Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Antibiotici Beta lattamici

3
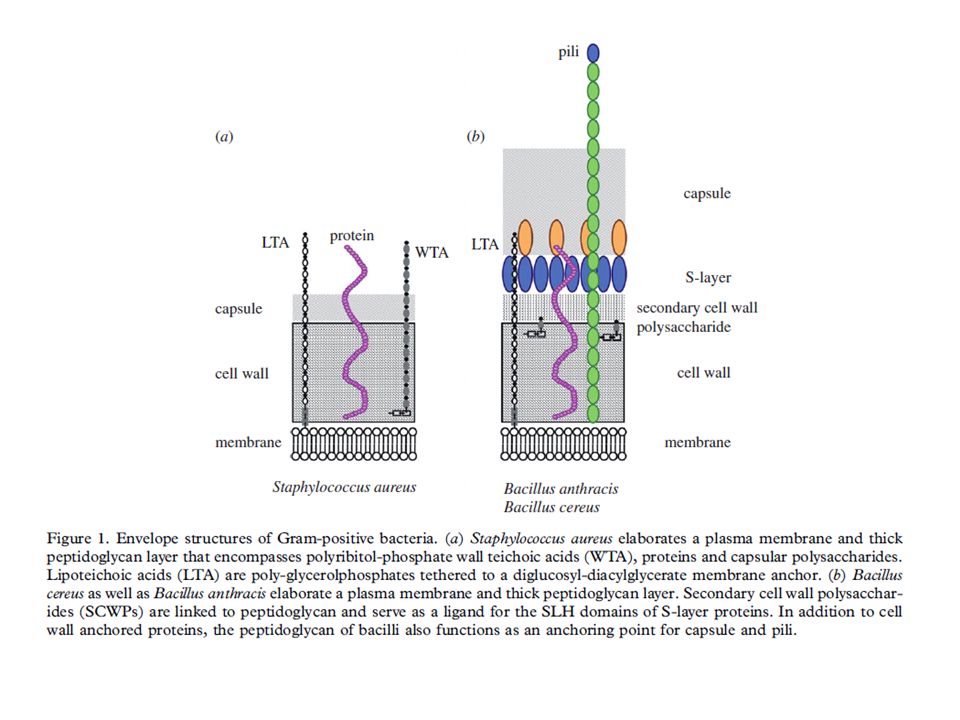
Schematic of the monoderm Gram-positive cell envelope
Schematic of the monoderm Gram-positive cell envelope. LTA: lipoteichoic acid polymers; WTA: wall teichoic acid polymers; M: N-acetyl-muramic acid; G: N-acetyl glucosamine. Refer to text for further details.

