Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Sindromi eruttive e febbrili:
Vaiolo Pasquale Urbano Collegamenti: consensus Linee guida

2
Vedi il testo completo Vedi anche

3
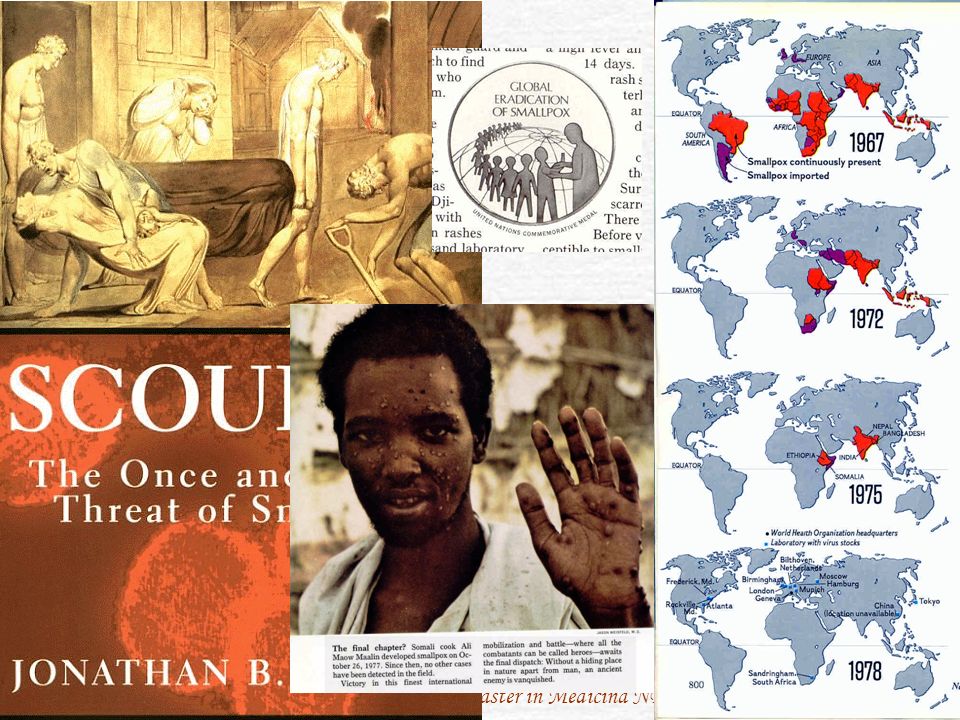
Vaiolo: Variola major Most physicians today in the United States have not seen this disease. This slide is to help familiarize physicians with what smallpox looks like. Note the concentration of the rash on the face, and less so on the trunk. The smallpox rash tends to be more peripherally distributed. Smallpox is probably the most feared bioterrorist agent. This is because of the risk of secondary spread, the lack of effective known treatment, the large portion of the population that no longer has antibodies to it, and because of the disease’s visibility and disfiguring nature. It is highly contagious, affecting about 1 in 12 people exposed. It is estimated that each case of the disease could infect 10 to 12 new contacts. A large portion of the population is susceptible because immunity wanes with time. The last known natural case was in Somalia in Since then, the only known cases were caused by a laboratory accident in 1978 in Birmingham, England, which killed one person and caused a limited outbreak. Smallpox was officially declared eradicated in 1979. Vaccinations were stopped in the United States in 1972. Smallpox could easily become reestablished in the world if it were released as a bioterrorist agent. Source: World Health Organization Communicable Disease Surveillance and Response. Frequently asked questions on smallpox, 26 October Available at: Photo Source: World Health Organization Communicable Disease Surveillance and Response Slide Set on Diagnosis of Smallpox,

4
Vaiolo grave, letale La foto ritrae uno dei numerosi moulages in cera raccolti nel museo della ex Scuola di Sanità Militare, Via Venezia, Firenze

5
Vaioloide o alastrim La foto ritrae uno dei numerosi moulages in cera raccolti nel museo della ex Scuola di Sanità Militare, Via Venezia, Firenze

6
Sebastiano Cunsolo soffre di vaiolo, chiaramente visibile dale macchie rosse sulla sua faccia, sul torace, braccia e gambe. La donna a sinistra, verosimilmente sua moglie o sua sorella, alza le braccia in preghiera verso Santa Marta invocando una pronta guarigione mentre il medico presiede alle cure. "Miracolo Farto a Sabastiano Gunsolo al 8 Dicembre" Sebastiano Cunsolo soffre di vaiolo, chiaramente visibile dale macchie rosse sulla sua faccia, sul torace, braccia e gambe. La donna a sinistra, verosimilmente sua moglie o sua sorella, alza le braccia in preghiera verso Santa Marta invocando una pronta guarigione mentre il medico presiede alle cure. "Miracolo Farto a Sabastiano Gunsolo al 8 Dicembre"

7
Aztec smallpox victims
from Historia De Las Casas de Nueva Espana, Volume 4, Book 12, Lam. cliii, plate 114.

9
Ancora preoccupazioni
Dopo l’ultimo caso ‘naturale’, c’è stato un episodio di diffusione di Variola major da un laboratorio I ceppi ufficialmente conservati presso Stati Uniti e Russia non sono ancora stati eliminati Timori che caschino nelle mani di malintenzionati Il vaiolo delle scimmie [Monkeypox] può passare all’uomo Recente [25 Mar 2010] la segnalazione di sospetti casi di vaiolo in campi profughi dell’Uganda: vedi nota UNDIAGNOSED ILLNESS, POX VIRUS SUSPECTED - UGANDA (BUDUDA): REQUEST FOR INFORMATION *********************************************************************** A ProMED-mail post < ProMED-mail is a program of the International Society for Infectious Diseases < Date: Thurs 25 Mar 2010 From: Daily Monitor (Uganda) online [edited] < Small pox reported in Bududa camps Four children in Internally Displaced People's camps in Bududa District, reportedly suffering from small pox, have been taken to Bukigai and Bulucheke Health Centres III and II, respectively. Ms Kevin Nabutuwa, Uganda Red Cross' regional programme officer for eastern Uganda, said last evening that the infections were registered on Monday and Tuesday. Spread contained "These are cases in the IDP camps but the spread has been contained," she said by phone. In Kampala, Dr Richard Nduhuura, the state minister for Health (general duties), said he is "unaware" of the outbreak of the disease that scientists say can kill three out of every 10 infected persons. He referred this newspaper to the acting Director General of Health Services, Dr Kenya Mugisha, who was unavailable for comment Information posted on the World Health Organisation website indicates that small pox, an ancient communicable disease infamous for killing Queen Mary II of England, is transmitted mainly through infected aerosols and air droplets. "The frequency of infection is highest after face-to-face contact with a patient," says WHO. Symptoms include fever, headache, and back/abdominal pangs. Survivors usually remain with deep-pitted scars (pockmarks), most prominently on the face. - -- Communicated by: Sharon Sanders for Flutrackers.com [Natural infection with smallpox (Variola major) having been eliminated, our past experience with these types of reports usually reveals an outbreak of chickenpox, molluscum, or rarely true pox virus infections such as monkeypox Of course, the possibility of intentional or accidental release of variola is always of extreme concern. More information is urgently requested from those with firsthand knowledge of the situation. A map of the Bududa district, near the Kenyan border, can be found at: < - Mod.LM] [see also: Vaccinia, human, oral rabies vaccine - USA: (PA) Vaccinia, laboratory-acquired - USA: (VA), Smallpox vaccination, adverse events - USA: prog. vaccinia Cowpox, rodents, human (06): Europe, background Cowpox, rodents, human (04): Europe Cowpox, rodents, human - Germany, France ex Czech Rep Molluscum contagiosum, swimming pool - Spain (02) ]
: REQUEST FOR INFORMATION. *********************************************************************** A ProMED-mail post. < ProMED-mail is a program of the. International Society for Infectious Diseases < Date: Thurs 25 Mar From: Daily Monitor (Uganda) online [edited] < Small pox reported in Bududa camps Four children in Internally Displaced People s camps in Bududa District, reportedly suffering from small pox, have been taken to Bukigai and Bulucheke Health Centres III and II, respectively. Ms Kevin Nabutuwa, Uganda Red Cross regional programme officer for eastern Uganda, said last evening that the infections were registered on Monday and Tuesday. Spread contained. These are cases in the IDP camps but the spread has been contained, she said by phone. In Kampala, Dr Richard Nduhuura, the state minister for Health (general duties), said he is unaware of the outbreak of the disease that scientists say can kill three out of every 10 infected persons. He referred this newspaper to the acting Director General of Health Services, Dr Kenya Mugisha, who was unavailable for comment. Information posted on the World Health Organisation website indicates that small pox, an ancient communicable disease infamous for killing Queen Mary II of England, is transmitted mainly through infected aerosols and air droplets. The frequency of infection is highest after face-to-face contact with a patient, says WHO. Symptoms include fever, headache, and back/abdominal pangs. Survivors usually remain with deep-pitted scars (pockmarks), most prominently on the face Communicated by: Sharon Sanders for Flutrackers.com. [Natural infection with smallpox (Variola major) having been eliminated, our past experience with these types of reports usually reveals an outbreak of chickenpox, molluscum, or rarely true pox virus infections such as monkeypox Of course, the possibility of intentional or accidental release of variola is always of extreme concern. More information is urgently requested from those with firsthand knowledge of the situation. A map of the Bududa district, near the Kenyan border, can be found at: < - Mod.LM] [see also: Vaccinia, human, oral rabies vaccine - USA: (PA) Vaccinia, laboratory-acquired - USA: (VA), Smallpox vaccination, adverse events - USA: prog. vaccinia Cowpox, rodents, human (06): Europe, background Cowpox, rodents, human (04): Europe Cowpox, rodents, human - Germany, France ex Czech Rep Molluscum contagiosum, swimming pool - Spain (02) ]")
10
EID Volume 17, Number 4–April 2011 Policy Review Should Remaining Stockpiles of Smallpox Virus (Variola) Be Destroyed? Raymond S. Weinstein Leggi in: Abstract in nota Abstract In 2011, the World Health Organization will recommend the fate of existing smallpox stockpiles, but circumstances have changed since the complete destruction of these cultures was first proposed. Recent studies suggest that variola and its experimental surrogate, vaccinia, have a remarkable ability to modify the human immune response through complex mechanisms that scientists are only just beginning to unravel. Further study that might require intact virus is essential. Moreover, modern science now has the capability to recreate smallpox or a smallpox-like organism in the laboratory in addition to the risk of nature re-creating it as it did once before. These factors strongly suggest that relegating smallpox to the autoclave of extinction would be ill advised.

