Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Licia Laurino and Angelo P. Dei Tos
Confronto Interistituzionale in Patologia Mammaria: determinazione immunofenotipica di ER/PR Licia Laurino and Angelo P. Dei Tos Dipartimenti di Patologia ed Oncologia Treviso

2
Breast Cancer Diagnosis
Necessary Difficult Insufficient for planning the adjuvant treatment

4
St. Gallen Conference Absolute importance of timely, accurate and reliable histopathologic assessment Target identification and quantitation Enhanced partnership between clinician and pathologists substantially improved outcomes.

6
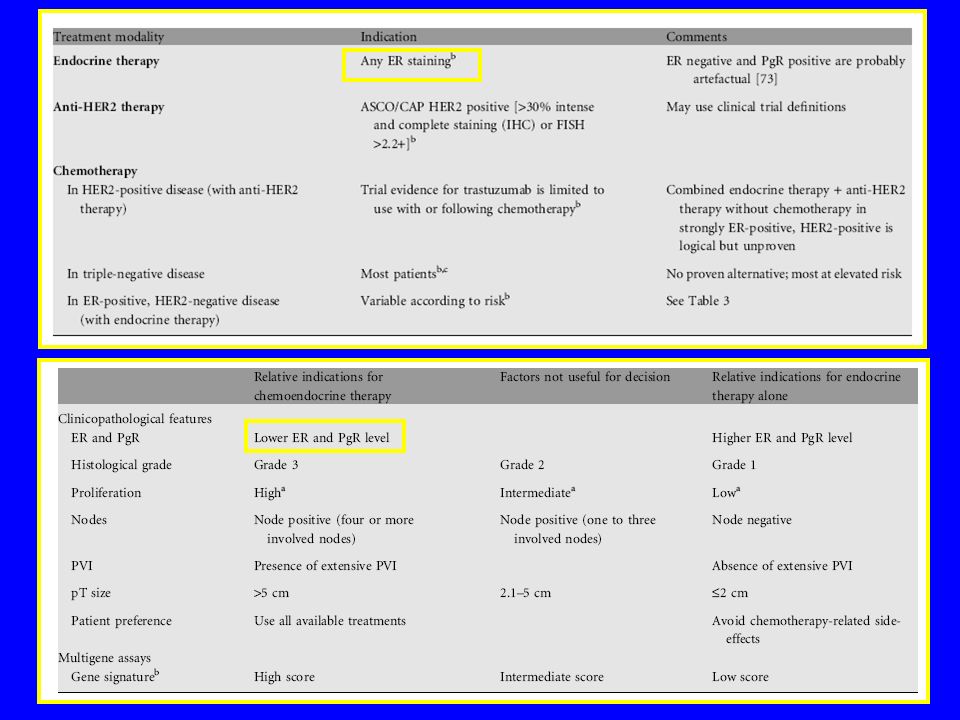
Treatment Options Endocrine therapy Anti HER2 therapy Chemotherapy
Any detectable ER Anti HER2 therapy HER2 + (ASCO/CAP) Chemotherapy
 Chemotherapy.")
8
Gene Epression Signatures
“…after a long debate, the Panel supported the use of a validated multigene-profiling assay, as an adjunct to high quality phenotyping of breast cancer in cases in which the indication for adj chemo remained uncertain”

10
Currently accepted prognostic/predictive parameters
Patient Age characteristics (Race) Disease Tumor size characteristics Tumor type Axillary status Tumor grade Peritum. vascular invasion Biomarkers Receptor status HER2/neu expression Ki-67 labeling index
 Disease Tumor size. characteristics Tumor type. Axillary status. Tumor grade. Peritum. vascular invasion. Biomarkers Receptor status. HER2/neu expression Ki-67 labeling index.")
11
The histopathologic report
Invasive ductal ca, NOS, G2, negative margins, with 2 lymph node mets in post-meno patient. ER: 90%; PgR 90%, HER2 negative, Ki67: 12% Endocrine-responsive tumor with an intermediate risk. Adjuvant Tamoxifen for 2 yrs, followed by AI for additional 3 yrs. Then wait for the results of current trials of extended endocrine treatment

12
The histopathologic report
Invasive ductal ca, NOS, G2, negative margins, with 2 lymph node mets in post-meno patient. ER: 90%; PgR 90%, HER2 negative, Ki67: 12% Endocrine-responsive tumor with an intermediate risk. Adjuvant Tamoxifen for 2 yrs, followed by AI for additional 3 yrs. Then wait for the results of current trials of extended endocrine treatment

13
Increasing Roles for Pathologist
Taxane most effective on endocrine Non or INCOMPLETELY responsive tumors Optimal ER/PgR/HER2 assessment Microtubule binding protein TAU predicts response to Paclitaxel Topoisomerase II alpha amplification and protein overxpression predict response to anthracyclins (?) Basal –like tumors (often associated with BRCA1) more responsive to DNA damaging agents (platinum)
 Basal –like tumors (often associated with BRCA1) more responsive to DNA damaging agents (platinum)")
14
External quality controls for ER
UK-NEQAS (round #53) (#54) Score >12/20 49% 69% Score % 16% Score <10/20 24% 15% German Q.A.: False-negative rate = 11-24% (Am J Surg Pathol 2002)
 (#54) Score >12/20 49% 69% Score % 16% Score <10/20 24% 15% German Q.A.: False-negative rate = 11-24% (Am J Surg Pathol 2002)")
15
J Nat Cancer Inst 2008, 100:836.

