Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
INFIAMMAZIONE Dr C. Montesano

2
INFIAMMAZIONE Ippocrate: individua fenomeni quali rossore e gonfiore
Celso: definisce i 4 punti cardinali della infiammazione Galeno introduce il concetto della “funzione lesa” Hunter: non si tratta di una malattia ma di una risposta agli stimoli E. Metchnicoff: scopre i macrofagi Lewis: scopre il ruolo dell’Istamina Definizione generale L’Infiammazione è il più importante processo morboso reattivo locale che forma la base patologica delle malattie

3
Infiammazione (sintesi)
Che cosa è: processo reattivo (morboso) locale, base delle malattie Sede: vascolo-connettivale Nomenclatura: suffisso “ITE” con il nome dell’organo interessato, polmonite, pancreatite, gastrite…. Andamento stereotipato. Per effetto dei mediatori e nonostante la diversità degli stimoli. Fenomeni elementari costanti: vasodilatazione, variazione permeabiltà, migrazione cellulare. Decorso: variabile per quantità e diversità stimoli, e delle reattività dell’ospite ( danno variabile).
 locale, base delle malattie. Sede: vascolo-connettivale. Nomenclatura: suffisso ITE con il nome dell’organo interessato, polmonite, pancreatite, gastrite…. Andamento stereotipato. Per effetto dei mediatori e nonostante la diversità degli stimoli. Fenomeni elementari costanti: vasodilatazione, variazione permeabiltà, migrazione cellulare. Decorso: variabile per quantità e diversità stimoli, e delle reattività dell’ospite ( danno variabile).")
4
Cosa è l’infiammazione?
Rubor Tumor Calor Dolor (rossore) (gonfiore) (calore) (dolore) Quattro segni chiave (noti già a Greci e Romani)
 (gonfiore) (calore) (dolore) Quattro segni chiave. (noti già a Greci e Romani)")
5
INFIAMMAZIONE: generalità
L'infiammazione è una reazione complessa ad agenti nocivi, come i microbi e cellule danneggiate, di solito necrotiche. Si compone di molteplici meccanismi di risposta: vascolare, migrazione e attivazione dei leucociti, e di reazioni sistemiche La caratteristica unica del processo infiammatorio è la reazione dei vasi sanguigni, provocando l'accumulo di liquidi e leucociti nei tessuti extra-vascolare. La risposta infiammatoria è strettamente connessa con il processo di riparazione. L'infiammazione è fondamentalmente una risposta protettiva, il cui fine ultimo è quello di liberare l'organismo dalla causa iniziale di danno cellulare (per esempio, i microbi, tossine) e dalle conseguenze di tale danno (ad esempio, cellule e tessuti necrotici). Senza infiammazione, le infezioni sarebbero non controllate, le ferite non guarirebbero. Comunque, l'infiammazione e la riparazione possono essere potenzialmente dannosi: Reazioni infiammatorie, per esempio, sono alla base di comuni malattie croniche, come l'artrite reumatoide, l'arteriosclerosi, e la fibrosi polmonare, così come le reazioni di ipersensibilità a punture di insetti, droghe e tossine. Riparazione che comportano fibrosi possono portare a cicatrici deturpanti o formazioni di bande fibrose che causano ostruzione intestinale o di limitare la mobilità delle articolazioni The inflammatory response consists of two main components, a vascular reaction and a cellular reaction.
 e dalle conseguenze di tale danno (ad esempio, cellule e tessuti necrotici). Senza infiammazione, le infezioni sarebbero non controllate, le ferite non guarirebbero. Comunque, l infiammazione e la riparazione possono essere potenzialmente dannosi: Reazioni infiammatorie, per esempio, sono alla base di comuni malattie croniche, come l artrite reumatoide, l arteriosclerosi, e la fibrosi polmonare, così come le reazioni di ipersensibilità a punture di insetti, droghe e tossine. Riparazione che comportano fibrosi possono portare a cicatrici deturpanti o formazioni di bande fibrose che causano ostruzione intestinale o di limitare la mobilità delle articolazioni. The inflammatory response consists of two main components, a vascular reaction and a cellular reaction.")
6
Reazioni infiammatorie acute sono attivate da una varietà di stimoli
Infezioni (batteriche, virali, parassitarie) e le tossine microbiche Trauma Agenti fisici e chimici (lesione termica, ad esempio, ustioni o congelamento, irradiazione, alcuni prodotti chimici ambientali) Necrosi dei tessuti Corpi estranei (schegge, sporcizia, suture) Reazioni immunitarie (chiamate anche reazioni di ipersensibilità)
 e le tossine microbiche. Trauma. Agenti fisici e chimici (lesione termica, ad esempio, ustioni o congelamento, irradiazione, alcuni prodotti chimici ambientali) Necrosi dei tessuti. Corpi estranei (schegge, sporcizia, suture) Reazioni immunitarie (chiamate anche reazioni di ipersensibilità)")
7
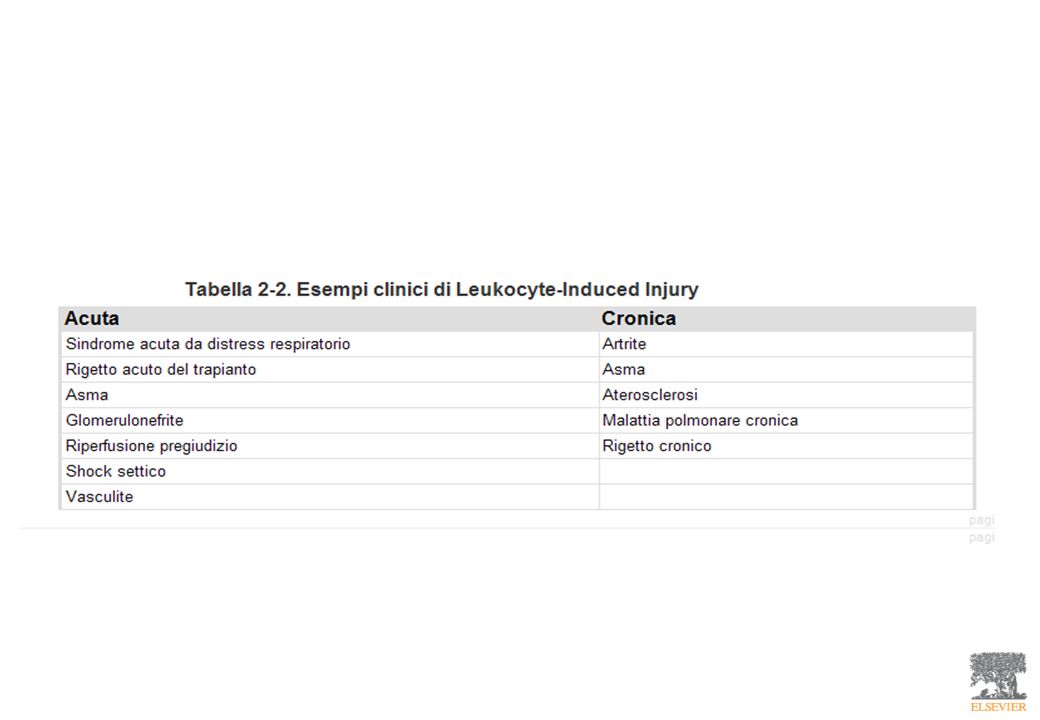
Prodotti leucocitari e lesione tissutale indotta da leucociti
Durante l’attivazione e la fagocitosi i leucociti liberano prodotti microbicidi e di altra natura non solo all’interno dei fagolisosomi ma anche nello spazio extracellulare Enzimi lisosomiali Metaboliti reattivi dell’ossigeno Prodotti dell’acido arachidonico (prostaglandine e leucotrieni) Possono causare lesioni endoteliali e danno tissutale e possono amplificare gli effetti dell’agente lesivo iniziale. Se persistente e non controllato lo stesso infiltrato leucocitario diviene l’agente lesivo, e il danno tissutale dipendente dai leucociti è alla base di patologie umane acute e croniche
 Possono causare lesioni endoteliali e danno tissutale e possono amplificare gli effetti dell’agente lesivo iniziale. Se persistente e non controllato lo stesso infiltrato leucocitario diviene l’agente lesivo, e il danno tissutale dipendente dai leucociti è alla base di patologie umane acute e croniche.")
10
Difetti funzionali dei leucociti
Difetti di adesione dei leucociti. Difetti in funzione phagolysosome Difetti di attività microbicida