11
Vaiolo: Presentazione
Incubazione: ~ 12 gg (fino a 17 gg) I sintomi precoci sono aspecifici Febbre, malessere, dolori diffusi, per 2-4 gg; poi aggravamento L’eruzione compare alle estremità, con aspetto uniforme Croste per 1-2 settimane Contagioso fino a caduta completa di tutte le croste Probably the most feared BT agent because of possibility of further spread. Very contagious once rash appears First appears in the mouth,then spreads to the extremities and then to the trunk Rash will have a uniform appearance Patients with clinical smallpox are toxic and very ill. If fatal, death usually occurs in the second week of illness, and probably results from the toxemia of circulating immune complexes and soluble variola antigens. Photo source: World Health Organization Communicable Disease Surveillance and Response Slide Set on Diagnosis of Smallpox. Sulla contagiosità: Contagiousness is high (after face to face contact with patient once the fever has begun and during the first week of rash, when the virus is released via the respiratory tract), or moderate (in the later stages of the disease until the last scabs fall off; the large amounts of virus shed from the skin are not highly infectious) and infected host is contagious for days; the incubation period lasts usually usually (7-)12(-17) day(s). Viral shedding starts 3-7 days after onset of infection; { } continues for days.
 I sintomi precoci sono aspecifici. Febbre, malessere, dolori diffusi, per 2-4 gg; poi aggravamento. L’eruzione compare alle estremità, con aspetto uniforme. Croste per 1-2 settimane. Contagioso fino a caduta completa di tutte le croste. Probably the most feared BT agent because of possibility of further spread. Very contagious once rash appears. First appears in the mouth,then spreads to the extremities and then to the trunk. Rash will have a uniform appearance. Patients with clinical smallpox are toxic and very ill. If fatal, death usually occurs in the second week of illness, and probably results from the toxemia of circulating immune complexes and soluble variola antigens. Photo source: World Health Organization Communicable Disease Surveillance and Response Slide Set on Diagnosis of Smallpox. Sulla contagiosità: Contagiousness is high (after face to face contact with patient once the fever has begun and during the first week of rash, when the virus is released via the respiratory tract), or moderate (in the later stages of the disease until the last scabs fall off; the large amounts of virus shed from the skin are not highly infectious) and infected host is contagious for days; the incubation period lasts usually usually (7-)12(-17) day(s). Viral shedding starts 3-7 days after onset of infection; { } continues for days.")
12
Vaiolo Isolamento Notifica IMMEDIATA Diagnosi Laboratorio
Escludere la varicella – EM - PCR Isolamento Stretto isolamento respiratorio e da contatto (pressione negativa) Rintracciare tutti i contatti dei 17 gg precedenti all’insorgenza Trattamento Nessuno efficace; Cidofovir? ST246? [sperimentale] Letalità ~ 30% Because local labs can’t test for smallpox, if tests for chicken pox are negative, your index of suspicion for smallpox should be very high. The lab must be notified if smallpox is even slightly suspected, so that they can take precautions, and so the specimen can be referred immediately to the local public health department. The state public health department will send vesicle scrapings to the CDC. It is important to notify the local public health department immediately to initiate a response to the outbreak even before confirmation has been determined. Names and contact information of anybody who may have been in contact with an infected person should be collected before anyone is allowed to leave the area. Contacts must be traced up to 17 days prior to the presentation of illness. Public health officials must identify and locate all people with whom the infected person had contact and provide vaccination to prevent secondary transmissions. Respiratory isolation is necessary. Isolation is especially important to try to prevent any secondary spread, and negative pressure rooms are preferred (Henderson, 1999). Because most hospitals would quickly run out of isolation rooms, infection control will likely have to use a cohort strategy. (Patients with suspected smallpox would be clustered together in a ward or other area.) Cidofovir might be of use, but because there is no more human smallpox it cannot be tested in humans. It is also expensive and in limited supply. Article References: Gordon S. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine. 1999; 66(10): Breman J, Henderson DA. Poxvirus dilemmas: Monkeypox, smallpox, and biological terrorism. New England J of Medicine. 1998; 339(8): Henderson DA et al. Smallpox as a biological weapon: Medical and public health management. JAMA. June 09, 1999; 281(22): Photo of smallpox virus. Source: CDC New Potential Smallpox Therapeutic Reported A report published in the October 2005 issue of the Journal of Virology details the development of a new potential therapeutic for smallpox. Currently , there is no FDA-approved therapeutic product to treat smallpox. The researchers report that they developed a high-throughput screening assay to assess compounds for their ability to inhibit vaccinia virus-induced cytopathic effect in cultured cells. Vaccinia virus is a close relative of the virus that causes smallpox, variola virus, and is the virus that comprises Dryvax, the only smallpox vaccine that is currently approved for human use by the U.S. Food and Drug Administration. Both are members of the orthopoxvirus ( Orthopoxviridae ) family of viruses. Using this assay, the researchers screened 356,240 compounds and discovered a compound that is a specific inhibitor of orthopoxvirus replication. The compound, ST-246, is a low-molecular-weight compound (MW 376) that was found to have potent and specific antiviral activity against orthopoxviruses in vitro including: vaccinia virus, two strains of variola virus; cowpox virus; ectromelia (mousepox) virus; monkeypox virus; and camelpox virus. The researchers also report that oral administration of ST-246 was successful in protecting mice from lethal orthopoxvirus challenge in several mouse models of orthopoxvirus disease.
 Rintracciare tutti i contatti dei 17 gg precedenti all’insorgenza. Trattamento. Nessuno efficace; Cidofovir ST246 [sperimentale] Letalità ~ 30% Because local labs can’t test for smallpox, if tests for chicken pox are negative, your index of suspicion for smallpox should be very high. The lab must be notified if smallpox is even slightly suspected, so that they can take precautions, and so the specimen can be referred immediately to the local public health department. The state public health department will send vesicle scrapings to the CDC. It is important to notify the local public health department immediately to initiate a response to the outbreak even before confirmation has been determined. Names and contact information of anybody who may have been in contact with an infected person should be collected before anyone is allowed to leave the area. Contacts must be traced up to 17 days prior to the presentation of illness. Public health officials must identify and locate all people with whom the infected person had contact and provide vaccination to prevent secondary transmissions. Respiratory isolation is necessary. Isolation is especially important to try to prevent any secondary spread, and negative pressure rooms are preferred (Henderson, 1999). Because most hospitals would quickly run out of isolation rooms, infection control will likely have to use a cohort strategy. (Patients with suspected smallpox would be clustered together in a ward or other area.) Cidofovir might be of use, but because there is no more human smallpox it cannot be tested in humans. It is also expensive and in limited supply. Article References: Gordon S. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine. 1999; 66(10): Breman J, Henderson DA. Poxvirus dilemmas: Monkeypox, smallpox, and biological terrorism. New England J of Medicine. 1998; 339(8): Henderson DA et al. Smallpox as a biological weapon: Medical and public health management. JAMA. June 09, 1999; 281(22): Photo of smallpox virus. Source: CDC. New Potential Smallpox Therapeutic Reported A report published in the October 2005 issue of the Journal of Virology details the development of a new potential therapeutic for smallpox. Currently , there is no FDA-approved therapeutic product to treat smallpox. The researchers report that they developed a high-throughput screening assay to assess compounds for their ability to inhibit vaccinia virus-induced cytopathic effect in cultured cells. Vaccinia virus is a close relative of the virus that causes smallpox, variola virus, and is the virus that comprises Dryvax, the only smallpox vaccine that is currently approved for human use by the U.S. Food and Drug Administration. Both are members of the orthopoxvirus ( Orthopoxviridae ) family of viruses. Using this assay, the researchers screened 356,240 compounds and discovered a compound that is a specific inhibitor of orthopoxvirus replication. The compound, ST-246, is a low-molecular-weight compound (MW 376) that was found to have potent and specific antiviral activity against orthopoxviruses in vitro including: vaccinia virus, two strains of variola virus; cowpox virus; ectromelia (mousepox) virus; monkeypox virus; and camelpox virus. The researchers also report that oral administration of ST-246 was successful in protecting mice from lethal orthopoxvirus challenge in several mouse models of orthopoxvirus disease.")
13
Vaiolo - contagiosità L’idea che la contagiosità sia limitata al periodo eruttivo è errata Il soggetto infetto comincia a costituire fonte di contagio, subdola, verso la fine del periodo di incubazione, e diventa estremamente pericoloso qualche giorno prima dell’eruzione cutanea, quando i sintomi sono aspecifici Goccioline di Pflugge

