Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Strategie di induzione nel late presenter
Roma 11 marzo 2011 Prof. Massimo Andreoni Cattedra di Malattie Infettive Università Tor Vergata Roma

2
Induzione ?? 4 farmaci ?? Strategia di terapia antiretrovirale
CD4+ HIV-RNA copie/ml Quali pazienti potrebbero beneficiare di una induzione? <50 cp/ml RNA ??? Mesi di terapia Andreoni 11/2010

4
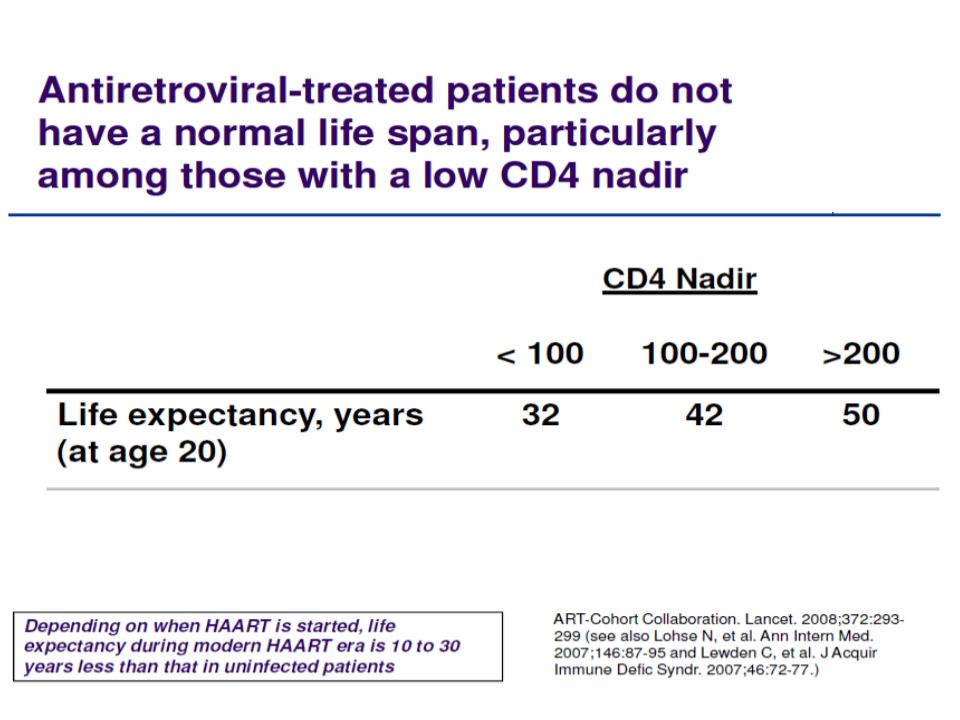
CASCADE: Nadir CD4 count predicts AIDS and non-AIDS events
CASCADE collaboration cohort (n = 9858) AIDS-related death Non-AIDS-related death Nadir CD4+ cell count 200–349 vs ≥ 350 200–349 vs ≥ 350 50–199 vs ≥ 350 50–199 vs ≥ 350 < 50 vs ≥ 350 < 50 vs ≥ 350 0.01 1.00 100.00 0.01 1.00 100.00 Liver disease death Non-AIDS cancer death 200–349 vs ≥ 350 200–349 vs ≥ 350 50–199 vs ≥ 350 50–199 vs ≥ 350 < 50 vs ≥ 350 < 50 vs ≥ 350 0.01 1.00 100.00 0.01 1.00 100.00 Marin et al. IAS Abstract WEPEB019
 AIDS-related death. Non-AIDS-related death. Nadir CD4+ cell count. 200–349 vs ≥ –349 vs ≥ –199 vs ≥ –199 vs ≥ 350. < 50 vs ≥ 350. < 50 vs ≥ Liver disease death. Non-AIDS cancer death. 200–349 vs ≥ –349 vs ≥ –199 vs ≥ –199 vs ≥ 350. < 50 vs ≥ 350. < 50 vs ≥ Marin et al. IAS Abstract WEPEB019.")
5
Guidelines