11
Estinzione della risposta infiammatoria acuta

12
ACUTE INFLAMMATION: STIMULI
Acute inflammatory reactions are triggered by a variety of stimuli: Infections (bacterial, viral, parasitic) and microbial toxins Trauma (blunt and penetrating) Physical and chemical agents (thermal injury, e.g., burns or frostbite; irradiation; some environmental chemicals) Tissue necrosis (from any cause) Foreign bodies (splinters, dirt, sutures) Immune reactions (also called hypersensitivity reactions)
 and microbial toxins. Trauma (blunt and penetrating) Physical and chemical agents (thermal injury, e.g., burns or frostbite; irradiation; some environmental chemicals) Tissue necrosis (from any cause) Foreign bodies (splinters, dirt, sutures) Immune reactions (also called hypersensitivity reactions)")
13
Inflammation is divided into acute and chronic patterns
Acute inflammation is rapid in onset (seconds or minutes) and is of relatively short duration, lasting for minutes, several hours, or a few days; its main characteristics are the exudation of fluid and plasma proteins (edema) and the emigration of leukocytes, predominantly neutrophils. Chronic inflammation is of longer duration and is associated histologically with the presence of lymphocytes and macrophages, the proliferation of blood vessels, fibrosis, and tissue necrosis. Many factors modify the course and morphologic appearance of both acute and chronic inflammation. The vascular and cellular reactions of both acute and chronic inflammation are mediated by chemical factors that are derived from plasma proteins or cells and are produced in response to or activated by the inflammatory stimulus. Such mediators, acting singly, in combinations, or in sequence, then amplify the inflammatory response and influence its evolution. Necrotic cells or tissues themselves-whatever the cause of cell death-can also trigger the elaboration of inflammatory mediators. Such is the case with the acute inflammation after myocardial infarction. Inflammation is terminated when the offending agent is eliminated and the secreted mediators are broken down or dissipated. In addition, there are active anti-inflammatory mechanisms that serve to control the response and prevent it from causing excessive damage to the host.
 and is of relatively short duration, lasting for minutes, several hours, or a few days; its main characteristics are the exudation of fluid and plasma proteins (edema) and the emigration of leukocytes, predominantly neutrophils. Chronic inflammation is of longer duration and is associated histologically with the presence of lymphocytes and macrophages, the proliferation of blood vessels, fibrosis, and tissue necrosis. Many factors modify the course and morphologic appearance of both acute and chronic inflammation. The vascular and cellular reactions of both acute and chronic inflammation are mediated by chemical factors that are derived from plasma proteins or cells and are produced in response to or activated by the inflammatory stimulus. Such mediators, acting singly, in combinations, or in sequence, then amplify the inflammatory response and influence its evolution. Necrotic cells or tissues themselves-whatever the cause of cell death-can also trigger the elaboration of inflammatory mediators. Such is the case with the acute inflammation after myocardial infarction. Inflammation is terminated when the offending agent is eliminated and the secreted mediators are broken down or dissipated. In addition, there are active anti-inflammatory mechanisms that serve to control the response and prevent it from causing excessive damage to the host.")
14
The components of acute and chronic inflammatory responses
Many tissues and cells are involved in these reactions, including the fluid and proteins of plasma, circulating cells, blood vessels, and cellular and extracellular constituents of connective tissue The circulating cells include neutrophils, monocytes, eosinophils, lymphocytes, basophils, and “platelets”. The connective tissue cells are the mast cells, which intimately surround blood vessels; the connective tissue fibroblasts; resident macrophages; and lymphocytes. The extracellular matrix, consists of the structural fibrous proteins (collagen, elastin), adhesive glycoproteins (fibronectin, laminin, nonfibrillar collagen, tenascin, and others), and proteoglycans. The basement membrane is a specialized component of the extracellular matrix consisting of adhesive glycoproteins and proteoglycans.
, adhesive glycoproteins (fibronectin, laminin, nonfibrillar collagen, tenascin, and others), and proteoglycans. The basement membrane is a specialized component of the extracellular matrix consisting of adhesive glycoproteins and proteoglycans.")
