Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Università degli Studi di Padova Clinica Psichiatrica
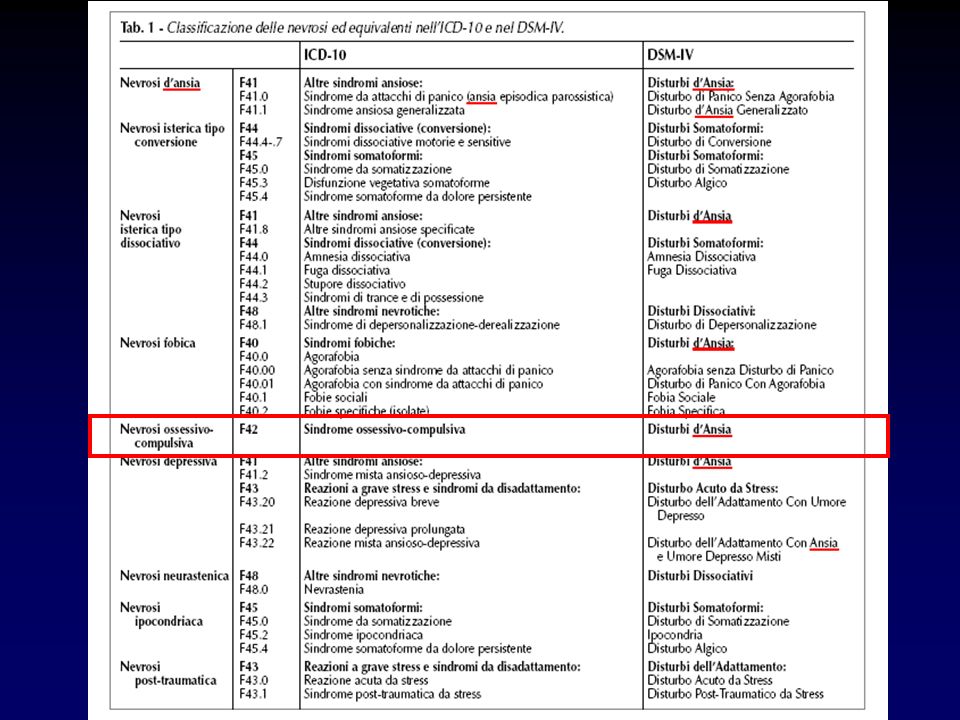
Dipartimento di Neuroscienze Giulia Perini Il disturbo Ossessivo-Compulsivo (OCD) nel DSM-IV-TR e nell’ICD-10
 nel DSM-IV-TR e nell’ICD-10.")
3
OCD Freud DSM-III Nevrosi Disturbi d’ansia ICD-10 DSM-IV
OCD rimane stabile come entità nosografica nella evoluzione delle classificazioni in psichiatria Con una prevalenza lifetime dall1.9 al 3.3%

4
F42.0 Predominantly obsessional thoughts or ruminations
International Classification of Diseases 10th Revision (ICD-10) Mental and behavioural disorders 1. Neurotic, stress-related and somatoform disorders (F40-F48) F42 Obsessive-compulsive disorder F42.0 Predominantly obsessional thoughts or ruminations F42.1 Predominantly compulsive acts (obsessional rituals) F42.2 Mixed obsessional thoughts and acts F42.8 Other obsessive-compulsive disorders F42.9 Obsessive-compulsive disorder, unspecified
 Mental and behavioural disorders. 1. Neurotic, stress-related and somatoform disorders (F40-F48) F42 Obsessive-compulsive disorder. F42.0 Predominantly obsessional thoughts or ruminations. F42.1 Predominantly compulsive acts (obsessional rituals) F42.2 Mixed obsessional thoughts and acts. F42.8 Other obsessive-compulsive disorders. F42.9 Obsessive-compulsive disorder, unspecified.")
5
2. Disorders of adult personality and behaviour (F60-F69)
International Classification of Diseases 10th Revision (ICD-10) Mental and behavioural disorders 2. Disorders of adult personality and behaviour (F60-F69) F60.5 Anankastic personality disorder Excludes: obsessive-compulsive disorder ( F42.- )
 Mental and behavioural disorders. 2. Disorders of adult personality and behaviour (F60-F69) F60.5 Anankastic personality disorder. Excludes: obsessive-compulsive disorder ( F42.- )")
6
OCD nell’ICD-10 F42.0 Predominanti pensieri ossessivi
Possono prendere la forma di idee, immagini mentali o impulsi all’azione, che sono sempre disturbanti per il paziente A volte le idee riguardano la considerazione senza fine e dubitante di alternative, associata all’incapacità di prendere le più banali ma necessarie decisioni della vita di tutti i giorni. A volte la relazione fra ossessioni ruminative e depressione è molto stretta e la diagnosi di DOC dovrebbe farsi solo se le ruminazioni nascono e persistono in assenza di un episodio depressivo.

