Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Come riconoscere le disfunzioni protesiche
Salvatore Felis

2
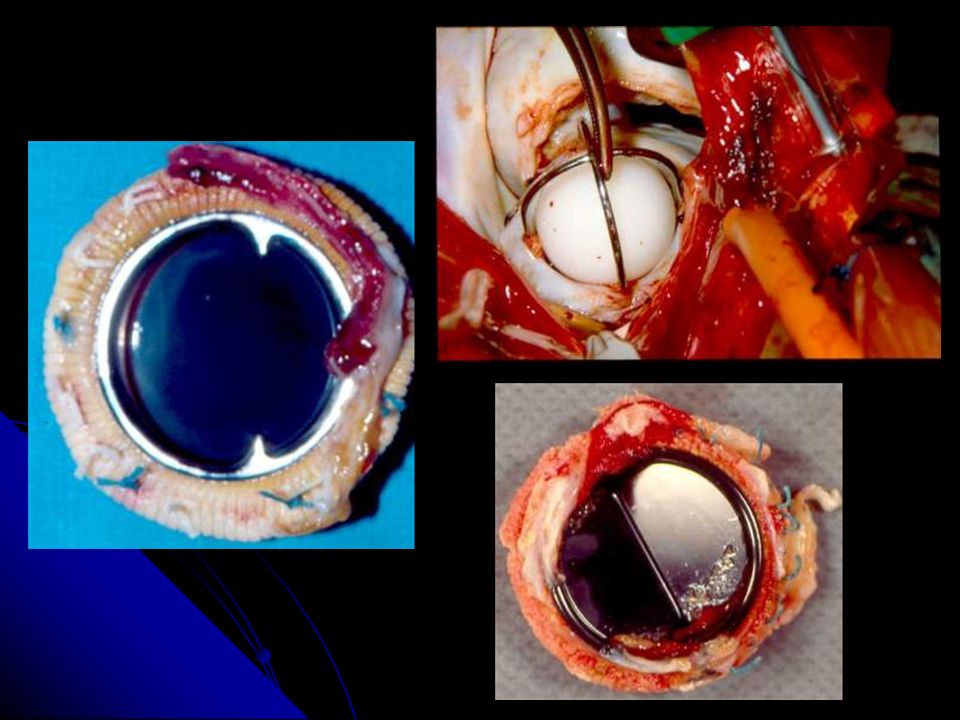
Bileaflet- tilting-disk
TIPI di PROTESI Hancock Carpentier-Edwards Ionescu-Shiley Bioprosthetic Heterograft Homograft Starr-Edwards Bjork-Shiley Medtronic-Hall Omnicarbon St. Jude Medical Carbomedics Edwards- Duromedics Mechanical Caged-ball Single-tilting- disk Bileaflet- tilting-disk MODEL TYPE

3
Normal Values for Doppler Echocardiographic Assessment of Heart Valve Prostheses:
aortic valve position Carbomedics Bileaflet St. Jude Medical Bileaflet n. Pz gr. max. gr.med n. Pz gr. max. gr.med 8.41 ± 2.83 19.05 ± 7.04 57 27 12.68 ± 4.29 26.31 ± 10.25 111 21 11.33 ± 3.8 24.61 ± 6.93 120 23 5.8 ± 3.2 12.53 ± 4.69 6 29 9.34 ± 4.65 20.25 ± 8.69 103 25 11.61 ± 5.08 33.3 ± 11.19 63 19 20.1 ± 7.1 33.4 ± 13.2 7 17 18.96 ± 6.27 35.17 ± 11.16 100 19 15.82 ± 5.67 28.34 ± 9.94 207 21 13.77 ± 5.33 25.28 ± 7.89 236 23 10 ± 6 16.0 4 31 9.86 ± 2.9 17.72 ± 6.42 18 29 11.18 ± 4.82 19.85 ± 7.55 82 27 12.65 ± 5.14 22.57 ± 7.68 169 25 Rosenhek R. Journal of American Society of Echocardiography

4
Normal Values for Doppler Echocardiographic Assessment of Heart Valve Prostheses:
aortic valve position Carpentier-Edwards pericadial Stented bioprothesis Toronto stentless Porcine Stentless bioprothesis n. Pz gr. max. gr.med n. Pz gr. max. gr.med 11.6 17.6 ± 0 1 29 13.01 ± 5.27 21.72 ± 8.57 20 23 9.04 ± 2.27 16.46 ± 5.41 5 25 5.6 19.2 ± 0 27 20.3 ± 9.08 25.69 ± 9.9 34 21 24.19 ± 8.6 32.13 ± 3.35 14 19 4.6 10.9 1 20 7.56 ± 4.4 18.64 ± 11.8 9 21 23.0 22 3.94 ± 2.15 7.91 ± 4.17 200 29 4.8 ± 2.33 9.96 ± 4.56 240 27 6.2 ± 3.05 12.17 ± 5.75 190 25 7.08 ± 4.33 13.55 ± 7.28 84 23 Rosenhek R. Journal of American Society of Echocardiography

