Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Treatment of very young women
Marina Guenzi Oncolgia Radioterapica Genova

2
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

3
problematiche da affrontare nelle pazienti giovani:
Secondi Tumori Radio-indotti BRCA mutation Gravidanza e neoplasia mammaria

4
Incidenza Fattori prognostici Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

5
most series recognize patients ≤35 years old as a “young” population.
Establishing the definition of “young” patients with breast cancer has been the subject of some controversy women “35 to 40 years of age or younger” defined a group of patients in which age was an independent risk factor for higher rates of recurrence the MEDLINE and CancerLit databases most series recognize patients ≤35 years old as a “young” population. Beadle et al., 2011

6
Breast cancer is rare in very young women.
Breast cancer in women ≤40 years of age is relatively uncommon, reflecting only 5% of new breast cancers from 2002 to 2006. Breast cancer is rare in very young women. Only 1.9% of all breast cancers occur in women 35 years, but the diagnosis is physically and emotionally devastating for these women Further data indicate that women aged 20 to 24 had the lowest breast cancer incidence rate, with 1.4 cases per 100,000 women. American Cancer Society,2010

7
2010

8
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

9
Regardless of the definition most series suggest a worse prognosis in young women compared with older women Age, tumor size, margins, systemic treatment Cefaro A.G, 2006 Age, EIC, margins Horst KD, 2005 Age, margins Leong C, 2004 Age, margins, chemotherapy, tamoxifene Livi L, 2007 Age, ductal and ductal plus lobular histotypes, 3 positive nodes Livi L, 2010

10
The reasons for these higher rates of recurrence are unclear….
young women tend to have more triple-negative and fewer luminal A and B breast cancers Carey LA, 2006 Cancello G, 2010 Bauer KR, 2007 young women tend to have tumors that are higher grade, have more extensive intraductal component, more lymphovascular space invasion, and are likely estrogen receptor (ER)-negative Nixon AJ, 1994 Kutz JM, 1990 Albain KS, 1994 Leborgne F, 1994
-negative. Nixon AJ, Kutz JM, Albain KS, Leborgne F,")
11
Breast tumors arising in younger women may be more enriched for aggressive subtypes and age-specific biologic differences observed in breast carcinomas may be highly subtype dependent. Anders CK, JCO 2008 Perou CM, Nature 2000

12
However, even after adjustment of those prognostic factors, women aged 35 or younger still have a worse prognosis. Therefore, the unfavorable common prognostic criteria cannot be the only explanation for the more aggressive disease. Different gene expression profiles could explain the differences between the young and the elderly. Anders et al revealed 367 biologically relevant gene sets significantly distinguishing breast tumors arising in young women and concluded that this could define a unique biologic entity.

13
prognosi sfavorevole…
perché è una donna giovane O per aggressività biologica e quindi prognosi sfavorevole

14
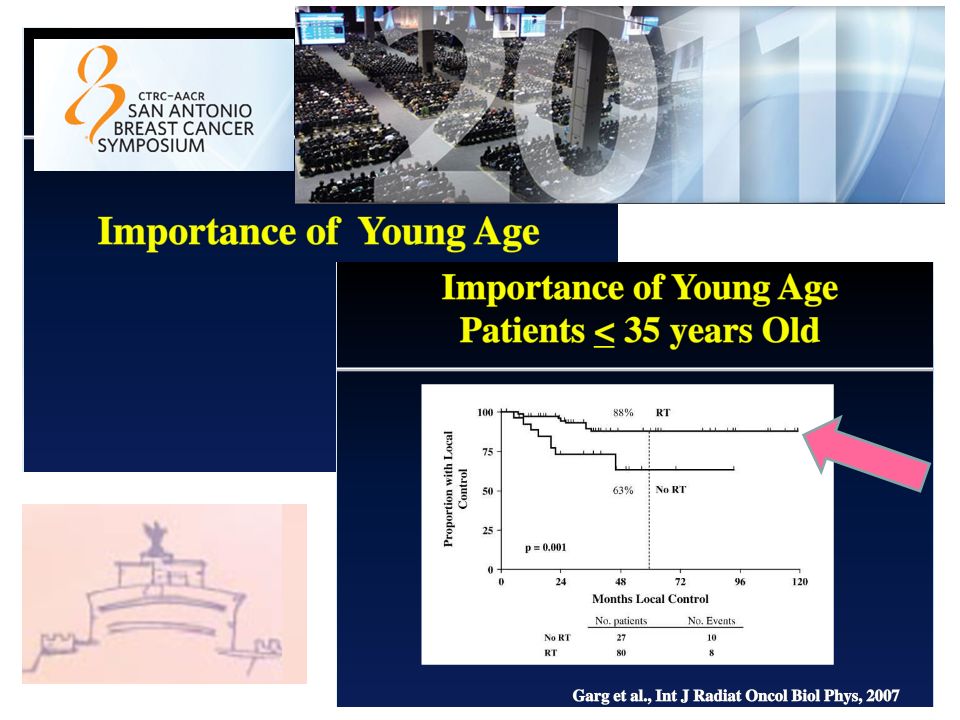
Worse outcome in local control and….
the risk of dying of breast cancer within 5 years of diagnosis in women aged younger than 35 with Stage I–IIb breast cancer has been reported to be 1.8-fold higher than in women aged 50 to 69 years Fredholm H, 2009 this age group showed a significantly worse outcome compared with older premenopausal women, and their risk of death rose by 5% for every 1-year reduction in age. Han W, Breast Cancer Res Treat 2009

