ is a cofactor in many of the steps, and that a number of the steps occur on pospholipid surfaces provided by activated platelets, activated endothelial cells and activated monocytes.

25
Superficie organizzatrice
Per ogni passaggio della coagulazione: Proteasi dal passaggio precedente Ca2+ Cofattore proteico zimogeno Superficie organizzatrice

26
Coagulation factor activation on phospholipid surfaces
Coagulation factor activation on phospholipid surfaces. Surface catalysis is critical for a number of the activation reactions in the coagulation cascade. Each activation reaction consistes of an enzyme (e.g. afctor IXa), a substrate (e.g. factor X), and a cofactor or rection accelerator (e.g. factor VIIIa), all f which are assembled on the phospholipid surface of activated platelets or endothelial cells. Ca 2+ allows the enzyme and substrate to adopt the propr conformation in each activation reaction. In the example shown, factor VIIIa and Ca2+ act as cofactors in the factor IXa-meduiated cleavage to factor Xa. Factor Va and Ca2+ then act as cofactors in the factor Xa.-mediated cleavage of prothrombin to thrombin.
, a substrate (e.g. factor X), and a cofactor or rection accelerator (e.g. factor VIIIa), all f which are assembled on the phospholipid surface of activated platelets or endothelial cells. Ca 2+ allows the enzyme and substrate to adopt the propr conformation in each activation reaction. In the example shown, factor VIIIa and Ca2+ act as cofactors in the factor IXa-meduiated cleavage to factor Xa. Factor Va and Ca2+ then act as cofactors in the factor Xa.-mediated cleavage of prothrombin to thrombin.")
27
MECCANISMI CHE LIMITANO LA PROPAGAZIONE DEL PROCESSO EMOSTATICO
Produzione di PGI2 da parte dell’endotelio intatto Antitrombina III

28
ANTI-COAGULANTI NATURALI

29
Similarities and differences between heparan sulphate and heparin
Similarities and differences between heparan sulphate and heparin. a | Heparan sulphate. b | Heparin. Both heparan sulphate and heparin consist of alternating units of glucosamine (GlcN) with glucuronic acid (GlcA) or iduronic acid (IdoA). Heparan sulphate contains a greater proportion of GlcA, whereas heparin contains more IdoA. Both molecules are sulphated (illustrated here by blue circles), heparin more extensively so, which provides a high degree of electronegativity. Heparan-sulphate glycosaminoglycan (GAG) chains tend to exist as proteoglycan components — that is, tethered to a protein core. In this way, they are expressed on the surfaces of cells, including those of the vascular endothelium and of circulating leukocytes, which provides a general net negative charge to these surfaces (depicted by white circles). Heparin, by contrast, is co-released with histamine from degranulating mast cells, and can dissociate from its protein core to exist as free GAG chains.
 with glucuronic acid (GlcA) or iduronic acid (IdoA). Heparan sulphate contains a greater proportion of GlcA, whereas heparin contains more IdoA. Both molecules are sulphated (illustrated here by blue circles), heparin more extensively so, which provides a high degree of electronegativity. Heparan-sulphate glycosaminoglycan (GAG) chains tend to exist as proteoglycan components — that is, tethered to a protein core. In this way, they are expressed on the surfaces of cells, including those of the vascular endothelium and of circulating leukocytes, which provides a general net negative charge to these surfaces (depicted by white circles). Heparin, by contrast, is co-released with histamine from degranulating mast cells, and can dissociate from its protein core to exist as free GAG chains.")
31
Antithrombin III action
Antithrombin III action. Antothrombin III inactivates thrombin and factors IXa, Xa, XIa and XIIa by forming a stoichionmetric complex with these coagulation factors. These reactions are catalyzed physiologically by heparin-like molecules expressed on healthy endothelial cells; sites of vascular injury do not express heparin-like molecules beacuse the endothelium is denuded or damaged. Pharmacologically, these reactions are catalyzed by exogenously administered heparin. In more detail, the binding of heparin to ATIII induces a conformational cahnge in ATIII (A) that allows the ATIII to bind thrombin or coagulation factors IXa, Xa, XIa, or XIIa. The stoichiometric complex betweenATII and the coagulation factor is highly stable, allowing heparin to dissociate without breaking up the complex. In this way, heparin serves as a true catalyst for the inactivation reaction (B)
 that allows the ATIII to bind thrombin or coagulation factors IXa, Xa, XIa, or XIIa. The stoichiometric complex betweenATII and the coagulation factor is highly stable, allowing heparin to dissociate without breaking up the complex. In this way, heparin serves as a true catalyst for the inactivation reaction (B)")
32
MECCANISMI CHE LIMITANO LA PROPAGAZIONE DEL PROCESSO EMOSTATICO
Produzione di PGI2 da parte dell’endotelio intatto Antitrombina III Proteina C/Proteina S