14
La vecchia prova biologica di Paul, inoculazione per scarificazione della cornea di coniglio
La foto ritrae uno dei numerosi moulages in cera raccolti nel museo della ex Scuola di Sanità Militare, Via Venezia, Firenze

15
Vaiolo vs. Varicella Variola Varicella Incubazone 7-17 d 14-21 d
Prodromi d minimi/assenti Distribuzione estremità tronco Progressione sincrona asincrona Formazione di croste d p rash 4-7 d p rash Caduta croste d p rash <14 d p rash Note the degree of illness, uniformity of lesions, and distribution of rash that characterize smallpox. The rash is centrifugal in distribution, most dense on the face and extremities. Lesions develop during a 1-to-2-day period and evolve at the same rate. On any given part of the body, they are generally at the same stage of development. This characteristic is in contrast with chickenpox (varicella), the disease most often confused with smallpox. With varicella, new lesions appear in crops every few days, and lesions at very different stages of maturation can be adjacent; varicella lesions are more concentrated on the trunk than on the face and extremities and are almost never found on the palms and soles.
, the disease most often confused with smallpox. With varicella, new lesions appear in crops every few days, and lesions at very different stages of maturation can be adjacent; varicella lesions are more concentrated on the trunk than on the face and extremities and are almost never found on the palms and soles.")
16
Vaiolo vs. Varicella Varicella (ceroplastica)
")
17
Vaiolo vs. Varicella Eruzione: tronco, diversi stadi di sviluppo
Note the dissimilarities between rashes. Photo Sources: Smallpox: World Health Organization Communicable Disease Surveillance and Response Slide Set on Diagnosis of Smallpox. Chickenpox: Eruzione: tronco, diversi stadi di sviluppo Eruzione: estremità, aspetto uniforme

18
The English doctor Edward Jenner carried out the first vaccination against smallpox in 1796.
Science & Society Picture Library

19
Vedi il testo completo 14 maggio 1797: prima VACCINAZIONE – da una pustola di Cowpox di Sarah Nelmes a Susan Phipps

20
`VACCINATION FROM THE CALF.' -
1. DISTINCTIVE MARK OF ANIMAL VACCINATION. 2. TAKING LYMPH FROM THE CALF. 3. VACCINATING INFANTS. Da una rivista del 1883

21
L’originale, dipinto a olio da A
L’originale, dipinto a olio da A. Touchemolin, si trova al Museo della Sanità Militare di Val de Grace, Parigi.

22
Il necessario THE VACCINE How much vaccine is available?
As of March 2003, there is enough vaccine for every citizen in the U.S. The CDC has 15.4 million doses of the Wyeth Dryvax. It can be diluted 1:5 to provide 77 million effective doses. It can be diluted 1:10 with only slightly less efficacy that will yield 154 million doses. Another supply of vaccine manufactured by Aventis Pastuer consists of an additional 80 million doses. It also can be diluted 1:5 for a total of 400 million doses. The addition of these doses from Aventis Pastuer (400 million) and Dryvax diluted 10:1 (154 million) would provide 554 million doses. This is more than enough to handle an outbreak in the United States (population 290 million). Furthermore, Acambis is scheduled to deliver the new vaccine that will ready for use in 2004 or The new vaccine may have fewer complications than the current vaccine supply, however this hypothesis has not been tested and proven.
 and Dryvax diluted 10:1 (154 million) would provide 554 million doses. This is more than enough to handle an outbreak in the United States (population 290 million). Furthermore, Acambis is scheduled to deliver the new vaccine that will ready for use in 2004 or The new vaccine may have fewer complications than the current vaccine supply, however this hypothesis has not been tested and proven.")
23
Scorte di vaccinia in Italia
Nel 2003 il Ministro della Salute ha affermato che possediamo scorte di vaccinia per 5 milioni di dosi, diluibili per proteggere 25 milioni di persone Si tratta di linfa vaccinica [prima generazione] Ha anche affermato l’intenzione di acquistare 500 dosi di Cidofovir

24
Nuovi vaccini Gli USA dispongono di un vaccino di seconda generazione, costituito di un ceppo di vaccinia coltivato su cellule diploidi. È in sviluppo un vaccino di terza generazione. Leggi nota, o vai a: How Much Vaccine is Available, and How Should it Be Used? The United States has ample supplies of second-generation and third-generation vaccines (25). The second-generation vaccine is ACAM2000 (Acambis, Cambridge, MA, USA), which is a plaque-purified distinct strain of New York City Board of Health vaccinia virus grown by using modern cell lines rather than the skin of calves. It produces reactions and immune responses similar to those of first-generation Dryvax vaccine (Wyeth Laboratories, New York, NY, USA) (26). Second-generation vaccines can be diluted 1:10 and still give excellent results. The third-generation vaccine is Immvamune (Bavarian Nordic, Kvistgaard, Denmark), a strain of modified vaccinia Ankara (MVA), which has been extensively tested for safety and protects animals from orthopoxvirus challenge (1). Two injections of MVA produce humoral and cellular immunity similar to that produced by first-generation and second-generation vaccines. Although a live virus, MVA does not replicate in human tissues and does not have the same risk of adverse reactions as first-generation and second-generation vaccines. It has been tested in patients with atopic dermatitis and in patients with HIV infections with T-cell counts >250 cells/mL (1). Third-generation vaccines such as MVA may not be optimal for outbreak control. MVA is frozen, and thus must be thawed in the field (the manufacturer is developing a freeze-dried formulation). It requires syringes and needles and must be administered by someone trained to give injections. First-generation and second-generation vaccines are lyophilized and can be reconstituted and administered in the field with bifurcated needle scarification by persons with minimal training. Because MVA does not produce a visible lesion or scar, rapid determination of who has been already vaccinated is difficult. Optimal immunity with MVA requires 2 injections. In contrast, single injections are fully protective for first-generation and second-generation vaccines. In the absence of a perfect animal model for smallpox, and because it is impossible to test these vaccines against smallpox, we have only laboratory evidence of their efficacy. Given these limitations, third-generation vaccines may be best for persons who anticipate possible exposure, such as military personnel or laboratory personnel working with orthopoxviruses. In an actual outbreak, ACAM2000 should be used for field vaccination. However, its use increases the risk for development of progressive vaccinia or eczema vaccinatum; these adverse events would then need to be treated with ST-246. WHO is planning on creating a modest real, and substantial virtual, stockpile of vaccines. There are ≈60 million doses of vaccine in this stockpile and plans to increase it to ≈200 million doses. How much of this stockpile should be second-generation or third-generation vaccines that may not yet have been licensed widely? What should be the rules for release of such vaccines from the stockpile? Widespread use of first-generation or second-generation smallpox vaccines in era of AIDS and iatrogenic immune suppression by cancer chemotherapy or for transplant surgery seems unlikely unless there are actual cases of smallpox. In that situation, we might respond by using first-generation and second-generation vaccines with proven efficacies.
. The second-generation vaccine is ACAM2000 (Acambis, Cambridge, MA, USA), which is a plaque-purified distinct strain of New York City Board of Health vaccinia virus grown by using modern cell lines rather than the skin of calves. It produces reactions and immune responses similar to those of first-generation Dryvax vaccine (Wyeth Laboratories, New York, NY, USA) (26). Second-generation vaccines can be diluted 1:10 and still give excellent results. The third-generation vaccine is Immvamune (Bavarian Nordic, Kvistgaard, Denmark), a strain of modified vaccinia Ankara (MVA), which has been extensively tested for safety and protects animals from orthopoxvirus challenge (1). Two injections of MVA produce humoral and cellular immunity similar to that produced by first-generation and second-generation vaccines. Although a live virus, MVA does not replicate in human tissues and does not have the same risk of adverse reactions as first-generation and second-generation vaccines. It has been tested in patients with atopic dermatitis and in patients with HIV infections with T-cell counts >250 cells/mL (1). Third-generation vaccines such as MVA may not be optimal for outbreak control. MVA is frozen, and thus must be thawed in the field (the manufacturer is developing a freeze-dried formulation). It requires syringes and needles and must be administered by someone trained to give injections. First-generation and second-generation vaccines are lyophilized and can be reconstituted and administered in the field with bifurcated needle scarification by persons with minimal training. Because MVA does not produce a visible lesion or scar, rapid determination of who has been already vaccinated is difficult. Optimal immunity with MVA requires 2 injections. In contrast, single injections are fully protective for first-generation and second-generation vaccines. In the absence of a perfect animal model for smallpox, and because it is impossible to test these vaccines against smallpox, we have only laboratory evidence of their efficacy. Given these limitations, third-generation vaccines may be best for persons who anticipate possible exposure, such as military personnel or laboratory personnel working with orthopoxviruses. In an actual outbreak, ACAM2000 should be used for field vaccination. However, its use increases the risk for development of progressive vaccinia or eczema vaccinatum; these adverse events would then need to be treated with ST-246. WHO is planning on creating a modest real, and substantial virtual, stockpile of vaccines. There are ≈60 million doses of vaccine in this stockpile and plans to increase it to ≈200 million doses. How much of this stockpile should be second-generation or third-generation vaccines that may not yet have been licensed widely What should be the rules for release of such vaccines from the stockpile Widespread use of first-generation or second-generation smallpox vaccines in era of AIDS and iatrogenic immune suppression by cancer chemotherapy or for transplant surgery seems unlikely unless there are actual cases of smallpox. In that situation, we might respond by using first-generation and second-generation vaccines with proven efficacies.")
25
Vaccino anti-vaioloso
Vaccinia virus vivo Inoculato intradermo con ago biforcato Pustula –> crosta in ~ 1 settimana; febbre lieve Può trasmettersi ad altri, fino a caduta della crosta Dubbi sulla durata a vita dell’immunità I vecchi vaccinati probabilmente hanno un ridotto rischio di letalità Efficace fino a diversi giorni dopo l’esposizione Immunity to vaccinia virus (cow pox) confers immunity to variola (smallpox) Most people are now susceptible, because immunity wanes with time after vaccination, and vaccination programs were stopped after 1972 in the United States. Could easily become re-established in the world if released as BT agent There is a limited supply of vaccine, however there are orders from the US Dept of DHHS to produce 300 million doses, enough to vaccinate the entire US. Dilutions of currently available vaccine appear to confer immunity. The existing smallpox vaccine is the live Vaccinia virus given intra-dermally on a bifurcated needle. The vaccine forms a pustule that scabs over in about 1 week and may produce mild fever (Henderson, 1999; Gordon, 1999). The need for pre-event smallpox vaccination is a matter of debate. Because the vaccine is effective up to several days AFTER exposure, it is important to make sure that a system is in place for rapid deployment of vaccine in the event of smallpox cases. In January 2003, the federal government embarked on a national voluntary vaccination program in an effort to have teams of vaccinated healthcare workers that would be able to respond to care for a case of smallpox and initiate urgent vaccination programs for at-risk citizens. Article References: Gordon S. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine. 1999; 66(10): Henderson DA et al. Smallpox as a biological weapon: Medical and public health management. JAMA. June 09, 1999; 281(22): Photo Source: Smithsonian Institution, History Wired,
 confers immunity to variola (smallpox) Most people are now susceptible, because immunity wanes with time after vaccination, and vaccination programs were stopped after 1972 in the United States. Could easily become re-established in the world if released as BT agent. There is a limited supply of vaccine, however there are orders from the US Dept of DHHS to produce 300 million doses, enough to vaccinate the entire US. Dilutions of currently available vaccine appear to confer immunity. The existing smallpox vaccine is the live Vaccinia virus given intra-dermally on a bifurcated needle. The vaccine forms a pustule that scabs over in about 1 week and may produce mild fever (Henderson, 1999; Gordon, 1999). The need for pre-event smallpox vaccination is a matter of debate. Because the vaccine is effective up to several days AFTER exposure, it is important to make sure that a system is in place for rapid deployment of vaccine in the event of smallpox cases. In January 2003, the federal government embarked on a national voluntary vaccination program in an effort to have teams of vaccinated healthcare workers that would be able to respond to care for a case of smallpox and initiate urgent vaccination programs for at-risk citizens. Article References: Gordon S. The threat of bioterrorism: A reason to learn more about anthrax and smallpox. Cleveland Clinic J of Medicine. 1999; 66(10): Henderson DA et al. Smallpox as a biological weapon: Medical and public health management. JAMA. June 09, 1999; 281(22): Photo Source: Smithsonian Institution, History Wired, ID=1.")
26
Inoculazione del Vaccino
CDC instructions for vaccine administration using the bifurcated needle - Multiple Puncture Vaccination During the global smallpox eradication effort, the bifurcated needle was used along with a technique called multiple puncture vaccination. Today, this is still the recommended method for administering smallpox vaccine. Each bifurcated needle is sterile and individually wrapped. The bifurcated needle is for one-time use only and should be discarded in an appropriate biohazard container immediately after vaccinating each patient. Step-by-Step Instructions 1. Review patient history for contraindications. 2. Choose the site for vaccination: The deltoid area on the upper arm is recommended. 3. Skin preparation: No skin preparation is required. Under no circumstances should alcohol be applied to the skin prior to vaccination as it has been shown to inactivate the vaccine virus. 4. Dip needle: The needle is dipped into the vaccine vial and withdrawn. The needle is designed to hold a tiny drop of vaccine of sufficient size and strength to ensure a take if properly administered. The same needle should never be dipped into the vaccine vial more than once, in order to avoid contamination of the vaccine vial. 5. Make perpendicular insertions within a 5-mm diameter area: The needle is held perpendicular to the site of insertion. The wrist of the vaccinator should be maintained in a firm position by resting on the arm of the vaccinee or another firm support. A number of perpendicular insertions are made in rapid order in an area approximately 5 mm in diameter. The number of insertions should be in accordance with the package insert, using 3 insertions for primary vaccination and 15 insertions for revaccination with the Dryvax vaccine. A trace of blood should appear at the site of vaccination within seconds. During primary vaccination, if no trace of blood is visible after 3 insertions, an additional 3 insertions should be made using the same bifurcated needle without reinserting the needle into the vaccine vial. The bifurcated needle is for one-time use only and should be discarded in an appropriate biohazard container immediately after vaccinating each patient. Directions are from the Centers for Disease Control and Prevention, Photo Source: WHO Communicable Disease Surveillance and Response,