5
Normal Values for Doppler Echocardiographic Assessment of Heart Valve Prostheses:
mitral valve position Carbomedics Bileaflet St Jude Medical Bleaflet 4.8 ± 2.5 8.8 ± 2.2 33 3.46 ± 1.03 8.79 ± 3.46 78 27 3.39 ± 0.97 8.78 ± 2.9 46 29 3.32 ± 0.87 8.87 ± 2.34 57 31 3.6 ± 0.6 10.3 ± 2.3 12 25 2 23 4.0 1 23 2.5 ± 1 4 25 5 ± 1.82 11 ± 4 16 27 4.46 ± 2.22 12 ± 6 41 31 4.15 ± 1.8 10 ± 3 40 29 Gradiente medio e di picco 6 ± 2 16 27 4.7 ± 2 22 29 6 ± 3 6 33 4.4 ± 2 31 Carpentier-Edwards Stented bioprosthesis Rosenhek R. Journal of American Society of Echocardiography

6
Disfunzione protesica
TIPO di PATOLOGIA 1. MISMATCH 7. ENDOCARDITE 2. TROMBOSI Disfunzione protesica 6. DISTACCO 3. EMBOLIA 5. EMOLISI 4. STRUCTURAL FAILURE

7
COME UTILIZZARE LE METODICHE
SCOPIA TTE ETE Sospetto malfunzionamento ULTERIORI INFORMAZIONI ELEVATA SENSIBILITA’ E SPECIFICITA’ DIAGNOSTICA protesi mitralica

8
PROTESI MITRALICA How to do it SCANNERIZZARE la PROTESI da 0 a 120°

9
How to do it VISUALIZZAZIONE MOVIMENTO DISCHI MISURAZIONE GRADIENTE VISUALIZZAZIONE TROMBI

10
RISCONTRO di GRADIENTE ELEVATO
in PROTESI AORTICA Pressure Recovery Disfunzione protesica Mismatch Fattori favorenti: - Anemia Febbre Tachicardia Alta portata Ostruzione sottovalvore residua

11
PROBLEMA SPECIFICO per PROTESI AORTICHE....
Gradiente elevato Sintomi da sforzo MISMATCH Modificazioni prognostiche? Mancata regressione ipertrofia

12
Patient Prosthesis Mismatch
Indexed effective orifice area at rest (cm2/m2) EOAI= EOA\BSA Blais C.; Circulation 2003
 EOAI= EOA\BSA. Blais C.; Circulation")
13
MISMATCH SCOPIA TT TE movimento gradiente . normale apertura dischi
normale elevato assenza di trombi The Am J Cardiol Jan 1. Vol 85

14
Impact of Valve Prosthesis-Patient Mismatch on Short-Term Mortality After Aortic Valve Replacement
Univariate analysis Multivariate analysis 7.2 ( ) 0.0003 5.5 ( ) 0.004 Severe PPM 3.9 ( ) 0.002 3.9 ( ) Cardioput bypass time > 120 minutes 4.5 ( ) 0.047 5.8 ( ) 0.005 Emergent/salvage operation Operative variables 3.7 ( ) 0.06 3.7 ( ) LV ejection fraction < 40% … 2.7 ( ) 0.02 Ventricular arhythmias 2.2 ( ) 0.03 Previous myocardial infarction Preoperative variables Risk Ratio (95% CI) P Risk Ratio (95% CI) Variable Predictors of Short-Term Mortality in Univariate and Multivariate analysys for the Subgroup of Patients with Moderate-Severe PPM (n=474) Blais C. Circulation 26, 2003.
 ( ) Severe PPM. 3.9 ( ) ( ) Cardioput bypass time > 120 minutes. 4.5 ( ) ( ) Emergent/salvage operation. Operative variables. 3.7 ( ) ( ) LV ejection fraction < 40% … 2.7 ( ) Ventricular arhythmias. 2.2 ( ) Previous myocardial infarction. Preoperative variables. Risk Ratio (95% CI) P. Risk Ratio (95% CI) Variable. Predictors of Short-Term Mortality in Univariate and Multivariate analysys for the Subgroup of Patients with Moderate-Severe PPM (n=474) Blais C. Circulation 26,")
15
Valve prosthesis-patient mismatch
Impact of Valve Prosthesis-Patient Mismatch on Short-Term Mortality After Aortic Valve Replacement LVEF < 40% LVEF ≥ 40% Mortality risk ratio Non significant Moderate Severe Valve prosthesis-patient mismatch Blais C. Circulation 26, 2003.