15
The components of acute and chronic inflammatory responses: circulating cells and proteins, cells of blood vessels, and cells and proteins of the extracellular matrix 2-1 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 © 2005 Elsevier.")
16
Consequences of Defective or Excessive Inflammation
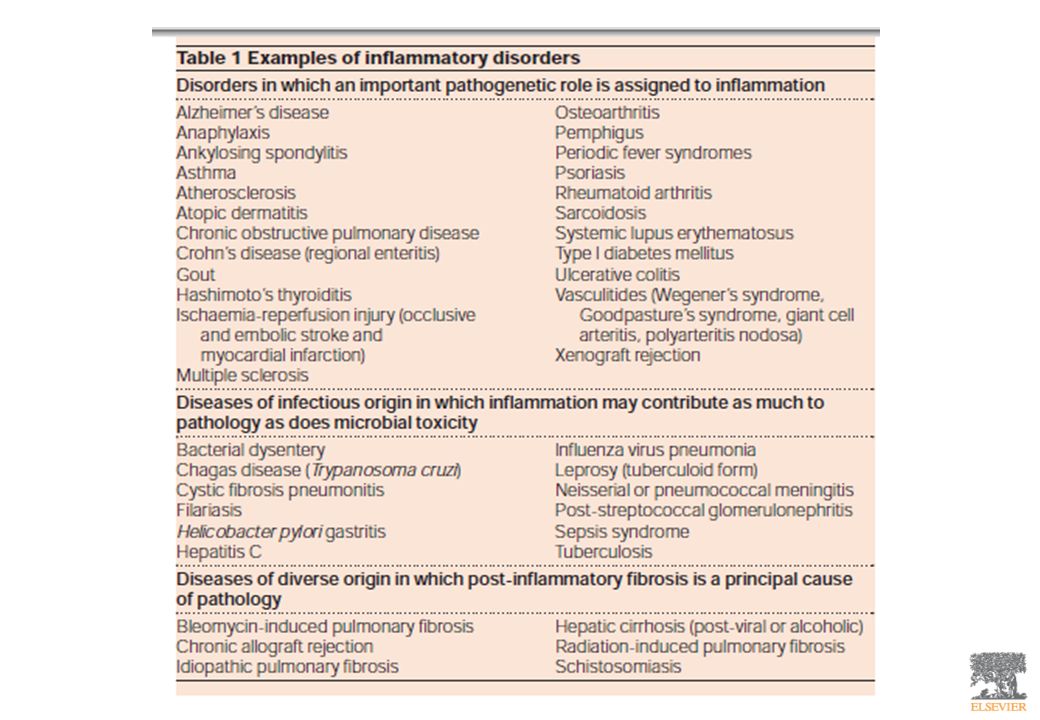
Defective inflammation typically results in increased susceptibility to infections and delayed healing of wounds and tissue damage. reflects the fundamental role of the inflammatory response in host defense, Delayed repair is because the inflammatory response is essential for clearing damaged tissues and debris, and provides the necessary stimulus to get the repair process started. Excessive inflammation is the basis of many categories of human disease. allergies, in which individuals mount unregulated immune responses against commonly encountered environmental antigens, autoimmune diseases, in which immune responses develop against normally tolerated self-antigens, are disorders in which the fundamental cause of tissue injury is inflammation. cancer, atherosclerosis and ischemic heart disease, and some neurodegenerative diseases such as Alzheimer disease (not primarily disorders of the immune system). prolonged inflammation and the fibrosis that accompanies it are responsible for much of the pathology in many chronic infectious, metabolic and other diseases.
. prolonged inflammation and the fibrosis that accompanies it are responsible for much of the pathology in many chronic infectious, metabolic and other diseases.")
17
Acute inflammation Acute inflammation is a rapid response to an injurious agent that serves to deliver mediators of host defense-leukocytes and plasma proteins-to the site of injury. Acute inflammation has three major components: (1) alterations in vascular caliber that lead to an increase in blood flow; (2) structural changes in the microvasculature that permit plasma proteins and leukocytes to leave the circulation; (3) emigration of the leukocytes from the microcirculation, their accumulation in the focus of injury, and their activation to eliminate the offending agent.
 alterations in vascular caliber that lead to an increase in blood flow; (2) structural changes in the microvasculature that permit plasma proteins and leukocytes to leave the circulation; (3) emigration of the leukocytes from the microcirculation, their accumulation. in the focus of injury, and their activation to eliminate the offending agent.")
18
The major local manifestations of acute inflammation
3. migrazione dei leucociti e accumulo nel sito del “danno” 2. Extravasazione e deposizione di fluido e proteine plasmatiche (edema) 3 2 3 2 1. dilatazione vascolare ed aumento del flusso sanguigno (che causa rossore e calore) 1 1 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 dilatazione vascolare ed aumento del flusso sanguigno (che causa rossore e calore) Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier.")
19
Acute inflammation Infiammazione acuta ha tre componenti principali:
(1) alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo
 alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo.")
20
Changes in Vascular Flow and Caliber
Changes in vascular flow and caliber begin early after injury and develop at varying rates depending on the severity of the injury. The changes occur in the following order: Vasodilation is one of the earliest manifestations of acute inflammation; sometimes, it follows a transient constriction of arterioles, lasting a few seconds. Vasodilation first involves the arterioles and then results in opening of new capillary beds in the area. Thus comes about increased blood flow, which is the cause of the heat and the redness. Vasodilation is induced by the action of several mediators, notably histamine and nitric oxide, on vascular smooth muscle. Vasodilation is quickly followed by increased permeability of the microvasculature, with the outpouring of protein-rich fluid into the extravascular tissues. The loss of fluid results in concentration of red cells in small vessels and increased viscosity of the blood, reflected by the presence of dilated small vessels packed with red cells and slower blood flow, a condition termed stasis. As stasis develops, leukocytes, principally neutrophils, accumulate along the vascular endothelium. Leukocytes then stick to the endothelium, and soon afterward they migrate through the vascular wall into the interstitial tissue, in processes that are described later.