15
This negative impact on survival was especially seen in patients with positive lymph nodes and those with positive hormonal receptors, underlining the key role of hormonal mechanisms in young patients with breast cancer. El Shagir NS, BMC Cancer 2006

16
It should be noted that in spite of the still poorer prognosis compared with older women, mortality in the younger age group decreased between 2000 and 2004 by around 30% (10 years follow up). This effect can partly be explained by the fact that younger patients are highly motivated and often have access to innovative therapeutic strategies, especially in clinical trials. Katalinic A, Breast Care 2009

17
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

18
Young women have a higher density of the glandular parenchyma, making it more difficult to differentiate between tumors and normal breast tissue by mammography. Sonography is more sensitive than mammography in evaluating breast masses in women younger than 45 making it more difficult to differentiate between tumors and normal breast tissue by mammography. Preoperative MRI did not reduce the reoperation rate may not be necessary and can result in extra use of resources with little or no benefit to residual health Steffi Hartmann, Clinical Breast Cancer 2011

19
digital mammography and histologic assessment.
In symptomatic young women, breast ultrasound should be the diagnostic method of choice and in case of a suspicious finding it should be supplemented by digital mammography and histologic assessment. In case of conventional imaging difficulties because of dense tissue, preoperative MRI may provide benefit in very young patients with breast cancer Steffi Hartmann, Clinical Breast Cancer 2011

20
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

21
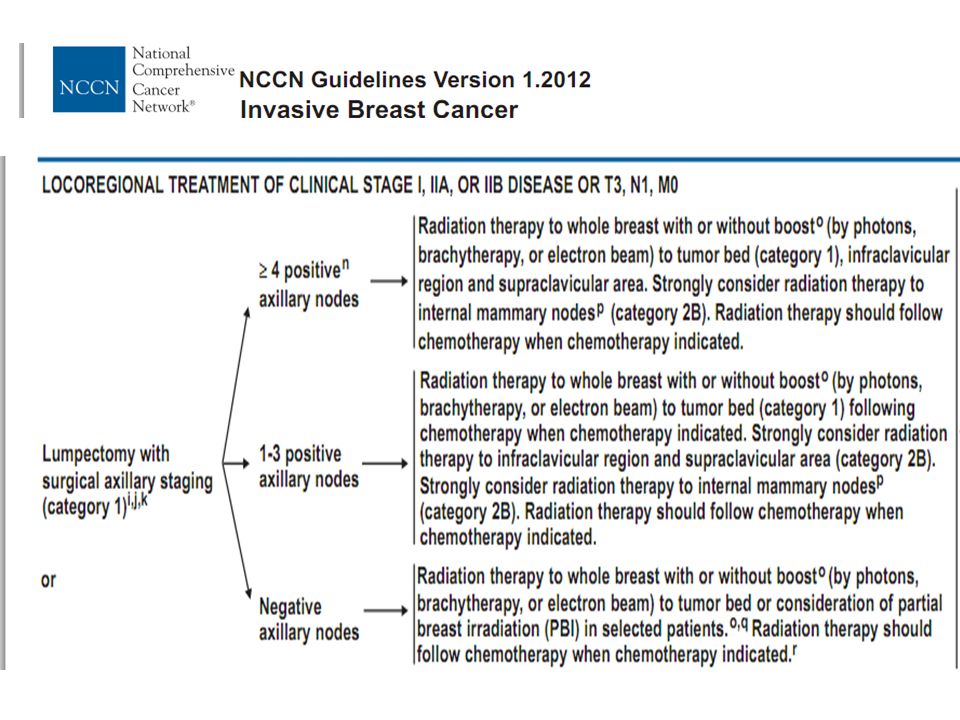
Surgical management is not different from that in older patients.
The decision about breast-conservation versus mastectomy is influenced by the fact that young women frequently present at an advanced stage Using the most frequent definition of young age, patients ≤35 years old, there is evidence of higher rates of LRR when BCT is used as locoregional treatment

22
Breast-conserving therapy is the preferred treatment for patients with early-stage breast cancer.
It offers an accetable local control and overall survival and superior psychosocial outcomes compared with modified radical mastectomy. However, an ipsilateral breast cancer recurrence can be traumatizing and lead to metastasis development and death

23
Prognostic factors related to the patient
Prognostic factors related to the tumor Prognostic factors related to the treatments

24
Prognostic factors related to the patient
Age BRCA mutation Ethnic disparities The poorer outcome of breast cancer in black women could be attributed, not only to socioeconomic reasons but also to biological differences Black women have a higher rate of estrogen-negative high-grade tumors that belong to the basal-like subtype Albain KS 2009, Pierce L 1992, Grann V 2006, Cunningham JE 2004, Carey LA 2006

25
Prognostic factors related to the tumor
Young age affects the annual rate of LRs, especially in the first 5 years after the initial treatment It is of major importance to distinguish so called ‘true recurrences’ that mostly appear during the first 5 years following the initial treatment from the ‘new primary breast cancer’ that tends to appear later.