16
Prosthesis-Patient Mismatch Affects Survival After Aortic Valve Replacement
ID/BSA ≤ 10 mm/mq. 59 ±1% Overall Survival (%) 28 ± 5% P = 0.03 1721 54 1386 39 959 19 585 6 336 2 Years Rao V. Circulation Nov 7; 102 (19 Suppl 3)
 28 ± 5% P = Years. Rao V. Circulation Nov 7; 102 (19 Suppl 3)")
17
Prosthesis-patient mismatch after aortic valve replacement predominantly affects patients with preexisting left ventricular dysfunction: Effect on survival, freedom from heart failure, and left ventricular mass regression 30.3% (12.1%) Heart failure symptoms or death from heart failure by 3 years after aortic valve replacement 14.9% (3.2%) Cumulative incidence (%) 8.1% (4.6%) 8.2% (1.9%) Normal LV; No PPM Normal LV; PPM Impared LV; No PPM Impared LV; PPM “..Implantation of an aortic valve prosthesis with an estimated indexed EOA of 0.85 cmq/mq or less should be avoided in patients with a preoperative LVEF of less than 50%”. 0.009 0.9 0.2 P Value 1.5; 1.7 0.4; 2.9 0.7; 5.7 95% CI 5.1 1.1 1.9 Adjusted odd ratio Ruel M .. J Thorac Cardiovasc Surg. 2006; May 131: (5)
 Heart failure symptoms or death from heart failure by 3 years after aortic valve replacement. 14.9% (3.2%) Cumulative incidence (%) 8.1% (4.6%) 8.2% (1.9%) Normal LV; No PPM. Normal LV; PPM. Impared LV; No PPM. Impared LV; PPM. ..Implantation of an aortic valve prosthesis with an estimated indexed EOA of 0.85 cmq/mq or less should be avoided in patients with a preoperative LVEF of less than 50% P Value. 1.5; ; ; % CI Adjusted odd ratio. Ruel M .. J Thorac Cardiovasc Surg. 2006; May 131: (5)")
18
COME EVITARE il MISMATCH ?
1. BSA x 0.85 = EOA minima (effective orifice area) Normal Reference Value of effective Orifice Areas for the Prosthetic Valves Prosthetic Valve Size, mm
 Normal Reference Value of effective Orifice Areas for the Prosthetic Valves. Prosthetic Valve Size, mm.")
19
OSTRUZIONE SOTTOVALVOLARE
TE Ipertrofia SIV basale ASSE LUNGO Possibilità di accurata valutazione morfologica del SIV basale 4C PWD Gradiente a partenza sotto la protesi nell’LVOT

20
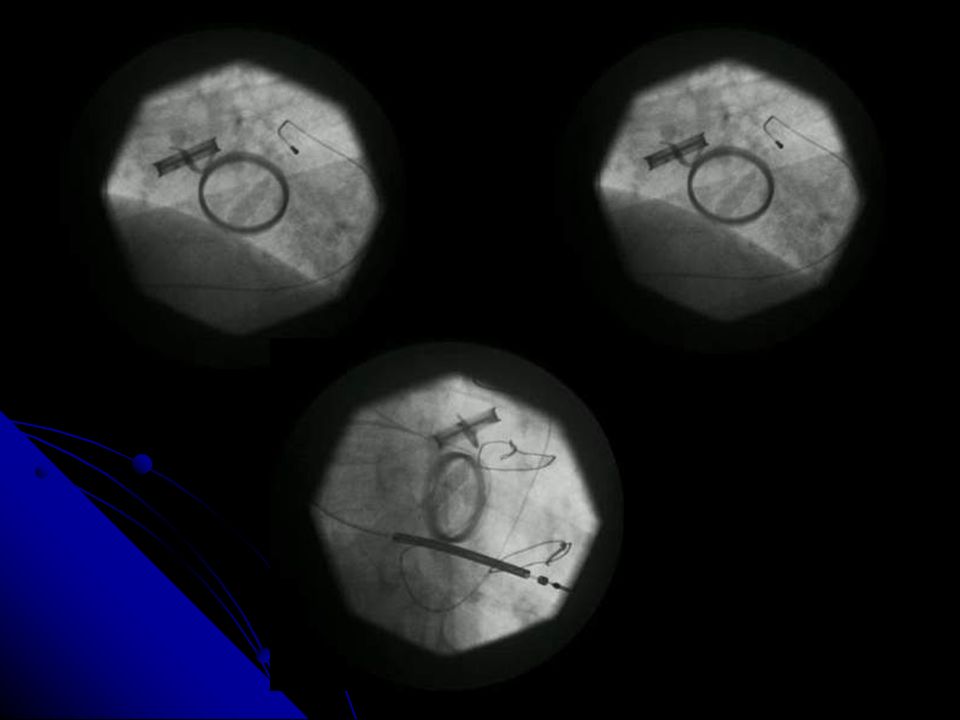
OSTRUZIONE PROTESICA (trombo / panno)
Incidenza: 0.1-5% pz/anno . Fattori di rischio: .. scoagulazione inadeguata ... trombofilia ... Velocità del flusso TT SCOPIA TE GRADIENTE RIDOTTA APERTURA PRESENZA di ELEVATO del/i DISCO/I TROMBO

21
PER la DIAGNOSI USARE: ECO + FLUOROSCOPIA SENS 87% SPEC 78% VP+ 80%
. < MOVIMENTO DISCO . > GRADIENTE . < AREA DI FLUSSO: PHT>220 . RIGURGITO INTRA-PROT . VISUALIZZAZIONE TROMBO (TE) SENS 87% SPEC 78% VP+ 80% SENS 75% SPEC 64% VP+ 57% GRADIENTE < ESCURSIONE dei DISCHI ACC/AHA Guidelines Circulation September 9
 SENS 87% SPEC 78% VP+ 80% SENS 75% SPEC 64% VP+ 57% GRADIENTE < ESCURSIONE dei DISCHI. ACC/AHA Guidelines Circulation September 9.")
22
Prosthetic Mitral Valve dysfunction? (n = 134)
IMPIEGO SEMPLIFICATO dell’ECO TT per VALUTARE il FUNZIONAMENTO di una PROTESI MITRALICA Prosthetic Mitral Valve dysfunction? (n = 134) E < 1.9 (n = 62) E ≥ 1.9 (n = 72) PHT < 130 (n= 58) PHT ≥ 130 (n = 3) PHT < 130 (n = 52) PHT ≥ 130 (n = 20) Any Dysf 5% Regurg 5% Obstr 0% Any Dysf 100% Regurg 0% Obstr 100% Any Dysf 71% Regurg 69% Obstr 2% Any Dysf 71% Regurg 5% Obstr 9% PZ con E < 2 e PHT < 130 HANNO 95% di PROBABILITA’ di avere una PROTESI NORMOFUNZIONANTE Am J Cardiol 2002; 89:704-10
 E < 1.9 (n = 62) E ≥ 1.9 (n = 72) PHT < 130 (n= 58) PHT ≥ 130 (n = 3) PHT < 130 (n = 52) PHT ≥ 130 (n = 20) Any Dysf 5% Regurg 5% Obstr 0% Any Dysf 100% Regurg 0% Obstr 100% Any Dysf 71% Regurg 69% Obstr 2% Any Dysf 71% Regurg 5% Obstr 9% PZ con E < 2 e PHT < 130. HANNO 95% di PROBABILITA’ di avere una PROTESI NORMOFUNZIONANTE. Am J Cardiol 2002; 89:")
23
ATTENZIONE al GRADIENTE !!!!
DOPPIO DISCO SINGOLO DISCO Il blocco di un solo disco in alcuni casi non comporta un aumento del gradiente 30% % HANNO un GRADIENTE NORMALE delle TROMBOSI