6
Schematic structure of PG and target sites of different enzymes (pointed by color arrows). The synthetic enzyme (PBP) is highlighted in red while the lytic enzymes (NagZ, AmpD, and LT) are highlighted in blue. Notably, NagZ and AmpD catalyze the liberated muropeptides instead of intact PG. Hexagons denote sugars while rectangles denote stem amino acids. The cross-linkage between the top and bottom glycan strands is D-Ala → meso-A2pm. LT, lytic transglycosylase; PBP, penicillin-binding protein, m-A2pm, meso-diaminopimelic acid; AnhMurNAc, 1,6-anhydro-MurNAc; β1 → 4, β-(1,4)-glycosidic bond.
-glycosidic bond.")
7
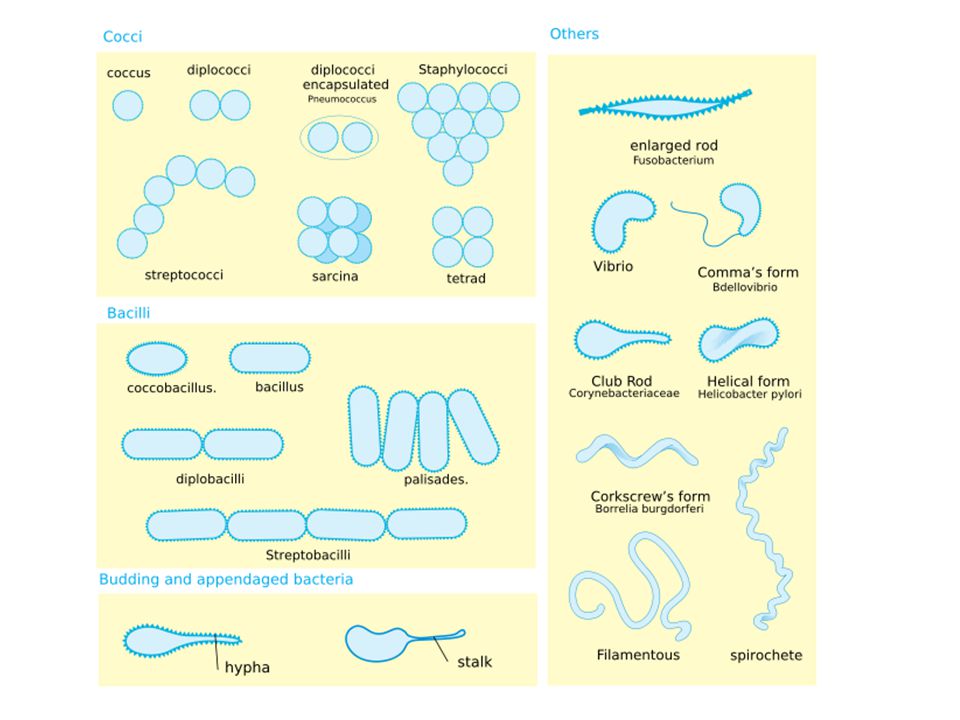
Colorazione di Gram Distingue gram positivi da gram negativi
Nata per distinguere la polmonite da streptococco (gram +) e quella da klebsiella (bacillo gram -)
 e quella da klebsiella (bacillo gram -)")
8
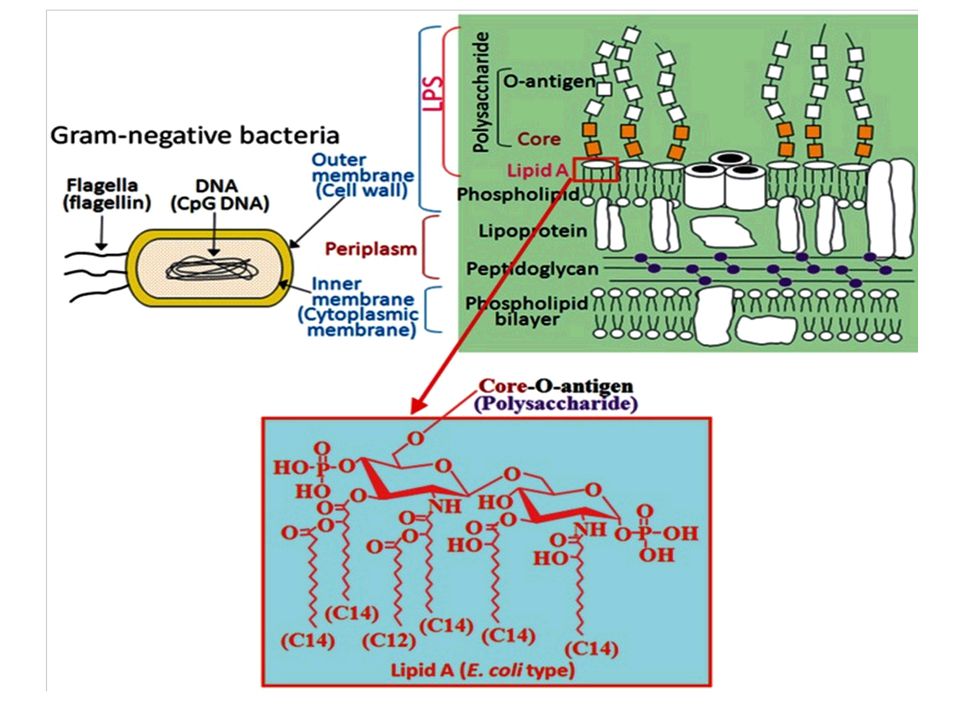
Hans Christian Gram used light microscopy to detect microbes that were stained with crystal violet/iodine. Microbes that cannot retain this dye following treatment with ethanol were counterstained with safranin (or fuchsin), thereby distinguishing Gram-positive from Gram-negative bacteria. The differential staining property is based on the peptidoglycan layer, which is considerably thicker in Gram-positive microbes. Another difference is that Gram-positive bacteria elaborate a single membrane, whereas Gram-negative microbes harbour a plasma membrane and an additional outer membrane with lipopolysaccharides.