7
OCD nell’ICD-10 F42.1 Predominanti azioni compulsive (rituali ossessivi) La maggior parte delle compulsioni riguardano la pulizia (particolarmente il lavaggio delle mani), il controllo ripetuto per assicurarsi che una potenziale situazione pericolosa non si verifichi e l’ordine o simmetria. Sottostante al comportamento espresso apertamente c’è una paura, usualmente di pericolo per il paziente o causato dal paziente e il rituale è un inefficace o simbolico tentativo di scongiurare quel determinato pericolo prevenire quel pericolo
, il controllo ripetuto per assicurarsi che una potenziale situazione pericolosa non si verifichi e l’ordine o simmetria. Sottostante al comportamento espresso apertamente c’è una paura, usualmente di pericolo per il paziente o causato dal paziente e il rituale è un inefficace o simbolico tentativo di scongiurare quel determinato pericolo prevenire quel pericolo.")
8
OCD nell’ICD-10 Obsessive-compulsive disorder
The essential feature is recurrent obsessional thoughts or compulsive acts. Obsessional thoughts are ideas, images, or impulses that enter the patient's mind again and again in a stereotyped form. They are almost invariably distressing and the patient often tries, unsuccessfully, to resist them. They are, however, recognized as his or her own thoughts, even though they are involuntary and often repugnant. Compulsive acts or rituals are stereotyped behaviours that are repeated again and again. They are not inherently enjoyable, nor do they result in the completion of inherently useful tasks. Their function is to prevent some objectively unlikely event, often involving harm to or caused by the patient, which he or she fears might otherwise occur. Usually, this behaviour is recognized by the patient as pointless or ineffectual and repeated attempts are made to resist. Anxiety is almost invariably present. If compulsive acts are resisted the anxiety gets worse. Includes: anankastic neurosis obsessive-compulsive neurosis Excludes: obsessive-compulsive personality (disorder) ( F60.5
 ( F60.5.")
9
OCD nel DSM-IV-TR

10
OCD nel DSM-IV-TR

11
OCD nel DSM-IV-TR

12
OCD in DSM-IV-TR

13
Obsessive-Compulsive Personality Disorders in ICD-10
F60.5 Disturbo di personalità anancastico: Disturbo di personalità caratterizzato da sentimenti di dubbio, perfezionismo, eccessiva coscienziosità, controllo e preoccupazione per i dettagli, testardaggine, cautela e rigidità. Possono esserci pensieri o impulsi insistenti e indesiderati che non raggiungono la severità di un DOC. Disturbo di personalità: · compulsivo · ossessivo · Ossessivo-compulsivo

14
Disturbo Ossessivo-Compulsivo di Personalità nel DSM-IV
Precede il DOC In circa il 50% Più frequente antecedente del DOC che della MD e del DAP

15
Aree di sovrapposizione fra ICD-10 e DSM-IV
In entrambe le classificazioni il DOC è una entità nosografica autonoma e ben distinta dalle altre Il quadro descrittivo è sostanzialmente sovrapponibile per le ossessioni e le compulsioni Vi è in entrambe le classificazioni un corrispondente disturbo di personalità