26
Prognostic factors related to the tumor
Tumor size Axillary involvement Extensive Intraductal Component Lobular in situ Proliferation or high grade Multifocal disease Hormone receptor Moleculare subtypes New relapses markers

27
Prognostic factors related to the treatments
Surgery Radiotherapy Systemic treatment Targeted Therapy

28
Breast conserving treatment or mastectomy?
Using the most frequent definition of young age, patients ≤35 years old, there is evidence of higher rates of LRR when BCT is used as locoregional treatment. Oh JL, 2006 Kim SH, 1998 RechtA, 1988 10-year actuarial LRR rate ( <35 years old) 20%. Beadle, 2009 10-year actuarial LRR rate ( <35 years old) 28%. Elkhuizen, 1998 10-year actuarial LRR rate (29-39 years old) 18% Coulombe, 2007
 20%. Beadle, year actuarial LRR rate ( <35 years old) 28%. Elkhuizen, year actuarial LRR rate (29-39 years old) 18% Coulombe,")
29
However, there is still controversy as to whether this difference in local control translates into inferior survival after BCT in young breast cancer patients Coulombe G, 2007 Kroman N, 2004 Veronesi U, 2002

30
2011 From two Dutch regional population-based cancer registries 1,453 women <40 years pathologically T1N0–1M0 breast cancer were selected. Cox regression survival analysis was used to study the effect of local treatment (BCT vs. mastectomy) stratified for nodal stage on survival and corrected for tumor size, age, period of diagnosis, and use of adjuvant systemic therapy.
 stratified for nodal stage on survival and corrected for tumor size, age, period of diagnosis, and use of adjuvant systemic therapy.")
31
median follow-up of 9.6 years
83% 84% 81% 78% N - 79% 71% N + median follow-up of 9.6 years ENJA J. BANTEMA-JOPPE, 2011

32
Breast conserving treatment or mastectomy?
the higher rates of LRR that have been shown make the choice of BCT or mastectomy especially controversial, but…. data from largely retrospective trials and the lack of information regarding the use of postmastectomy radiation in the mastectomy cohort historic datasets that may no longer be applicable in the time of modern surgery, radiation therapy chemotherapy quality of life and body image Beadle 2011

33
Is RT able to control microscopic foci?
Breast conserving treatment or mastectomy? Is RT able to control microscopic foci?

34
Let’s make things better….
The radiation oncologist have to irradiate the whole breast, using CT-based radiotherapy assuring that the right target is hit, with as little normal tissue as possible in order to achieve an optimal therapeutic ratio.

35
A boost should be systematically administered, with dose homogeneity and no geographical miss.
Improving the definition of the tumor-bed volume is of major importance to potentially decrease the relapse rate after breast-conserving surgery

36
80-90% of Local relapse in tumor bed
Following whole breast irradiation, it is recommended to deliver a boost to the tumour bed. 80-90% of Local relapse in tumor bed Three randomized trials have shown the importance of an increase in the dose to the tumour bed in order to improve local control (level 1, grade A). Romestaing P, 1997 Polgar C, 2002 Bartelink H, 2007
. Romestaing P, Polgar C, Bartelink H,")
37
In the EORTC 22881/10882 trial, youth was the single,
significant factor related to local recurrence The previous report on the EORTC trial established that for patients 40 years old or less, an additional radiation boost (16 Gy to the tumor bed) reduced the 5-year local recurrence rate from 20% to 10%
 reduced the 5-year local recurrence rate from 20% to 10%")
38
Differenza 9,8% 19,3% 9,8% Differenza 1.9%

39
Young patients are unsuitable for APBI
The standard of care for adjuvant RT of early breast carcinoma is whole breast irradiation Young patients are unsuitable for APBI

40
ASTRO 2009 Gec-ESTRO, 2010

41
One of the continuing controversies in the treatment
of patients with BCT is the appropriate dose and fractionation of treatment.

42
Trattamento conservativo del carcinoma infiltrante nelle donne giovani
Si considera indicata l’irradiazione dell’intero seno, dopo adeguata chirurgia conservativa (margini negativi ), con boost sul letto tumorale, correttamente identificato con l’ausilio di clip posizionate dal chirurgo Non sono disponibili dati “specifici” sull’irradiazione ipofrazionata Le pazienti giovani NON sono candidate a PBI
, con boost sul letto tumorale, correttamente identificato con l’ausilio di clip posizionate dal chirurgo. Non sono disponibili dati specifici sull’irradiazione ipofrazionata. Le pazienti giovani NON sono candidate a PBI.")
43
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

44
2010 Individual patient data were available for all four of the randomized trials that began before 1995, and that compared adjuvant radiotherapy vs no radiotherapy following breast-conserving surgery for ductal carcinoma in situ A total of 3925 women were randomized and a total of 3729 women were eligible for analysis.

