Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Elasticità e tessuto neoplastico Considerazioni di fisiopatologia
Antonio Pio Masciotra Campobasso-Molise-Italia Skype : antonio.masciotra

2
Mechanical (elastic) properties of neoplastic tissue Physiopathology
Antonio Pio Masciotra Campobasso-Molise-Italy Skype : antonio.masciotra

3
Elastografia mammaria : quantitativa o qualitativa?
Antonio Pio Masciotra Campobasso Skype : antonio.masciotra

4
Breast sonoelastography : quantitative or qualitative?
Antonio Pio Masciotra Campobasso-Molise-Italy Skype : antonio.masciotra

5
PRINCIPAL MECHANICAL PROPERTIES
Those characteristics of the materials which describe their behaviour under external loads are known as Mechanical Properties. The most important and useful mechanical properties are: Strength It is the resistance offered by a material when subjected to external loading. So, stronger the material the greater the load it can withstand. Depending upon the type of load applied the strength can be tensile, compressive, shear or torsional. The maximum stress that any material will withstand before destruction is called its ultimate strength. Elasticity Elasticity of a material is its power of coming back to its original position after deformation when the stress or load is removed. Elasticity is a tensile property of its material. The greatest stress that a material can endure without taking up some permanent set is called elastic limit. Stiffness (Rigidity) The resistance of a material to deflection is called stiffness or rigidity. Steel is stiffer or more rigid than aluminium. Stiffness is measured by Young’s modulus E. The higher the value of the Young’s modulus, the stiffer the material. Hardness It is the ability of a material to resist scratching, abrasion, indentation or penetration.
 The resistance of a material to deflection is called stiffness or rigidity. Steel is stiffer or more rigid than aluminium. Stiffness is measured by Young’s modulus E. The higher the value of the Young’s modulus, the stiffer the material. Hardness. It is the ability of a material to resist scratching, abrasion, indentation or penetration.")
6
PRINCIPALI PROPRIETA’ MECCANICHE
Le caratteristiche dei materiali che descrivono il loro comportamento quando vengono sottoposti a carichi esterni vengono definite PROPRIETA’ MECCANICHE. Le più importanti di esse sono: FORZA E’ la resistenza offerta da un materiale quando viene sottoposto ad un carico esterno. Pertanto, quanto più forte è un materiale tanto maggiore sarà il carico che esso può sorreggere. ELASTICITA’ E’ la capacità di un materiale a recuperare le sue posizione e forma iniziali dopo la rimozione di un carico od una forza, la cui applicazione ne aveva indotto la deformazione. STIFFNESS (RIGIDITA’) E’ la resistenza che un materiale oppone al suo ‘piegamento’. L’acciaio è più rigido dell’alluminio. La stiffness viene misurata dal Modulo di Young E. Quanto maggiore è il valore del modulo di Young tanto maggiore è la stiffness del materiale. DUREZZA E’ la capacità di un materiale a resistere al graffio, all’abrasione, alla scalfittura od alla penetrazione
 E’ la resistenza che un materiale oppone al suo ‘piegamento’. L’acciaio è più rigido dell’alluminio. La stiffness viene misurata dal Modulo di Young E. Quanto maggiore è il valore del modulo di Young tanto maggiore è la stiffness del materiale. DUREZZA. E’ la capacità di un materiale a resistere al graffio, all’abrasione, alla scalfittura od alla penetrazione.")
8
ATOMIC FORCE MICROSCOPE

9
Stiffness distribution of cells and results of migration and invasion test
Citation: Xu W, Mezencev R, Kim B, Wang L, McDonald J, et al. (2012) Cell Stiffness Is a Biomarker of the Metastatic Potential of Ovarian Cancer Cells. PLoS ONE 7(10): e doi: /journal.pone
 Cell Stiffness Is a Biomarker of the Metastatic Potential of Ovarian Cancer Cells. PLoS ONE 7(10): e doi: /journal.pone")
10
Normal cell toward cancer cell
The distribution of the actin network plays an important role in determining the mechanical properties of single cells. As cells transform from non-malignant to cancerous states, their cytoskeletal structure changes from an organized to an irregular network, and this change subsequently reduces the stiffness of single cells. Further progressive reduction of stiffness corresponds to an increase in invasive and migratory capacity of malignant cells. Less invasive Normal cell toward cancer cell Single cell stiffness reduction More invasive