16
Differenze fra ICD-10 e DSM-IV
Nell’ICD-10 il DOC è inserito nella categoria delle nevrosi insieme ai disturbi d’ansia, da stress e somatoformi Nel DSM-IV è inserito nella classificazione fra i disturbi d’ansia Criterio Funzionale presente nel DSM-IV assente nell’ICD-10 Il disturbo di personalità considerato alternativo per ICD-10, non per il DSM-IV

17
OCD tra ICD-10 e DSM-IV verso il DSM-V
Questioni aperte Il DOC è un disturbo d’ansia (o una nevrosi?) e come tale lo si deve mantenere anche nel DSM-V? Il DOC appartiene a uno spettro specifico, lo spettro DOC e, se si, quali altri disturbi appartengono allo spettro?
 e come tale lo si deve mantenere anche nel DSM-V Il DOC appartiene a uno spettro specifico, lo spettro DOC e, se si, quali altri disturbi appartengono allo spettro")
18
L’OCD è un disturbo d’ansia (o una nevrosi
L’OCD è un disturbo d’ansia (o una nevrosi?) e come tale lo si deve mantenere anche nel DSM-V?
 e come tale lo si deve mantenere anche nel DSM-V")
19
Se è un disturbo d’ansia
Se è un disturbo nello spettro ossessivo-compulsivo Quali sono i dati epidemiologici (comorbidità, familiarità) e neurobiologici e di trattamento che supportano una o l’altra classificazione
 e neurobiologici e di trattamento che supportano una o l’altra classificazione.")
20
OCD come disturbo d’ansia?
L’OCD è caratterizzato come disturbo d’ansia per il ruolo centrale che l’ansia ha nel disturbo L’Ansia come correlato soggettivo delle ossessioni e come motore delle compulsioni L’Evitamento delle situazioni che stimolano le ossessioni e le compulsioni frequente nell’OCD APPROCCIO FOCALIZZATO SUI SINTOMI L’Ansia però è un costrutto Transnosografico (depressione, disturbi bipolari, schizofrenia)
")
21
OCD è un disturbo d’ansia?
Studi sulla Comorbidità Studi sulle Famiglie Neurocircuiti Neurotrasmissione e Risposta al Trattamento