6
N Engl J Med 2003;349:

8
N Engl J Med 2003;349:

9
JAMA. 2006;296:

10
Gulick 2006

11
Gulick 2006

12
Gulick 2006

13
Gulick 2006

15
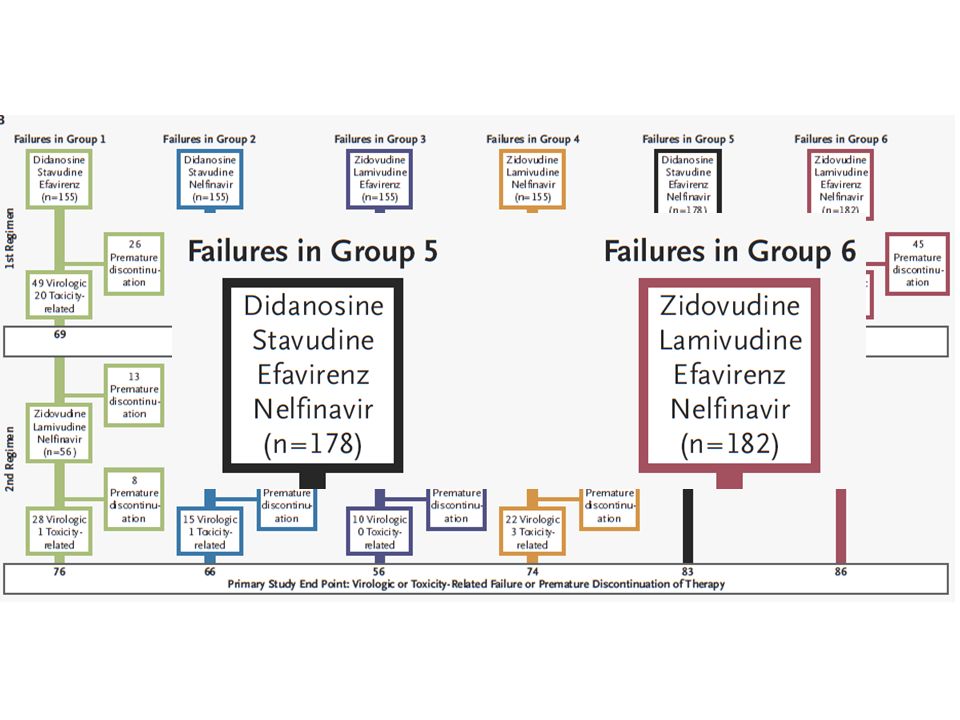
Sono queste le strategie che potremmo utilizzare oggi???
ACTG 384 DDI/d4T/EFV/NFV AZT/3TC/EFV/NFV ACTG 5095 AZT/3TC/ABC/EFV ma..... Sono queste le strategie che potremmo utilizzare oggi???

16
Considerations for First-line Therapy
Pt Factors Antiretroviral Drug Factors Readiness/commitment Baseline drug resistance Baseline CD4+ cell count/HIV-1 RNA Tolerability Age Long-term toxicity Sex Drug interactions Occupation Dosing frequency Comorbid conditions Pill burden Plans for pregnancy Pharmacokinetics Access to care Cost Concurrent medications Adherence to other medications This slide reviews patient‑ and drug-associated factors that might affect choice of first-line regimens. Most clinicians are familiar with these issues, but a patient’s occupation might be important or their ability to tolerate a high pill burden, dose frequency, or pharmacy cost. All of these factors need to be taken into consideration. 16

17
Adjusted risk of triple class virologic failure after the start of cART
Lodwick R, for COHERE, 16th CROI; Montreal (CA), 2009
,")
18
Boosted-PIs are associated with lower risk of HIV resistance at any level of adherence
* * *Plasma vira load log Lima VD et al, JID 2008 18 18