21
Acute inflammation Infiammazione acuta ha tre componenti principali:
(1) alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo
 alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo.")
22
Increased Vascular Permeability
A hallmark of acute inflammation is increased vascular permeability leading to the escape of a protein-rich fluid (exudate) into the extravascular tissue. The loss of protein from the plasma reduces the intravascular osmotic pressure and increases the osmotic pressure of the interstitial fluid. Together with the increased hydrostatic pressure owing to increased blood flow through the dilated vessels, this leads to a marked outflow of fluid and its accumulation in the interstitial tissue. The net increase of extravascular fluid results in edema.
 into the extravascular tissue. The loss of protein from the plasma reduces the intravascular osmotic pressure and increases the osmotic pressure of the interstitial fluid. Together with the increased hydrostatic pressure owing to increased blood flow through the dilated vessels, this leads to a marked outflow of fluid and its accumulation in the interstitial tissue. The net increase of extravascular fluid results in edema.")
23
Increased Vascular Permeability
pressure and plasma colloid osmotic forces in normal and inflamed microcirculation A, Normal Normal hydrostatic pressure (red arrows) is about 32 mm Hg at the arterial end of a capillary bed and 12 mm Hg at the venous end; the mean colloid osmotic pressure of tissues is approximately 25 mm Hg (green arrows), which is equal to the mean capillary pressure. Although fluid tends to leave the precapillary arteriole, it is returned in equal amounts via the postcapillary venule, so that the net flow (black arrows) in or out is zero. B, Acute inflammation Arteriole pressure is increased to 50 mm Hg, the mean capillary pressure is increased because of arteriolar dilation, venous pressure increases to approximately 30 mm Hg. At the same time, osmotic pressure is reduced (averaging 20 mm Hg) because of protein leakage across the venule. The net result is an excess of extravasated fluid. Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 is about 32 mm Hg at the arterial end of a capillary bed and 12 mm Hg at the venous end; the mean colloid osmotic pressure of tissues is approximately 25 mm Hg (green arrows), which is equal to the mean capillary pressure. Although fluid tends to leave the precapillary arteriole, it is returned in equal amounts via the postcapillary venule, so that the net flow (black arrows) in or out is zero. B, Acute inflammation. Arteriole pressure is increased to 50 mm Hg, the mean capillary pressure is increased because of arteriolar dilation, venous pressure increases to approximately 30 mm Hg. At the same time, osmotic pressure is reduced (averaging 20 mm Hg) because of protein leakage across the venule. The net result is an excess of extravasated fluid. Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier.")
24
2-4 Diagrammatic representation of five mechanisms of increased vascular permeability in inflammation Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 © 2005 Elsevier.")
25
2-5 Vascular leakage induced by chemical mediators
2-5 Vascular leakage induced by chemical mediators. A, This is a fixed and cleared preparation of a rat cremaster muscle examined unstained by transillumination. One hour before sacrifice, bradykinin was injected over this muscle, and colloidal carbon was given intravenously. Plasma, loaded with carbon, escaped, but most of the carbon particles were retained by the basement membrane of the leaking vessels, with the result that these became "labeled" black. Note that not all the vessels leak-only the venules. In B, a higher power, the capillary network is faintly visible in the background. (Courtesy of Dr. Guido Majno, University of Massachusetts Medical School, Worcester, MA.) Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier.")
26
Perdita di liquidi nell’infiammazione acuta:
riassumendo Nell’infiammazione acuta, la perdita di liquidi dai vasi con aumentata permeabilità avviene in 3 fasi distinte: (1) una risposta immediata transitoria della durata di 30 minuti o meno, mediata principalmente dalle azioni di istamina e di leucotrieni sull’endotelio; (2) una risposta ritardata a partire da circa 2 ore e della durata di circa 8 ore, mediata dalla chinine, prodotti del complemento e altri fattori, e (3) una risposta prolungata che è più evidente in seguito a lesioni dell’endotelio come per esempio, dopo le ustioni.
 una risposta immediata transitoria della durata di 30 minuti o meno, mediata principalmente dalle azioni di istamina e di leucotrieni sull’endotelio; (2) una risposta ritardata a partire da circa 2 ore e della durata di circa 8 ore, mediata dalla chinine, prodotti del complemento e altri fattori, e. (3) una risposta prolungata che è più evidente in seguito a lesioni dell’endotelio come per esempio, dopo le ustioni.")
27
Acute inflammation Infiammazione acuta ha tre componenti principali:
(1) alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo
 alterazione del calibro vascolare che porta a un aumento del flusso sanguigno; (2) modifiche strutturali del microcircolo che permettono alle proteine plasmatiche e ai leucociti di lasciare il circolo s. (3) migrazione dei leucociti dal microcircolo e loro accumulo.")
28
CELLULAR EVENTS: LEUKOCYTE EXTRAVASATION AND PHAGOCYTOSIS
The sequence of events in the journey of leukocytes from the vessel lumen to the interstitial tissue, called extravasation, can be divided into the following steps: In the lumen: margination, rolling, and adhesion to endothelium. Vascular endothelium normally does not bind circulating cells or impede their passage. In inflammation, the endothelium has to be activated to permit it to bind leukocytes, as a prelude to their exit from the blood vessels. Transmigration across the endothelium (also called diapedesis) Migration in interstitial tissues toward a chemotactic stimulus
 Migration in interstitial tissues toward a chemotactic stimulus.")
29
of leukocyte migration through blood vessels
The multistep process of leukocyte migration through blood vessels The leukocytes first roll, then become activated and adhere to endothelium, then transmigrate across the endothelium, pierce the basement membrane, and migrate toward chemoattractants emanating from the source of injury. Different molecules play predominant roles in different steps of this process-selectins in rolling; chemokines in activating the neutrophils to increase avidity of integrins (in green); integrins in firm adhesion; and CD31 (PECAM-1) in transmigration. 2.6 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
; integrins in firm adhesion; and CD31 (PECAM-1) in transmigration Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier.")
31
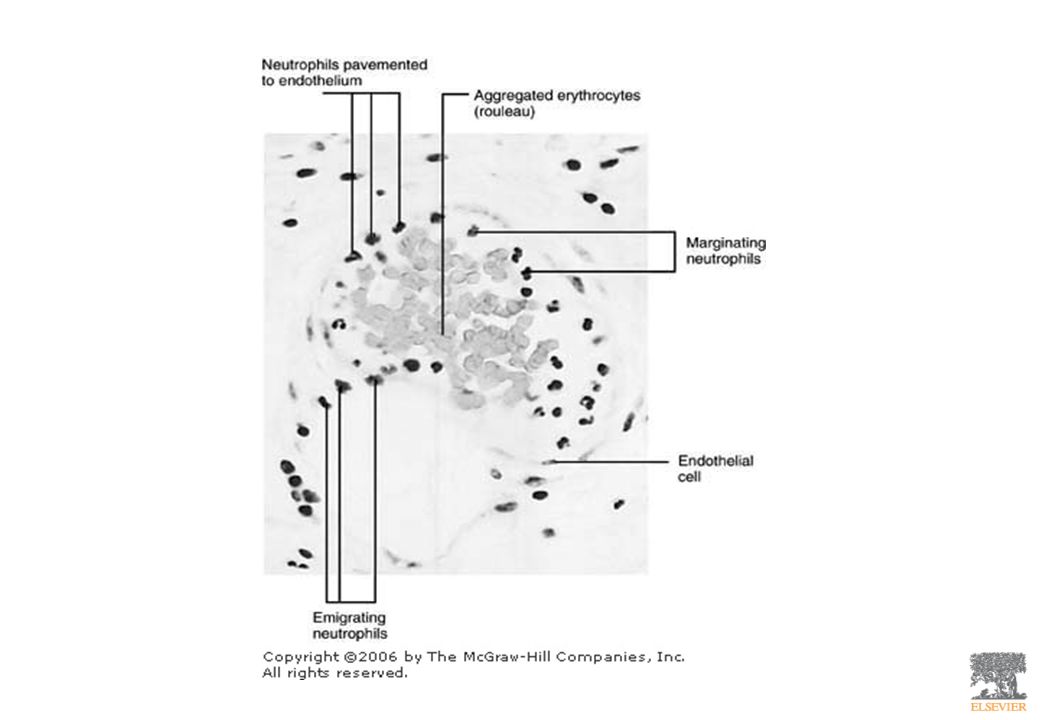
Leukocyte Margination and Diapedesis