22
Comorbidità DOC e Disturbi d’ansia
La depressione maggiore è in realtà il disturbo in comorbidità più frequente nel DOC (54-66% lifetime) Fra i disturbi d’ansia il più frequente è la fobia sociale (23-36%) Il rischio di depressione è stimato essere 10 volte superiore a quello nella popolazione generale La relazione TEMPORALE indica che OCD precede non segue la depressione nella maggior parte dei casi e quindi la depressione è un evoluzione negativa nel decorso DOC LaSalle, 2004, Denys, 2004 LA SALLE SU 334 PAZIENTI
 Fra i disturbi d’ansia il più frequente è la fobia sociale (23-36%) Il rischio di depressione è stimato essere 10 volte superiore. a quello nella popolazione generale. La relazione TEMPORALE indica che OCD precede non segue la depressione nella maggior parte dei casi e quindi la depressione è un evoluzione negativa nel decorso DOC LaSalle, 2004, Denys, LA SALLE SU 334 PAZIENTI.")
23
Comorbidità OCD e disturbi dello spettro OCD (sOCD)
Poiché sono disturbi rari nella popolazione non ci sono dati sul maggior rischio di SOCD rispetto lla popolazione generale negli OCD Gli OCD hanno più spesso in comorbidità Ipocondria, Disturbo Dismorfofobico, Tricotillomania e Compulsione patologica all’acquisto I disturbi dell’alimentazione 8X più frequenti nei DOC Bambini con Tourette Syndrome (TS) hanno OCD nel 50% dei casi, + un 8% lo sviluppa in corso di malattia .
 hanno OCD nel 50% dei casi, + un 8% lo sviluppa in corso di malattia .")
24
Studi sulle Famiglie OCD e Disturbi d’ansia: non dati conclusivi
Lo studio Johns Hopkins OCD Family Study (Nestad 2001) ha trovato che nei familiari di OCD, senza OCD, i disturbi più frequenti erano GAD e AGORAFOBIA, quelli con OCD avevano più MDD, ansia di separazione e panico Ipotesi: Un fattore familiare favorente l’OCD è l’essere apprensivi, ansiosi o evitanti mentre Depressione e panico sono secondari (?) 80 casi OCD Familiari 73 CT Controlli
 ha trovato che nei familiari di OCD, senza OCD, i disturbi più frequenti erano GAD e AGORAFOBIA, quelli con OCD avevano più MDD, ansia di separazione e panico. Ipotesi: Un fattore familiare favorente l’OCD è l’essere apprensivi, ansiosi o evitanti mentre Depressione e panico sono secondari ( ) 80 casi OCD 343 Familiari. 73 CT 300 Controlli.")
25
Studi sulle Famiglie OCD e Disturbi dello spettro OCD (sOCD)
Il Johns Hopkins OCD Family Study (Bienveu, 2000) ha trovato che alcuni sOCD- Ipocondria, Disturbo Dismorfofobico, Tricotillomania erano più frequenti nei familiari degli OCD, indipendentemente dall’avere o no l’OCD. Altri sOCD (anoressia/bulimia e disturbi del controllo degli impulsi) in questo studio non erano più frequenti nei familiari OCD Altri studi hanno mostrato che partendo dai disturbi dell’alimentazione si trova una elevata aggregazione familiare con OCD e sOCD (tic) (Bellodi, 2001) o l’OCDP (Lilenfeld,1998) Infine gli sOCD di tipo neurologico – Tourette e disturbi da tic- sono più frequenti nei parenti di OCD (Grados, 2001) e i familiari di bambini autistici con comportamenti ripetitivi hanno più spesso un DOC rispetto a quelli senza comportamenti ripetitivi
 ha trovato che alcuni sOCD- Ipocondria, Disturbo Dismorfofobico, Tricotillomania erano più frequenti nei familiari degli OCD, indipendentemente dall’avere o no l’OCD. Altri sOCD (anoressia/bulimia e disturbi del controllo degli impulsi) in questo studio non erano più frequenti nei familiari OCD. Altri studi hanno mostrato che partendo dai disturbi dell’alimentazione si trova una elevata aggregazione familiare con OCD e sOCD (tic) (Bellodi, 2001) o l’OCDP (Lilenfeld,1998) Infine gli sOCD di tipo neurologico – Tourette e disturbi da tic- sono più frequenti nei parenti di OCD (Grados, 2001) e i familiari di bambini autistici con comportamenti ripetitivi hanno più spesso un DOC rispetto a quelli senza comportamenti ripetitivi.")
26
Neurocircuiti dell’OCD diversi da quelli nell’ansia