24
PROBABILITA’ DIAGNOSTICA TROMBO vs PANNO
GRADIENTE ELEVATO MASSA MOBILE INSERZIONE sul DISCO INR < 2.5 TEE evaluation of suspected thrombus on pannus related MPVD N = 5 Elevated gradients Mobile mass Attachment to occluder INR ≤2.5 N = 18 N = 16 Prevalence (%) N = 10 Predictors: 0-1 2 3-4 N = 4 Probability: Low Intermediate High Risk factor(s) Am Journ Cardiol. Vol 86. Nov
 N = 10. Predictors: N = 4. Probability: Low. Intermediate. High Risk factor(s) Am Journ Cardiol. Vol 86. Nov")
25
3. MORFOLOGIA / CARATTERISTICHE del TROMBO
. < 5 mm > 5 mm . NON OSTRUENTE OSTRUENTE NON MOBILE MOBILE EPARINA TROMBOLISI / CHIRURGIA CHIRURGIA v. diapositive successive

26
COMPLICANZE / MORTALITA’ e DIMENSIONI del TROMBO
Complication Death 46.7 28.6 % 20 6.25 3.1 3.6 Thrombus <0.8 cmq cmq ≥1.6 cmq Area No. of Patients JACC Vol. 43. No 1. January 7, 2004: 77-84

27
INDICAZIONI al TEE: DIAGNOSI nei CASI DUBBI D.D. fra TROMBO e PANNO
trombo -> trombolisi panno -> intervento chirurgico 3. MORFOLOGIA/CARATTERISTICHE del TROMBO grosso e mobile -> no trombolisi; si chirurgia 4. EFFICACIA della TROMBOLISI scomparsa/riduzione delle dimensioni

28
Cinefluoscopy – Transthoracic Echocardiography
ALGORITMO di IMPIEGO DIAGNOSTICO ECO TEE Patients with suspected PVT (n = 82) Cinefluoscopy – Transthoracic Echocardiography A CF+/TTE+ B CF+/TTE - C CF-/TTE+ D CF-/TTE- TEE not required if: - Bileaflet prosthesis in mitral position (aortic position?) TEE not required if: - Aortic prosthesis, smal size (21,23) no symptoms TEE required if: - Mitral prosthesis, atrial fibrillation, systemic embolism TEE Not required: - In all cases TEE required if: Symptoms not explained by other cardiac or extracardiac source mitral prosthesis? TEE required if: - Monocuspid valve (Lillehei-Kaster, Bicer prostheses) TEE not required: - All other cases Am J Cardiol. Vol 85. Jan 1, 2000
 Cinefluoscopy – Transthoracic Echocardiography. A. CF+/TTE+ B. CF+/TTE - C. CF-/TTE+ D. CF-/TTE- TEE not required if: - Bileaflet prosthesis in mitral position (aortic position ) TEE not required if: - Aortic prosthesis, smal size (21,23) no symptoms. TEE required if: - Mitral prosthesis, atrial fibrillation, systemic embolism. TEE. Not required: - In all cases. TEE required if: Symptoms not explained by other cardiac or extracardiac source. mitral prosthesis TEE required if: - Monocuspid valve (Lillehei-Kaster, Bicer prostheses) TEE not required: - All other cases. Am J Cardiol. Vol 85. Jan 1,")
29
2. DIAGNOSI DIFFERENZIALE: TROMBO vs PANNO
CRITERIO TROMBO PANNO Tempo dall’impianto anche < 6 mesi > 6 mesi Durata dei sintomi breve (< 1 mese) lunga Scoagulazione inadeguata (2/3) adeguata Anomalo movimento disco frequente (up to 100%) raro (up to 60%) Morfologia massa larga, estesa in AS non estesa in AS omogenea disomogenea (calcif) soft ecoriflettente Movimento mobile/immobile solo immobile Localizzazione cerniera/disco anello
 lunga. Scoagulazione inadeguata (2/3) adeguata. Anomalo movimento disco frequente (up to 100%) + raro (up to 60%) Morfologia massa larga, estesa in AS non estesa in AS. omogenea disomogenea (calcif) soft + ecoriflettente. Movimento mobile/immobile solo immobile. Localizzazione cerniera/disco anello.")
30
ALGORITMO DECISIONALE
ECO TT + SCOPIA ECO TE Gradiente medio > 8 mm Hg Ridotto movimento / blocco disco/i Rigurgito intraprotesico DD trombo / panno Caratteristiche del trombo ALTO RISCHIO se: trombo > 0.8 cmq > 1.6 cmq estensione extraprot. CHIRURGIA TROMBOLISI 1. TROMBO MOBILE PZ ad ALTO RISCHIO CHIRURGICO 2. BLOCCO di 1 DISCO DISCHI IPOMOBILI indip dalla durata > 21 gg e dalla classe NYHA 3. PANNO BLOCCO di DISCO < 21 gg 4. BRIDGE alla CHIRURGIA