27
Inoculazione del Vaccino
CDC instructions for vaccine administration using the bifurcated needle - Multiple Puncture Vaccination 6. Absorb Excess Vaccine: After vaccination, excess vaccine should be absorbed with sterile gauze. Discard the gauze in a safe manner (usually in an infection control receptacle) in order not to contaminate the site or infect others who may come in contact with it. 7. Cover vaccination site: It is important that the vaccination site be covered to prevent dissemination of virus. Recommended coverings include the following: Gauze loosely secured by first aid adhesive tape (taking care to obtain history of tape sensitivity). When working in a health care setting, vaccinees should keep their vaccination site covered with gauze or a similar absorbent material. This dressing should, in turn, be covered with a semipermeable dressing. Products combining an absorbent base with an overlying semipermeable layer also can be used to cover the vaccination site. Healthcare workers do not need to be placed on leave after receiving a smallpox vaccination. Vaccinees in settings where close personal contact is likely (such as parents of infants and young children) should cover the vaccination site with gauze or a similar absorbent material, wear a shirt or other clothing that would cover the vaccination site, and also make sure to practice good hand hygiene. Note: The use of semipermeable dressing alone could cause maceration of the vaccination site and increased, prolonged irritation and itching at the site, thereby increasing touching, scratching, and contamination of the hands. Thus, only persons working in healthcare settings should use semipermeable dressings (over gauze or a similar absorbent material as described above). 8. Educate vaccinee: To avoid contact transmission of the virus, vaccinees must be cautioned to do the following: Do not rub or scratch the vaccination site. Keep the site covered and change gauze-only dressings every 1–2 days or if wet. Change semipermeable dressings at least every 3-5 days. Keep the vaccination site dry, covering it with a water-proof bandage while bathing. Discard gauze carefully in plastic zip bags. Set aside a laundry hamper for clothes, towels, sheets and other items that may come into contact with the vaccination site. Wash clothing or other materials that come into contact with the vaccination site in hot water with detergent and/or bleach. Wash hands afterward. Wash hands thoroughly with soap and warm water or with alcohol-based hand rubs such as gels or foams after touching the vaccination site, or bandages, clothing, towels, or sheets that have come into contact with the vaccination site. When the scab falls off, throw it away in a plastic zip bag. Report any problems by calling the phone number provided on the “Post-Vaccination and Follow-Up Information” sheet, calling your health care provider, or visiting and emergency room. Return 7 days after vaccination for a “take” check (to see if the vaccination was successful). 9. Record the vaccination: Record vaccination information as instructed by the CDC. Directions are from the Centers for Disease Control and Prevention, Photo Source: Centers for Disease Control and Prevention,
 in order not to contaminate the site or infect others who may come in contact with it. 7. Cover vaccination site: It is important that the vaccination site be covered to prevent dissemination of virus. Recommended coverings include the following: Gauze loosely secured by first aid adhesive tape (taking care to obtain history of tape sensitivity). When working in a health care setting, vaccinees should keep their vaccination site covered with gauze or a similar absorbent material. This dressing should, in turn, be covered with a semipermeable dressing. Products combining an absorbent base with an overlying semipermeable layer also can be used to cover the vaccination site. Healthcare workers do not need to be placed on leave after receiving a smallpox vaccination. Vaccinees in settings where close personal contact is likely (such as parents of infants and young children) should cover the vaccination site with gauze or a similar absorbent material, wear a shirt or other clothing that would cover the vaccination site, and also make sure to practice good hand hygiene. Note: The use of semipermeable dressing alone could cause maceration of the vaccination site and increased, prolonged irritation and itching at the site, thereby increasing touching, scratching, and contamination of the hands. Thus, only persons working in healthcare settings should use semipermeable dressings (over gauze or a similar absorbent material as described above). 8. Educate vaccinee: To avoid contact transmission of the virus, vaccinees must be cautioned to do the following: Do not rub or scratch the vaccination site. Keep the site covered and change gauze-only dressings every 1–2 days or if wet. Change semipermeable dressings at least every 3-5 days. Keep the vaccination site dry, covering it with a water-proof bandage while bathing. Discard gauze carefully in plastic zip bags. Set aside a laundry hamper for clothes, towels, sheets and other items that may come into contact with the vaccination site. Wash clothing or other materials that come into contact with the vaccination site in hot water with detergent and/or bleach. Wash hands afterward. Wash hands thoroughly with soap and warm water or with alcohol-based hand rubs such as gels or foams after touching the vaccination site, or bandages, clothing, towels, or sheets that have come into contact with the vaccination site. When the scab falls off, throw it away in a plastic zip bag. Report any problems by calling the phone number provided on the Post-Vaccination and Follow-Up Information sheet, calling your health care provider, or visiting and emergency room. Return 7 days after vaccination for a take check (to see if the vaccination was successful). 9. Record the vaccination: Record vaccination information as instructed by the CDC. Directions are from the Centers for Disease Control and Prevention, Photo Source: Centers for Disease Control and Prevention,")
28
Vaccinia: Reazioni comuni
Dolore al braccio Adenopatia Febbre Fino a 1/3 presenta reazioni tali da impedire le normali attività (scuola, lavoro, …) Minor reactions to smallpox vaccine are relatively common. More recent experience with smallpox vaccination suggests that fewer people will be ill enough to miss work.
 Minor reactions to smallpox vaccine are relatively common. More recent experience with smallpox vaccination suggests that fewer people will be ill enough to miss work.")
29
Eczema Vaccinatum Serious complication occurs in some vaccinees and their close contacts with either active or healed eczema. Vaccinial skin lesions extend to cover all or most of area once or currently afflicted with eczema. This complication occurs in about per million (or 1:50,000) vaccinated Vaccinia immune globulin (VIG) used for treatment. Photo Source: CDC.
 vaccinated. Vaccinia immune globulin (VIG) used for treatment. Photo Source: CDC.")
30
Reazioni alla vaccinazione antivaiolosa
Rischi per milione di prime vaccinazioni: Inoculazione Accidentale : > 500 Vaccinia Generalizzata : 242 Eczema Vaccinatum: 12 – 39 Vaccinia Progressiva : 1 – 2 Encefalite: 3 – 12 Morte: 1 - 2 Rischi molto ridotti nei già vaccinati Rischi più elevati negli immunodepressi Although serious adverse reactions to smallpox vaccine are rare, they do occur, and are more likely for first-time vaccinees. This slide summarizes the incidence of adverse reactions that were found during smallpox vaccination in the U.S. during the 1960’s.