9
Staphylococcus aureus causes a broad spectrum of disease.
Humans are colonized by this organism mainly in the nasopharynx and on the skin. Staphylococcus aureus has the unique propensity to infect and destroy normal healthy tissue, causing skin and wound infections, bloodstream infection (BSI), pneumonia, osteomyelitis, endocarditis, lung abscess, and pyomyositis.
, pneumonia, osteomyelitis, endocarditis, lung abscess, and pyomyositis.")
12
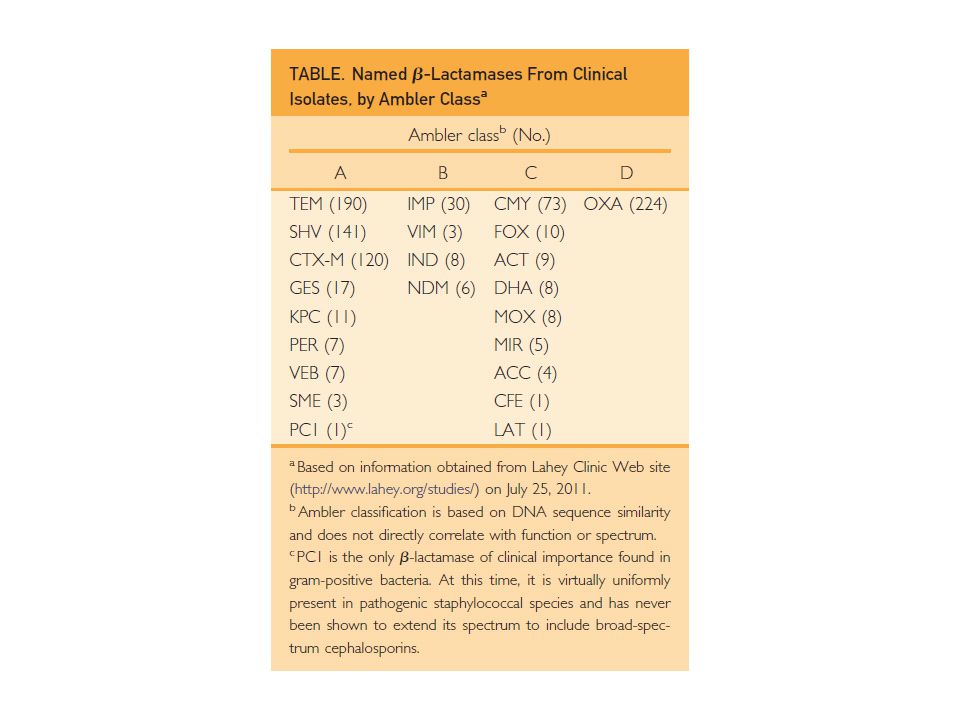
Classi di Antibiotici beta-lattamici
Amoxicillina, Ampicillina, Azlocillina, Bacampacillina, Carbenicillina, Cloxacillina, Dicloxacillina, Flucoxacillina, Piperacillina, Ticarcillina 1) Penicilline 2) Cefalosporine 3) Monobactami 4) Carbapenemi 1a Cefalessina 2a Cefamandolo 3a Cefotaxima 4a cefepime 5a Ceftobiprolo Aztreonam Imipenem, Carbapenem, Meropenem
 Penicilline. 2) Cefalosporine. 3) Monobactami. 4) Carbapenemi. 1a Cefalessina. 2a Cefamandolo. 3a Cefotaxima. 4a cefepime. 5a Ceftobiprolo. Aztreonam. Imipenem, Carbapenem, Meropenem.")
14
Inibitori beta-lattamasi
Acido clavulanico

15
Meticillina Farmaco di riferimento nel determinare la sensibilità batterica

16
Monobactami Aztreonam

17
Carbapenemi Imipenem Porzione in comune

18
6-aminopenicillanico Amidasi Penicillinasi Acido penicilloico

20
Spettro di azione delle Penicilline:
Staphylococcus, Streptococcus, Enterococcus, Actinobacteria Nocardia Polmoniti, Endocarditi, Meningiti Faringite, Scarlattina, Polmonite Endocardite, Infezione tratto urinario Lesioni toraciche

21
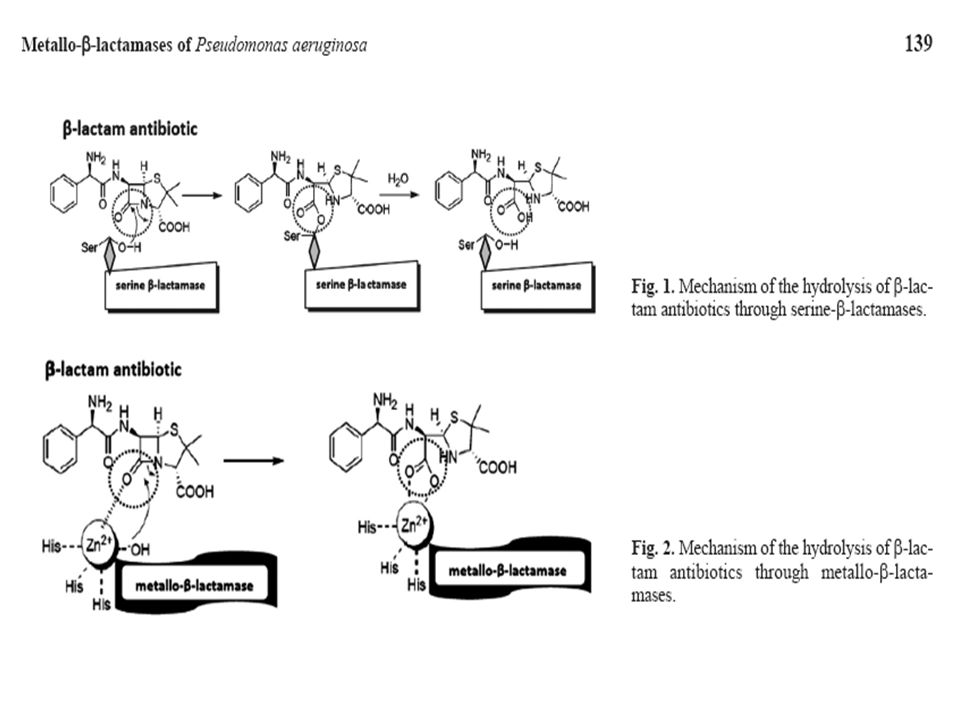
Meccanismo di azione beta lattamici

24
Inibitori beta lattamasi
Tazobactam Sulbactam Acido Clavulanico

26
Spettro di azione delle Penicilline: Bacillus anthracis (G+),
Pseudomonas (G-), Neisseria gonorrhoeae (G-), Listeria (G+) Treponema pallidum Sifilide Polmonite Infezioni Tratto Urinario Gonorrea Meningite, Endocardite, Batteriemia
, Neisseria gonorrhoeae (G-), Listeria (G+) Treponema pallidum Sifilide. Polmonite. Infezioni Tratto Urinario. Gonorrea. Meningite, Endocardite, Batteriemia.")
27
Farmacocinetica

