Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Critical Methological Issues in Recent Randomised Trials
MSO – ROMEa November 23, 2012 Critical Methological Issues in Recent Randomised Trials Paolo Bruzzi Epidemiologia Clinica IRCCS AUO San Martino IST

2
Topics Changes in the methodology of the Phases of cancer trials
Efficacy: Do we still need (Large) Randomised Controlled Trials? Perspectives ?
 Randomised Controlled Trials Perspectives")
3
Topics Changes in the methodology of the Phases of cancer trials
Efficacy: Do we still need (Large) Randomised Controlled Trials? Perspectives ?
 Randomised Controlled Trials Perspectives")
4
Conventional Methodology
- Phase I: dose increases -> MTD Phase II: Uncontrolled -> % Response in metastatic pts with a specific cancer Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
5
Conventional Methodology
- Phase I: dose increases -> MTD The More the Better? DOSE –RESPONSE! PHASE I-II TRIALS

6
Conventional Methodology
Phase II: Uncontrolled -> % Response in metastatic pts with a specific cancer

7
Conventional Methodology
Phase II: Uncontrolled -> % Response in metastatic pts with a specific cancer Response? Direct anticancer effect? Metastatic pts? Activity in pts with less disease burden Need of repeated biopsies

8
Modern Methodology Phase II trials: Biological Endpoints
Window-of-opportunity studies- Neoadjuvant trials – Locally advanced dis. Randomised Controls

9
Conventional Methodology
- Phase I: dose increases -> MTD Phase II: Uncontrolled -> % Response in metastatic pts with a specific cancer Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
10
Topics Changes in the methodology of the Phases of cancer trials
Efficacy: Do we still need (Large) Randomised Controlled Trials? Perspectives ?
 Randomised Controlled Trials Perspectives")
12
Conventional Methodology
- Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
13
Conventional Methodology
- Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
14
Conventional Methodology
- Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
15
Conventional Methodology
- Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
16
Conventional Methodology
- Phase III: Large RCT’s in relatively heterogeneous pts: OS (or EFS)
")
17
Reasons for the need of Randomised Control groups
Inability to predict individual outcome Inability to predict group outcome Inability to predict effect of treatments based on mechanisms

18
Reasons for the need of Randomised Control groups
Inability to predict individual outcome Inability to predict group outcome Inability to predict effect of treatments based on mechanisms STILL TRUE!

19
On the other hand ...

20
if a new drug, with a well-identified molecular target which is present in subgroups of cancers in different sites produces a strong benefit in one of these cancers, …it may become ETHICALLY unacceptable to run a randomised trial in other cancers with the same target

21
Example Mortality Tumor X Nil vs A 15% vs 12.5% N=12000 P = 0.0007
H0 Rejected: A is effective in X

22
Example Mortality Tumor X Nil vs A 15% vs 12.5% N=12000 P = 0.0007
Tumor Y Nil vs A % vs 7.5% N= P=0.066 H0 not rejected: A not shown effective in y

23
Prior Information: Mortality Tumor X Nil vs A 15% vs 12.5%
N= P = Tumor Y Nil vs A % vs 7.5% N= P=0.066

24
Prior Information: tumors X and Y are BRAF+
Mortality Tumor X Nil vs A 15% vs 12.5% N= P = Tumor Y Nil vs A % vs 7.5% N= P=0.066

25
Prior Information: tumors X and Y are BRAF+ A = Anti BRAF
Mortality Tumor X Nil vs A 15% vs 12.5% N= P = Tumor Y Nil vs A % vs 7.5% N= P=0.066 Interpretation?

26
Prior Information: tumors X and Y are BRAF+ A = Anti BRAF
I have to plan a trial in the rare tumor Z, which is usually BRAF+, and for which there is no effective treatment Do I need a randomised control group? Is it ethically acceptable?

27
GLEEVEC CML -> Large RCT GIST -> Large uncontrolled trial Chordomas -> Case Series

28
New paths to drug use Large RCT in a frequent cancer with the target - Proof of principle – Toxicity Uncontrolled (but formal) trial(s) in other cancers with the target Off label use in individual cases with the target
 trial(s) in other cancers with the target Off label use in individual cases with the target")
29
Acceptable? Methodology?
New paths to drug use Large RCT in a frequent cancer with the target - Proof of principle – Toxicity Uncontrolled (but formal) trial(s) in other cancers with the target Off label use in individual cases with the target Acceptable? Methodology?
 trial(s) in other cancers with the target Off label use in individual cases with the target Acceptable Methodology")
30
Topics Changes in the methodology of the Phases of cancer trials
Efficacy: Do we still need (Large) Randomised Controlled Trials? Perspectives?
 Randomised Controlled Trials Perspectives")
31
3. Perspectives Adaptive trials ‘Personalised’ Medicine
New Statistical Approaches

32
3. Perspectives Adaptive trials ‘Personalised’ Medicine New Statistical Approaches

33
3. Perspectives Radical changes in the way cancer trials are designed and analysed Adaptive trials ‘Personalised’ Medicine New Statistical Approaches

34
Three modern revolutions
1950 Randomized Clinical Trial Evidence Based Medicine 1990 Molecular Medicine

35
Three modern revolutions
1950 Randomized Clinical Trial Evidence Based Medicine 1990 Molecular Medicine

36
Preclinical work + Clinical observations
Empirical Approach Preclinical work + Clinical observations Clinical rationale