31
Vaccinia Immune Globulin-VIG
Trattamento primario delle reazioni avverse Prodotto con plasma di soggetti vaccinati Stoccato ai CDC Disponibile solo per IM Indicazioni Eczema vaccinatum Vaccinia generalizzata Inoculazione Accidentale con lesioni estese Non raccomandato per la cheratite vaccinica Vaccinia immune globulin is used to treat severe adverse reactions to smallpox vaccination. It must be requested from CDC.

32
Vaccinia: Inoculazione accidentale
This is a picture of a child with accidental inoculation of vaccinia in the diaper area. This occurs from the virus being accidentally transferred from the vaccine site to another site on the body. It occurs more often in children because they are more prone to scratch the vaccine site. Usually this is not severe, but occasionally can cause severe problems, depending on where the virus is implanted (e.g., eye). This complication occurs in more than 500 per million (or 1:2000) vaccinated. If you see such a patient post-vaccination, you should notify public health (smallpox vaccine reactions are reportable), and consult an ID specialist for treatment. Most are managed conservatively, but they may require VIG if extensive or in a sensitive area. Photo Source: CDC.
. This complication occurs in more than 500 per million (or 1:2000) vaccinated. If you see such a patient post-vaccination, you should notify public health (smallpox vaccine reactions are reportable), and consult an ID specialist for treatment. Most are managed conservatively, but they may require VIG if extensive or in a sensitive area. Photo Source: CDC.")
33
Vaccinia: Inoculazione accidentale
We report a case of ocular vaccinia infection in an unvaccinated laboratory worker. The patient was infected by a unique strain used in an experiment performed partly outside a biosafety cabinet. Vaccination should continue to be recommended, but laboratories with unvaccinated workers should also implement more stringent biosafety practices. Lewis FMT, Chernak E, Goldman E, Li Y, Karem K, Damon IK, et al. Ocular vaccinia infection in laboratory worker, Philadelphia, Emerg Infect Dis [serial on the Internet] Jan [date cited].

34
Vaccinia Generalizzata
This occurs when the virus becomes disseminated through the bloodstream. This is typically not a life-threatening condition in persons who have an intact immune system. Lesions emerge between 6 and 9 days after vaccination, and range from a few lesions to generalized disease. This complication occurs in about 242 per million (or 1:4000) vaccinated. Usually self-limited. Only in severe cases, Vaccinia Immune Globulin (VIG) is indicated. Patients with active post-vaccination rashes are capable of transmitting vaccinia to susceptible immuno-compromised individuals. Since smallpox is vaccine is being reintroduced in the US, if you see a patient with post-vaccination cutaneous manifestations contact your local health department and hospital infection control. Photo Source: CDC.
 vaccinated. Usually self-limited. Only in severe cases, Vaccinia Immune Globulin (VIG) is indicated. Patients with active post-vaccination rashes are capable of transmitting vaccinia to susceptible immuno-compromised individuals. Since smallpox is vaccine is being reintroduced in the US, if you see a patient with post-vaccination cutaneous manifestations contact your local health department and hospital infection control. Photo Source: CDC.")
35
Vaccinia Progressiva Also known as Vaccinia Gangrenosa, this occurs when the virus progressively replicates locally. Occurs both among primary vaccinees and revaccinees: frequently fatal complication among those with immune deficiency disorders. Vaccinial lesion fails to heal and progresses to involve adjacent skin with necrosis of tissue, spreading to other parts of skin, bones, and viscera. This complication occurs in about per million vaccinated Vaccinia immune globulin (VIG) used for this problem. One case in a soldier with acquired immunodeficiency syndrome was successfully treated with VIG and ribavirin. Photo Source: CDC.
 used for this problem. One case in a soldier with acquired immunodeficiency syndrome was successfully treated with VIG and ribavirin. Photo Source: CDC.")
36
Vaccinia Progressiva Progressive vaccinia can cause necrosis that leads to amputation or death. Photo Source: CDC.