45
RT reduced the absolute 10-year risk of any ipsilateral breast event
regardless of the age at diagnosis, extent of breast-conserving surgery, use of tamoxifen, method of DCIS detection, margin status, focality, grade, comedonecrosis, architecture, or tumor size

46
The proportional reduction in the rate of ipsilateral breast events achieved with radiotherapy was greater in older than in younger women but did not differ significantly according to any other factor.

47
From 1974 to 2003, 207 cases were collected in 12 French Cancer Centers.
Median age was 36.3 years and median follow-up 160 months. This study is the largest series of patients with DCIS aged under 40 published in the literature.

48
DCIS of the breast is a relatively rare disease in women under 40 years of age (approximately 4% of a total 7000 breast cancers per year in France), which tends to be diagnosed by clinical findings, incidentally, or after plastic surgery … women under 50 who are not part of French national screening programs and are diagnosed with more advanced tumor stages at diagnosis, greater analysis of predictive factors for recurrence is needed

49
Tunon de Lara, 2010

50
The 10-year actuarial recurrence rates were 3.3% (M), 23% (LA),
35.6% (LRT) 29.9% (LRT and boost). RT does not compensate for surgical margins which are not free of cancer In the EORTC trial, RT reduced the risk of local recurrences, but this decrease was less important in young patients than in older patients This rate of recurrences is similar to rates reported in the EORTC trial for younger women (34% at 10 years ) positive margins 12% 16% Tunon de Lara, 2010
 29.9% (LRT and boost). RT does not compensate for surgical margins which are not free of cancer. In the EORTC trial, RT reduced the risk of local recurrences, but this decrease was less important in young patients than in older patients. This rate of recurrences is similar to rates reported in the EORTC trial for younger women (34% at 10 years ) positive margins. 12% 16% Tunon de Lara,")
51
The 10-year global breast-specific survival rates after M, LA or LRT were 98.4%, 98.2% and 94.7% respectively. In patients with relapses, the 10-year survival rate was 67.2% compared to 98% overall for patients with no recurrences. Tunon de Lara, 2010

52
histological size >10 mm ( p 0.011), necrosis ( p 0.022)
The following were significant independent predictive factors of local recurrence: comedocarcinoma ( p 0.004), histological size >10 mm ( p 0.011), necrosis ( p 0.022) positive margins ( p 0.019) The following factors were not predictive of local recurrence: age under 35 ( p 0.32), tumor grade ( p 0.19) radiotherapy with (p 0.62) or without boost (p 0.33) Tunon de Lara, 2010
, histological size >10 mm ( p 0.011), necrosis ( p 0.022) positive margins ( p 0.019) The following factors were not predictive of local recurrence: age under 35 ( p 0.32), tumor grade ( p 0.19) radiotherapy with (p 0.62) or without boost (p 0.33) Tunon de Lara,")
53
Impact of radiotherapy
Unlike in other series radiation therapy with or without boost did not reduce the incidence of local recurrences. Solin LJ, Cancer 2005 Cutuli B, Presse Med 2004 Bijker N, J Clin oncol 2006 Fowble B, IJROBP 1997 Fisher ER, Cancer 2004 Omlin A, Lancet Oncol 2006 Tunon de Lara, 2010

54
Patients under 40 with DCIS constitute a particularly
poor prognosis group with a higher risk of recurrence and poorer survival. Age appears to be one more parameter that should be considered in the complex decision-making process if we want to reduce local recurrence risks, thus improving chances for survival Tunon de Lara, 2010

55
We recommend to limit the use of a safe conservative surgery
to tumors with margins 2 mm, DCIS size 11 mm or smaller free of necrosis and comedocarcinoma. Mastectomy ought to be proposed in cases of multifocal DCIS, tumors larger than 10 mm, positive margins after re-excision, DCIS with necrosis or comedocarcinoma or small breasts Tunon de Lara, 2010

56
Boost radiotherapy in young women with ductal carcinoma in situ: a multicentre, retrospective study of the Rare Cancer Network. Omlin A, Amichetti M, Azria D, et al. Lancet Oncol 2006 373 patients age 45 years or younger 10-year local-recurrence-free survival rates excision alone (15%), 46% excision + WBRT (45%) 72% excision WBRT + boost (40%); 86% (p<0·0001). The investigators conclude that a boost is useful in the management of DCIS.
, 46% excision + WBRT (45%) 72% excision WBRT + boost (40%); 86% (p<0·0001). The investigators conclude that a boost is useful in the management of DCIS.")
57
San antonio e bombis