28
Lo stafilococco aureus può causare intossicazione da cibo, polmoniti, batteriemia, impetigo (acuta piogenica che colpisce soprattutto in età pediatrica riguardante gli strati superficiali della cute, la cui comparsa di solito si limita al volto e agli arti), follicoliti e osteomieliti nell’uomo, mastiti artriti e infezioni del tratto urinario negli animali. Lo stafilococco è la principale causa di infezioni nosocomiali del sistema nervoso centrale e l’aureus è il più comune agente della batteriemia.

29
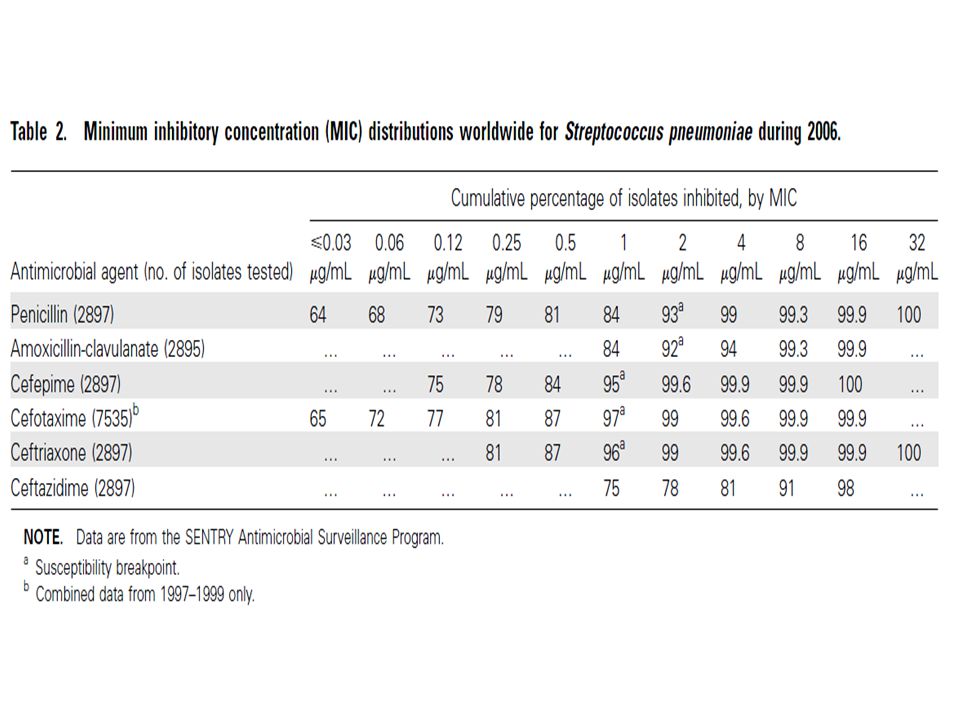
Acute bacterial meningitis caused by Streptococcus pneumoniae resistant to the antimicrobian agents and their serotypes La resistenza allo streptococco pneumonie da parte delle penicilline è dovuta ad una minor affinità di queste alla parete cellulare di questo batterio in particolare alle penicillin binding proteins. C’è una progressiva riduzione della sensibilità alla penicillina ed altri beta lattamici che causa il bisogno di aumentare le dosi per inibire la crescita batterica.

33
Treponema pallidum

34
Pseudomonas aeruginosa (gram negativo)
")
35
Lo Pseudomonas aeruginosa (P. A
Lo Pseudomonas aeruginosa (P.A.)è un batterio gram negativo di cui è nota la sua la sua versatilità ambientale, l’abilità di causare la malattia in particolari individui suscettibili e di resistere agli antibiotici. La complicazione più seria in cui è coinvolto è la fibrosi cistica e porta ad infezione respiratoria diffusa. Lo P. A. può produrre un numero considerevole di proteine tossiche le quali non solo causano un esteso danno tissutale ma anche interferiscono con il sistema immunitario. Queste proteine possono uccidere le cellule entrandovici o portare danni al tessuto connettivo.
è un batterio gram negativo di cui è nota la sua la sua versatilità ambientale, l’abilità di causare la malattia in particolari individui suscettibili e di resistere agli antibiotici. La complicazione più seria in cui è coinvolto è la fibrosi cistica e porta ad infezione respiratoria diffusa. Lo P. A. può produrre un numero considerevole di proteine tossiche le quali non solo causano un esteso danno tissutale ma anche interferiscono con il sistema immunitario. Queste proteine possono uccidere le cellule entrandovici o portare danni al tessuto connettivo.")
36
Penicilline antipseudomonas
Antibiotico MIC (microgrammi/ml) Pseudomonas E.Coli Carbenicillina 32 8 Piperacillina 4 2 Ticarcillina Mezlocillina
 Pseudomonas. E.Coli. Carbenicillina Piperacillina Ticarcillina. Mezlocillina.")
38
Sintomi della Gonorrea
La gonorrea è causata dal batterio Neisseria gonorrhoeae.Il periodo di incubazione è di 10/20 giorni con comparsa dei sintomi tra il 15 e il 20 giorno dopo l’infezione. Un piccolo numero di persone sono asintomatici per tutta la vita. Tra il 30 e il 60% delle persone con gonorrea hanno la malattia in uno stato subclinico. Nelle donne questa malattia si può manifestare con perdite uterine, difficoltà di urinare, alterazione del ciclo mestruale o sanguinamento dopo rapporto sessuale. La cervice pu; apparire in varie forme; da normale ad stremamente infiammata con pus. Infezioni dell’uretra e della cervice sono frequenti. L’infezione si trasmette per via vaginale, orale e anale. Gli uomini hanno solo un 20% di probabilità di infettarsi per via sessuale mentre le donne per il 50%. Una madre affetta da gonorrea può trasferirla al nascituro durante il parto producendogli oftalmia neonatale.