32
Neutrophil Pavementing (lining the venule)
")
33
2.9

34
Neutrophil Transendothelial Migration (Diapedesis)
")
35
Schematic and histologic sequence of events following acute injury
Schematic and histologic sequence of events following acute injury. The photomicrographs are representative of the early (neutrophilic) (left) and later (mononuclear) cellular infiltrates (right) of infarcted myocardium. The kinetics of edema and cellular infiltration are approximations. For sake of simplicity, edema is shown as an acute transient response, although secondary waves of delayed edema and neutrophil infiltration can also occur. 2.8 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 (left) and later (mononuclear) cellular infiltrates (right) of infarcted myocardium. The kinetics of edema and cellular infiltration are approximations. For sake of simplicity, edema is shown as an acute transient response, although secondary waves of delayed edema and neutrophil infiltration can also occur Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier.")
36
The multistep process of leukocyte migration through blood vessels, shown here for neutrophils. The leukocytes first roll, then become activated and adhere to endothelium, then transmigrate across the endothelium, pierce the basement membrane, and migrate toward chemoattractants emanating from the source of injury. Different molecules play predominant roles in different steps of this process-selectins in rolling; chemokines in activating the neutrophils to increase avidity of integrins (in green); integrins in firm adhesion; and CD31 (PECAM-1) in transmigration. 2.6 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 © 2005 Elsevier.")
37
Adhesion Molecules Selectins, characterized by an extracellular N-terminal domain related to sugarbinding mammalian lectins, E-selectin (CD62E, endothelium), P-selectin (CD62P, endothelium and platelets), and L-selectin (CD62L, leukocytes) immunoglobulin family molecules include two endothelial adhesion molecules: ICAM-1 (intercellular adhesion molecule 1) and VCAM-1 (vascular cell adhesion molecule 1), CD31. Both these molecules serve as ligands for integrins found on leukocytes Integrins transmembrane heterodimeric glycoproteins expressed on many cell types, bind to ligands on endothelial cells, other leukocytes, and the extracellular matrix (CD11a/CD18 and CD11b/CD18 Mucin-like glycoproteins, such as heparan sulfate, serve as ligands for the leukocyte adhesion molecule called CD44. These glycoproteins are found in the extracellular matrix and on cell surfaces.
, P-selectin (CD62P, endothelium and platelets), and L-selectin (CD62L, leukocytes) immunoglobulin family molecules include two endothelial adhesion molecules: ICAM-1 (intercellular adhesion molecule 1) and VCAM-1 (vascular cell adhesion molecule 1), CD31. Both these molecules serve as ligands for integrins found on leukocytes. Integrins transmembrane heterodimeric glycoproteins expressed on many cell types, bind to ligands on endothelial cells, other leukocytes, and the extracellular matrix (CD11a/CD18 and CD11b/CD18. Mucin-like glycoproteins, such as heparan sulfate, serve as ligands for the leukocyte adhesion molecule called CD44. These glycoproteins are found in the extracellular matrix and on cell surfaces.")
38
Regulation of endothelial and leukocyte adhesion molecules
Redistribution of P-selectin Cytokine activation of endothelium Increased binding avidity of integrins 2.7 Downloaded from: StudentConsult (on 15 November :34 AM) © 2005 Elsevier
 © 2005 Elsevier.")
39
Leukocyte activation Microbes, products of necrotic cells, antigen-antibody complexes, and cytokines, including chemotactic factors, induce a number of responses in leukocytes that are part of the defensive functions of the leukocytes (neutrophils and monocytes/macrophages) and are referred to under the rubric of leukocyte activation Activation results from several signaling that are triggered in leukocytes, resulting in increases in cytosolic Ca2+ and activation of enzymes such as protein kinase C and phospholipase A2.
 and are referred to under the rubric of leukocyte activation. Activation results from several signaling that are triggered in leukocytes, resulting in increases in cytosolic Ca2+ and activation of enzymes such as protein kinase C and phospholipase A2.")
40
The functional responses that are induced on leukocyte activation include the following:
Production of arachidonic acid metabolites from phospholipids, as a result of activation of phospholipase A2 by increased intracellular calcium and other signals. Degranulation and secretion of lysosomal enzymes and activation of the oxidative burst (discussed below under phagocytosis). Secretion of cytokines, which amplify and regulate inflammatory reactions. Activated macrophages are the chief source of the cytokines that are involved in inflammation, but mast cells and other leukocytes may contribute. Modulation of leukocyte adhesion molecules. Different cytokines cause increased endothelial expression of adhesion molecules and increased avidity of leukocyte integrins, allowing firm adhesion of activated neutrophils to endothelium.
. Secretion of cytokines, which amplify and regulate inflammatory reactions. Activated macrophages are the chief source of the cytokines that are involved in inflammation, but mast cells and other leukocytes may contribute. Modulation of leukocyte adhesion molecules. Different cytokines cause increased endothelial expression of adhesion molecules and increased avidity of leukocyte integrins, allowing firm adhesion of activated neutrophils to endothelium.")
41
Leukocytes express a number of surface receptors that are involved in their activation
Toll-like receptors (TLRs), Different seven-transmembrane G-protein-coupled receptors Receptors for cytokines Receptors for opsonin: FcγRI (antibodies IgG), type 1 complement receptor, CR1 (complement proteins, C3b), C1q receptor (mannose-binding lectin MBL, fibronectin, fibrinogen, and C-reactive protein)
, Different seven-transmembrane G-protein-coupled receptors. Receptors for cytokines. Receptors for opsonin: FcγRI (antibodies IgG), type 1 complement receptor, CR1 (complement proteins, C3b), C1q receptor (mannose-binding lectin MBL, fibronectin, fibrinogen, and C-reactive protein)")
42
Different classes of cell surface receptors of leukocytes recognize different stimuli.
The receptors initiate responses that mediate the functions of the leukocytes. 2.10 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
43
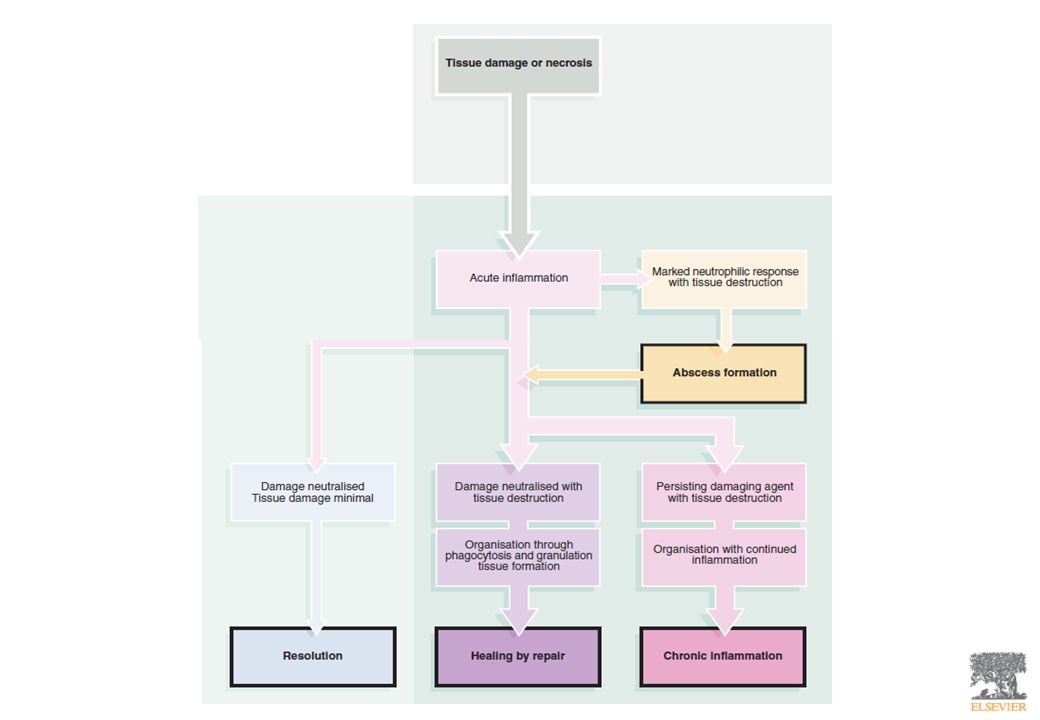
Outcomes of acute inflammation:
resolution, healing by fibrosis, or chronic inflammation Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
45
Chemical mediators of inflammation
2-12 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
46
AMINE VASOATTIVE ISTAMINA SEROTONINA