27
Circuiti dell’ANSIA Corteccia associativa Insula
Corteccia somatosensoriale “Long Loop” “Short Loop”

28
Le vie neurali della Paura Condizionata
Stimolo condizionato Stimolo aversivo non condizionato Stimolo Condizionato La risposta condizionata di allarme è una forma di apprendimento nel quale uno stimolo condizionato (SC) acquisisce la capacità di elicitare una serie di risposte comportamentali autonomiche comportamentali ed endocrine se associato ad uno stimolo negativo Lo stimolo condizionato può essere esplicito (rumore) oppure un contesto nel quale avviene un condizionamento. Il condizionamento viene acquisito rapidamente e mantenuto a lungo. La paura condizionata richiede la capacità di distinguere segnali di pericolo e segnali di sicurezza in modo corretto : attacchi di Panico, fobia sociale e PTSD non hanno questa capacità CG= CENTRAL GRAY LH= LATERAL HYPOTHALAMUS PVN= PARAVENTRICULAR NUCLEUS LA= AMIGDALA LATERALE CA= AMIGDALA CENTRALE
 acquisisce la capacità di elicitare una serie di risposte comportamentali autonomiche comportamentali ed endocrine se associato ad uno stimolo negativo. Lo stimolo condizionato può essere esplicito (rumore) oppure un contesto nel quale avviene un condizionamento. Il condizionamento viene acquisito rapidamente e mantenuto a lungo. La paura condizionata richiede la capacità di distinguere segnali di pericolo e segnali di sicurezza in modo corretto : attacchi di Panico, fobia sociale e PTSD non hanno questa capacità. CG= CENTRAL GRAY. LH= LATERAL HYPOTHALAMUS. PVN= PARAVENTRICULAR NUCLEUS. LA= AMIGDALA LATERALE. CA= AMIGDALA CENTRALE.")
29
L’anatomia dell’estinzione della paura
+ - Nell’uomo la paura situazionale è appresa durante eventi traumatici con stimoli minacciosi e è aumentata dalla predisposizione genetica Normalmente le situazioni di pericolo vengono regolarment incontrate nell’ambiente quotidiano ma anche affrontate e dimenticate. Tuttavia quando le situazioni sono troppo paurose o il sistema neurale funziona in maniera subottimale le paure vengono apprese ma non dimenticate creando quindi forme di ansia (PTSD, GAD, DAP) Numerosi dati preclinici mostrano che l’amigdala è il cuore dei circuiti per la formazione e l’estinzione della paura condizionata
 Numerosi dati preclinici mostrano che l’amigdala è il cuore dei circuiti per la formazione e l’estinzione della paura condizionata.")
30
Neurocircuiti OCD e Ansia
I neurocircuiti dell’OCD sono diversi da quelli dell’ansia, interessano cioè i Circuiti fronto-striatali, mentre l’amigdala è centrale nella neurobiologia dell’ansia Recentemente ci sono però evidenze di una parziale interessamento crociato dei neurocircuiti dell’OCD e dell’ansia (fobie e GAD): nel DOC vi può essere un interessamento dell’amigdala in associazione all’ansia, nelle fobie e GAD un interessamento della corteccia OFC
: nel DOC vi può essere un interessamento dell’amigdala in associazione all’ansia, nelle fobie e GAD un interessamento della corteccia OFC.")
31
Dissezione farmacologica Neurotrasmissione e Trattamento
I principali Neurotrasmettitori interessati nell’OCD e nei disturbi dello spettro OCD sono la Serotonina(SE) e la Dopamina (DA), insieme all’ossitocina in alcuni sottogruppi diagnostici. Nei Disturbi d’ansia i neurotrasmettitori implicati sono molteplici e profili diversi sono presenti per ciascun tipo di disturbo ( PTSD- HPA, Ne e Se; Panico - SE, NE, HPA, Neurosteroidi, CCK; Fobia Sociale - DA e SE, GAD- GABA e SE) OCD e sOCD rispondono bene agli SSRI e, in alcuni sottogruppi (TIC, Tricotillomania, ) agli antipsicotici ma non alle BZD
 e la Dopamina (DA), insieme all’ossitocina in alcuni sottogruppi diagnostici. Nei Disturbi d’ansia i neurotrasmettitori implicati sono molteplici e profili diversi sono presenti per ciascun tipo di disturbo ( PTSD- HPA, Ne e Se; Panico - SE, NE, HPA, Neurosteroidi, CCK; Fobia Sociale - DA e SE, GAD- GABA e SE) OCD e sOCD rispondono bene agli SSRI e, in alcuni sottogruppi (TIC, Tricotillomania, ) agli antipsicotici ma non alle BZD.")
32
2.Il DOC appartiene a uno spettro specifico, lo spettro DOC e, se si, quali altri disturbi appartengono allo spettro?