37
Preclinical work + Clinical observations
Empirical Approach Preclinical work + Clinical observations Clinical rationale CLINICAL STUDIES INTERPRETATION

38
Fondamenti della sperimentazione clinica randomizzata
Protezione da risultati falsamente positivi: Randomizzazione Protocolli rigidi/Piano statistico predeterminato Intention to treat (doppio cieco) Protezione da risultati falsamente negativi Dimensioni
 Protezione da risultati falsamente negativi. Dimensioni.")
39
Fondamenti della sperimentazione clinica randomizzata
Protezione da risultati falsamente positivi: Randomizzazione Protocolli rigidi/Piano statistico predeterminato Intention to treat (doppio cieco) Protezione da risultati falsamente negativi Dimensioni
 Protezione da risultati falsamente negativi. Dimensioni.")
40
RCT -> EBM in Oncology Golden Age
Rigid protocols Drugs – Doses – Cycles Modifications for toxicity or progression/relapse Generic Selection Criteria Site (e.g. Stomach) Histology (ADK vs Lymphoma) Stage (early vs late)
 Histology (ADK vs Lymphoma) Stage (early vs late)")
41
RCT -> EBM in Oncology Golden Age
Large and Simple Clinical Trials - Systematic Reviews – Meta-analyses Clinical Guidelines/Recommendations – Generic Flexibility in pt management not considered

42
Evidence Based Medicine ≈ Cookbook Medicine?

43
New Century Patients Heterogeneity New Approaches!
Technological advances – Discoveries Cellular functions Molecular mechanisms/pathways Genes/Mutations /Gene Functions Genomics/Proteomics/(Metabolomics) Targeted Drugs Patients Heterogeneity New Approaches!
 Targeted Drugs. Patients Heterogeneity. New Approaches!")
44
3. Perspectives Adaptive trials ‘Personalised’ Medicine
New Statistical Approaches

45
a) Adaptive design FDA’s draft guidance for industry on adaptive design clinical trials (

47
Adaptive design clinical trial
FDA’s Definition: “… a study that includes a prospectively planned opportunity for modification of one or more specified aspects of the study design and hypotheses based on analysis of data (usually interim data) from subjects in the study”
 from subjects in the study")
48
Why adaptive designs are so attractive?
Early Responses Effects in Subgroups of patients Toxicity It is possible to obtain, during the trial, crucial information to improve some of its design features

49
Most conventional trials have an adaptive component
Stopping rules based on interim analyses: Toxicity Rejection of null-hypothesis Futility

50
Conventional Trials Few, if any, planned interim analyses
Change selection criteria ? Change treatment protocol ? NO Change of the Endpoint NO Change of the Statistical Plan

51
Adaptive designs Interim analyses critical in study design
Change selection criteria Change treatment protocol Change Endpoint Change Statistical Plan

52
Adaptive designs Interim analyses Change selection criteria (target)
Change treatment protocol Change Endpoint Change Statistical Plan

53
3. Perspectives Adaptive trials ‘Personalised’ Medicine
New Statistical Approaches

54
Adaptive designs Interim analyses Change selection criteria (target)
Change treatment protocol Change Endpoint Change Statistical Plan

55
3. Perspectives Adaptive trials ‘Personalised’ Medicine
New Statistical Approaches

56
New Statistical approaches
Bayesian statistics (rare tumors and subgroups) Changing the null hypothesis (Sobrero & Bruzzi, ) Statistical methods for uncontrolled trials
 Changing the null hypothesis (Sobrero & Bruzzi, ) Statistical methods for uncontrolled trials.")
57
New Statistical approaches
Bayesian statistics (rare tumors and subgroups) Changing the null hypothesis (Sobrero & Bruzzi, ) Statistical methods for uncontrolled trials
 Changing the null hypothesis (Sobrero & Bruzzi, ) Statistical methods for uncontrolled trials.")
58
Metodologia dei trials clinici: Elementi critici
Primary Aim(s) Endpoint(s) Selection of patients Study Design Randomization Assessment of outcome Statistics (Statistical plan, ITT analysis)
 Endpoint(s) Selection of patients. Study Design. Randomization. Assessment of outcome. Statistics (Statistical plan, ITT analysis)")
59
Metodologia dei trials clinici: Prospettive
Validita’ Interna (Statistica) = Assenza di bias Validita’ Esterna = Implicazioni Generalizzazioni (Proof of Principle) Applicazioni (pratica clinica, sanita’, ricerca,…)
 = Assenza di bias. Validita’ Esterna. = Implicazioni. Generalizzazioni (Proof of Principle) Applicazioni (pratica clinica, sanita’, ricerca,…)")
60
Metodologia dei trials clinici: Elementi critici
Primary Aim(s) Endpoint(s) Selection of patients Study design Randomization Assessment of outcome Statistics (Statistical plan, ITT analysis) Validita’ Interna (Assenza di Bias)
 Endpoint(s) Selection of patients. Study design. Randomization. Assessment of outcome. Statistics (Statistical plan, ITT analysis) Validita’ Interna (Assenza di Bias)")
61
Industry-Sponsored Trials
} Randomizzazione Valutazione outcome Statistica I moderni trial dell’industria, nella stragrande maggioranza, sono studi di altissima qualita’, privi di bias rilevanti Tecnicamente perfetti !