47
Istamina principal mediator of the immediate transient phase of increased vascular permeability, causing venular gaps Histamine is widely distributed in tissues, the richest source being the mast cells that are normally present in the connective tissue adjacent to blood vessels It is also found in blood basophils and platelets. Preformed histamine is present in mast cell granules and is released by mast cell degranulation in response to a variety of stimuli: (1) physical injury such as trauma, cold, or heat; (2) immune reactions involving binding of antibodies to mast cells; (3) fragments of complement called anaphylatoxins (C3a and C5a); (4) histamine-releasing proteins derived from leukocytes; (5) neuropeptides (e.g., substance P); and (6) cytokines (IL-1, IL-8). histamine causes dilation of the arterioles and increases the permeability of venules (it, however, constricts large arteries) A flat spread of omentum showing mast cells around blood vessels and in the interstitial tissue. Stained with metachromatic stain to identify the mast cell granules (dark blue or purple). The red structures are fat globules stained with fat stain. (Courtesy of Dr. G. Majno, University of Massachusetts Medical School, Worcester, MA.) 2.13 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 physical injury such as trauma, cold, or heat; (2) immune reactions involving binding of antibodies to mast cells; (3) fragments of complement called anaphylatoxins (C3a and C5a); (4) histamine-releasing proteins derived from leukocytes; (5) neuropeptides (e.g., substance P); and. (6) cytokines (IL-1, IL-8). histamine causes dilation of the arterioles and increases the permeability of venules (it, however, constricts large arteries) A flat spread of omentum showing mast cells around blood vessels and in the interstitial tissue. Stained with metachromatic stain to identify the mast cell granules (dark blue or purple). The red structures are fat globules stained with fat stain. (Courtesy of Dr. G. Majno, University of Massachusetts Medical School, Worcester, MA.) Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
48
Serotonina Preformed vasoactive mediator with actions similar to those of histamine. Present in platelets and enterochromaffin cells, and in mast cells in rodents but not humans. Release of serotonin (and histamine) from platelets is stimulated when platelets aggregate after contact with collagen, thrombin, adenosine diphosphate (ADP), and antigen-antibody complexes. Platelet aggregation and release are also stimulated by Platelet Activating Factors (PAF) derived from mast cells during IgE-mediated reactions. In this way, the platelet release reaction results in increased permeability during immunologic reactions. 2.13 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 from platelets is stimulated when platelets aggregate after contact with collagen, thrombin, adenosine diphosphate (ADP), and antigen-antibody complexes. Platelet aggregation and release are also stimulated by Platelet Activating Factors (PAF) derived from mast cells during IgE-mediated reactions. In this way, the platelet release reaction results in increased permeability during immunologic reactions Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
49
Platelet Activating Factors (PAF) Fattore attivante piastrine
A variety of cell types, including platelets, basophils (and mast cells), neutrophils, monocytes/macrophages, and endothelial cells, can elaborate PAF, in both secreted and cell-bound forms PAF causes platelet aggregation, but it is now known to have multiple inflammatory effects PAF causes vasoconstriction and bronchoconstriction, and at extremely low concentrations it induces vasodilation and increased venular permeability with a potency 100 to 10,000 times greater than that of histamine. PAF also causes increased leukocyte adhesion to endothelium (by enhancing integrin-mediated leukocyte binding), chemotaxis, degranulation, and the oxidative burst
, neutrophils, monocytes/macrophages, and endothelial cells, can elaborate PAF, in both secreted and cell-bound forms. PAF causes platelet aggregation, but it is now known to have multiple inflammatory effects. PAF causes vasoconstriction and bronchoconstriction, and at extremely low concentrations it induces vasodilation and increased venular permeability with a potency 100 to 10,000 times greater than that of histamine. PAF also causes increased leukocyte adhesion to endothelium (by enhancing integrin-mediated leukocyte binding), chemotaxis, degranulation, and the oxidative burst.")
50
PROTEINE PLASMATICHE Sistema del Complemento Sistema delle chinine
Sistema della coagulazione