33
ANTI-COAGULANTI NATURALI

34
MECCANISMI CHE LIMITANO LA PROPAGAZIONE DEL PROCESSO EMOSTATICO
Prooduzione di PGI2 da parte dell’endotelio intatto Antitrombina III Proteina C/Proteina S Inibitore del percorso del fattore tessutale (TFPI)
")
35
ANTI-COAGULANTI NATURALI

36
MECCANISMI CHE LIMITANO LA PROPAGAZIONE DEL PROCESSO EMOSTATICO
Produzione di PGI2 da parte dell’endotelio intatto Antitrombina III Proteina C/Proteina S Inibitore del percorso del fattore tessutale (TFPI) Attivatore tessutale del plasminogeno (tPA)
 Attivatore tessutale del plasminogeno (tPA)")
37
Antithrombin III action
Antithrombin III action. Antothrombin III inactivates thrombin and factors IXa, Xa, XIa and XIIa by forming a stoichionmetric complex with these coagulation factors. These reactions are catalyzed physiologically by heparin-like molecules expressed on healthy endothelial cells; sites of vascular injury do not express heparin-like molecules beacuse the endothelium is denuded or damaged. Pharmacologically, these reactions are catalyzed by exogenously administered heparin. In more detail, the binding of heparin to ATIII induces a conformational cahnge in ATIII (A) that allows the ATIII to bind thrombin or coagulation factors IXa, Xa, XIa, or XIIa. The stoichiometric complex betweenATII and the coagulation factor is highly stable, allowing heparin to dissociate without breaking up the complex. In this way, heparin serves as a true catalys for the inactivation reaction (B)
 that allows the ATIII to bind thrombin or coagulation factors IXa, Xa, XIa, or XIIa. The stoichiometric complex betweenATII and the coagulation factor is highly stable, allowing heparin to dissociate without breaking up the complex. In this way, heparin serves as a true catalys for the inactivation reaction (B)")
38
Blood coagulation. A schematic representation of blood coagulation in which the central role of thrombin is outlined (for details see Refs 14,15). Initiation: tissue factor (TF) is exposed by vessel damage; coagulation factor VIIa (FVIIa) binds to TF and activates small amounts of FX to FXa and FIX to FIXa. This leads to trace amounts of thrombin. Amplification: the trace amounts of thrombin activate the co-factors FV and FVIII to FVa and FVIIIa and platelets (via cleavage of protease-activated receptors, PAR1 and PAR4), which leads to the formation of complexes of factors for more efficient thrombin generation. Propagation: more thrombin is available leading to activation of FXI (to FXIa) for more thrombin generation, fibrin formation, activation of FXIII (to FXIIIa) to reinforce the fibrin structure and activation of thrombin activatable fibrinolysis inhibitor (TAFI) for prevention of fibrinolysis. Termination: thrombin leaking out of the clotting area activates protein C (to APC), which inactivates FVa and FVIIIa. This is important because it restricts the blood coagulation to the area of vessel damage. Amber arrows: direct effects of thrombin; green arrows: indirect effects of thrombin that stimulate plasma coagulation and platelet aggregation; red arrows: indirect effects of thrombin that inhibit plasma coagulation and fibrinolysis.
. Initiation: tissue factor (TF) is exposed by vessel damage; coagulation factor VIIa (FVIIa) binds to TF and activates small amounts of FX to FXa and FIX to FIXa. This leads to trace amounts of thrombin. Amplification: the trace amounts of thrombin activate the co-factors FV and FVIII to FVa and FVIIIa and platelets (via cleavage of protease-activated receptors, PAR1 and PAR4), which leads to the formation of complexes of factors for more efficient thrombin generation. Propagation: more thrombin is available leading to activation of FXI (to FXIa) for more thrombin generation, fibrin formation, activation of FXIII (to FXIIIa) to reinforce the fibrin structure and activation of thrombin activatable fibrinolysis inhibitor (TAFI) for prevention of fibrinolysis. Termination: thrombin leaking out of the clotting area activates protein C (to APC), which inactivates FVa and FVIIIa. This is important because it restricts the blood coagulation to the area of vessel damage. Amber arrows: direct effects of thrombin; green arrows: indirect effects of thrombin that stimulate plasma coagulation and platelet aggregation; red arrows: indirect effects of thrombin that inhibit plasma coagulation and fibrinolysis..")
40
Positive and negative effects of heparin anticoagulant therapy
Positive and negative effects of heparin anticoagulant therapy. a | Heparin modulates blood coagulation through inhibition of the serine-protease factors XIIa, XIa, Xa, IXa and IIa (thrombin), either directly, or through potentiation of the plasma serine-protease inhibitor antithrombin. Heparin also inhibits platelet activation, an effect that is, in part, secondary to it binding to thrombin, a potent platelet-activating substance. b | A considerable percentage of patients receiving heparin therapy go on to develop the serious adverse reaction of heparin-induced thrombocytopaenia type 2. This arises when antibodies are raised against a complex of heparin and platelet factor 4 (PF4). Subsequent binding of platelet-surface PF4 by heparin results in immune-mediated platelet activation and possible thrombosis. Therefore, heparin chains with insufficient length to bind PF4 are considered to be less immunogenic. V, factor V; VIII, factor VIII; vWF, von Willebrand factor.
, either directly, or through potentiation of the plasma serine-protease inhibitor antithrombin. Heparin also inhibits platelet activation, an effect that is, in part, secondary to it binding to thrombin, a potent platelet-activating substance. b | A considerable percentage of patients receiving heparin therapy go on to develop the serious adverse reaction of heparin-induced thrombocytopaenia type 2. This arises when antibodies are raised against a complex of heparin and platelet factor 4 (PF4). Subsequent binding of platelet-surface PF4 by heparin results in immune-mediated platelet activation and possible thrombosis. Therefore, heparin chains with insufficient length to bind PF4 are considered to be less immunogenic. V, factor V; VIII, factor VIII; vWF, von Willebrand factor.")
45
SVANTAGGI DELLA TERAPIA CON ANTICOAGULANTI ORALI
Interazioni con altri farmaci e con componenti della dieta Finestra terapeutica ristretta Lenta insorgenza e reversione degli effetti