62
Metodologia dei trials clinici: Elementi critici
Primary Aim(s) Endpoint(s) Selection of patients Study Design Randomization Assessment of outcome Statistics (Statistical plan, ITT analysis)
 Endpoint(s) Selection of patients. Study Design. Randomization. Assessment of outcome. Statistics (Statistical plan, ITT analysis)")
63
Metodologia dei trials clinici: Elementi critici
Scopo/i Primario/i Endpoint(s) Selezione dei pazienti Disegno di studio ‘Validita’ Esterna’ = = Rilevanza Clinica e di Sanita’ Pubblica
 Selezione dei pazienti. Disegno di studio. ‘Validita’ Esterna’ = = Rilevanza Clinica e di Sanita’ Pubblica.")
64
1. Scopo Possibili scopi di un Trial Clinico Valutare:
(Attivita’ – meccanismi -> Fase II) Efficacy (proof of principle) Effectiveness (benefici clinici concreti)
 Efficacy (proof of principle) Effectiveness (benefici clinici concreti)")
65
Industry-Sponsored Trials
Scopo Primario: Rifiutare l’ipotesi nulla H0: P<0.05 H0: Trattamento Sperimentale (con/senza treatment (with/without standard) identico allo Standard
 identico allo Standard.")
72
Significativita’ Statistica
P = Probabilita’ di osservare, per caso, un differenza grande quanto quella osservata o piu’ grande se i due trattamenti sono identici (H0) Nota: Nei trials di fase III, H0 spesso non plausibile (precedenti trials di fase II, in altre malattie/stadi)
 Nota: Nei trials di fase III, H0 spesso non plausibile. (precedenti trials di fase II, in altre malattie/stadi)")
73
Significativita’ Statistica
P = Probabilita’ di osservare, per caso, un differenza grande quanto quella osservata o piu’ grande se i due trattamenti sono identici (H0) Rilevanza Clinica: Beneficio per i pazienti sufficiente per far adottare il trattamento sperimentale come standard (considerando costi, tossicita’, rischi)
 Rilevanza Clinica: Beneficio per i pazienti sufficiente per far adottare il trattamento sperimentale come standard (considerando costi, tossicita’, rischi)")
74
Trials Sponsorizzati dalle industrie farmaceutiche
1. Scopo: Trovare una differenza statisticamente significativa 2. Endpoint 3. Criteri di Selezione 4. Disegno di Studio Sample Size Collocazione temporale delle analisi

75
2. Endpoints Endpoints naturali nei trials di efficacia:
= Scopi del trattamento: Aumentare Quantita’ e/o di vita Qualita’

76
2. Endpoints Endpoints naturali nei trials di efficacia:
Overall Survival Quality of Life (Qualy)
")
77
2. Endpoints Endpoints spesso usati nei trials di efficacia:
Endpoints di attivita’ Endpoints Surrogati non sempre validati

78
Endpoints Surrogati in oncologia
Relapse-Free Survival, Disease-Free Survival nella malattia operata Progression-Free Survival nella malattia metastatica

79
Perche’ i trials dell’industria si basano cosi’ fortemente su endpoints surrogati ?

80
Perche’ i trials dell’industria si basano cosi’ fortemente su endpoints surrogati ?
Per abbreviare il tempo alle analisi ad interim e finale (piu’ eventi) (Basterebbe aspettare) Effetto piu’ forte! soprattutto nel periodo iniziale del follow-up - Maggiore potenza e ‘rilevanza clinica’
 (Basterebbe aspettare) Effetto piu’ forte! soprattutto nel periodo iniziale del follow-up - Maggiore potenza e ‘rilevanza clinica’")
81
3. Popolazione in studio Pazienti selezionati (es. Eta’) Compliance
Suscettibili agli effetti del trattamento Meno sensibili alla tossicita’ Massimizzare gli effetti del trattamento Possibilita’ di extrapolare a popolazioni di pazienti differenti? (Trials adiuvanti nel BC - eta’ mediana : 50years)
")
82
4. Disegno di Studio a) Sample Size
b) Timing delle analisi ad interim e finale
 Timing delle analisi ad interim e finale.")
83
4. Study Design a) Sample Size : Aumentando le dimensioni dello studio, differenze Clinicamente poco importanti -> Statisticamente significative Es. Molti farmaci ‘targeted’ con effetti sul PFS<3 mesi in vari tumori solidi e p<0.001

84
Conventional Trial HR =0.8 Power= 80% 635 events MCWE, H1
No Difference, H0 HR =0.8 Power= 80% 635 events HR=0.86 P=0.05 HR

85
Conventional Trial HR =0.8 Power= 95% 1050 events MCWE, H1
No Difference, H0 HR =0.8 Power= 95% 1050 events HR=0.89 P=0.05 HR

86
Conventional Trials HR =0.8 Power= 95% 1050 events MCWE, H1
No Difference, H0 HR =0.8 Power= 95% 1050 events HR=0.89 Confidence Limits: From No Effect to MCWE HR