39
Antibiotici che possono essere usati in caso di gonorrea
Amoxicillina 2 g più probenecid 1 g orale Ampicillina 2 to 3 g più probenecid 1 g orale Azitromicina 2 g orale Cefixime 400 mg orale Cefotaxime 500 mg per iniezione muscolare Cefoxitin 2 g per iniezione muscolare , plus probenecid 1 g orale Cefpodoxime (Vantin) 400 mg orale Ceftriaxone (Rocephin) 125 to 250 mg per iniezione muscolare Ciprofloxacina 500 mg orale Levofloxacina 250 mg orale Ofloxacina 400 mg orale Spectinomicina 2 g per iniezione muscolare Penicilline Macrolidi Cefalosporine Chinolonici Aminociclitolo
 400 mg orale. Ceftriaxone (Rocephin) 125 to 250 mg per iniezione muscolare. Ciprofloxacina 500 mg orale. Levofloxacina 250 mg orale. Ofloxacina 400 mg orale. Spectinomicina 2 g per iniezione muscolare. Penicilline. Macrolidi. Cefalosporine. Chinolonici. Aminociclitolo.")
40
Indicazioni Terapeutiche
per le Penicilline: Endocarditi batteriche Gonorrea Meningite Polmoniti Ascessi polmonari Sifilide Setticemia

41
Antibiotic-induced liver toxicity: mechanisms, clinical features and causality assessment.
Robles M, Toscano E, Cotta J, Lucena MI, Andrade RJ. Source Liver Unit, Gastroenterology Service and Department of Medicine, Vírgen de Victoria University Hospital, University of Málaga, Spain. Abstract Antibiotics are the therapeutic agents most often associated with hepatotoxicity. However, this is mainly due to the widespread prescription of these drugs. The relative risk of antibiotic-related hepatotoxicity is low. Causality assessment of suspected drug-induced liver injury (DILI) related to antibiotics can be difficult, particularly because some cases occur long after the drug has been stopped. Among the penicillins, amoxicillin clavulanate is the most associated with hepatotoxicity and is the most frequent cause of DILI-related hospitalisations. Flucloxacillin ranks as the second highest cause of DILI in many countries. The severity of antibiotic-induced DILI varies widely, with the hepatitis-like (hepatocellular) damage tending to be more severe that than cholestatic/mixed type. The pattern is strongly influenced by age. Recently telithromycin (a new generation macrolide) has been linked with DILI, with a typical pattern, which includes abrupt commencement of fever, abdominal pain, jaundice and, in some cases, ascites. Antibiotic-induced DILI appears, in most instances, to be idiosyncratic. Genetic-association studies have recently identified genotypes related to flucloxacillin and possibly to amoxicillin-clavulanate hepatotoxicity.
 related to antibiotics can be difficult, particularly because some cases occur long after the drug has been stopped. Among the penicillins, amoxicillin clavulanate is the most associated with hepatotoxicity and is the most frequent cause of DILI-related hospitalisations. Flucloxacillin ranks as the second highest cause of DILI in many countries. The severity of antibiotic-induced DILI varies widely, with the hepatitis-like (hepatocellular) damage tending to be more severe that than cholestatic/mixed type. The pattern is strongly influenced by age. Recently telithromycin (a new generation macrolide) has been linked with DILI, with a typical pattern, which includes abrupt commencement of fever, abdominal pain, jaundice and, in some cases, ascites. Antibiotic-induced DILI appears, in most instances, to be idiosyncratic. Genetic-association studies have recently identified genotypes related to flucloxacillin and possibly to amoxicillin-clavulanate hepatotoxicity.")
42
Carbapenemi Imipenem Porzione in comune

43
Carbapenemi A questa classe appartengono: l’imipenem, il meropenem, l’ertapenem, e il doripenem. Questi agenti hanno il più vasto spettro antibatterico rispetto agli altri beta lattamici. Sono resistenti alle beta lattamasi. Sono attivi contro i gram positivi e negativi con l’eccezione di quelli intracellulari come le clamidie. Essi provvedono ad una maggiore copertura nei confronti dei batteri gram negativi rispetto agli altri beta lattamici e sono stabili nei confronti delle beta lattamasi e nei confronti di batteri multiresistenti.