46
FATTORI CHE POTENZIANO L’AZIONE DEGLI
ANTICOAGULANTI ORALI Malattie Malattie epatiche Condizioni che aumentano il metabolismo Farmaci Farmaci che inibiscono il metabolismo epatico Farmaci che inibiscono la funzionalità piastrinica Farmaci che spiazzano gli OA dal legame con le proteine Farmaci che diminuiscono la riduzione della vitamina K Farmaci che diminuiscono la disponibilità di vitamina K

47
FATTORI CHE RIDUCONO L’AZIONE DEGLI
ANTICOAGULANTI ORALI Malattie Gravidanza Ipotiroidismo Farmaci Vitamina K Farmaci che inducono il metabolismo epatico Farmaci che diminuiscono l’assorbimento intestinale

48
ANTICOAGULANTI INDIPENDENTI DA ANTITROMBINA III
Irudina Irugeno Argatroban PPACK (tripeptide clorometilchetone)
")
50
Current repertoire of clinically evaluated anticoagulants
Current repertoire of clinically evaluated anticoagulants. Org42675 displays a distinct pharmacological profile among the current repertoire of clinically evaluated anticoagulants, including UFH, LMWH, direct thrombin inhibitors and warfarin. The direct inhibitors of fXa are currently in clinical Phase II. The potent and selective dual inhibitor Org42675 inhibits several essential targets in the coagulation cascade, with potential application in the prevention and effective treatment of thrombosis with a low hemorrhagic risk. Abbreviation: UFH, unfractionated heparin.

51
* * anisoylated plasminogen streptokinase activator complex (APSAC)
")
Presentazioni simili