31
Thrombosis of Prosthetic Heart Valves
Class I Transtoracici and Doppler Echocardiography is indicated in patients with suspected prosthetic valve thrombosis to asses hemodynamic severity. (Level of Evidence: B) Class I Transesophageal echocardiography and/or fluoroscopy is indicated in patietns with suspected valve thrombosis to asses valve motion and clot burden. (Level of Evidence: B) ACC/AHA Guidelines JACC Vol 48 N 6.
 Class I. Transesophageal echocardiography and/or fluoroscopy is indicated in patietns with suspected valve thrombosis to asses valve motion and clot burden. (Level of Evidence: B) ACC/AHA Guidelines JACC Vol 48 N 6.")
37
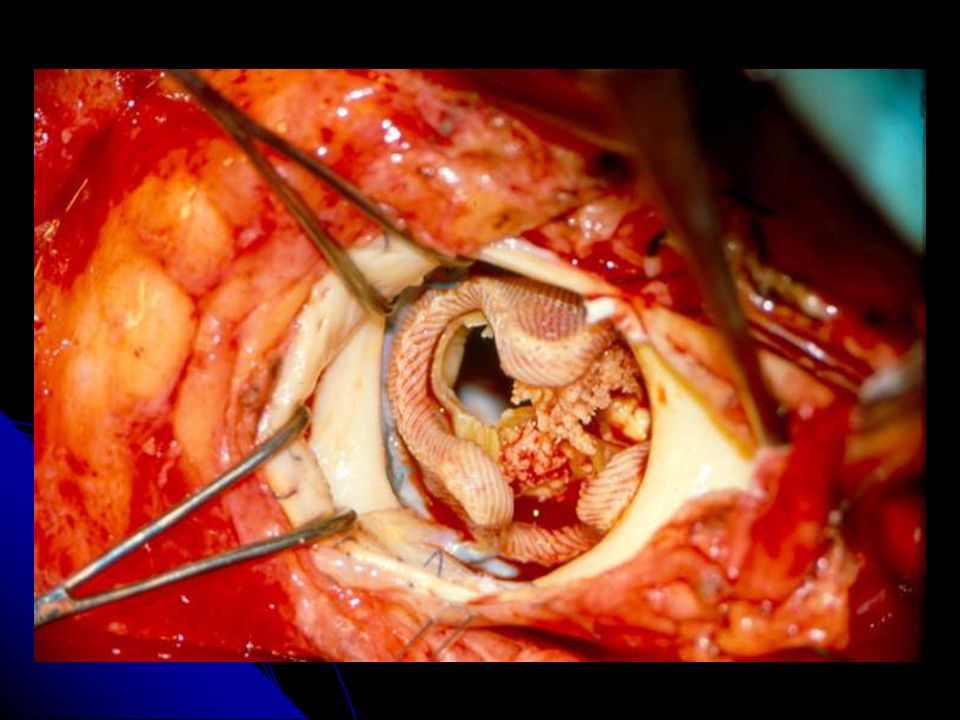
Panno

40
3. EMBOLIE PREVALENZA 1% pz/anno FATTORI di RISCHIO: Protesi mitralica
Protesi multiple Età > 70 anni Fibrillazione atriale Disfunzione ventricolare sx

41
EMBOLIA ENDOCARDITE PROTESI TROMBOSI PROTESI INDICAZIONE a ECO TE
AURICOLARE CAUSE SCONOSCIUTE MALATTIA CAROTIDEA ATEROMA AORTA