19
PI Efficacy at Higher and Lower Baseline HIV-1 RNA
Systematic review of 21 treatment arms from 12 treatment-naive clinical trials reported from January March 2008 (N = 4895) Conclusion: significantly ↑ rates of HIV-1 RNA < 50 copies/mL at 48 wks with TDF/FTC vs ABC/3TC by ITT-TLOVR or nearest equivalent endpoint LPV/RTV TDF (n = 1798) < 100,000 copies/mL ABC (n = 787) ≥ 100,000 copies/mL ATV/RTV TDF (n = 440) ABC (n = 433) FPV/RTV 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; DRV, darunavir; FPV, fosamprenavir; FTC, emtricitabine; ITT-TLOVR, intent-to-treat-time to loss of virologic response; LPV, lopinavir; RTV, ritonavir; TDF, tenofovir; VF, virologic failure. On the other hand, the data are not quite the same with boosted PIs. These data are from a presentation by Hill and colleagues at the 2008 joint Interscience Conference on Antimicrobial Agents and Chemotherapy/Infectious Diseases Society of America meeting. In this graph, individuals who had HIV-1 RNA < 100,000 copies/mL at baseline are represented by dark circles and patients who had HIV-1 RNA ≥ 100,000 copies/mL at baseline are represented by open circles. These are 48‑week data. For each boosted PI pair, regardless of whether patients received tenofovir or abacavir, a higher response rate was seen when HIV-1 RNA was < 100,000 copies/mL than when baseline HIV-1 RNA was ≥ 100,000 copies/mL. The clinical importance of this finding is not entirely clear, and although these are data from randomized studies, these are not randomized comparisons. However, it is helpful to keep in mind that at very high HIV-1 RNA levels, the pace of suppression to HIV-1 RNA < 50 copies/mL seems to be at a lower rate with the boosted PIs. TDF (n = 53) ABC (n = 756) DRV/RTV TDF (n = 343) 40 50 60 70 80 90 100 HIV-1 RNA < 50 copies/mL at 48 Wks (%) Hill A, et al. ICAAC/IDSA Abstract 1254. 1
 Conclusion: significantly ↑ rates of HIV-1 RNA < 50 copies/mL at 48 wks with TDF/FTC vs ABC/3TC by ITT-TLOVR or nearest equivalent endpoint. LPV/RTV. TDF (n = 1798) < 100,000 copies/mL. ABC (n = 787) ≥ 100,000 copies/mL. ATV/RTV. TDF (n = 440) ABC (n = 433) FPV/RTV. 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; DRV, darunavir; FPV, fosamprenavir; FTC, emtricitabine; ITT-TLOVR, intent-to-treat-time to loss of virologic response; LPV, lopinavir; RTV, ritonavir; TDF, tenofovir; VF, virologic failure. On the other hand, the data are not quite the same with boosted PIs. These data are from a presentation by Hill and colleagues at the 2008 joint Interscience Conference on Antimicrobial Agents and Chemotherapy/Infectious Diseases Society of America meeting. In this graph, individuals who had HIV-1 RNA < 100,000 copies/mL at baseline are represented by dark circles and patients who had HIV-1 RNA ≥ 100,000 copies/mL at baseline are represented by open circles. These are 48‑week data. For each boosted PI pair, regardless of whether patients received tenofovir or abacavir, a higher response rate was seen when HIV-1 RNA was < 100,000 copies/mL than when baseline HIV-1 RNA was ≥ 100,000 copies/mL. The clinical importance of this finding is not entirely clear, and although these are data from randomized studies, these are not randomized comparisons. However, it is helpful to keep in mind that at very high HIV-1 RNA levels, the pace of suppression to HIV-1 RNA < 50 copies/mL seems to be at a lower rate with the boosted PIs. TDF (n = 53) ABC (n = 756) DRV/RTV. TDF (n = 343) HIV-1 RNA < 50 copies/mL at 48 Wks (%) Hill A, et al. ICAAC/IDSA Abstract")
20
Emergenza di resistenza e ricombinazione virale
CD4 Viremia plasmatica Ricombinazione intracellulare del materiale genetico di HIV Giorni di HAART