11
Mammary epithelial growth and morphogenesis is regulated by matrix stiffness.
(A) 3D cultures of normal mammary epithelial cells within collagen gels of different concentration. Stiffening the ECM through an incremental increase in collagen concentration (soft gels: 1 mg/ml Collagen I, 140 Pa; stiff gels 3.6 mg/ml Collagen I, 1200 Pa) results in the progressive perturbation of morphogenesis, and the increased growth and modulated survival of MECs. Altered mammary acini morphology is illustrated by the destabilization of cell–cell adherens junctions and disruption of basal tissue polarity indicated by the gradual loss of cell–cell localized β-catenin (green) and disorganized β4 integrin (red) visualized through immunofluorescence and confocal imaging. Kass et al. Page 9 Int J Biochem Cell Biol. Author manuscript; available in PMC 2009 March 19. NIH-PA
 3D cultures of normal mammary epithelial cells within collagen gels of different concentration. Stiffening the ECM through an incremental increase in collagen concentration (soft gels: 1 mg/ml Collagen I, 140 Pa; stiff gels 3.6 mg/ml Collagen I, 1200 Pa) results in the progressive perturbation of morphogenesis, and the increased growth and modulated survival of MECs. Altered mammary acini morphology is illustrated by the destabilization of cell–cell adherens junctions and disruption of basal tissue polarity indicated by the gradual loss of cell–cell localized β-catenin (green) and disorganized β4 integrin (red) visualized through. immunofluorescence and confocal imaging. Kass et al. Page 9. Int J Biochem Cell Biol. Author manuscript; available in PMC 2009 March 19. NIH-PA.")
13
Tumor cells’ stiffness decreases
Extracellular matrix’s stiffness increases

14
La rigidità delle cellule neoplastiche diminuisce
La rigidità della matrice extracellulare aumenta

15
Colorazioni istopatologiche
per evidenziare Cellularità HES NV V CD 31 Densità dei vasi Fibrosis Masson’s Trichrome

16
Histopathology techniques show
Cellularity HES NV V CD 31 Microvascular density Fibrosis Masson’s Trichrome

17
Stiffness in funzione del volume
5 mm 7 mm 11 mm 16 mm a) Molto ‘molle’ (9 kPa) ‘Molle’ (22 kPa) ‘Duro’ (50 kPa) Molto ‘duro’ (108 kPa)
 Molto ‘molle’ (9 kPa) ‘Molle’ (22 kPa) ‘Duro’ (50 kPa) Molto ‘duro’ (108 kPa)")
18
Stiffness depending on volume
5 mm 7 mm 11 mm 16 mm a) Very soft (9 kPa) Soft (22 kPa) Stiff (50 kPa) Very stiff (108 kPa)
 Very soft (9 kPa) Soft (22 kPa) Stiff (50 kPa) Very stiff (108 kPa)")
19
Stiffness in funzione della composizione
Cellularità Densità dei vasi Fibrosi Molto ‘molle’ ‘Molle’ ‘Duro’ Molto ‘duro’

20
Stiffness depending on composition
Cellularity Microvascular density Fibrosis Very soft Soft Stiff Very stiff

21
Pathological stiffness score

22
Transizione da un ‘imaging’ ‘morfologico’ ad un’imaging fisiopatologico?

23
Going from a morphologic to a physiopathologic ‘imaging’?

24
Transizione da un ‘imaging’ ‘morfologico’ ad un’imaging fisiopatologico?
SOFTVUE SOFTVUE

25
Going from a morphologic to a physiopathologic ‘imaging’?
SOFTVUE SOFTVUE

26
Nell’Antico Egitto il riscontro di una massa dura nel corpo veniva correlata ad uno stato di malattia. Nella Medicina Ippocratica la palpazione era parte essenziale dell’esame fisico del paziente. Nel Terzo Millennio la «Palpazione Remota» sta diventando realtà grazie all’ Imaging Elastografico.