58
Trattamento conservativo del carcinoma in situ nelle donne giovani
La RT dopo chirurgia conservativa adeguata, secondo la maggior parte degli autori, riduce il rischio di ricaduta locale Sempre secondo alcuni autori, il boost deve essere preso in considerazione, in base al rischio di ricaduta locale La mastectomia deve essere considerata, discussa con la paziente e proposta nei casi in cui la situazione sia tale da non consentire un adeguato controllo con la sola chirurgia conservativa

59
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

60
Forme avanzate, ad alto e medio rischio…

64
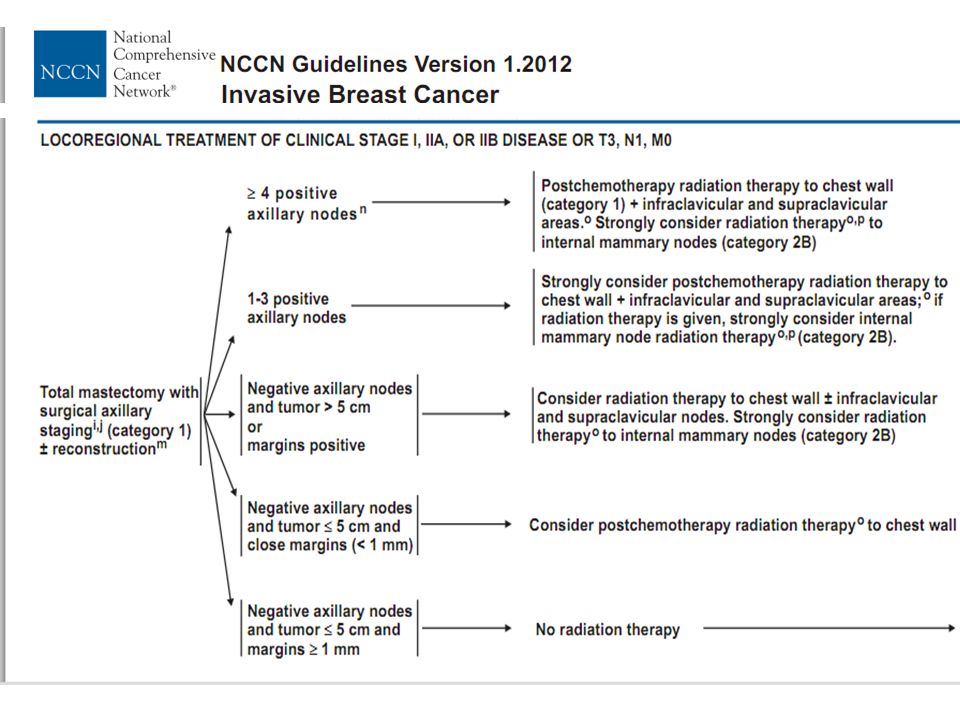
Post-mastectomy radiation therapy was strongly supported for patients with four or more axillary lymph nodes involved. While not in general favoring irradiation for those with lesser nodal involvement, the Panel by a slim majority favored post-mastectomy radiation for patients younger than 45 years with 1–3 positive nodes and for patients at any age with extensive vascular invasion in two or more blocks in conjunction with 1–3 positive nodes.

65
N+ 1-->3 patient-related factors: age <40 years, tumor 3 cm,
2002 patient-related factors: age <40 years, tumor 3 cm, negative estrogen receptor lymphovascular invasion. 66.7% p 7.8%

66
N - In node negative patients, post-mastectomy RT should be indicated on the basis of the existence of one or more risk factors for local relapse, described by the working group as: age less than 40 years, size ≥pT3, grade III, multifocality, lymphovascular and/or muscular and/or cutaneous invasion (expert agreement).
.")
67
RT dopo CT neoadiuvante
Malattia localmente avanzata, inoperabile all'esordio Chirurgia Whatever the type of surgery and the response to neoadjuvant CT……………………… the RT indication should be taken into consideration by considering the initial tumour criteria. Belkacemy Y, Crit Rev Oncol Hematol 2010