51
Complemento Increased vascular permeability, chemotaxis, and opsonization. Complement proteins are present as INACTIVE forms in plasma and are numbered C1 through C9 Many of these proteins are activated to become proteolytic enzymes that degrade other complement proteins The critical step is the activation of the third and most abundant component, C3. Cleavage of C3 can occur by one of three pathways: the classical pathway, the alternative pathway, the lectin pathway.

52
Complemento classical pathway which is triggered by fixation of C1 to antibody (IgM or IgG) combined with antigen lectin pathway in which plasma mannose-binding lectin binds to carbohydrates on microbes and directly activates C1 alternative pathway which can be triggered by microbial surface molecules (e.g., endotoxin, or LPS), complex polysaccharides, cobra venom, and other substances, in the absence of antibody Il risultato è sempre l’attivazione della C3 convertasi che cliva il C3 in C3a e C3b
, complex polysaccharides, cobra venom, and other substances, in the absence of antibody. Il risultato è sempre l’attivazione della C3 convertasi che cliva il C3 in C3a e C3b.")
53
Complemento Il risultato è sempre l’attivazione della C3 convertasi che cliva il C3 in C3a e C3b

54
C5 convertasi

55
cell lysis by the MAC, and
The biologic functions of the complement system fall into two general categories: cell lysis by the MAC, and the effects of proteolytic fragments of complement. Complement-derived factors mediate a variety of phenomena in acute inflammation: Leukocyte adhesion, chemotaxis, and activation. C5a is a powerful chemotactic agent for neutrophils, monocytes, eosinophils, and basophils. Vascular phenomena. C3a, C5a, and, to a lesser extent, C4a are split products of the corresponding complement components that stimulate histamine release from mast cells and thereby increase vascular permeability and cause vasodilation. They are called anaphylatoxins because they have effects similar to those of mast cell mediators that are involved in the reaction called anaphylaxis. C5a also activates the lipoxygenase pathway of arachidonic acid (AA) metabolism in neutrophils and monocytes, causing further release of inflammatory mediators. 2.14 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 metabolism in neutrophils and monocytes, causing further release of inflammatory mediators Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
56
Anafilotossine C3a, C5a (e C4a)
Vascular phenomena. C3a, C5a, and, to a lesser extent, C4a are split products of the corresponding complement components that stimulate histamine release from mast cells and thereby increase vascular permeability and cause vasodilation. They are called anaphylatoxins because they have effects similar to those of mast cell mediators that are involved in the reaction called anaphylaxis. C5a also activates the lipoxygenase pathway of arachidonic acid (AA) metabolism in neutrophils and monocytes, causing further release of inflammatory mediators. C3 e C5 possono essere attivati da diversi enzimi proteolitici presenti nell’essudato infiammatorio: plasmina ed enzimi lisosomiali rilasciati dai neutrofili.
 metabolism in neutrophils and monocytes, causing further release of inflammatory mediators. C3 e C5 possono essere attivati da diversi enzimi proteolitici presenti nell’essudato infiammatorio: plasmina ed enzimi lisosomiali rilasciati dai neutrofili.")
57
Ruolo multiplo del fattore di Hageman (XIIa)
attivato dal contatto con una superficie caricata negativamente

58
Chininogeno ad alto peso molecolare
Legame a diversi recettori Che stimolano infiammazione: Mobilizzazione di selectina P Produzione di chemochine Espressione di molecole di adesione endoteliali per le integrine leucocitarie Produzione prostaglandine Produzione di PAF Produzione di NO Aumenta la permeabilità vascolare Contrazione del muscolo liscio, Dilatazione dei vasi sanguigni Dolore 2-15 Interrelationships between the four plasma mediator systems triggered by activation of factor XII (Hageman factor). Note that thrombin induces inflammation by binding to protease-activated receptors (principally PAR-1) on platelets, endothelium, smooth muscle cells, and other cells. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
. Note that thrombin induces inflammation by binding to protease-activated receptors (principally PAR-1) on platelets, endothelium, smooth muscle cells, and other cells. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
59
CITOCHINE E CHEMOCHINE
Fattore di necrosi tumorale, TNF-alfa Interleuchina-1, IL-1

60
2-18 Major effects of interleukin-1 (IL-1) and tumor necrosis factor (TNF) in inflammation.
Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
61
Macrophage Pro-inflammatory Mediators
Macrophage ingests and degrades bacteria and is activated to secrete monokines Activates vascular endothelium Activates lymphocytes Local tissue destruction increased access of effector cells Chemotactic factor for leukocytes increases access of effector cells Activates binding by b2 integrins endothelium and increases vascular permeability which leads to increased entry of IgG complement and cells and increased fluid drainage to lymph nodes Lymphocyte activation increased antibody production Activates NK cells induces the differentiation of CD4 T cells into TH1 cells Fever Production of IL-6 Local effects Systemic effects Fver Mobilisation of metabolites Shock Induces acute phase protein production IL-1 IL-8 TNF-a IL-6 IL-12

62
Cytokines from activated macrophages coordinate the
body’s response to infection. FEVER What are acute phase proteins?

63
The acute phase response increases the supply of recognition molecules of innate immunity.

64
Acute-phase proteins (CRP and MBP) produced by the liver can each
bind structural features of bacterial cells. Upon binding they act as opsonins and also activate complement (lysis – dotted bacterial margin). MBP CRP (found as far back as invertebrates)
. MBP. CRP. (found as far back as invertebrates)")
65
Encapsulated bacteria are more efficiently engulfed by phagocytosis
when the bacteria are coated with antibody, C3b, CRP or MBP.