87
P<0.03

88
4. Study design b) Timing delle analisi: Interim Analisi precoci
Effetti precoci molto plausibili (Attivita’) Effetti maggiori e minore focalizzazione sui fallimenti a lungo termine (tumori avanzati) Minore focalizzazione sulla tossicita’ a lungo termine (malattia precoce)
 Effetti maggiori e minore focalizzazione sui fallimenti a lungo termine (tumori avanzati) Minore focalizzazione sulla tossicita’ a lungo termine (malattia precoce)")
89
Typical treatment effect in advanced solid tumors
Interim Analysis

90
Interim analyses I metodi di correzione della p usati nella analisi ad interim servono a preservare solo l’errore alfa Per vari motivi statistici, gli studi interrotti per interim analisi positive tendono a fornire SOVRASTIME dell’efficacia del trattamento sperimentale Queste stime quindi non dovrebbero essere usate per valutazioni cliniche e costi/benefici

91
Case-study: Aromatase Inhibitors in early breast cancer
Three original papers Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial - Lancet 2002 A Randomized Trial of Letrozole in Postmenopausal Women after Five Years of Tamoxifen Therapy for Early-Stage Breast Cancer – NEJM Nov. 2003 A Randomized Trial of Exemestane after two to three years of Tamoxifen therapy in postmenopausal women with primary Breast Cancer – NEJM March 2004

92
Trials results (1st analysis)
Stage Sample Size F-up Events DFS red. % Tam vs Anastrovs A+T Postmenop 61% N- 84% HR+ 6200 (2/3 arms) 2.7 years 696 -17% (-14%) Letro vs Placebo 5-yrs Tam Postm ER+ 50% N- 5187 2.4 years 207 (73) - 43% Tam vs Exem. 2-3yrs Tam Postm/ER+? 51% N- 4742 2.5 years 449 (199) -32%
 2.7 years % (-14%) Letro vs Placebo. 5-yrs Tam. Postm ER+ 50% N years. 207 (73) - 43% Tam vs. Exem. 2-3yrs Tam. Postm/ER+ 51% N years. 449 (199) -32%")
93
Effetti - a lungo termine? - su mortalita’?
Cross-over programmato Altre terapie Diluzione effetto? Tecniche statistiche non ITT

94
Ultima Generazione di trials sponsorizzati dall’industria
Trials sovradimensionati per garantire P significativa ad effetti moderati Analisi concentrate su endpoints surrogati e/o nelle analisi ad interim Effetti precoci spesso plausibili, ma benefici e tossicita’ a lungo termine? Endpoints Surrogati + Interim Analyses: Sovrastima del beneficio?

95
Trials sponsorizzati dall’ Industria
I moderni trials: virtualmente privi di difetti dal punto di vista metodologico e statistico Disegnati per massimizzare la probabilita’ di osservare un effetto ‘statisticamente signficativo’ del farmaco sperimentale, a prescindere dalla rilevanza clinica dell’effetto ‘reale’

96
Trials sponsorizzati dall’ Industria (2)
Questi trials forniscono una prospettiva distorta sulla reale efficacia dei nuovi farmaci Ciononostante, sulla base di questi risultati, spesso le agenzie regolatorie approvano questi farmaci, scaricando il problema degli alti costi x benefici limitati sui sistemi sanitari locali

97
Soluzioni? Trials Indipendenti (?)
Contrattazione ‘forte’ tra agenzie sanitarie-comunita’ scientifica internazionale e Big Pharma Nuovi requisiti per l’approvazione dei farmaci

98
Proposals of new statistical designs for phase III cancer trials A
Proposals of new statistical designs for phase III cancer trials A. Sobrero, P. Bruzzi

99
Sintesi della proposta
Trials di efficacia Scopo : rifiutare H0: Delta < MCWE (Minimal Clinically Worthwhile Effect)
")
100
Example Metastatic Colorectal Cancer
Expected Overall Survival: 24 months Experimental treatment: Limited toxicity and costs MCWE: increase in OS = 3 months (HR= 0.9)
")
101
New proposal MCWE, H0 LIMBO H0: No effect Discard APPROVE
HR

102
Issues to discuss Choice of the MCWE P value computation
Power/required sample size Analysis and interpretation of the results Adaptive designs/Interim analyses

103
Conclusione La metodologia delle sperimentazioni cliniche e dell’intero processo di sviluppo delle terapie oncologiche e’ destinata a modificarsi radicalmente nei prossimi anni per rispondere alle esigenze che derivano dai progressi nella quantita’ e nel tipo delle conoscenze disponibili

104
Processo di sviluppo delle nuove metodologie Esperti + Stakeholders
Pazienti (assoc.) Clinici Ricercatori Statistici Agenzie Regolatorie Cost-efficacy
 Clinici. Ricercatori. Statistici. Agenzie Regolatorie. Cost-efficacy.")
106
Bevacizumab (BEV) plus chemotherapy (CT) continued beyond first progression in patients with metastatic colorectal cancer (mCRC) previously treated with BEV + CT: Results of a randomised phase III intergroup study – TML (ML18147) D Arnold1, T Andre2, J Bennouna3, J Sastre4, P Österlund5, R Greil6 E Van Cutsem7, R von Moos8, I Reyes-Rivera9, B Bendahmane10, S Kubicka11 on behalf of the AIO, GERCOR, FFCD, UNICANCER GI, TTD, GEMCAD and AGMT groups 1Hamburg, Germany; 2Paris, France; 3Nantes, France; 4Madrid, Spain 5Helsinki, Finland; 6Salzburg, Austria; 7Leuven, Belgium; 8Chur, Switzerland 9South San Francisco, USA; 10Basel, Switzerland; 11Reutlingen, Germany