37
Progressive vaccinia in a military smallpox vaccinee United States, 2009
On [2 Mar 2009], a US Navy Hospital contacted the Poxvirus Program at CDC to report a possible case of PV in a male military smallpox vaccinee. The service member had been newly diagnosed with acute myelogenous leukemia M0 (AML M0). To support future public health needs adequately, the estimated national supply of therapeutics and diagnostic resources required to care for smallpox vaccine adverse events should be reevaluated. Vedi nota SMALLPOX VACCINATION, ADVERSE EVENTS - USA: PROGRESSIVE VACCINIA ********************************************* A ProMED-mail post < ProMED-mail is a program of the International Society for Infectious Diseases < Date: Tue 19 May 2009 Progressive vaccinia in a military smallpox vaccinee -- United States, 2009 Progressive vaccinia (PV), previously known as vaccinia necrosum, vaccinia gangrenosum, or disseminated vaccinia, is a rare, often fatal adverse event after vaccination with smallpox vaccine, which is made from live vaccinia virus (1). During recent vaccination programs potential cases of PV were investigated, but none met standard case definitions (2). PV has not been confirmed to have occurred in the United States since 1987 (3). On [2 Mar 2009], a US Navy Hospital contacted the Poxvirus Program at CDC to report a possible case of PV in a male military smallpox vaccinee. The service member had been newly diagnosed with acute myelogenous leukemia M0 (AML M0). During evaluation for a chemotherapy-induced neutropenic fever, he was found to have an expanding and nonhealing painless vaccination site 6.5 weeks after receipt of smallpox vaccine. Clinical and laboratory investigation confirmed that the vaccinee met the Brighton Collaboration and CDC adverse event surveillance guideline case definition for PV (4,5). This report summarizes the patient's protracted clinical course and the military and civilian interagency governmental, academic, and industry public health contributions to his complex medical management. The quantities of investigational and licensed therapeutics and diagnostics used were greater than anticipated based on existing smallpox preparedness plans. To support future public health needs adequately, the estimated national supply of therapeutics and diagnostic resources required to care for smallpox vaccine adverse events should be reevaluated. Case description On 13 Jan 2009, a healthy service member aged 20 years received a primary smallpox vaccination (ACAM2000 [Acambis, Inc., Cambridge, Massachusetts]) in accordance with the US Department of Defense smallpox vaccination policy*; no other vaccinations were administered that day. Twelve days later, the patient visited a local hospital with fever and headache of one day's duration and was admitted for workup of leukopenia after his white blood cell count was found to be 1400 cells/mm3. On [28 Jan 2009], after transfer to a US Navy tertiary-care facility, he was diagnosed with AML M0. On [30 Jan and 13 Feb 2009], the patient underwent 2 successive rounds of induction chemotherapy with cytarabine, idarubicin, and dexamethasone. Before initial chemotherapy, the vaccination site pustule had a central crust and measured approximately 1 cm [0.4 in] in diameter with minimal surrounding erythema. During the patient's hospital stay from the end of January to the beginning of March [2009], his vaccination site dressing was changed daily. On [2 Mar 2009], during the evaluation of neutropenic fever, the failure of the patient's vaccination site to heal was described. An annular lesion with a deep bulla, raised violaceous leading edge, and a central crust that bled with pressure was noted. The size of the lesion had progressed to approximately 4 x 4 cm [1.6 x 1.6 in] with minimal surrounding erythema or induration. The patient described no pain at the site, although he reported occasional pruritus. A swab of the lesion and serum were sent to CDC for viral and serologic analysis. Viral analysis of the swab by multiple real-time polymerase chain reaction (PCR) assays for orthopoxvirus and vaccinia yielded evidence of viral DNA; viral culture was positive for orthopoxvirus. Serum showed equivocal to absent levels of anti-orthopoxvirus immunoglobulin G (IgG) and immunoglobulin M (IgM) by enzyme-linked immunosorbent assay. The results of the diagnostic testing combined with the patient's medical history met the PV level 1 case definition as defined by the Brighton Collaboration and the confirmed case definition as described by CDC surveillance guidelines (4,5). The criteria met by both case definitions were 1) a documented clinical diagnosis of a disease that is known to be associated with cell-mediated immunodeficiency (in this case AML M0), 2) the primary vaccination site's failure to resolve (in this case more than 6 weeks post vaccination), and 3) the laboratory confirmation of vaccinia virus as the causative agent. On [3 Mar 2009], imiquimod was applied directly to the lesion. Within 24 hours of confirmation of PV on [4 Mar 2009], the patient received licensed Vaccinia Immune Globulin Intravenous (Human) (VIGIV) (Cangene Corporation, Winnipeg, Canada). On [5 Mar and 6 Mar 2009], oral and topical ST-246 (SIGA Technologies, Corvallis, Oregon) were administered under an Emergency Investigational New Drug (E-IND) application. The patient remained stable until the evening of [7 Mar 2009], when he became septic with _Pseudomonas aeruginosa_, likely from a perirectal abscess. He required intubation, maximal vasopressor support, multiple antibiotics, and stress dose corticosteroids. He then developed multiorgan failure and began continuous venovenous hemodialysis. During the next 12 days, the patient slowly stabilized. As a consequence of the duration and amount of vasopressor support, the patient required a bilateral trans-tibial amputation because of dry gangrene of his feet. During [6-19 Mar 2009] the patient received additional oral and topical ST-246 and VIGIV; his ST-246 levels were noted to be lower than those achieved both in healthy subjects in phase I clinical trials and in successful treatment of nonhuman primates with systemic orthopoxvirus disease. The lesion size remained unchanged, but the central crust of the vaccination site sloughed off, followed by most of the outer "ring" flattening, leaving a shallow ulcer with healthy-appearing granulation tissue. During his steroid taper, additional satellite lesions surrounding the vaccination site appeared on [18 Mar 2009], and viral DNA was detected again in the blood. These lesions became vesicular in nature, and on [26 Mar 2009], after a 2nd E-IND was issued, CMX001 (Chimerix, Inc., Research Triangle Park, North Carolina), a lipid conjugate of cidofovir, was administered. From [24 Mar 2009] onward, the satellite and main vaccination site lesions continued to crust, the scabs separated, and underlying tissue epithelialized. Blood viral DNA levels cleared on [29 Mar 2009]. On [10 Apr 2009], the borders of lesions again appeared raised; a shave biopsy grew methicillin-resistant _Staphylococcus aureus_, which responded to antibiotic therapy. The patient received intermittent granulocyte colony-stimulating factor, and his absolute neutrophil and lymphocyte count increased over time. By [1 May 2009], significant portions of the scabs/eschars had fallen off or were removed manually, revealing healthy epidermis. Numerous therapeutics with different biologic mechanisms were used to treat PV in this patient. From [21 Feb 2009] onward, the patient had remained in contact isolation, first for a _Clostridium difficile_ infection and then for his progressive vaccinia infection. On [5 May 2009], contact precautions were discontinued because of the lack of viable virus in lesion specimens from the previous 4 weeks. No cases of contact vaccinia were identified among this patient's health-care workers or close contacts. During [3 Mar-18 May 2009], nearly 200 clinical specimens (lesion and satellite swabs/crusts, ethylenediaminetetraacetic acid [EDTA] blood, bone marrow, and serum) were collected and submitted to CDC to evaluate disease progression and guide therapeutic interventions. After [23 Apr 2009], swabs from satellite lesions or the main vaccination site showed significantly reduced or absent levels of viral DNA, and no viable virus was detected after [2 Apr 2009]. Oropharyngeal sampling and bone marrow biopsies from early and late March [2009], respectively, were negative for vaccinia virus. Orthopoxvirus DNA was detected in EDTA blood at intermittent times during the course of the patient's infection; however, no viable virus was cultured from blood. As of [12 May 2009], the patient had no demonstrable IgM response to orthopoxvirus; IgG levels appeared fully reliant on VIGIV infusion. During [3 Mar-18 May 2009], a total of 20 conference calls to discuss patient status and treatment options were held between the Vaccine Healthcare Centers Network, Military Vaccine Agency (MILVAX), Bureau of Medicine and Surgery of the Navy, CDC, Food and Drug Administration (FDA), National Institutes of Health (NIH), SIGA Technologies, Chimerix, Inc., and academic and health-care professionals. As of [18 May 2009], MILVAX provided 22 and the Strategic National Stockpile (SNS) provided 254 vials of VIGIV used in treatment of this case. [Reported by: E Lederman, MD, H Groff, MD, T Warkentien, MD, A Reese, MD, US Naval Medical Center. D Hruby, PhD, T Bolken, D Grosenbach, PhD, S Yan, PhD, SIGA Technologies, Corvallis, Oregon. W Painter, MD, L Trost, MD, B Lampert, MD, Chimerix, Inc., Research Triangle Park, North Carolina. J Cohen, MD, National Institutes of Health; R Engler, MD, Walter Reed Vaccine Healthcare Center; W Davidson, MPH, S Smith, MS, K Wilkins, Z Braden, Y Li, PhD, I Damon, MD, Div of Viral and Rickettsial Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC] MMWR editorial note Although PV is a rare adverse event (one case per million during routine vaccination during ), its case fatality rate in primary US vaccinees was 15 percent despite treatment with massive amounts of VIG (intramuscular) (6). Extensive surgical debridement was sometimes required, even necessitating disarticulation of the arm to "debulk" the amount of infectious material (7). Before smallpox vaccination, patients are screened for numerous contraindications (8). At the time of his vaccination, the patient described in this report did not have any obvious signs or symptoms that would meet any exclusion criteria for vaccination. Training in use of, and careful adherence to, screening tools can identify vaccine candidates at risk for PV and other adverse events (2). Despite this, vaccinees with occult immunodeficiencies might not be recognized, and therefore appropriately deferring vaccination in these persons is not always possible. Lack of inflammation at the expanding vaccination site is the hallmark of PV. Any smallpox vaccinee who has an expanding, nonhealing, painless vaccination site without inflammation for more than 2 weeks should be evaluated for an underlying immunodeficiency, and diagnosis of and treatment for PV should be considered. Health-care providers should report suspected cases of PV or other adverse events to the Vaccine Adverse Event Reporting System (VAERS). Suspected cases of PV also should be reported to state health officials and CDC for clinical consultation and to obtain select therapeutics available only through the SNS. State health departments should call the CDC Emergency Operations Center at This patient's protracted clinical course is consistent with previously published cases reports and surveillance summaries. The development of progressive vaccinia, historically observed in patients with cellular immunodeficiencies, often leads to superinfection and subsequent sepsis (that is, fungal, parasitic, and bacterial infections resulting in toxic or septicemic shock, then ultimately death). Past treatment typically included massive doses of VIG, administration of thiosemicarbazone, blood products, and supportive care for accompanying infections (7,9). The improvement of progressive vaccinia in this patient was associated with receipt of VIGIV (the only licensed product for treatment of vaccinia adverse events stockpiled by the SNS), ST-246, and CMX001, and an increase in lymphocyte count. The use of 2 antiviral agents with different mechanisms of action (see note 1) was enabled by the research and development of medical countermeasures for smallpox preparedness activities, as well as the use of the emergency IND process. As of [18 May 2009], the patient had shed nearly all of the scab material on and around the vaccination site. The rapid mobilization of military, CDC, FDA, NIH, drug manufacturer, and academic and health-care human resources to review the case's status and to provide daily, then biweekly laboratory findings that guided treatment recommendations, was enabled by smallpox public health preparedness research and training efforts. Continuing medical education and reinforcement of training related to the prevention, early recognition, and treatment of smallpox vaccine-related adverse events should be part of smallpox vaccination programs. The patient described in this report received VIGIV in the amount originally estimated to treat 30 persons. The extraordinary amounts of VIGIV used to treat this single case of PV underscore the need to reevaluate the adequacy of the national stockpiled supply of this or other medical countermeasures (treatment or prophylactic). Such reevaluation, with additional focus on immunocompromised hosts, will aid in the smallpox vaccination program planning and overall smallpox preparedness efforts. References 1. CDC: Recommendations for using smallpox vaccine in a pre-event vaccination program. Supplemental recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR 2003; 52 (No. RR-7) [available at < 2. Vellozzi C, Lane JM, Averhoff F, et al: Generalized vaccinia, progressive vaccinia, and eczema vaccinatum are rare following smallpox (vaccinia) vaccination: United States surveillance, 2003. Clin Infect Dis 2005; 41: [abstract available at < 3. Redfield RR, Wright DC, James WD, Jones TS, Brown C, Burke DS: Disseminated vaccinia in a military recruit with human immunodeficiency virus (HIV) disease. N Engl J Med 1987; 316: 4. Nell P, Kohl KS, Graham PL, et al: Progressive vaccinia as an adverse event following exposure to vaccinia virus: case definition and guidelines of data collection, analysis, and presentation of immunization safety data. Vaccine 2007; 25: 5. CDC. Surveillance guidelines for smallpox vaccine (vaccinia) adverse reactions. MMWR 2006; 55 (No. RR-1) [available at < 6. Aragon TJ, Ulrich S, Fernyak S, Rutherford GW: Risks of serious complications and death from smallpox vaccination: a systematic review of the United States experience, BMC Public Health 2003; 3: 26 [abstract available at < 7. Maurer DM, Harrington B, Lane JM: Smallpox vaccine: contraindications, administration, and adverse reactions. Am Fam Physician 2003; 68: [available at < 8. Fulginiti VA, Papier A, Lane JM, Neff JM, Henderson DA: Smallpox vaccination: a review, part II. Adverse events. Clin Infect Dis 2003; 37: 9. Bray M, Wright ME: Progressive vaccinia. Clin Infect Dis 2003; 36: [abstract available at < 10. Quenelle, DC, Prichard MN, Keith KA, et al: Synergistic efficacy of the combination of ST-246 with CMX001 against orthopoxviruses. Antimicrob Agents Chemother 2007; 51: [available at < Note 1. ST-246 prevents viral egress, whereas CMX001 inhibits viral replication, and some data suggest they are synergistic in vitro (10). Note 2. * Information about US Department of Defense policies regarding smallpox vaccination and screening before smallpox vaccination is available at < CDC's clinical evaluation tools for smallpox vaccine adverse reactions are available at <
. To support future public health needs adequately, the estimated national supply of therapeutics and diagnostic resources required to care for smallpox vaccine adverse events should be reevaluated. Vedi nota. SMALLPOX VACCINATION, ADVERSE EVENTS - USA: PROGRESSIVE VACCINIA. ********************************************* A ProMED-mail post. < ProMED-mail is a program of the. International Society for Infectious Diseases < Date: Tue 19 May Progressive vaccinia in a military smallpox vaccinee -- United States, Progressive vaccinia (PV), previously known as vaccinia necrosum, vaccinia gangrenosum, or disseminated vaccinia, is a rare, often fatal adverse event after vaccination with smallpox vaccine, which is made from live vaccinia virus (1). During recent vaccination programs potential cases of PV were investigated, but none met standard case definitions (2). PV has not been confirmed to have occurred in the United States since 1987 (3). On [2 Mar 2009], a US Navy Hospital contacted the Poxvirus Program at CDC to report a possible case of PV in a male military smallpox vaccinee. The service member had been newly diagnosed with acute myelogenous leukemia M0 (AML M0). During evaluation for a chemotherapy-induced neutropenic fever, he was found to have an expanding and nonhealing painless vaccination site 6.5 weeks after receipt of smallpox vaccine. Clinical and laboratory investigation confirmed that the vaccinee met the Brighton Collaboration and CDC adverse event surveillance guideline case definition for PV (4,5). This report summarizes the patient s protracted clinical course and the military and civilian interagency governmental, academic, and industry public health contributions to his complex medical management. The quantities of investigational and licensed therapeutics and diagnostics used were greater than anticipated based on existing smallpox preparedness plans. To support future public health needs adequately, the estimated national supply of therapeutics and diagnostic resources required to care for smallpox vaccine adverse events should be reevaluated. Case description On 13 Jan 2009, a healthy service member aged 20 years received a primary smallpox vaccination (ACAM2000 [Acambis, Inc., Cambridge, Massachusetts]) in accordance with the US Department of Defense smallpox vaccination policy*; no other vaccinations were administered that day. Twelve days later, the patient visited a local hospital with fever and headache of one day s duration and was admitted for workup of leukopenia after his white blood cell count was found to be 1400 cells/mm3. On [28 Jan 2009], after transfer to a US Navy tertiary-care facility, he was diagnosed with AML M0. On [30 Jan and. 13 Feb 2009], the patient underwent 2 successive rounds of induction chemotherapy with cytarabine, idarubicin, and dexamethasone. Before initial chemotherapy, the vaccination site pustule had a central crust and measured approximately 1 cm [0.4 in] in diameter with minimal surrounding erythema. During the patient s hospital stay from the end of January to the beginning of March [2009], his vaccination site dressing was changed daily. On [2 Mar 2009], during the evaluation of neutropenic fever, the failure of the patient s vaccination site to heal was described. An annular lesion with a deep bulla, raised violaceous leading edge, and a central crust that bled with pressure was noted. The size of the lesion had progressed to approximately 4 x 4 cm [1.6 x 1.6 in] with minimal surrounding erythema or induration. The patient described no pain at the site, although he reported occasional pruritus. A swab of the lesion and serum were sent to CDC for viral and serologic analysis. Viral analysis of the swab by multiple real-time polymerase chain reaction (PCR) assays for orthopoxvirus and vaccinia yielded evidence of viral DNA; viral culture was positive for orthopoxvirus. Serum showed equivocal to absent levels of anti-orthopoxvirus immunoglobulin G (IgG) and immunoglobulin M (IgM) by enzyme-linked immunosorbent assay. The results of the diagnostic testing combined with the patient s medical history met the PV level 1 case definition as defined by the Brighton Collaboration and the confirmed case definition as described by CDC surveillance guidelines (4,5). The criteria met by both case definitions were 1) a documented clinical diagnosis of a disease that is known to be associated with cell-mediated immunodeficiency (in this case AML M0), 2) the primary vaccination site s failure to resolve (in this case more than 6 weeks post vaccination), and 3) the laboratory confirmation of vaccinia virus as the causative agent. On [3 Mar 2009], imiquimod was applied directly to the lesion. Within. 24 hours of confirmation of PV on [4 Mar 2009], the patient received licensed Vaccinia Immune Globulin Intravenous (Human) (VIGIV) (Cangene Corporation, Winnipeg, Canada). On [5 Mar and 6 Mar 2009], oral and topical ST-246 (SIGA Technologies, Corvallis, Oregon) were administered under an Emergency Investigational New Drug (E-IND) application. The patient remained stable until the evening of [7 Mar 2009], when he became septic with _Pseudomonas aeruginosa_, likely from a perirectal abscess. He required intubation, maximal vasopressor support, multiple antibiotics, and stress dose corticosteroids. He then developed multiorgan failure and began continuous venovenous hemodialysis. During the next 12 days, the patient slowly stabilized. As a consequence of the duration and amount of vasopressor support, the patient required a bilateral trans-tibial amputation because of dry gangrene of his feet. During [6-19 Mar 2009] the patient received additional oral and topical ST-246 and VIGIV; his ST-246 levels were noted to be lower than those achieved both in healthy subjects in phase I clinical trials and in successful treatment of nonhuman primates with systemic orthopoxvirus disease. The lesion size remained unchanged, but the central crust of the vaccination site sloughed off, followed by most of the outer ring flattening, leaving a shallow ulcer with healthy-appearing granulation tissue. During his steroid taper, additional satellite lesions surrounding the vaccination site appeared on [18 Mar 2009], and viral DNA was detected again in the blood. These lesions became vesicular in nature, and on [26 Mar 2009], after a 2nd E-IND was issued, CMX001 (Chimerix, Inc., Research Triangle Park, North Carolina), a lipid conjugate of cidofovir, was administered. From [24 Mar 2009] onward, the satellite and main vaccination site lesions continued to crust, the scabs separated, and underlying tissue epithelialized. Blood viral DNA levels cleared on [29 Mar 2009]. On [10 Apr 2009], the borders of lesions again appeared raised; a shave biopsy grew methicillin-resistant _Staphylococcus aureus_, which responded to antibiotic therapy. The patient received intermittent granulocyte colony-stimulating factor, and his absolute neutrophil and lymphocyte count increased over time. By [1 May 2009], significant portions of the scabs/eschars had fallen off or were removed manually, revealing healthy epidermis. Numerous therapeutics with different biologic mechanisms were used to treat PV in this patient. From [21 Feb 2009] onward, the patient had remained in contact isolation, first for a _Clostridium difficile_ infection and then for his progressive vaccinia infection. On [5 May 2009], contact precautions were discontinued because of the lack of viable virus in lesion specimens from the previous 4 weeks. No cases of contact vaccinia were identified among this patient s health-care workers or close contacts. During [3 Mar-18 May 2009], nearly 200 clinical specimens (lesion and satellite swabs/crusts, ethylenediaminetetraacetic acid [EDTA] blood, bone marrow, and serum) were collected and submitted to CDC to evaluate disease progression and guide therapeutic interventions. After [23 Apr 2009], swabs from satellite lesions or the main vaccination site showed significantly reduced or absent levels of viral DNA, and no viable virus was detected after [2 Apr 2009]. Oropharyngeal sampling and bone marrow biopsies from early and late March [2009], respectively, were negative for vaccinia virus. Orthopoxvirus DNA was detected in EDTA blood at intermittent times during the course of the patient s infection; however, no viable virus was cultured from blood. As of [12 May 2009], the patient had no demonstrable IgM response to orthopoxvirus; IgG levels appeared fully reliant on VIGIV infusion. During [3 Mar-18 May 2009], a total of 20 conference calls to discuss patient status and treatment options were held between the Vaccine Healthcare Centers Network, Military Vaccine Agency (MILVAX), Bureau of Medicine and Surgery of the Navy, CDC, Food and Drug Administration (FDA), National Institutes of Health (NIH), SIGA Technologies, Chimerix, Inc., and academic and health-care professionals. As of [18 May 2009], MILVAX provided 22 and the Strategic National Stockpile (SNS) provided 254 vials of VIGIV used in treatment of this case. [Reported by: E Lederman, MD, H Groff, MD, T Warkentien, MD, A Reese, MD, US Naval Medical Center. D Hruby, PhD, T Bolken, D Grosenbach, PhD, S Yan, PhD, SIGA Technologies, Corvallis, Oregon. W Painter, MD, L Trost, MD, B Lampert, MD, Chimerix, Inc., Research Triangle Park, North Carolina. J Cohen, MD, National Institutes of Health; R Engler, MD, Walter Reed Vaccine Healthcare Center; W Davidson, MPH, S Smith, MS, K Wilkins, Z Braden, Y Li, PhD, I Damon, MD, Div of Viral and Rickettsial Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC] MMWR editorial note Although PV is a rare adverse event (one case per million during routine vaccination during ), its case fatality rate in primary US vaccinees was 15 percent despite treatment with massive amounts of VIG (intramuscular) (6). Extensive surgical debridement was sometimes required, even necessitating disarticulation of the arm to debulk the amount of infectious material (7). Before smallpox vaccination, patients are screened for numerous contraindications (8). At the time of his vaccination, the patient described in this report did not have any obvious signs or symptoms that would meet any exclusion criteria for vaccination. Training in use of, and careful adherence to, screening tools can identify vaccine candidates at risk for PV and other adverse events (2). Despite this, vaccinees with occult immunodeficiencies might not be recognized, and therefore appropriately deferring vaccination in these persons is not always possible. Lack of inflammation at the expanding vaccination site is the hallmark of PV. Any smallpox vaccinee who has an expanding, nonhealing, painless vaccination site without inflammation for more than 2 weeks should be evaluated for an underlying immunodeficiency, and diagnosis of and treatment for PV should be considered. Health-care providers should report suspected cases of PV or other adverse events to the Vaccine Adverse Event Reporting System (VAERS). Suspected cases of PV also should be reported to state health officials and CDC for clinical consultation and to obtain select therapeutics available only through the SNS. State health departments should call the CDC Emergency Operations Center at This patient s protracted clinical course is consistent with previously published cases reports and surveillance summaries. The development of progressive vaccinia, historically observed in patients with cellular immunodeficiencies, often leads to superinfection and subsequent sepsis (that is, fungal, parasitic, and bacterial infections resulting in toxic or septicemic shock, then ultimately death). Past treatment typically included massive doses of VIG, administration of thiosemicarbazone, blood products, and supportive care for accompanying infections (7,9). The improvement of progressive vaccinia in this patient was associated with receipt of VIGIV (the only licensed product for treatment of vaccinia adverse events stockpiled by the SNS), ST-246, and CMX001, and an increase in lymphocyte count. The use of 2 antiviral agents with different mechanisms of action (see note 1) was enabled by the research and development of medical countermeasures for smallpox preparedness activities, as well as the use of the emergency IND process. As of. [18 May 2009], the patient had shed nearly all of the scab material on and around the vaccination site. The rapid mobilization of military, CDC, FDA, NIH, drug manufacturer, and academic and health-care human resources to review the case s status and to provide daily, then biweekly laboratory findings that guided treatment recommendations, was enabled by smallpox public health preparedness research and training efforts. Continuing medical education and reinforcement of training related to the prevention, early recognition, and treatment of smallpox vaccine-related adverse events should be part of smallpox vaccination programs. The patient described in this report received VIGIV in the amount originally estimated to treat 30 persons. The extraordinary amounts of VIGIV used to treat this single case of PV underscore the need to reevaluate the adequacy of the national stockpiled supply of this or other medical countermeasures (treatment or prophylactic). Such reevaluation, with additional focus on immunocompromised hosts, will aid in the smallpox vaccination program planning and overall smallpox preparedness efforts. References CDC: Recommendations for using smallpox vaccine in a pre-event vaccination program. Supplemental recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR 2003; 52 (No. RR-7) [available at. < 2. Vellozzi C, Lane JM, Averhoff F, et al: Generalized vaccinia, progressive vaccinia, and eczema vaccinatum are rare following smallpox (vaccinia) vaccination: United States surveillance, Clin Infect Dis 2005; 41: [abstract available at < 3. Redfield RR, Wright DC, James WD, Jones TS, Brown C, Burke DS: Disseminated vaccinia in a military recruit with human immunodeficiency virus (HIV) disease. N Engl J Med 1987; 316: Nell P, Kohl KS, Graham PL, et al: Progressive vaccinia as an adverse event following exposure to vaccinia virus: case definition and guidelines of data collection, analysis, and presentation of immunization safety data. Vaccine 2007; 25: CDC. Surveillance guidelines for smallpox vaccine (vaccinia) adverse reactions. MMWR 2006; 55 (No. RR-1) [available at < 6. Aragon TJ, Ulrich S, Fernyak S, Rutherford GW: Risks of serious complications and death from smallpox vaccination: a systematic review of the United States experience, BMC Public Health 2003; 3: 26 [abstract available at < 7. Maurer DM, Harrington B, Lane JM: Smallpox vaccine: contraindications, administration, and adverse reactions. Am Fam Physician 2003; 68: [available at < 8. Fulginiti VA, Papier A, Lane JM, Neff JM, Henderson DA: Smallpox. vaccination: a review, part II. Adverse events. Clin Infect Dis 2003; 37: Bray M, Wright ME: Progressive vaccinia. Clin Infect Dis 2003; 36: [abstract available at < 10. Quenelle, DC, Prichard MN, Keith KA, et al: Synergistic efficacy of the combination of ST-246 with CMX001 against orthopoxviruses. Antimicrob Agents Chemother 2007; 51: [available at < Note 1. ST-246 prevents viral egress, whereas CMX001 inhibits viral replication, and some data suggest they are synergistic in vitro (10). Note 2. * Information about US Department of Defense policies regarding smallpox vaccination and screening before smallpox vaccination is available at < CDC s clinical evaluation tools for smallpox vaccine adverse reactions are available at <")
38
Vaccinia Fetale Pregnancy (or close contact with a pregnant woman) is considered a contraindication to smallpox vaccination because of the risk of fetal vaccinia, which is known to cause birth defects and death. Photo Source: CDC.
 is considered a contraindication to smallpox vaccination because of the risk of fetal vaccinia, which is known to cause birth defects and death. Photo Source: CDC.")
39
A livello di popolazione, un episodio di vaiolo imporrebbe la vaccinazione di massa della popolazione, in cerchi concentrici, attorno ai primi casi. Negli S.U. si procede già a vaccinare gli operatori che si troverebbero in prima linea, e a predisporre piani di razionamento delle scorte di vaccino [ di dosi, giudicate insufficienti]. E’ stato varato un piano per riprendere la produzione di vaccino antivaioloso.