68
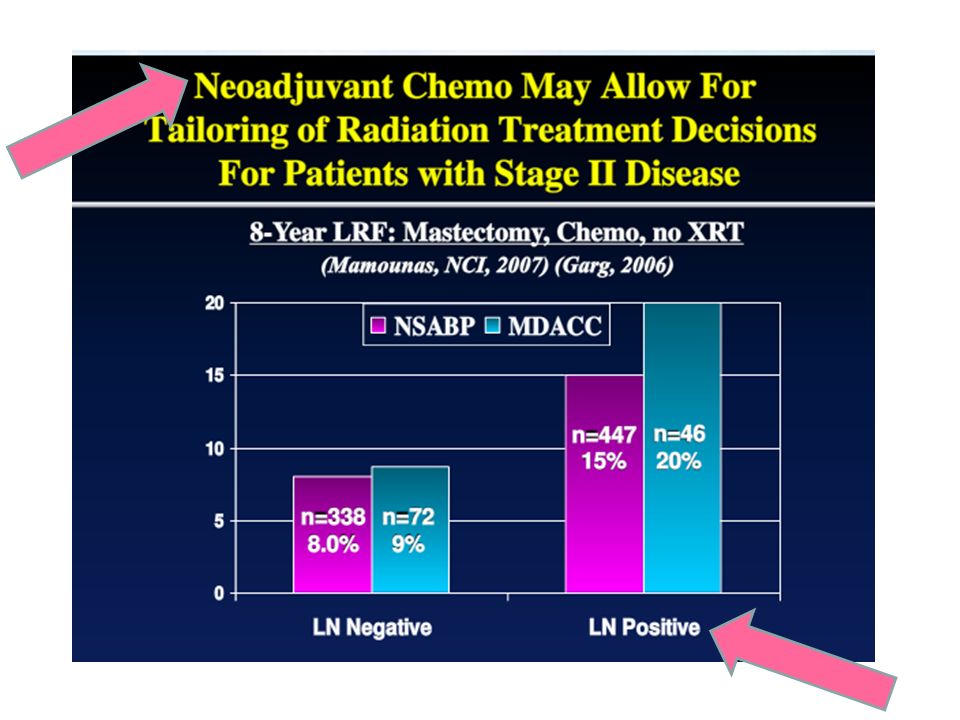
neoadjuvant chemotherapy and mastectomy is determined not just by the
Mc Guire SE, 2007 Freedom from local recurrence the LRR risk after neoadjuvant chemotherapy and mastectomy is determined not just by the extent of residual disease after treatment but also by the extent of disease before treatment

69
…. radiation use was also associated with a
….radiation use was also associated with a statistically significant reduction in the rate of Distant Metatases and an improved CauseSpecificSurvival and Overal Survival in the patients with Stage III disease. freedom from distant relapse Overall survival Mc Guire SE

72
Dopo CT neoadiuvante è indicata la RT…

74
Trattamento delle forme avanzate, alto e medio rischio, anche in caso di mastectomia, insorte nelle donne giovani La RT deve essere eseguita in caso di T>5 cm, T4 N+ in numero > a 4 N+ 13 … giovane età è un fattore di rischio N0 con fattori di rischio… giovane età dopo CT neoadiuvante per LABC, anche in caso di ricostruzione

75
Trattamento delle forme avanzate, alto e medio rischio insorte nelle donne giovani
Devono essere irradiati mammella / parete toracica N sopra-sottoclaveari N mammari interni in caso di elevato numero di N +ascellari N+ e T quadranti centrali /interni N mammari interni clinicamente + N mammari interni RX + volumi

76
Problematiche da affrontare nelle pazienti giovani:
Secondi Tumori Radio-indotti BRCA mutation Gravidanza e neoplasia mammaria

77
Problematiche da affrontare nelle pazienti giovani:
Secondi Tumori Radio-indotti BRCA mutation Gravidanza e neoplasia mammaria

78
2010

79
Controlateral breast cancer
40% of all second tumors among women with breast cancer, with a 25-year cumulative risk of 6.9%. largely related to preexisting breast cancer risk factors, but prior radiation therapy, especially treatment at a young age, may contribute to increased risk. In early case-control studies the overall relative risk of contralateral breast cancer was not significantly increased after radiation therapy (RR 1.2; 95% CI, 0.94, 1.2). Boice JD Jr, N Engl J Med 1992 Storm HH, Br J Cancer 1986
. Boice JD Jr, N Engl J Med Storm HH, Br J Cancer")
80
ma… among women age <45 years at the time of irradiation, the relative risk in the Boice et al study was 1.6 Boice JD Jr, N Engl J Med 1992 women 40 years of age who received 1 Gy of absorbed radiation dose to the contralateral breast had a 2.5-fold greater risk for cancer than unexposed women for women 40 years of age followed for 5 years, a 3-fold risk was observed, with a significant dose–response Stovall M, IJROBP 2008

81
Other solid tumors that have been linked to RT for breast cancer include lung cancer, esophageal cancer, and soft tissue sarcoma….. In several studies, women who received radiation had a 1.5- to 3-fold increased risk of developing lung cancer compared with women who did not receive radiation therapy.

82
Il miglior trattamento oggi…..
I rischi di domani… La complicanza più grave che possiamo evidenziare…. è il mancato controllo della malattia

83
Seminars in Oncology, Vol 36, No 3, June 2009
Approximately 7% of women with breast cancer are diagnosed before the age of 40 years…. Survival rates are worse when compared to those in older women, and multivariate analysis has shown younger age to be an independent predictor of adverse outcome. Inherited syndromes, specifically BRCA1 and BRCA2, must be considered when developing treatment algorithms for younger women..