107
Aims and objectives The efficacy and safety of BEV continued after first PD has not been investigated in a randomised clinical trial TML (ML18147) is the first randomised phase III study to evaluate BEV continued with standard second-line CT in patients with mCRC who progressed after BEV plus standard first-line CT
 is the first randomised phase III study to evaluate BEV continued with standard second-line CT in patients with mCRC who progressed after BEV plus standard first-line CT.")
108
Statistical considerations
Study initiated as AIO KRK 0504 then transferred to Roche (after enrolment of 261 patients) Primary endpoint changed from PFS to OS Sample size increased from 572 to 810 patients Designed to detect 30% (HR 0.77) improvement in median OS (90% power, 2- sided 5%) 613 events required for analysis OS curves estimated using Kaplan–Meier method, differences assessed using unstratified log-rank tests Unstratified Cox regression model used to estimate HR for OS Stratified log-rank tests and Cox regression analyses used as supportive analyses
 Primary endpoint changed from PFS to OS. Sample size increased from 572 to 810 patients. Designed to detect 30% (HR 0.77) improvement in median OS (90% power, 2- sided 5%) 613 events required for analysis. OS curves estimated using Kaplan–Meier method, differences assessed using unstratified log-rank tests. Unstratified Cox regression model used to estimate HR for OS. Stratified log-rank tests and Cox regression analyses used as supportive analyses.")
109
Main eligibility criteria
Inclusion Patients ≥18 years with histologically confirmed diagnosis of mCRC Eastern Cooperative Oncology Group (ECOG) PS 0–2 PD (≥1 measurable lesion according to RECIST v1 assessed by investigator, documented by CT or MRI), ≤4 weeks prior to start of study treatment Previously treated with BEV plus standard first-line CT, not candidates for primary metastasectomy Exclusion Diagnosis of PD >3 months after last BEV administration First-line patients with PFS in first-line of <3 months Patients receiving <3 consecutive months of BEV in first-line
 PS 0–2. PD (≥1 measurable lesion according to RECIST v1 assessed by investigator, documented by CT or MRI), ≤4 weeks prior to start of study treatment. Previously treated with BEV plus standard first-line CT, not candidates for primary metastasectomy. Exclusion. Diagnosis of PD >3 months after last BEV administration. First-line patients with PFS in first-line of <3 months. Patients receiving <3 consecutive months of BEV in first-line.")
110
Demographic and baseline characteristics: Randomised patients
BEV + CT (n=409) Male, % 63 65 Age, median years ECOG performance status, % 1 2 First-line PFS, % ≤9 months >9 months 56 44 54 46 First-line CT, % Irinotecan-based Oxaliplatin-based 58 42 59 41 Patients were accrued between February 2006 and June 2010
 Male, % Age, median years. ECOG performance status, % First-line PFS, % ≤9 months >9 months First-line CT, % Irinotecan-based. Oxaliplatin-based Patients were accrued between February 2006 and June")
111
Demographic and baseline characteristics: Randomised patients (cont’d)
BEV + CT (n=409) Duration from last BEV dose to randomisation, % ≤42 days >42 days 77 23 Patient populationa, % AIO ML18147 32 68 Liver metastasis only, % No Yes 71 29 73 27 No. of organs with metastasis, % 1 >1 39 61 36 64 aPatient population refers to sequential enrolment of patients in original AIO study and subsequent enrolment in ML18147 when study was transferred to Roche
 Duration from last BEV dose to randomisation, % ≤42 days >42 days Patient populationa, % AIO ML Liver metastasis only, % No Yes No. of organs with metastasis, % 1 > aPatient population refers to sequential enrolment of patients in original AIO study and subsequent enrolment in ML18147 when study was transferred to Roche.")
112
Second-line chemotherapy during study: Randomised patients
Second-line CT regimen, % CT (n=407) BEV + CT Irinotecan-based CT 43 42 FOLFIRI 14 16 LV5FU2 + CPT11 (Douillard regimen1) 7 XELIRI 12 Other regimens 10 Oxaliplatin-based CT 57 58 FOLFOX4 / mFOLFOX4 18 19 FOLFOX6 13 FUFOX 9 6 XELOX 11 4 1. Douillard et al. Lancet 2000;355:1041–7
 BEV + CT. Irinotecan-based CT FOLFIRI LV5FU2 + CPT11 (Douillard regimen1) 7. XELIRI. 12. Other regimens. 10. Oxaliplatin-based CT FOLFOX4 / mFOLFOX FOLFOX FUFOX XELOX Douillard et al. Lancet 2000;355:1041–7.")
113
Primary endpoint: overall survival