33
Disturbo dismorfofobico
Tricotillomania Tic disorders Ipocondria Am.J Psych. September 2007

34
OCD disturbo centrale dello spettro OCD

35
Disturbi del Continuum OCD nel DSM-IV
Disturbi dello spettro OCD ristretto attualmente considerati DISTURBI DEL CONTROLLO DEGLI IMPULSI (TRICOTILLOMANIA) Disturbi associati a PREOCCUPAZIONI CORPOREE (DISTURBO DISMORFOFOBICO; IPOCONDRIA DISTURBI NEUROLOGICI (TOURETTE, PANDAS)
 Disturbi associati a PREOCCUPAZIONI CORPOREE (DISTURBO DISMORFOFOBICO; IPOCONDRIA. DISTURBI NEUROLOGICI (TOURETTE, PANDAS)")
36
ICD-10 Habit and impulse disorders
F63 Habit and impulse disorders This category includes certain disorders of behaviour that are not classifiable under other categories. They are characterized by repeated acts that have no clear rational motivation, cannot be controlled, and generally harm the patient's own interests and those of other people. The patient reports that the behaviour is associated with impulses to action. The cause of these disorders is not understood and they are grouped together because of broad descriptive similarities, not because they are known to share any other important features. Excludes: habitual excessive use of alcohol or psychoactive substances ( F10-F19 ) impulse and habit disorders involving sexual behaviour ( F65.- )
 impulse and habit disorders involving sexual behaviour ( F65.- )")
37
Habit and impulse disorders
F63.0 Pathological gambling The disorder consists of frequent, repeated episodes of gambling that dominate the patient's life to the detriment of social, occupational, material, and family values and commitments. Compulsive gambling Excludes: excessive gambling by manic patients ( F30.- ) gambling and betting NOS ( Z72.6 ) gambling in dissocial personality disorder ( F60.2 ) F63.1 Pathological fire-setting [pyromania] Disorder characterized by multiple acts of, or attempts at, setting fire to property or other objects, without apparent motive, and by a persistent preoccupation with subjects related to fire and burning. This behaviour is often associated with feelings of increasing tension before the act, and intense excitement immediately afterwards. Excludes: fire-setting (by)(in): · adult with dissocial personality disorder ( F60.2 ) · alcohol or psychoactive substance intoxication ( F10-F19 , with common fourth character .0) · as the reason for observation for suspected mental disorder ( Z03.2 ) · conduct disorders ( F91.- ) · organic mental disorders ( F00-F09 ) · schizophrenia ( F20.- )
 gambling and betting NOS ( Z72.6 ) gambling in dissocial personality disorder ( F60.2 ) F63.1 Pathological fire-setting [pyromania] Disorder characterized by multiple acts of, or attempts at, setting fire to property or other objects, without apparent motive, and by a persistent preoccupation with subjects related to fire and burning. This behaviour is often associated with feelings of increasing tension before the act, and intense excitement immediately afterwards. Excludes: fire-setting (by)(in): · adult with dissocial personality disorder ( F60.2 ) · alcohol or psychoactive substance intoxication ( F10-F19 , with common fourth character .0) · as the reason for observation for suspected mental disorder ( Z03.2 ) · conduct disorders ( F91.- ) · organic mental disorders ( F00-F09 ) · schizophrenia ( F20.- )")
38
Disturbi del controllo degli impulsi non altrimenti classificati nel DSM-IV

39
Habit and impulse disorders
F63.2 Pathological stealing [kleptomania] Disorder characterized by repeated failure to resist impulses to steal objects that are not acquired for personal use or monetary gain. The objects may instead be discarded, given away, or hoarded. This behaviour is usually accompanied by an increasing sense of tension before, and a sense of gratification during and immediately after, the act. Excludes: depressive disorder with stealing ( F31-F33 ) organic mental disorders ( F00-F09 ) shoplifting as the reason for observation for suspected mental disorder ( Z03.2 ) F63.3 Trichotillomania A disorder characterized by noticeable hair-loss due to a recurrent failure to resist impulses to pull out hairs. The hair-pulling is usually preceded by mounting tension and is followed by a sense of relief or gratification. This diagnosis should not be made if there is a pre-existing inflammation of the skin, or if the hair-pulling is in response to a delusion or a hallucination. Excludes: stereotyped movement disorder with hair-plucking (F98.4)
 organic mental disorders ( F00-F09 ) shoplifting as the reason for observation for suspected mental disorder ( Z03.2 ) F63.3 Trichotillomania. A disorder characterized by noticeable hair-loss due to a recurrent failure to resist impulses to pull out hairs. The hair-pulling is usually preceded by mounting tension and is followed by a sense of relief or gratification. This diagnosis should not be made if there is a pre-existing inflammation of the skin, or if the hair-pulling is in response to a delusion or a hallucination. Excludes: stereotyped movement disorder with hair-plucking (F98.4)")
40
Tricotillomania nel DSM-IV