84
problematiche da affrontare nelle pazienti giovani:
Secondi Tumori Radio-indotti BRCA mutation Gravidanza e neoplasia mammaria

85
BRCA mutation 628 women age 40 and younger diagnosed with breast
cancer from 1996 to 2008.

86
Tumors were first detected by self-examination in 71%, with a median invasive tumor size of 2.0 cm.
Imaging performed at or after diagnosis visualized most tumors; mammography visualized 86%, magnetic resonance imaging (MRI) visualized 96%, mammography plus MRI visualized more than 98% For 81% of patients, the mammogram at diagnosis was their first mammogram. Although 50% had a family history of breast or ovarian cancer, few underwent genetic testing before their cancer diagnosis; 61 of 247 (25%) ultimately tested had a BRCA mutation
 visualized 96%, mammography plus MRI visualized more than 98% For 81% of patients, the mammogram at diagnosis was their first mammogram. Although 50% had a family history of breast or ovarian cancer, few underwent genetic testing before their cancer diagnosis; 61 of 247 (25%) ultimately tested had a BRCA mutation.")
87
BRCA1 mutation carriers develop tumours of a higher grade and proliferation index, with lower oestrogen receptor levels than patients with no such mutation, and tend to have worse outcomes Chappuis PO, 2000 Adem C, 2003 Stoppa-Lyonnet D, 2000 Foulkes WD, 2000 BRCA2 mutation carriers, on the contrary, present tumours with pathologic features similar to those of sporadic tumours Robson M, 2004 Venkitaraman A, 2002

88
Institute Gustave Roussy
2010 Institute Gustave Roussy A history of BRCA1/2 mutation is related to a higher lifetime risk of developing breast cancer and breast conserving treatment remains debatable in this patient population owing to the residual presence of breast tissue which still contains all remaining cells carrying the same deleterious mutations.

89
BRCA mutation Mastectomia o trattamento conservativo?
Ruolo della radioterapia in pazienti con mutazione BRCA: è efficace nel prevenire le ricadute? Il trattamento locale influenza la sopravvivenza?

90
BRCA1 and BRCA2 mutation carriers show enhanced
The molecular pathway involved in DNA repair, particularly the role of BRCA1/2 proteins, would suggest a profile of tumor resistance to ionizing radiation in case of BRCA1/2 mutation Bourgier C, 2010 BRCA1 and BRCA2 mutation carriers show enhanced radiosensitivity, presumably because of the involvement of the BRCA genes in deoxyribonucleic acid repair and cell cycle control mechanisms , with increased radiation-induced apoptosis. Beroukas E, IJROBP 2010 Gowen LC, 1998 Hanawalt PC, 1994 Freneaux p, 2000 morte cellulare programmata per danno al DNA dovuto a RT

91
Familial breast cancer: clinical response to induction
chemotherapy or radiotherapy related to BRCA1/2 mutations status. Fourquet A, Am J Clin Oncol. 2009 90 pts (93 tumors) Median tumor size was 40 mm induction CT +/- RT complete clinical response 15/39 (46%) BRCA 1/2 mutated 7/54 (17%) non mutated tumors (P = 0.008).
 Median tumor size was 40 mm induction CT +/- RT. complete clinical response. 15/39 (46%) BRCA 1/2 mutated. 7/54 (17%) non mutated tumors. (P = 0.008).")
92
The overall complete or major clinical response rate in the tumors treated with induction radiotherapy was 68% (13/19 tumors). Breast conservation after induction treatment was higher in BRmut+ tumors, and clinical response was related to aggressive tumor features correlated with BRCA1/2 mutations. This suggests that impaired repair mechanisms related to the BRCA1/2 mutations increased the chemosensitivity and radiosensitivity of large breast cancers Forquet A, 2009

93
ma… An incorrect repair of DNA double-strand breaks after IR, due to BRCA1/2 mutation, could lead to the development of new primary breast cancer As the residual presence of breast tissue which still contains all remaining cells carrying the same deleterious mutations Bourgier C, 2010

94
655 breast cancer with BRCA1/2 mutations
2010 655 breast cancer with BRCA1/2 mutations BCT (n = 302) LR 23.5% (p=0,0001) M (n = 353) LR 5.5% BCT + chemotherapy was 11.9% (P = 0.08 compared to M)
 LR 23.5% (p=0,0001) M (n = 353) LR 5.5% BCT + chemotherapy was 11.9% (P = 0.08 compared to M)")
95
70% second tumors 82% true recur. Pierce L, 2010 Local failure
Cons. Treatm 23.5% 70% second tumors Mastect. 5.5% 82% true recur.

96
Chirurgia conservativa
RT Chemosensibilità fourquet, 2009 RT+CT Pierce L, 2010 at 15 years >chemiosensibilità Fourquet A, 2009 96

97
Aumento delle neoplasie controlaterali
Metcalfe, JCO 2004 BRCA1 43% BRCA2 35% a 10 aa Pierce L, JCO 2006 BRCA1/2 45% Although studies have shown a risk reduction of CBC in BRCA mutation carriers who take tamoxifen or undergo oophorectomy, no intervention has shown more efficacy in reducing this risk than contralateral prophylactic mastectomy, which can decrease it by up to 91%

98
Prophylactic mastectomy in BRCA mutated patients
5% in Europe 28% in Canada 49% in the United States. It is not clear whether this difference was a result of patient preference or because the operation was not routinely offered in European countries. there is proven efficacy of prophylactic mastectomy for risk reduction, there are no data to support an improvement in survival compared with close surveillance.