114
OS: ITT population CT (n=410) 1.0 BEV + CT (n=409) 0.8
OS estimate Time (months) 1.0 0.8 0.6 0.4 0.2 No. at risk CT BEV + CT CT (n=410) BEV + CT (n=409) 9.8 mo 11.2 mo Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p= (log-rank test) Stratifiedb HR: 0.83 (95% CI: 0.71–0.97) p= (log-rank test) Median follow-up: CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0) aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)
 No. at risk. CT BEV + CT CT (n=410) BEV + CT (n=409) 9.8 mo mo. Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p= (log-rank test) Stratifiedb HR: 0.83 (95% CI: 0.71–0.97) p= (log-rank test) Median follow-up: CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0) aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)")
115
Subsequent anti-cancer therapies: Safety population
Subsequent therapy, % CT (n=409) BEV + CT (n=401) Patients who received ≥1 subsequent anti-cancer therapy 67.7 68.6 Subsequent anti-cancer therapies BEV 12.2 11.5 Anti-EGFR 41.3 39.2 Other 50.4 54.9 EGFR: epidermal growth factor receptor
 BEV + CT (n=401) Patients who received ≥1 subsequent anti-cancer therapy Subsequent anti-cancer therapies. BEV Anti-EGFR Other EGFR: epidermal growth factor receptor.")
116
Subgroup analysis of OS: ITT population
Category Subgroup n HR (95% CI) All 819 0.81 (0.69–0.94) Patient populationa AIO 260 0.86 (0.67–1.11) ML18147 559 0.78 (0.64–0.94) Gender Female 294 0.99 (0.77–1.28) Male 525 0.73 (0.60–0.88) Age <65 years 458 0.79 (0.65–0.98) ≥65 years 361 0.83 (0.66–1.04) ECOG performance status 357 0.74 (0.59–0.94) ≥1 0.87 (0.71–1.06) First-line PFS ≤9 months 449 0.89 (0.73–1.09) >9 months 369 0.73 (0.58–0.92) First-line CT Oxaliplatin-based 343 0.79 (0.62–1.00) Irinotecan-based 476 0.82 (0.67–1.00) Time from last BEV ≤42 days 630 0.82 (0.69–0.97) >42 days 189 0.76 (0.55–1.06) Liver metastasis only No 592 0.81 (0.67–0.97) Yes 226 0.79 (0.59–1.05) No. of organs with metastasis 1 307 0.83 (0.64–1.08) >1 511 0.77 (0.64–0.94) HR 0 1 2 aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when study was transferred to Roche. All patients listed under AIO were included in primary analysis
 All (0.69–0.94) Patient populationa. AIO (0.67–1.11) ML (0.64–0.94) Gender. Female (0.77–1.28) Male (0.60–0.88) Age. <65 years (0.65–0.98) ≥65 years (0.66–1.04) ECOG performance status (0.59–0.94) ≥ (0.71–1.06) First-line PFS. ≤9 months (0.73–1.09) >9 months (0.58–0.92) First-line CT. Oxaliplatin-based (0.62–1.00) Irinotecan-based (0.67–1.00) Time from last BEV. ≤42 days (0.69–0.97) >42 days (0.55–1.06) Liver metastasis only. No (0.67–0.97) Yes (0.59–1.05) No. of organs with metastasis (0.64–1.08) > (0.64–0.94) HR aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when study was transferred to Roche. All patients listed under AIO were included in primary analysis.")
117
Subgroup analysis of PFS (ITT population)