42
Detection of Prosthetic Valve Strands by Transesophageal Echocardiography: Clinical Significance in Patients With Suspected Cardiac Source of Embolism Prevalence of Strands by Valve Type and Location Each Indication Indication for Study NS 1/19 (5%) 1/5 (20%) Aortic bioprosthetic (n=24) 0.001 4/65 (6%) 9/29 (31%) Aortic mechanical (n=94) 2/32 (6%) 1/3 (33%) Mitral bioprosthetic (n=35) 0.0001 15/60 (25%) 23/35 (66%) Mitral mechanical (n=95) 0.07 3/51 (6%) 2/8 (25%) All bioprosthetic (n=59) 19/125 (15%) 32/64 (50%) All mechanical (n=189) P Value PVD/Misc CSE Valve Type Orsinelli D. JACC. Dicember Vol 26. N 7:
 1/5 (20%) Aortic bioprosthetic (n=24) /65 (6%) 9/29 (31%) Aortic mechanical (n=94) 2/32 (6%) 1/3 (33%) Mitral bioprosthetic (n=35) /60 (25%) 23/35 (66%) Mitral mechanical (n=95) /51 (6%) 2/8 (25%) All bioprosthetic (n=59) 19/125 (15%) 32/64 (50%) All mechanical (n=189) P Value. PVD/Misc. CSE. Valve Type. Orsinelli D. JACC. Dicember Vol 26. N 7:")
43
Transesophageal Echocardiographic Findings in Patients With Nonobstructed Prosthetic Valves and Suspected Cardiac Source of Embolism 27 (52%) No abnormality 12 (23%) Spontaneous echo contrast 1 (2%) Protrunding nonmobile aortic atheroma 5 (10%) Suspected thrombus/strands Periaortic graft thrombus 6 (12%) Prosthetic valve thrombus Patients (n=52) TEE Findings MODIFICAZIONI TERAPEUTICHE in circa il 20% dei CASI Shiran A. Am J Cardiol Dicember 15. Vol 86
 No abnormality. 12 (23%) Spontaneous echo contrast. 1 (2%) Protrunding nonmobile aortic atheroma. 5 (10%) Suspected thrombus/strands. Periaortic graft thrombus. 6 (12%) Prosthetic valve thrombus. Patients (n=52) TEE Findings. MODIFICAZIONI TERAPEUTICHE. in circa il 20% dei CASI. Shiran A. Am J Cardiol Dicember 15. Vol 86.")
45
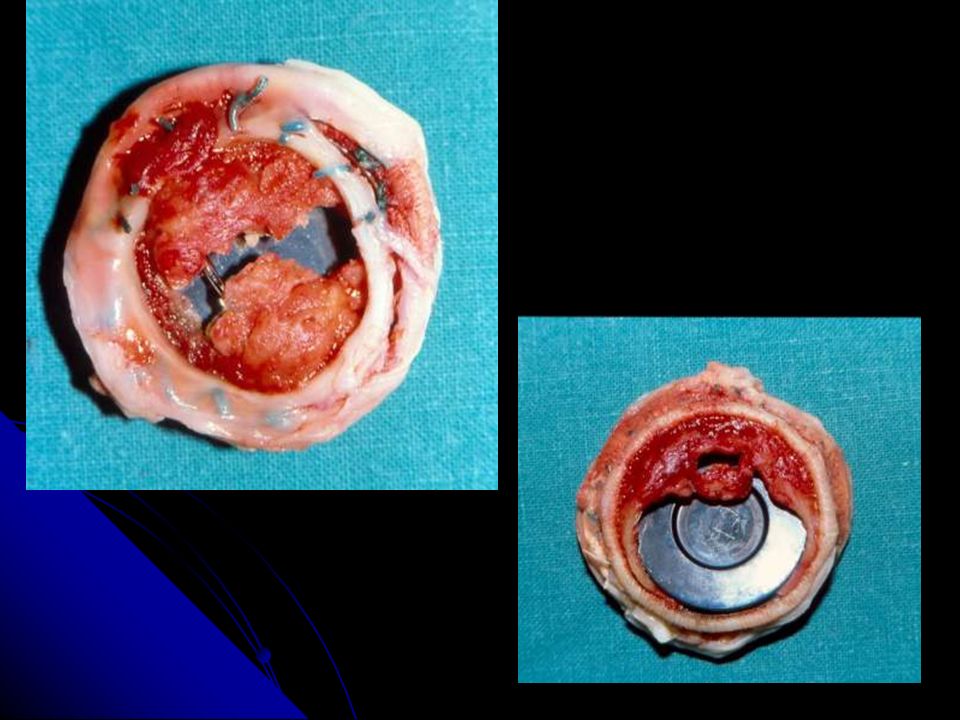
4. DEGENERAZIONE BIOPROTESI
Circa 30% a anni + frequente in: Giovani (< 40 anni) Posizione mitralica Insorgenza graduale dei sintomi 10 ≥70 15 60-69 21 50-59 30 40-49 42 < 40 Percent with Valve Failure After 10 years Patient’s Age (YR) Heterograft valve failure 10 years after valve replacement according to the pateitn’s age at the time of implantation
 Posizione mitralica. Insorgenza graduale dei sintomi. 10. ≥ < 40. Percent with Valve Failure After 10 years. Patient’s Age (YR) Heterograft valve failure 10 years after valve replacement according to the pateitn’s age at the time of implantation.")
46
ECO INSUFFICIENZA da: lesione o rottura di una o + cuspidi
STENOSI INSUFFICIENZA da: lesione o rottura di una o + cuspidi secondaria alla calcificazione

49
6. DISTACCO NON SETTICHE Errori nell’impianto
Degenerazione/calcificazione anulus SETTICHE endocardite CAUSE:

50
OBIETTIVI SEDE ESTENSIONE ENTITA’

51
SEDE-ESTENSIONE 1 = antero-mediale 4 = anteriore-medio
3 5 1 2 3 4 2 6 4 1 = antero-mediale 4 = anteriore-medio 5 = antero-laterale 3 = postero-mediale 6 = posteriore-medio 2 = postero-laterale 3 1 6 4 2 5