22
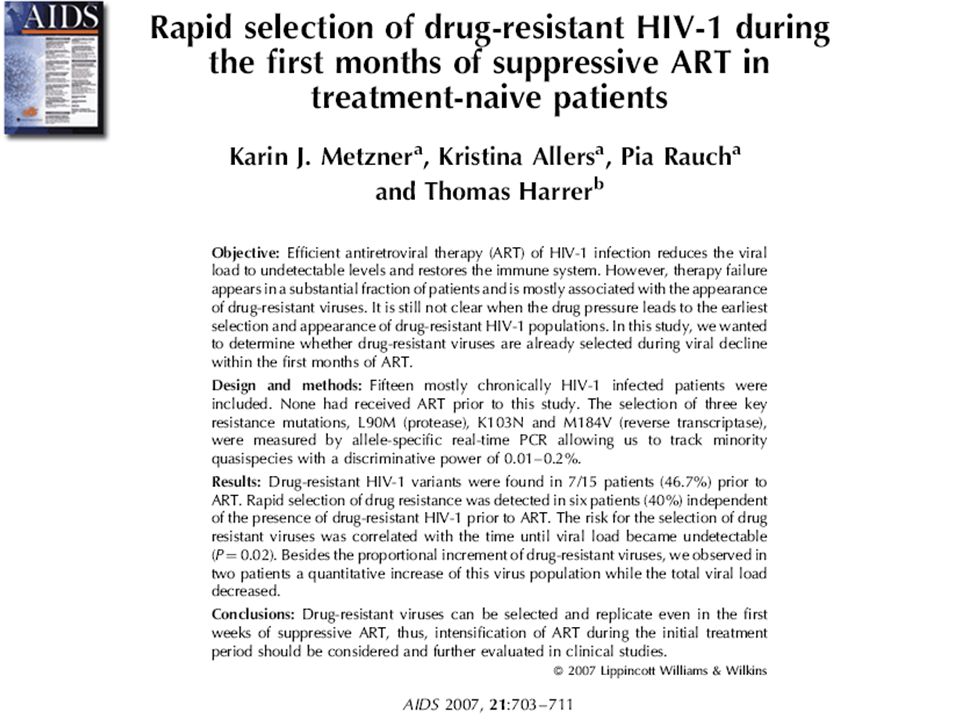
Viral load (RNA copies/ml plasma) Time after ART initiation (months)
Patient with detectable minority quasispecies of drug-resistant HIV-1 at baseline and selection of drug-resistant variants during initial months of 1st ART K103N variant (RNA copies/ml) Viral load (RNA copies/ml plasma) M184V variant (RNA copies/ml) Time after ART initiation (months)
 Viral load (RNA copies/ml plasma) M184V variant (RNA copies/ml) Time after ART initiation (months)")
23
Emergenza di resistenza e ricombinazione virale
CD4 Viremia plasmatica Ricombinazione intracellulare del materiale genetico di HIV Giorni di HAART

24
Decay of viral load with RTG vs. EFV in study P004
36 → 30 patients RTG 150→ 121 patients Murray, AIDS 2007 24

25
PROGRESS: Primary Efficacy Endpoint at Week 48:
LPV/r + RAL was non-inferior to LPV/r+TDF/FTC in treatment-naïve subjects at 48 weeks PROGRESS 48 week results – XVIII IAC 19-Jul-10

26
SPARTAN : Response Rate (HIV RNA < 50 c/mL) through Week 48 VR-OC
ATV+RAL ATV+RTV + TDF/FTC 100 n 82.2% n o n n n n o o n n 80 n n n o o o o 76.0% o 60 n o Percent Responders (95% CI) o 40 o n 20 o o o n B/L 4 8 12 16 20 24 28 32 36 40 44 48 Weeks ATV+RAL: N= ATV+RTV+TDF/FTC: N= VR-OC is an on-treatment method. It classifies subjects as responders according to a single on-treatment HIV RNA measurement < 50 c/mL closest to the planned visit and within a pre-defined visit window. The denominator is based on subjects with an on-treatment HIV RNA measurement in that visit window. IAC July 22, 2010: SPARTAN: THLBB204
 o. 40. o. n. 20. o. o. o. n. B/L Weeks. ATV+RAL: N= ATV+RTV+TDF/FTC: N= VR-OC is an on-treatment method. It classifies subjects as responders according to a single on-treatment HIV RNA. measurement < 50 c/mL closest to the planned visit and within a pre-defined visit window. The denominator is based. on subjects with an on-treatment HIV RNA measurement in that visit window. IAC July 22, 2010: SPARTAN: THLBB204.")
27
Mean CD4 change from baseline through week 48
ATV+RAL ATV+RTV + TDF/FTC o n 50 100 150 200 250 300 B/L 4 8 12 16 20 24 28 32 36 40 44 48 235 197 Mean CD4 Change cells/mm3 (SE) Weeks ATV+RAL: N= ATV+RTV+TDF/FTC: N= ATV+RAL: Mean CD4 change from baseline at week 24: 166 ATV/RTV + TDF/FTC: Mean CD4 change from baseline at week 24: 127 IAC July 22, 2010: SPARTAN: THLBB204 27
 Weeks. ATV+RAL: N= ATV+RTV+TDF/FTC: N= ATV+RAL: Mean CD4 change from baseline at week 24: 166. ATV/RTV + TDF/FTC: Mean CD4 change from baseline at week 24: 127. IAC July 22, 2010: SPARTAN: THLBB")
29
There was 6.4% of CXCR4-using HIV-1 in plasma during primary infection.
The HIV-1 RNA load and CD4+ T-cell count during primary infection were not related to virus tropism. Raymond S, 2010