99
IEO Pazienti sottoposte ad attenta sorveglianza e valutazione clinico strumentale Possibilità di diagnosi precoce Aumento delle ricadute locali dopo chirurgia conservativa, malgrado la maggiore sensibilità a RT e CT Sembrano essere prevalentemente seconde neoplasie e non ricadute vere

100
Aumento delle neoplasie controlaterali, per le quali la terapia più efficace sembra essere la mastectomia profilattica. Non si evidenzia aumento delle ricadute regionali o sistemiche legate al tipo di trattamento locale Non ci sono dati che dimostrino per altro che un trattamento chirurgico radicale ottenga migliori risultati in sopravvivenza della stretta e accurata sorveglianza

101
neoplasia mammaria e mutazione BRCA…..
Trattemento conservativo ? Mastectomia ? Coinvolgimento psicologico……… gestire il rischio di avere di nuovo una neoplasia o tollerare lo stress legato ad una mutilazione, sia pur con ricostruzione?

102
La decisione deve essere presa con la paziente dopo adeguata informazione sui rischi e sui benefici delle diverse opzioni terapeutiche

103
Carcinoma mammario insorto durante gravidanza
Problematiche da affrontare nelle pazienti giovani: Gravidanza e neoplasia mammaria Carcinoma mammario insorto durante gravidanza Gravidanza in paziente trattata in precedenza per neoplasia mammaria

104
Carcinoma mammario insorto durante la gravidanza…
evento raro, di psicologico profondo impatto sulla vita della paziente, della sua famiglia e del medico e che comporta anche risvolti di tipo etico e confessionale. Per le tossicità attese dai diversi trattamenti, non è sempre possibile ottenere il massimo beneficio per la paziente ed il minimo danno per il feto ed è necessaria una precisa conoscenza dei dati della letteratura e dei fenomeni biologici coinvolti La decisione della paziente va sempre rispettata Carcinoma mammario insorto durante la gravidanza…

105
Time after conception (weeks) Effect Dose threshold
0–2 Prenatal death 10 cGy deterministic 2-15 Malformation, Microcephaly, growth retardation 10-20 cGy 8–25 Mental retardation, IQ decrease, Growth retardation 50 cGy 0–38 Leukaemia, solid tumours in childhood, lifetime risk of fatal cancer after fetal exposure, hereditary effects through generations stochastic

106
As expected, fetal dose increased as the pregnancy became more advanced

107
una controindicazione assoluta al trattamento radiante
Sebbene non vi sia unanime consenso e alcuni autori presentino dati su bambini nati sani dopo irradiazione con dosi significative (0,039 Gy al primo trimestre; 0,14-0,18 Gy al terzo trimestre), la maggior parte delle fonti bibliografiche considera la gravidanza, in ogni epoca gestazionale, una controindicazione assoluta al trattamento radiante
, la maggior parte delle fonti bibliografiche considera. la gravidanza, in ogni epoca gestazionale, una controindicazione assoluta al trattamento radiante.")
108
Diagnosi nel primo trimestre:
Mastectomia + DA, eventuale PMRT dopo il parto Diagnosi alla fine del secondo o nel terzo trimestre: chirurgia conservativa seguita da RT da effettuarsi dopo il parto, (eventualmente anticipato non appena vi siano idonee condizioni di maturazione respiratoria per il bambino).
.")
109
Gravidanza in paziente trattata in precedenza per neoplasia mammaria
La possibile disfunzione ovarica indotta dalla chemioterapia adiuvante può rendere difficoltoso il realizzarsi di una gravidanza . Solo il 10% delle donne trattate per neoplasia mammaria concepisce e complessivamente si riscontra in questa popolazione la metà delle maternità registrate nella popolazione sana di analoga età Oktem O, Cancer 2007 Ives A, BMJ 2007

110
La gravidanza non sembra influenzare negativamente la prognosi.
Generalmente si consiglia di dilazionare il concepimento fino ad almeno due anni dal termine dei trattamenti: non è noto quale sia il tempo ottimale, ma si considera che il maggior rischio di ricaduta si riscontri entro tale limite. L’allattamento, che può essere reso problematico dalla precedente radioterapia, non aumenta il rischio di ripresa di malattia o di una eventuale comparsa di neoplasia nel bambino allattato. Hickey M, 2009 Ives A 2007

111
Incidenza Fattori prognostici Procedure Diagnostiche Il trattamento locale nel carcinoma infiltrante Il trattamento locale nel carcinoma in situ Trattamento delle forme avanzate, alto e medio rischio

112
problematiche da affrontare nelle pazienti giovani:
Secondi Tumori Radio-indotti BRCA mutation Gravidanza e neoplasia mammaria

113
Grazie per l’attenzione !
Treatment of very young women Marina Guenzi Oncolgia Radioterapica Genova Grazie per l’attenzione !

Presentazioni simili









>")










>")