44
Carbapenems versus other beta-lactams in treating severe infections in intensive care: a systematic review of randomised controlled trials. Edwards SJ, Clarke MJ, Wordsworth S, Emmas CE. Carbapenems have not been comprehensively compared in clinical trials with fourth-generation cephalosporins (4GC) and antipseudomonal penicillins (APP) in the treatment of severe infections (SI) and febrile neutropenia (FN). Of the 265 papers identified, 12 were appropriate for meta-analysis (four 4GC and eight APP). The results showed that carbapenems are associated with a significant reduction in all-cause mortality compared to APP in the treatment of SI, and withdrawals due to adverse events (RR 0.65, 95% CI: 0.45 to 0.96; p=0.03) are also less common. When compared in the treatment of FN, carbapenems are associated with a significant increase in clinical response during the initial 72 h of treatment (RR 1.37, 95% CI: 1.09 to 1.74; p=0.008) and bacteriologic response (RR 1.73, 95% CI: 1.03 to 2.89; p=0.04). For all other outcomes, including all comparisons with 4GC, there were no significant differences between treatments. The use of carbapenems rather than APP could reduce mortality and, by simplifying treatment decisions, reduce the time before patients receive appropriate antibiotic treatment.
 and antipseudomonal penicillins (APP) in the treatment of severe infections (SI) and febrile neutropenia (FN). Of the 265 papers identified, 12 were appropriate for meta-analysis (four 4GC and eight APP). The results showed that carbapenems are associated with a significant reduction in all-cause mortality compared to APP in the treatment of SI, and withdrawals due to adverse events (RR 0.65, 95% CI: 0.45 to 0.96; p=0.03) are also less common. When compared in the treatment of FN, carbapenems are associated with a significant increase in clinical response during the initial 72 h of treatment (RR 1.37, 95% CI: 1.09 to 1.74; p=0.008) and bacteriologic response (RR 1.73, 95% CI: 1.03 to 2.89; p=0.04). For all other outcomes, including all comparisons with 4GC, there were no significant differences between treatments. The use of carbapenems rather than APP could reduce mortality and, by simplifying treatment decisions, reduce the time before patients receive appropriate antibiotic treatment.")
45
Un esempio: Nella esacerbazione acuta della bronchite cronica
First-Line : Amoxicillin, ampicillin, pivampicillin, TMP/SMX, and doxycycline were considered to be first-line antibiotics for the management of patients with AECB (acute exacerbations of chronic bronchitis). and Second-Line Antibiotics: Amoxicillin/clavulanic acid, macrolides (ie, roxithromycin, clarithromycin, and azithromycin), second-generation or third-generation cephalosporins (ie, cefaclor), and quinolones were considered to be advanced or second-line antibiotics for this indication according to published guidelines.
. and Second-Line Antibiotics: Amoxicillin/clavulanic acid, macrolides (ie, roxithromycin, clarithromycin, and azithromycin), second-generation or third-generation cephalosporins (ie, cefaclor), and quinolones were considered to be advanced or second-line antibiotics for this indication according to published guidelines.")
46
Monobactami Aztreonam possiede una forte attività nei confronti dei batteri gram-negativi compreso lo Pseudomonas aeruginosa. Non è attivo nei confronti dei gram positivi o gli anaerobi. E’ efficace nei confronti di un gran numero di batteri tra I quali: IlCitrobacter, l’Enterobacter, l’E coli, l’Haemophilus, la Klebsiella, il Proteus, e le specie di Serratia. Attualmente si sta studianto la somministrazione di aztreonam per via inalatoria come lisinato nel trattamento della fibrosi cistica polmonare.

47
Klebsiella Serratia Polmoniti Infezioni del tratto urinario Setticemia
Spondilite anchilosante Serratia Responsabile delle infezioni nosocomiali (S. marcescens)
")
48
Proteus E’ un batterio a forma di bastoncino ed ha alte capacità di produrre ureasi che rappresenta il modo di riconoscerlo. L’ureasi idrolizza l’urea in ammoniaca e perciò alcalinizza maggiormente le urine. L’alcalinizzazione può portare a formazione di cristalli che possono precipitare nei tubuli. Questo batterio può essere trovato nei calcoli renali e questi possono ricominciare l’infezione se non eliminati. Questi calcoli possono portare anche a morte renale. Il proteus può anche causare infezioni nelle ferite, setticemia e polmoniti sopratutto nei pazienti ospedalizzati.