27
In ancient Egypt, a link was established between
a hard mass within the human body & pathology. In Hippocratic medicine, palpation was an essential part of a physical examination. In the 21st century, «remote palpation» by means of elastographic imaging is becoming a reality.

28
Sonoelasticity: KJ Parker et al, 1990
Many R& D techniques have emerged since the 1990s, based on the Ultrasound and Magnetic Resonance imaging modalities. Sonoelasticity: KJ Parker et al, 1990 Ultrasound Strain Elastography: J Ophir et al, 1991 MR Elastography: R Sinkus et al, 2000 Shear Wave Elastography: J Bercoff et al, 2004 All techniques are based on the same principle: Generate a stress, and then use an imaging technique to map the tissue response to this stress in every point of the image. but differ substantially in terms of their performance characteristics: Qualitative / quantitative nature, absolute / relative quantification. Accuracy / precision / reproducibility, … Spatial / temporal resolution, sensitivity / penetration, …

29
Initially introduced by Hitachi, and later on Siemens, in the early 2000s.
More manufacturers have followed in the last year(s). The basic principle used is the one proposed by Ophir’s group in the early 1990s: Tissue compression (Stress) is induced manually by the user. Multiple images are recorded using conventional imaging at standard frame rates. The relative deformation (Strain) is estimated using Tissue Doppler techniques. The derived strains are displayed as a qualitative elasticity image.
. The basic principle used is the one proposed. by Ophir’s group in the early 1990s: Tissue compression (Stress) is induced. manually by the user. Multiple images are recorded using. conventional imaging at standard frame rates. The relative deformation (Strain) is estimated. using Tissue Doppler techniques. The derived strains are displayed as. a qualitative elasticity image.")
30
Strain Elastography Summary
Stress Source Manual Compression (user-dependent). Stress Frequency Static (user-induced vibration < 2 Hz). Result Type Qualitative image (E=Stress/Strain, but Stress is unknown). Relative quantification (Background-to-Lesion-Ratio). Straightforward implementation on current scanners (standard acquisition architecture, plus Tissue-Doppler-like processing).. Stress penetration / uniformity issues. User-applied compression is attenuated by soft objects & depth and cannot penetrate hard-shelled lesions. User-dependence. User-applied compression is attenuated by soft objects & depth, and cannot penetrate hard-shelled lesions.
. Stress Frequency Static (user-induced vibration < 2 Hz). Result Type Qualitative image (E=Stress/Strain, but Stress is unknown). Relative quantification (Background-to-Lesion-Ratio). Straightforward implementation on. current scanners (standard acquisition. architecture, plus Tissue-Doppler-like processing).. Stress penetration / uniformity issues. User-applied compression is attenuated by. soft objects & depth and cannot penetrate hard-shelled lesions. User-dependence. User-applied compression is attenuated by soft objects & depth, and cannot penetrate hard-shelled lesions.")
31
SuperSonic Imagine has developed a novel method called SonicTouch,
External Mechanical force Natural Heart SuperSonic Imagine has developed a novel method called SonicTouch, which is based on focused ultrasound, and can remotely generate Shear Wave-fronts providing uniform coverage of a 2D area interest.

32
Esempio di viscosità La sostanza in basso ha maggior viscosità della sostanza acquosa in alto

33
Viscosity demonstration
The bottom substance has higher viscosity than the clear liquid above

34
Strain vs. Shear Wave Elastography
Strain Elastography tends to produce a binary classification, where the whole lesion is either hard or soft. Shear Wave Elastography provides richer & more complex information with many cases of hard borders plus soft centers. The differences between Strain and Shear Wave Elastography are not surprising, given the very different principles on which they are based.