18
CQ Veneto 09 Inviate sezioni di mammella normale, carcinoma papillare, (+vo) carcinoma adenoidocistico (-vo), carcinoma lobulare pleomorfo (debolmente +vo) 14 centri
 carcinoma adenoidocistico (-vo), carcinoma lobulare pleomorfo (debolmente +vo) 14 centri.")
19
Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica TV OK 100% 2% SP1 / 636 Polimero DAKO A - disomog ++ Deb pos ? 2% deb 100% deb ? SP1/Ab8 ultravision C 30-40% ? Vector D Deb 50% Contr. Ins. Bond-max E 90% <5% 6F11/1A6 F SP1/ 1E2 Ventana G 90% debole

20
TV Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica OK 100% 2%
2% SP1 / 636 Polimero DAKO H disomog SP1 /1E2 Ventana I Deb Contr. Ins. Polimero L np 6F11 / 636 Bondmax N SP1/1E2 ? O P R 60% S BondMax

21
Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica TV OK 100% 2% SP1 / 636 Polimero DAKO A - disomog ++ Deb pos ? 2% deb 100% deb ? SP1/Ab8 ultravision C 30-40% ? Vector D Deb 50% Contr. Ins. Bond-max E 90% <5% 6F11/1A6 F SP1/ 1E2 Ventana G 90% debole

22
TV Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica OK 100% 2%
2% SP1 / 636 Polimero DAKO H disomog SP1 /1E2 Ventana I Deb Contr. Ins. Polimero L np 6F11 / 636 Bondmax N SP1/1E2 ? O P R 60% S BondMax

23
Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica TV OK 100% 2% SP1 / 636 Polimero DAKO A - disomog ++ Deb pos ? 2% deb 100% deb ? SP1/Ab8 ultravision C 30-40% ? Vector D Deb 50% Contr. Ins. Bond-max E 90% <5% 6F11/1A6 F SP1/ 1E2 Ventana G 90% debole

24
TV Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica OK 100% 2%
2% SP1 / 636 Polimero DAKO H disomog SP1 /1E2 Ventana I Deb Contr. Ins. Polimero L np 6F11 / 636 Bondmax N SP1/1E2 ? O P R 60% S BondMax

25
Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica TV OK 100% 2% SP1 / 636 Polimero DAKO A - disomog ++ Deb pos ? 2% deb 100% deb ? SP1/Ab8 ultravision C 30-40% ? Vector D Deb 50% Contr. Ins. Bond-max E 90% <5% 6F11/1A6 F SP1/ 1E2 Ventana G 90% debole

26
TV Nor ER Nor PR Pos PR Neg Neg PR Deb ER Deb PR Metodica OK 100% 2%
2% SP1 / 636 Polimero DAKO H disomog SP1 /1E2 Ventana I Deb Contr. Ins. Polimero L np 6F11 / 636 Bondmax N SP1/1E2 ? O P R 60% S BondMax

27
PR normal breast

28
ER normal breast

30
ER

31
PR

33
ER

35
ER Low expressing

36
PR +ve ?

37
ER

38
ER

39
PR-ve

41
Statement 14. Scelta del campione per la determinazione dei fattori prognostico predittivi
E’ necessario che l’ inclusione scelta per la determinazione dei parametri biologici includa anche parenchima mammario non neoplastico in tutti i casi in cui ciò sia possibile. 41

42
Statement 15. Scelta del campione per la determinazione dei fattori prognostico predittivi
La valutazione dei parametri biologici (assetto recettoriale, stato di HER2 e Ki-67) deve essere effettuata anche sulle biopsie pre-operatorie se è prevista terapia neo-adiuvante e sulle biopsie di recidive e metastasi 42
 deve essere effettuata anche sulle biopsie pre-operatorie se è prevista terapia neo-adiuvante e sulle biopsie di recidive e metastasi. 42.")
43
Statement 16. Scelta del campione per la determinazione dei fattori prognostico predittivi
Nel caso di neoplasie multiple, la determinazione dei parametri biologici va effettuata su tutte le lesioni solo se di diverso istotipo o grado 43

44
Statement 17. Determinazione sulle neoplasie in situ di fattori prognostico predittivi
La determinazione dell’assetto recettoriale (ER/PR) deve essere effettuata anche su neoplasie intraduttali
 deve essere effettuata anche su neoplasie intraduttali.")
45
Statement 18. Determinazione dei recettori ormonali
Il referto deve riportare il clone utilizzato per la determinazione immunocitochimica dei recettori La valutazione dell’assetto dei recettori ormonali deve essere espressa in valori percentuali indipendentemente dalla intensità di colorazione

46
Statement 19. Determinazione dei recettori ormonali
La valutazione dell’assetto recettoriale deve corrispondere alla espressione media di recettori dell’ intera sezione esaminata

47
Statement 20. Determinazione dei recettori ormonali
Il controllo positivo interno deve mostrare una colorazione eterogenea delle cellule luminali normali, con cellule non colorate accanto a cellule debolmente colorate e a cellule intensamente colorate. Una colorazione limitata a poche cellule e di uguale intensità può essere dovuta ad una scarsa sensibilità della reazione. Le cellule mioepiteliali e i fibroblasti rappresentano un utile controllo negativo interno: una loro colorazione per quanto debole è segno di aspecificità della reazione

48
Conclusions The pathology report of breast cancer is the choice of adjuvant therapy The report must be complete and accurate – in the diagnosis and in the assessment of prognostic/predictive parameters Pathologists should be more and more aware of their role in the management of patients with breast carcinoma

49
Conclusions Good laboratory practice Technical validation
Clinical validation Correlation with outcome Internal and external quality control programs

Presentazioni simili









>")