40
Incognite sul vaiolo Non è noto R0 [il tasso basico di riproduzione] del vaiolo le stime vanno da 2-3 a 10-20 Non è nota l’efficacia della protezione residua nei vaccinati da oltre trent’anni Non c’è accordo sulle stime di Rx [il tasso effettivo di riproduzione dell’infezione] C’è accordo sull’idea che l’introduzione del vaiolo in una popolazione metropolitana innescherebbe un’epidemia molto vasta
![Incognite sul vaiolo Non è noto R0 [il tasso basico di riproduzione] del vaiolo. le stime vanno da 2-3 a](http://slideplayer.it/slide/556099/1/images/40/Incognite+sul+vaiolo+Non+%C3%A8+noto+R0+%5Bil+tasso+basico+di+riproduzione%5D+del+vaiolo.+le+stime+vanno+da+2-3+a.jpg "Non è nota l’efficacia della protezione residua nei vaccinati da oltre trent’anni. Non c’è accordo sulle stime di Rx [il tasso effettivo di riproduzione dell’infezione] C’è accordo sull’idea che l’introduzione del vaiolo in una popolazione metropolitana innescherebbe un’epidemia molto vasta.")
41
I poxvirus - Lezione della Prof
I poxvirus - Lezione della Prof.ssa Azzi Gli ultimi colpi di coda del vaiolo - presentazione del Magg. F. Urbano