30
In untreated patients with primary infection the detection of CXCR4-using virus was associated with an accelerated rate of disease progression Raymond S, 2010

32
CXCR4-specific viral load predicts disease progression during ART
Kaplan–Meier curves of the association of clinical progression with quantity of X4 and R5 (QXR) at baseline of 1 ( ) and < 1 ( ) Weiser B, AIDS 2008
 at baseline of 1 ( ) and < 1 ( ) Weiser B, AIDS")
33
Caso clinico : consulenza infettivologica in neurologia
Uomo 38 anni, ricoverato (1/10/200) presso il reparto di neurologia per rallentamento ideo motorio e disturbi neuro-psichiatrici. Condizioni generali scadute,paziente febbrile (38°C), parametri emodinamici stabili. Tono dell’umore fortemente depresso.
 presso il reparto di neurologia per rallentamento ideo motorio e disturbi neuro-psichiatrici. Condizioni generali scadute,paziente febbrile (38°C), parametri emodinamici stabili. Tono dell’umore fortemente depresso.")
34
Anamnesi A febbraio 2009 riduzione tono dell’umore, apatia con ritiro sociale, ideazioni a carattere paranoideo, insonnia. Marzo 2009 ricovero per “sindrome depressiva severa con idee melanconiche“ in clinica psichiatrica a Monaco. Viene consigliata terapia antipsicotica e antidepressiva.

35
Test HIV ELISA E Western Blot positivo
Esame obiettivo Rallentamento nei movimenti e nell’eloquio, vigile, non orientato nel tempo e nello spazio, no deficit neurologici sensitivo-motori. CD4+:27 /μL (6%), HIV RNA cp/ml Test HIV ELISA E Western Blot positivo
, HIV RNA cp/ml. Test HIV ELISA E Western Blot positivo.")
36
RMN Encefalo ….aree di alterata intensità del segnale, iperintense in corrispondenza della sostanza bianca periventricolare delle corona radiata e dei centri semiovali bilateralmente ….. ….circoscritta area di alterata intensità del segnale in sede fronto basale sinistra …

37
Fibroncoscopia con Broncolavaggio
TC Torace …aspetto a vetro smerigliato, più evidente a livello dei lobi superiori in sede mantellare Fibroncoscopia con Broncolavaggio Pneumocystis jirovecii esame microscopico, ricerca diretta e PCR: positvo

38
Stadiazione dell’infezione
CD4+:27 /μL (6%) HIV-RNA: cp/ml CDC : C3 Genotypic resistance testing for HIV: wild-type TEST HLA B5701 negativo
 HIV-RNA: cp/ml. CDC : C3. Genotypic resistance testing for HIV: wild-type. TEST HLA B5701 negativo.")
39
Puntura Lombare HIV RNA liquor: cp/ml

40
Leucopenia, neutropenia, trombocitopenia
23/10/09 3TC/AZT +LPV/R+RAL CPE :12 07/10/09 3TC/AZT +ATZ/R CPE: 8 potenziamento Leucopenia, neutropenia, trombocitopenia TERAPIA HAART Ag CMV 25cell, CMV Pcr Dna cp/ml 05/11/09: 3TC/ABC +LPV/R+Maraviroc CPE: 11 30/10/09: 3TC/ABC +LPV/R+RAL CPE: 11 rabdomiolisi

41
Parametri immuno-virologici I
HIV RNA PLASMA HIV RNA LIQUOR

42
Parametri immuno-virologici II

Presentazioni simili




 Roma 24 marzo Organizzazione Key4biz FORUM 2011.>")
