Category Subgroup n HR (95% CI) All 819 (0.59–0.78) Patient populationa AIO 260 (0.51–0.84) ML18147 559 (0.58–0.82) Gender Female 294 (0.67–1.07) Male 525 (0.50–0.72) Age <65 years 458 (0.55–0.80) ≥65 years 361 (0.57–0.87) ECOG PS 357 (0.48–0.74) ≥1 (0.63–0.92) First-line PFS ≤9 months 449 (0.62–0.90) >9 months 369 (0.47–0.72) First-line CT Oxaliplatin-based 343 (0.55–0.85) Irinotecan-based 476 (0.56–0.81) Time from last BEV ≤42 days 630 (0.61–0.85) >42 days 189 (0.41–0.75) Liver metastasis only No 592 (0.57–0.80) Yes 226 (0.52–0.89) No. of organs with metastasis 1 307 (0.59–0.94) >1 511 (0.53–0.77) HR 0 1 2 aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when study transferred to Roche. All patients listed under AIO were included in primary analysis
 All (0.59–0.78) Patient populationa. AIO (0.51–0.84) ML (0.58–0.82) Gender. Female (0.67–1.07) Male (0.50–0.72) Age. <65 years (0.55–0.80) ≥65 years (0.57–0.87) ECOG PS (0.48–0.74) ≥ (0.63–0.92) First-line PFS. ≤9 months (0.62–0.90) >9 months (0.47–0.72) First-line CT. Oxaliplatin-based (0.55–0.85) Irinotecan-based (0.56–0.81) Time from last BEV. ≤42 days (0.61–0.85) >42 days (0.41–0.75) Liver metastasis only. No (0.57–0.80) Yes (0.52–0.89) No. of organs with metastasis (0.59–0.94) > (0.53–0.77) HR aPatient population refers to sequential enrolment of patients in original AIO and subsequent enrolment in ML18147 when study transferred to Roche. All patients listed under AIO were included in primary analysis.")
118
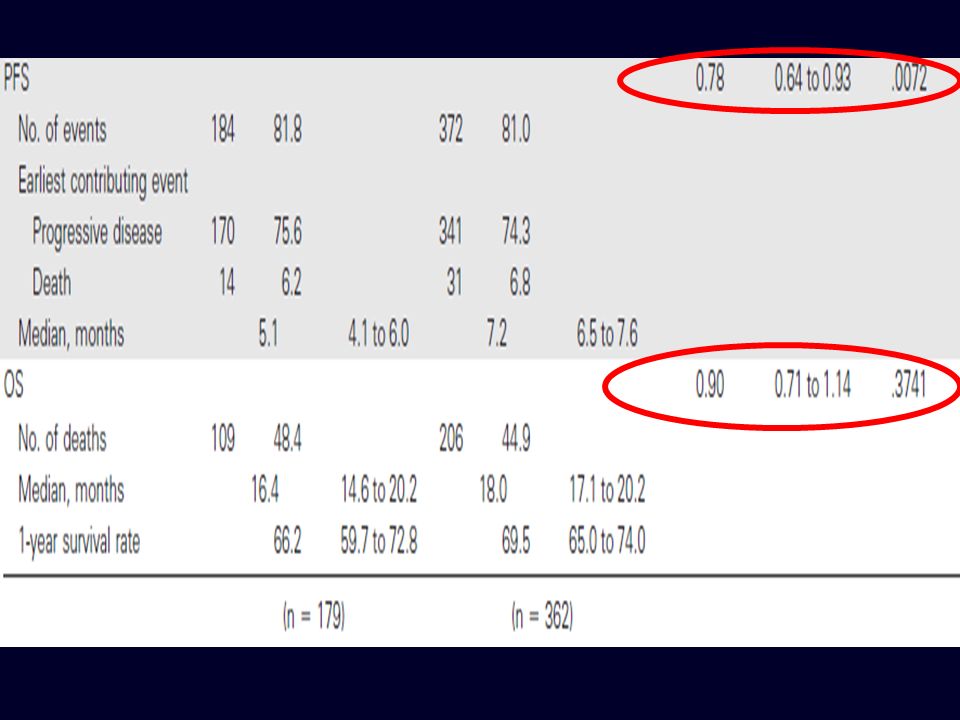
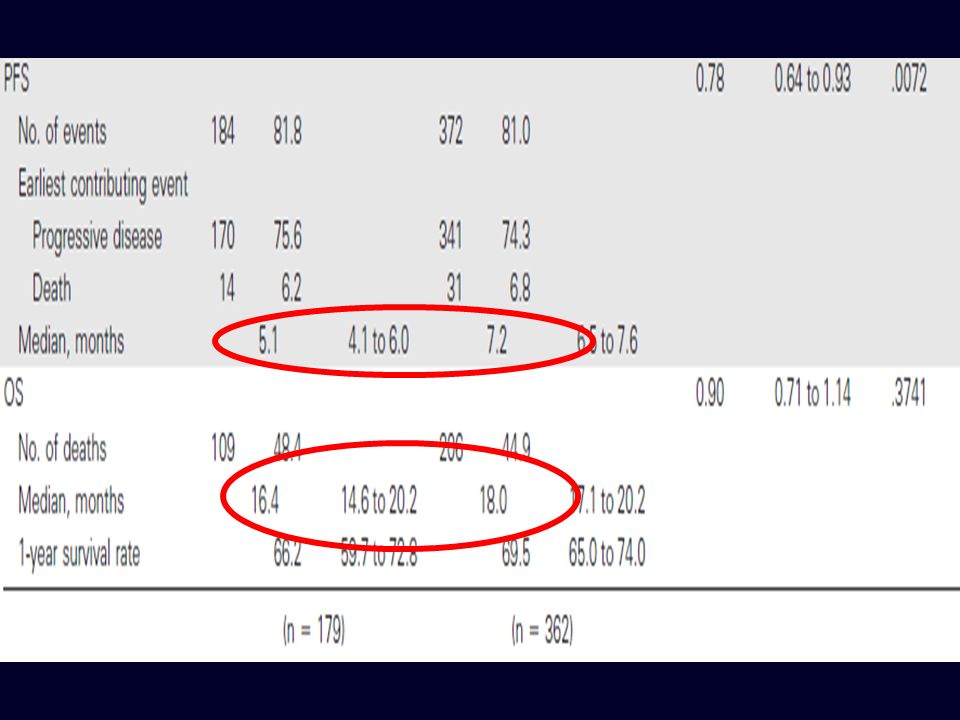
Summary BEV + standard second-line CT, crossed over from BEV + standard first-line CT, significantly prolongs OS and PFS OS Median: BEV + CT 11.2 months, CT 9.8 months HR: 0.81 (95% CI: 0.69–0.94), p=0.0062a PFS Median: BEV + CT 5.7 months, CT 4.1 months HR: 0.68 (95% CI: 0.59–0.78), p≤0.0001a Findings from subgroup analyses for OS generally consistent with overall population Treatment effect according to gender appeared to be different; however, treatment-gender interaction test was not statistically significant Differences in best overall response rate not statistically significant; low response rate in both treatment groups AEs not increased when continuing BEV beyond PD; AE profile consistent with previous findings
, p=0.0062a. PFS. Median: BEV + CT 5.7 months, CT 4.1 months. HR: 0.68 (95% CI: 0.59–0.78), p≤0.0001a. Findings from subgroup analyses for OS generally consistent with overall population. Treatment effect according to gender appeared to be different; however, treatment-gender interaction test was not statistically significant. Differences in best overall response rate not statistically significant; low response rate in both treatment groups. AEs not increased when continuing BEV beyond PD; AE profile consistent with previous findings.")
119
Conclusions First randomised clinical trial that prospectively investigated the impact of continued VEGF inhibition with BEV beyond first progression Study confirms that continuing BEV beyond first progression while modifying CT is beneficial for patients with mCRC and leads to a significant improvement in OS and PFS This provides a new second-line treatment option for patients who have been treated with BEV + standard CT in first line while maintaining an acceptable safety profile Findings indicate a potential new model for treatment approaches through multiple lines and this is currently being investigated in other tumour types