52
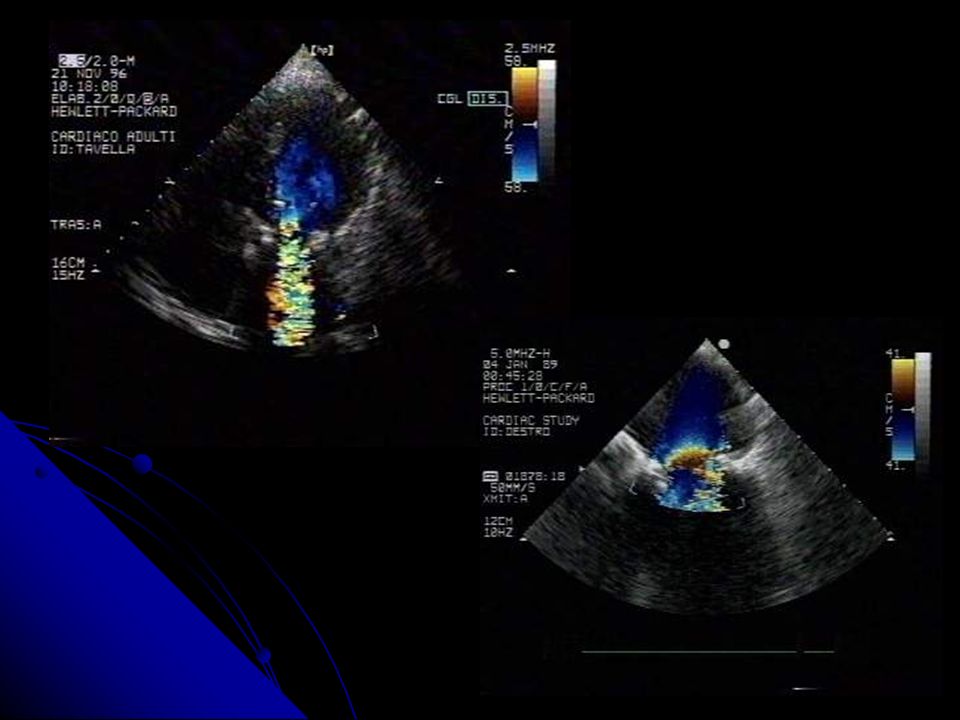
ENTITA’ 1. JET area LIEVE = < 3 cmq MODERATO = 3-6 cmq
SEVERO = > 6 cmq 2. PISA LIEVE = < 0.5 cm MODERATO = cm SEVERO = > 1 cm 3. VOLUME di RIGURGITO LIEVE = < 40 ml MODERATO = ml SEVERO = > 60 ml 4. ERO LIEVE = < 20 mm2 MODERATO = mm2 SEVERO = > 40 mm2 4. FLUSSO VENOSO POLM LIEVE = S = D MODERATO = DOMINANZA DIASTOLICA SEVERO = FLUSSO SISTOLICO INVERTITO ENTITA’

53
DECISION MAKING ASSENZA di SCOMPENSO - SCOMPENSO
ASSENZA di EMOLISI EMOLISI IMPORTANTE LEAK PICCOLO LEAK ESTESO -RIGURGITO LIEVE RIGURGITO SEVERO OSSERVAZIONE INTERVENTO

55
7. ENDOCARDITE DATI: In RIDUZIONE (oggi intorno all’1% entro il 1° anno) MORTALITA’ ANCORA ELEVATA (25-65%) ESTENSIONE LOCALE del PROCESSO 3. COLPISCE prevalentemente l’ANELLO e le STRUTTURE PERIANULARI Ann Thorac Surg 2000; 69:

56
ENDOCARDITE HOSPITAL COMMUNITY ACQUIRED ACQUIRED
(< 60 gg) (> 1 anno) RECRUDESCENZA CAUSE REINFEZIONE INFEZIONE PERI-OP BATTERIEMIA (sala op, via centrale, cute etc..) Staf coag AGENTE = a E. NATIVA Funghi maggior % di Staf aureus patogeni Stp epid inusuali PEGGIORE PROGNOSI MIGLIORE
 (> 1 anno) RECRUDESCENZA CAUSE -REINFEZIONE. INFEZIONE PERI-OP -BATTERIEMIA. (sala op, via centrale, cute etc..) Staf coag - AGENTE = a E. NATIVA. Funghi maggior % di. Staf aureus patogeni. Stp epid inusuali. PEGGIORE PROGNOSI -MIGLIORE.")
57
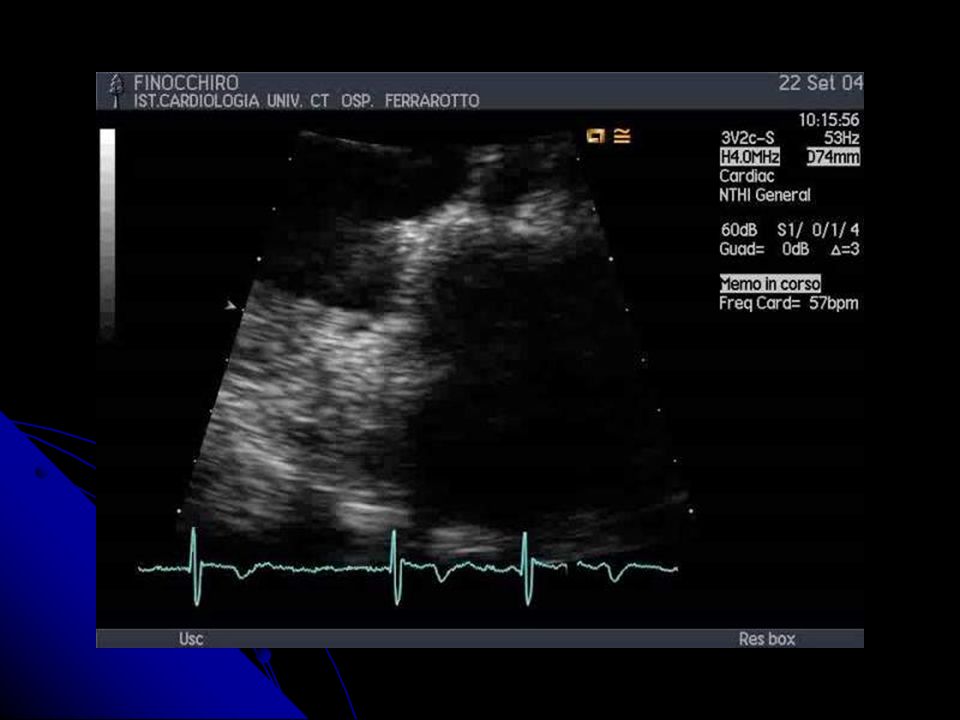
PECULIARITA’ FREQUENTE COINVOLGIMENTO dell’ANELLO e delle STRUTTURE PERIANULARI 2. FLOW MASKING PROTESI Sensitivity of TEE versus TTE in the diagnosis of prosthetic valve endocarditis 44 86 Zabalgoitia et al. (1993) (bioprothesis) 36 82 33 Daniel et al. (1993) 17 100 6 Alton et al. (1992) 83 12 Taams et al. (1990) TTE sensitivity (%) TEE sensitivity (%) No. Of patients TE in AGGIUNTA al TT in OGNI CASO
 (bioprothesis) Daniel et al. (1993) Alton et al. (1992) Taams et al. (1990) TTE sensitivity (%) TEE sensitivity (%) No. Of patients. TE in AGGIUNTA al TT in OGNI CASO.")
58
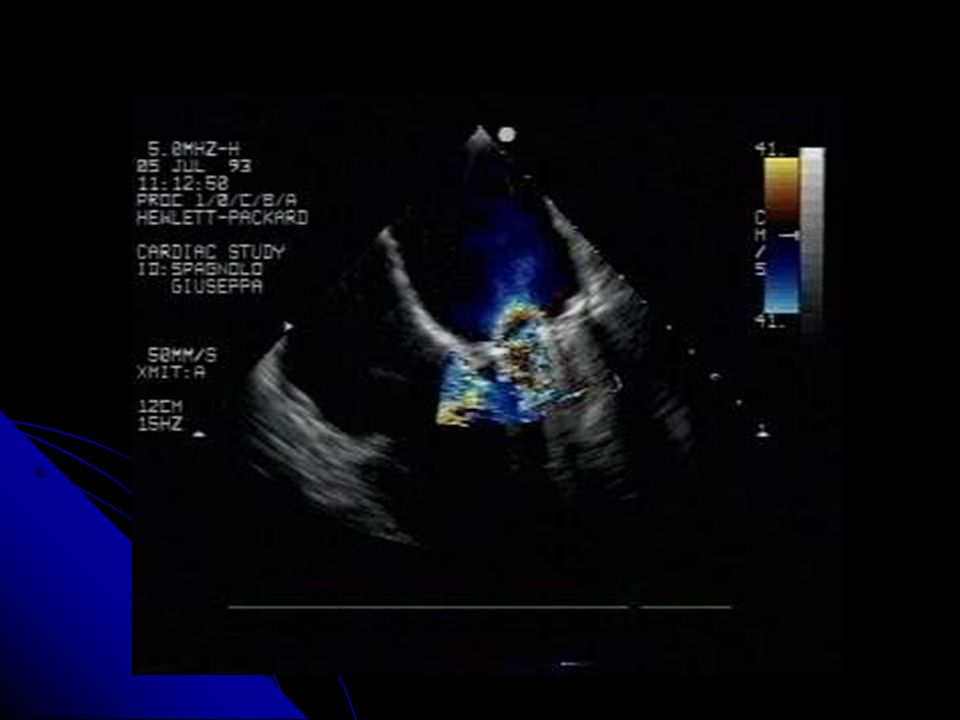
TEE VEGETAZIONI COMPLICANZE ENTITA’ PERI-ANULARI DISTACCO
ASCESSO PSEUDOANEURISMA FISTOLA

59
ASCESSO FISTOLA DIAGNOSI TEE PSEUDOANEURISMA Comunicazione
con flusso tra aorta e cavità cardiaca Cavità ben delineata Ridotta ecodensità Non comunicante Assenza di flusso DIAGNOSI TEE Idem ma comunicante Presenza di flusso PSEUDOANEURISMA

60
FISTOLE AS CS Visualizzazione NC CD - Soluzione di continuo (2D) +
AD VD Visualizzazione - Soluzione di continuo (2D) + - Jet turbolento (color) NC CD AD VD
 + - Jet turbolento (color) NC CD. AD VD.")
61
ESTENSIONE PERIANULARE ?
COSA COMPORTA la ESTENSIONE PERIANULARE ? MAGGIORE INCIDENZA di CHF MAGGIORE MORTALITA’ in TM fino al 30-40% 3. PIU’ FREQUENTE RICORSO alla CHIRURGIA rr 3.2 INTERVENTO PIU’ COMPLESSO e di MAGGIORE DURATA 5. MAGGIORE MORBILITA’ e MORTALITA’ PERI-OP

62
grazie

Presentazioni simili