35
Shear Wave Elastography
Phantom with liquid center inside hard lesion Highly-localized estimation of tissue elasticity Especially, inside hard lesions Shear Wave Elastography can “see” inside the hard lesion, because the shear waves can propagate through the hard shell. Strain Elastography interprets the whole lesion as hard, because the applied manual compression cannot penetrate the hard shell.

36
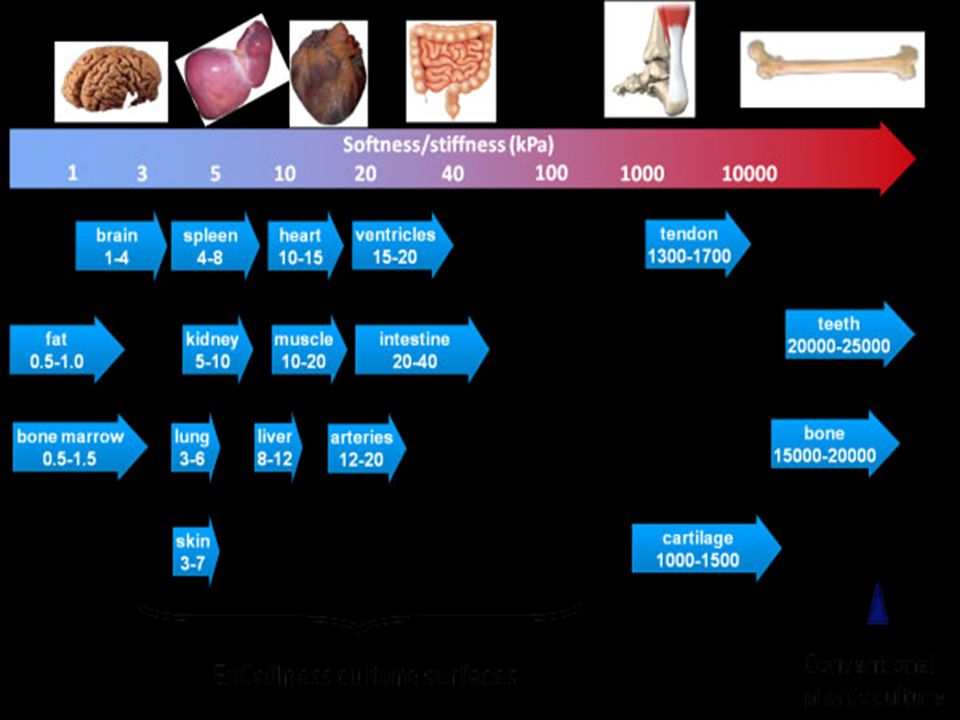
Tipo di tessuto/organo
Young’s modulus E (kPa) Densità (kg/L) Mammella Tessuto adiposo normale 18-24 1.0 ± 10% ~ Acqua Tessuto ghiandolare normale 28-66 Tessuto fibroso 96-244 Carcinoma 22-560 Prostata Parte anteriore normale 55-63 Parte posteriore normale 62-71 Iperplasia benigna 36-41 96-241 Muscolo 6-7 Fegato Parenchima sano 0.4-6 Rene 10-55
 Densità. (kg/L) Mammella. Tessuto adiposo normale ± 10% ~ Acqua. Tessuto ghiandolare normale Tessuto fibroso Carcinoma Prostata. Parte anteriore normale Parte posteriore normale Iperplasia benigna Muscolo Fegato. Parenchima sano Rene")
37
Breast multiple fibroadenomas – Directional PD
Mother (58 years old) Daughter (29 years old)
 Daughter (29 years old)")
38
Breast multiple fibroadenomas – SW Elastography
Mother (58 years old) Daughter (29 years old)
 Daughter (29 years old)")
39
Breast SWE – Normal Fat kPa Gland kPa