49
Cephalosporin use in treatment of patients with penicillin allergies.
DePestel DD, Benninger MS, Danziger L, LaPlante KL, May C, Luskin A, Pichichero M, Hadley JA. Department of Clinical Sciences, College of Pharmacy, University of Michigan Hospitals and Health Centers, University of Michigan, Ann Arbor 48109, USA. OBJECTIVE: To review the evidence that supports the use of certain cephalosporins in penicillin-allergic patients. DATA SYNTHESIS: Physicians may now prescribe certain cephalosporins in patients with a history of a nonserious, non-life-threatening penicillin reaction. Exclusions include type I anaphylaxis, Stevens-Johnson syndrome, toxic epidermal necrolysis, angioedema, and other potentially life-threatening responses to medication. Recent reports demonstrate that a considerable body of literature describing the cross-reactivity between cephalosporins and penicillin was established based on nonallergic adverse reactions or in vitro studies rather than on clinically relevant immune-mediated reactions. Oral rechallenge and skin testing data support the relationship of the beta-lactam side-chain structures of these drugs as a predictor of cross-reactivity. CONCLUSION: Recent data suggest that the incidence of cross-reactivity among penicillins and cephalosporins is lower than historically reported. Pharmacists should be aware that cephalosporin cross-reactivity in a penicillin-allergic patient is not necessarily a class effect. Dispensing should be evaluated based on the type of allergic manifestations and the drug prescribed.