42
Smallpox Smallpox FAQ, 2005 Smallpox as a Biological Weapon: Medical & Public Health Management [JAMA 281(22),1999] Smallpox Fact Sheet Smallpox Virus Destruction Current Smallpox Vaccination Information Centers for Disease Control and Prevention Smallpox Vaccination in 2003: Key Information for Clinicians
![Smallpox Smallpox FAQ, Smallpox as a Biological Weapon: Medical & Public Health Management [JAMA 281(22),1999]](http://slideplayer.it/slide/556099/1/images/42/Smallpox+Smallpox+FAQ%2C+Smallpox+as+a+Biological+Weapon%3A+Medical+%26+Public+Health+Management+%5BJAMA+281%2822%29%2C1999%5D.jpg "Smallpox Fact Sheet. Smallpox Virus Destruction. Current Smallpox Vaccination Information Centers for Disease Control and Prevention. Smallpox Vaccination in 2003: Key Information for Clinicians.")
43
Training module Efficacissimo modulo didattico interattivo su ‘What every clinician should know about smallpox’ Impegna per circa 2,5 ore Offre domande di autovalutazione, ed eventualmente crediti [americani]

44
Altri collegamenti CDC:Main Smallpox Site: Specifics of smallpox vaccination strategy: Response Plan: Smallpox Vaccination Information Sheet (VIS): Infectious Disease Society of America:Smallpox vaccine, vaccination, complications and links to other sites: National Network for Immunization Information: (general information for public) (for heath professionals)
: Infectious Disease Society of America:Smallpox vaccine, vaccination, complications and links to other sites: National Network for Immunization Information: (general information for public) id=48 (for heath professionals)")
45
Grazie dell’attenzione
Domande?

Presentazioni simili