40
Breast SWE – Hyperechoic nodule in fat
Fat 7.8 kPa Nodule 4.8 kPa

41
Breast SWE – unilateral gynecomastia 16 years
Nodule 14.8 kPa Parenchima 21.3 kPa

42
RT induced effects on breast Bidimensional US
6 months after RT 13 years after RT

43
RT induced effects on breast SW Elastography
6 months after RT 135 kPa 13 years after RT 25 kPa

44
RT induced breast subacute effects 3D US

45
RT induced breast subacute effects 3D SWE

47
Breast complicated cyst Bidimensional US
First study 7 days after therapy

48
Breast complicated cyst Powerdoppler
First study 7 days after therapy

49
Breast complicated cyst SW Elastography
First study 7 days after therapy

50
Breast complicated cyst 3D US
First study 7 days after therapy

51
Breast complicated cyst 3D SWE
First study 7 days after therapy

52
Breast complicated cyst SWE different settings
Resolution mode Penetration mode

53
Breast fibroadenomas Bidimensional US
Almost homogeneous Inhomogeneous

54
Breast fibroadenomas SW Elastography
Different kPa 26kPa Vs 83 kPa Similar elasticity ratio 2.1 Vs 2.5

55
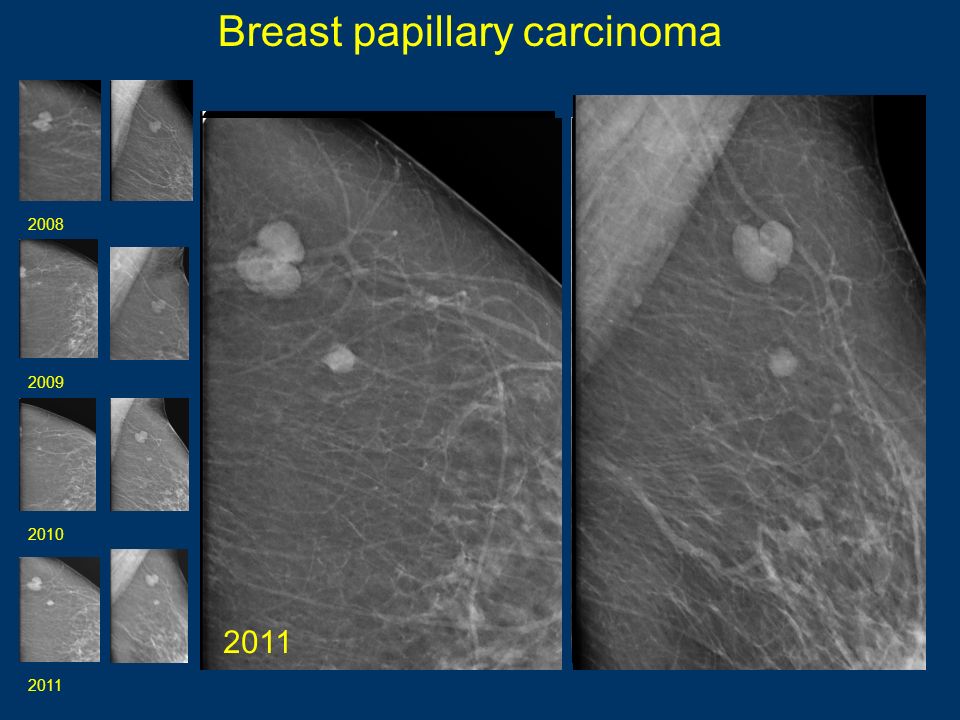
Breast papillary carcinoma
2008 2011 2010 2009 2008 2009 2010 2011
56
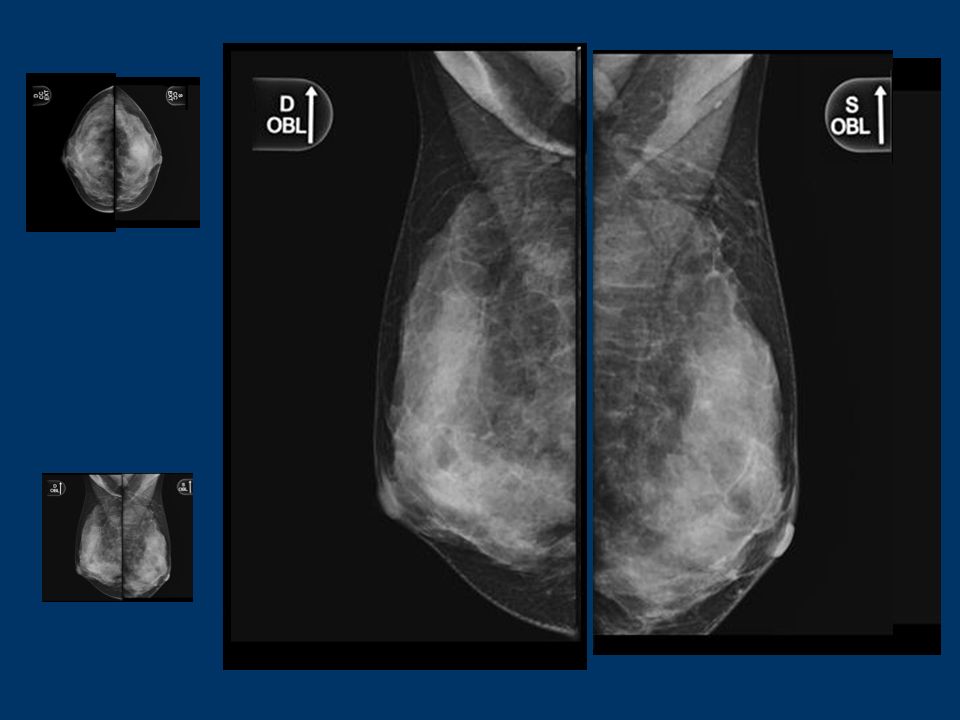
Breast carcinoma – Mammography
Benign Malignant