66
Cytokines from activated macrophages coordinate the
body’s response to infection. FEVER Has fever any benefits?

67
FEVER IL-1, IL-6 and TNFα (endogenous pyrogens) released by macrophages act on the hypothalamus and on muscle and fat cells to raise body temperature (induce fever). Fever helps the immune system fight infection because: Most bacterial and viral pathogens grow better at temperatures lower than human body temperature (37oC). 2. Human cells become more resistant to the deleterious effects of TNFα at raised temperatures. 3. Adaptive immunity becomes more potent at higher temperatures (antigen processing is enhanced). How else do macrophages promote T lymphocytes in the inflamed region?
. Fever helps the immune system fight infection because: Most bacterial and viral pathogens grow better at temperatures. lower than human body temperature (37oC). 2. Human cells become more resistant to the deleterious effects of. TNFα at raised temperatures. 3. Adaptive immunity becomes more potent at higher temperatures. (antigen processing is enhanced). How else do macrophages promote T lymphocytes in the inflamed region")
68
Macrophage cytokines influencing T cells:
IL A general activator of all T cells IL T cell growth and differentiation IL Preferentially activates TH1 cells TH1 cytokines released in response to macrophage (MØ) cytokines: Interferon-γ (IFN- γ) expression of MHC on MØs and other local cells MØ antigen processing induces MØ maturation NK cell activity inhibits TH2 cells causes antiviral effects Tumour necrosis factor (TNF) several roles in inflammation but high local levels can cause tissue destruction and has potent systemic effect of causing weight loss.
 cytokines: Interferon-γ (IFN- γ) expression of MHC on MØs and other local cells. MØ antigen processing. induces MØ maturation. NK cell activity. inhibits TH2 cells. causes antiviral effects. Tumour necrosis factor (TNF) several roles in inflammation but high local. levels can cause tissue destruction and has. potent systemic effect of causing weight loss.")
69
Th1 cell cytokine effects on MØs

70
NITRIC OXIDE (NO) factor released from endothelial cells that caused vasodilation by relaxing vascular smooth muscle and was therefore called endothelium-derived relaxing factor 2-19 Functions of nitric oxide (NO) in blood vessels and macrophages, produced by two NO synthase enzymes. NO causes vasodilation, and NO free radicals are toxic to microbial and mammalian cells. NOS, nitric oxide synthase. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 in blood vessels and macrophages, produced by two NO synthase enzymes. NO causes vasodilation, and NO free radicals are toxic to microbial and mammalian cells. NOS, nitric oxide synthase. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
71
Figure 2-20 Ultrastructure and contents of neutrophil granules, stained for peroxidase activity. The large peroxidase-containing granules are the azurophil granules; the smaller peroxidase-negative ones are the specific granules (SG). N, portion of nucleus; BPI, bactericidal permeability increasing protein. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
72
Metaboliti dell’acido arachidonico
Prostaglandine Leucotrieni Lipossine

73
2-16 Generation of arachidonic acid metabolites and their roles in inflammation. The molecular targets of action of some anti-inflammatory drugs are indicated by a red X. COX, cyclooxygenase; HETE, hydroxyeicosatetraenoic acid; HPETE, hydroperoxyeicosatetraenoic acid. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
74
Figure 2-17 Biosynthesis of leukotrienes and lipoxins by cell-cell interaction. Activated neutrophils generate LTB4 from arachidonic acid-derived LTA4 by the action of 5-lipoxygenase, but they do not possess LTC4-synthase activity and consequently do not produce LTC4. In contrast, platelets cannot form LTC4 from endogenous substrates, but they can generate LTC4 and lipoxins from neutrophil-derived LTA4. (Courtesy of Dr. C. Serhan, Brigham and Women's Hospital, Boston, MA.) Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
75
Figure 2-22 Events in the resolution of inflammation: (1) return to normal vascular permeability; (2) drainage of edema fluid and proteins into lymphatics or (3) by pinocytosis into macrophages; (4) phagocytosis of apoptotic neutrophils and (5) phagocytosis of necrotic debris; and (6) disposal of macrophages. Macrophages also produce growth factors that initiate the subsequent process of repair. Note the central role of macrophages in resolution. (Modified from Haslett C, Henson PM: In Clark R, Henson PM (eds): The Molecular and Cellular Biology of Wound Repair. New York, Plenum Press, 1996.) Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
76
Figure 2-27 Maturation of mononuclear phagocytes
Figure 2-27 Maturation of mononuclear phagocytes. (From Abbas AK, et al: Cellular and Molecular Immunology, 5th ed. Philadelphia, Saunders, 2003.) Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
77
Figure 2-28 The roles of activated macrophages in chronic inflammation
Figure 2-28 The roles of activated macrophages in chronic inflammation. Macrophages are activated by cytokines from immune-activated T cells (particularly IFN-γ) or by nonimmunologic stimuli such as endotoxin. The products made by activated macrophages that cause tissue injury and fibrosis are indicated. AA, arachidonic acid; PDGF, platelet-derived growth factor; FGF, fibroblast growth factor; TGFβ, transforming growth factor β. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 or by nonimmunologic stimuli such as endotoxin. The products made by activated macrophages that cause tissue injury and fibrosis are indicated. AA, arachidonic acid; PDGF, platelet-derived growth factor; FGF, fibroblast growth factor; TGFβ, transforming growth factor β. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
78
Figure 2-29 A, Chronic inflammation in the lung, showing all three characteristic histologic features: (1) collection of chronic inflammatory cells (*), (2) destruction of parenchyma (normal alveoli are replaced by spaces lined by cuboidal epithelium, arrowheads), and (3) replacement by connective tissue (fibrosis, arrows). B, By contrast, in acute inflammation of the lung (acute bronchopneumonia), neutrophils fill the alveolar spaces and blood vessels are congested. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
79
Figure 2-30 Mechanisms of macrophage accumulation in tissues
Figure 2-30 Mechanisms of macrophage accumulation in tissues. The most important is continued recruitment from the microcirculation. (Adapted from Ryan G, Majno G: Inflammation. Kalamazoo, MI, Upjohn, 1977.) Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier.")
80
Figure 2-31 Macrophage-lymphocyte interactions in chronic inflammation
Figure 2-31 Macrophage-lymphocyte interactions in chronic inflammation. Activated lymphocytes and macrophages influence each other and also release inflammatory mediators that affect other cells. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
81
Figure 2-32 A focus of inflammation showing numerous eosinophils.
Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
82
Figure 2-33 Typical tuberculous granuloma showing an area of central necrosis, epithelioid cells, multiple Langhans-type giant cells, and lymphocytes. Downloaded from: StudentConsult (on 15 November :35 AM) © 2005 Elsevier
 © 2005 Elsevier.")
Presentazioni simili

 064825120 - fax.>")















>")
>")