50
Tossicità da beta lattamici

51
Tossicità da beta lattamici

52
Acc Chem Res. 2008 Jan;41(1):11-20. Inhibitors of FabI, an enzyme drug target in the bacterial fatty acid biosynthesis pathway. Lu H, Tonge PJ. Source Department of Chemistry and Institute for Chemical Biology & Drug Discovery, Stony Brook University, Stony Brook, New York , USA. Abstract The modern age of drug discovery, which had been slowly gathering momentum during the early part of the twentieth century, exploded into life in the 1940s with the isolation ofpenicillin and streptomycin. The immense success of these early drug discovery efforts prompted the general view that many infectious diseases would now be effectively controlled and even eradicated. However this initial optimism was misplaced, and pathogens such as multidrug-resistant Mycobacterium tuberculosis and methicillin-resistant Staphylococcus aureus present a major current threat to human health. Drug resistance arises through the unrelenting pressure of natural selection, and there is thus a continuing need to identify novel drug targets and develop chemotherapeutics that circumvent existing drug resistance mechanisms. In this Account, we summarize current progress in developing inhibitors of FabI, the NADH-dependent enoyl reductase from the type II bacterial fatty acid biosynthesis pathway (FAS-II), a validated but currently underexploited target for drug discovery. The FabI inhibitors have been divided into two groups, based on whether they form a covalent adduct with the NAD (+) cofactor. Inhibitors that form a covalent adduct include the diazaborines, as well as the front-line tuberculosis drug isoniazid. The NAD adducts formed with these compounds are formally bisubstrate enzyme inhibitors, and we summarize progress in developing novel leads based on these pharmacophores. Inhibitors that do not form covalent adducts form a much larger group, although generally these compounds also require the cofactor to be bound to the enzyme. Using structure-based approaches, we have developed a series of alkyl diphenyl ethers that are nanomolar inhibitors of InhA, the FabI from M. tuberculosis, and that are active against INH-resistant strains of M. tuberculosis. This rational approach to inhibitor development is based on the proposal that high-affinity inhibition of the FabI enzymes is coupled to the ordering of a loop of amino acids close to the active site. Compounds that promote loop ordering are slow onset FabI inhibitors with increased residence time on the enzyme. The diphenyl ether skeleton has also been used as a framework by us and others to develop potent inhibitors of the FabI enzymes from other pathogens such as Escherichia coli, S. aureus, and Plasmodium falciparum. Meanwhile chemical optimization of compounds identified in high-throughput screening programs has resulted in the identification of several classes of heteroaromatic FabI inhibitors with potent activity both in vitro and in vivo. Finally, screening of natural product libraries may provide useful chemical entities for the development of novel agents with low toxicity. While the discovery that not all pathogens contain FabI homologues has led to reduced industrial interest in FabI as a broad spectrumtarget, there is substantial optimism that FabI inhibitors can be developed for disease-specific applications. In addition, the availability of genome sequencing data, improved methods for target identification and validation, and the development of novel approaches for determining the mode of action of current drugs will all play critical roles in the road ahead and in exploiting other components of the FAS-II pathway.
, a validated but currently underexploited target for drug discovery. The FabI inhibitors have been divided into two groups, based on whether they form a covalent adduct with the NAD (+) cofactor. Inhibitors that form a covalent adduct include the diazaborines, as well as the front-line tuberculosis drug isoniazid. The NAD adducts formed with these compounds are formally bisubstrate enzyme inhibitors, and we summarize progress in developing novel leads based on these pharmacophores. Inhibitors that do not form covalent adducts form a much larger group, although generally these compounds also require the cofactor to be bound to the enzyme. Using structure-based approaches, we have developed a series of alkyl diphenyl ethers that are nanomolar inhibitors of InhA, the FabI from M. tuberculosis, and that are active against INH-resistant strains of M. tuberculosis. This rational approach to inhibitor development is based on the proposal that high-affinity inhibition of the FabI enzymes is coupled to the ordering of a loop of amino acids close to the active site. Compounds that promote loop ordering are slow onset FabI inhibitors with increased residence time on the enzyme. The diphenyl ether skeleton has also been used as a framework by us and others to develop potent inhibitors of the FabI enzymes from other pathogens such as Escherichia coli, S. aureus, and Plasmodium falciparum. Meanwhile chemical optimization of compounds identified in high-throughput screening programs has resulted in the identification of several classes of heteroaromatic FabI inhibitors with potent activity both in vitro and in vivo. Finally, screening of natural product libraries may provide useful chemical entities for the development of novel agents with low toxicity. While the discovery that not all pathogens contain FabI homologues has led to reduced industrial interest in FabI as a broad spectrumtarget, there is substantial optimism that FabI inhibitors can be developed for disease-specific applications. In addition, the availability of genome sequencing data, improved methods for target identification and validation, and the development of novel approaches for determining the mode of action of current drugs will all play critical roles in the road ahead and in exploiting other components of the FAS-II pathway.")
53
Recent Pat Antiinfect Drug Discov. 2007 Jan;2(1):73-7.
Linezolid in children: recent patents and advances. Velissariou IM. Source Research Fellow in Pediatric Infectious Diseases and Pulmonology, P and A Kyriakou Children's Hospital, Athens, Greece. Abstract Linezolid is the first approved member of a new generation of antibiotics, the synthetic oxazolidinones, to become available, with a broad spectrum of in vitro activity against Gram-positive organisms, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus faecalis and vancomycin-resistant Enterococcus faecium. It has an excellent bioavailability both intravenously and orally and a very good safety profile both in adults and in children. With regards to its antimicrobial action, linezolid has a predominantly bacteriostatic action, rather than a bacteriocidal effect and is active against Gram-positive bacteria that are resistant to other antibiotics. Linezolid is currently showing great promise for the treatment of multi-resistant Gram-positive infections, both in the community and in a hospital setting. Clinical indications so far include skin and soft tissue infections, community-acquired or nosocomial pneumonia due to MRSA, VRE bacteremia and community-acquired pneumonia due to penicillin-resistant Streptococcus pneumoniae. We anticipate that this new generation of antimicrobial agents will provide adequate cover in the future for infections that cause significant treatment failures so far, such as VRE- associated endocarditis, bone and joint multi-drug resistant infections and possibly central nervous system infections, both in adult and children populations. Some patents on linezolid are also discussed in this review.
, vancomycin-resistant Enterococcus faecalis and vancomycin-resistant Enterococcus faecium. It has an excellent bioavailability both intravenously and orally and a very good safety profile both in adults and in children. With regards to its antimicrobial action, linezolid has a predominantly bacteriostatic action, rather than a bacteriocidal effect and is active against Gram-positive bacteria that are resistant to other antibiotics. Linezolid is currently showing great promise for the treatment of multi-resistant Gram-positive infections, both in the community and in a hospital setting. Clinical indications so far include skin and soft tissue infections, community-acquired or nosocomial pneumonia due to MRSA, VRE bacteremia and community-acquired pneumonia due to penicillin-resistant Streptococcus pneumoniae. We anticipate that this new generation of antimicrobial agents will provide adequate cover in the future for infections that cause significant treatment failures so far, such as VRE- associated endocarditis, bone and joint multi-drug resistant infections and possibly central nervous system infections, both in adult and children populations. Some patents on linezolid are also discussed in this review.")
54
Pharmacotherapy. 2008 Apr;28(4):458-68.
Telavancin: an antimicrobial with a multifunctional mechanism of action for the treatment of serious gram-positive infections. Leonard SN, Rybak MJ. Source Anti-Infective Research Laboratory, Pharmacy Practice 4148, Eugene Applebaum College of Pharmacy and Health Sciences, Wayne State University, Detroit, MI 48201, USA. Abstract Telavancin is a once-daily lipoglycopeptide antibiotic structurally derived from vancomycin. It has broad-spectrum activity against gram-positive bacteria, including strains with reduced susceptibility to vancomycin. Telavancin's multifunctional mechanism of action, including inhibition of peptidoglycan synthesis and disruption of membrane potential, account for this enhanced activity as well as rapid bactericidal properties. In vitro activity has been demonstrated against a wide range of gram-positive pathogens such as multidrug-resistant Streptococcus pneumoniae, as well as methicillin-resistant, glycopeptide-intermediate, and vancomycin-resistant Staphylococcus aureus. The agent also displays activity against many gram-positive anaerobic organisms. Predictable linear pharmacokinetics have been demonstrated over a wide range of doses, with the most common adverse effects being taste disturbance and nausea. Clinical experience with telavancin in phase II and III studies for complicated skin and skin structure infections has shown it to have similar efficacy and tolerability compared with vancomycin and antistaphylococcal penicillins, and recently telavancin received an approvable letter from the United States Food and Drug Administration for this indication. Telavancin appears to be a promising agent for the treatment of serious infections caused by gram-positive pathogens, including drug-resistant pathogens. Further clinical experience will clarify its role in therapy.

Presentazioni simili








 064825120 - fax.>")















>")