57
Breast carcinoma – US Bidimensional – 0.89 cm 3D – 1.86 xm

58
Breast carcinoma – SWE Bidimensional 3D

59
Breast carcinoma – SWE High transparence Low transparence

60
Breast carcinoma Vs Fibroadenoma SWE
High transparence High transparence

61
2 more nodules in the same breast Bidimensional US
Nodule n. 1 Nodule n. 2

62
2 more nodules in the same breast SW Elastography (both benign at histology)
Nodule n. 1 Nodule n. 2

63
Breast carcinoma – Axilla US
Bidimensional 3D

64
Breast carcinoma – Axilla SWE
Bidimensional 3D

65
Breast cancer metastasis
Lymphnodes 2D US B cell Lymphoma Breast cancer metastasis

66
Lymphnodes US 3D Breast cancer metastasis B cell Lymphoma

67
Breast cancer metastasis
Lymphnodes SWE Breast cancer metastasis B cell Lymphoma

68
Lymphnodes in different sites in the same patient Bidimensional US
B cell Lymphoma ext. iliac B cell Lymphoma inguinal

69
Lymphnodes in different sites in the same patient SW Elastography
B cell Lymphoma ext. iliac B cell Lymphoma inguinal

70
Lymphnodes SWE Different stiffness depending on histology
B cell Lymphoma kPa Breast cancer metastasis – 16 kPa NET metastasis -209 kPa

72
Correct tissue elasticity quantification
Aims of elastography Correct tissue elasticity quantification Identification of ‘cut off’ elasticity values for the right diagnostic workup of diffuse and focal diseases

73
Breast lipomas SW Elastography precision and repeatibility
Fat 19.9 kPa Lipoma 20.5 kPa SW Ratio 1.03 Ore 10:07:09 Fat 8.0 kPa Lipoma 7.8 kPa SW Ratio 1.03 Ore 10:07:34

74
Breast sonoelastography :
Question n. 1 : quantitative or qualitative? Answer n. 1 Quantitative! Question n. 2 : SW or Strain Elastography? Answer n. 2 SW Elastography Antonio Pio Masciotra Campobasso-Molise-Italy Skype : antonio.masciotra

75
Skype : antonio.masciotra

Presentazioni simili


 064825120 - fax.>")








>")





>")
>")