120
OS: ITT population 9.8 mo 11.2 mo CT (n=410) 1.0 BEV + CT (n=409) 0.8
OS estimate Time (months) 1.0 0.8 0.6 0.4 0.2 No. at risk CT BEV + CT CT (n=410) BEV + CT (n=409) 9.8 mo 11.2 mo Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p= (log-rank test) Stratifiedb HR: 0.83 (95% CI: 0.71–0.97) p= (log-rank test) Median follow-up: CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0) aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)
 No. at risk. CT BEV + CT CT (n=410) BEV + CT (n=409) 9.8 mo mo. Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p= (log-rank test) Stratifiedb HR: 0.83 (95% CI: 0.71–0.97) p= (log-rank test) Median follow-up: CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0) aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)")
125
Long term benefit?

126
Long term benefit?

127
Long term benefit? 2 mos

128
2-3 months 3.5 months

129
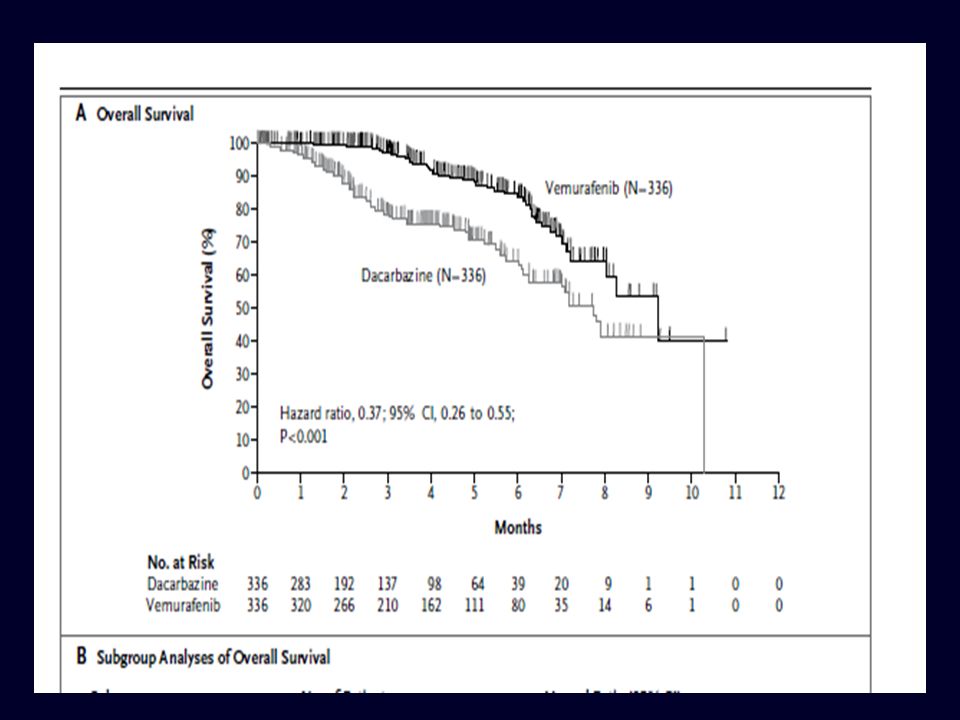
Clinically Worthwhile Effect?
Median follow-up: 3.8 vs 2.3 months HR = 0.37 ( ): Meaningless! Long term benefit: None (Mature data?) Increase in median survival: ≈ 2 months Average benefit:< 2 months 30% of the pts: 3 months 30% of the pts: 2 months 40% of the pts: 0 } Clinically worthwhile?
: Meaningless! Long term benefit: None (Mature data ) Increase in median survival: ≈ 2 months. Average benefit:< 2 months. 30% of the pts: 3 months. 30% of the pts: 2 months. 40% of the pts: 0. } Clinically worthwhile")
130
Conclusions The medical research community should rethink the terms of cooperation with industry in clinical trials, taking into account a wider clinical and public health perspective.

131
Conclusions The medical research community should rethink the terms of cooperation with industry in clinical trials, taking into account a wider clinical and public health perspective. Our health systems risk bankruptcy for the skyrocketing costs of drugs that were developed on their own patients, using strategies that ignore the patients’ needs and priorities.

132
Conclusions The medical research community should rethink the terms of cooperation with industry in clinical trials, taking into account a wider clinical and public health perspective. Our health systems risk bankruptcy for the skyrocketing costs of drugs that were developed on their own patients, using strategies that ignore the patients’ needs and priorities. Governments, health systems, and regulatory agencies must identify new paths for drug development and set new standards for drug approval

Presentazioni simili

























>")