41
Habit and impulse disorders
F63.8 Other habit and impulse disorder Other kinds of persistently repeated maladaptive behaviour that are not secondary to a recognized psychiatric syndrome, and in which it appears that the patient is repeatedly failing to resist impulses to carry out the behaviour. There is a prodromal period of tension with a feeling of release at the time of the act. Intermittent explosive disorder F63.9 Habit and impulse disorder, unspecified

42
Disturbi dello spettro OCD Disturbi somatoformi

43
Disorders usually first diagnosed in infancy, childhood or adolescence: Tic disorders
F95 Tic disorders Syndromes in which the predominant manifestation is some form of tic. A tic is an involuntary, rapid, recurrent, nonrhythmic motor movement (usually involving circumscribed muscle groups) or vocal production that is of sudden onset and that serves no apparent purpose. Tics tend to be experienced as irresistible but usually they can be suppressed for varying periods of time, are exacerbated by stress, and disappear during sleep. Common simple motor tics include only eye-blinking, neck-jerking, shoulder- shrugging, and facial grimacing. Common simple vocal tics include throat-clearing, barking, sniffing, and hissing. Common complex tics include hitting oneself, jumping, and hopping. Common complex vocal tics include the repetition of particular words, and sometimes the use of socially unacceptable (often obscene) words (coprolalia), and the repetition of one's own sounds or words (palilalia). F95.0 Transient tic disorder Meets the general criteria for a tic disorder but the tics do not persist longer than 12 months. The tics usually take the form of eye-blinking, facial grimacing, or head-jerking. F95.1 Chronic motor or vocal tic disorder Meets the general criteria for a tic disorder, in which there are motor or vocal tics (but not both), that may be either single or multiple (but usually multiple), and last for more than a year.
 or vocal production that is of sudden onset and that serves no apparent purpose. Tics tend to be experienced as irresistible but usually they can be suppressed for varying periods of time, are exacerbated by stress, and disappear during sleep. Common simple motor tics include only eye-blinking, neck-jerking, shoulder- shrugging, and facial grimacing. Common simple vocal tics include throat-clearing, barking, sniffing, and hissing. Common complex tics include hitting oneself, jumping, and hopping. Common complex vocal tics include the repetition of particular words, and sometimes the use of socially unacceptable (often obscene) words (coprolalia), and the repetition of one s own sounds or words (palilalia). F95.0 Transient tic disorder Meets the general criteria for a tic disorder but the tics do not persist longer than 12 months. The tics usually take the form of eye-blinking, facial grimacing, or head-jerking. F95.1 Chronic motor or vocal tic disorder. Meets the general criteria for a tic disorder, in which there are motor or vocal tics (but not both), that may be either single or multiple (but usually multiple), and last for more than a year.")
44
Disturbo di Tourette nel DSM-IV

45
Tic disorders F95.2 Combined vocal and multiple motor tic disorder
[de la Tourette] A form of tic disorder in which there are, or have been, multiple motor tics and one or more vocal tics, although these need not have occurred concurrently. The disorder usually worsens during adolescence and tends to persist into adult life. The vocal tics are often multiple with explosive repetitive vocalizations, throat-clearing, and grunting, and there may be the use of obscene words or phrases. Sometimes there is associated gestural echopraxia which may also be of an obscene nature (copropraxia).
.")
46
CONCLUSIONI/ 1 Leckman ,2007)
")
47
CONCLUSIONI/ 2

48
ICD-10 DSM-IV DSM-V

Presentazioni simili











>")







