Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Farmaci biologici nel trattamento dell’artrite reumatoide
Carlomaurizio Montecucco PAVIA Alma Ticinensis Universitas LaRIT

2
Il fattore tempo è cruciale nel trattamento dell’AR
Il trattamento va iniziato il più rapidamente possibile Il trattamento inefficace va modificato il più rapidamente possibile La risposta al trattamento (remissione) va ottenuta il più rapidamente possibile
 va ottenuta il più rapidamente possibile.")
5
Qualità di vita dei pazienti con artrite reumatoide che devono iniziare terapia con farmaci biologici Han C et al Arthritis Res Ther 2007

6
Effetto dell’AR sulla mortalità
Donne Statunitensi Uomini Statunitensi Donne di Stanford con AR Uomini di Stanford con AR 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Probabilità di sopravvivenza N = 886 RMS* = 3.08 Anni dall’inizio dello studio *Rapporto di mortalità standardizzato = 2.24 Wolfe F et al, Arthritis Rheum 37:481–494, 1994

7
A set of 10 recommendations to improve the management of RA in clinical practice, based on evidence from the literature and on expert opinion. Ann Rheum Dis 2010

8
Algorithm to treat RA to Target
Active RA Main target Alternative target Remission Sustained Remission Low disease activity Sustained low disease activity Adapt therapy according to disease activity if state is lost Use a composite measure of disease activity every 1-3 months Assess disease activity about every 3-6 months If state is lost

9
P-EAC: treatment protocol
Pavia early arthritis clinic P-EAC: treatment protocol UPA RA (ACR/EULAR) HCQ 200mg/day MTX mg/w DAS-guided therapy Change if DAS > 2.4 Tight control Evaluation every 2 months for 6 months then every 3 months thereafter MTX 20 mg/w MTX 25 mg/w
 HCQ 200mg/day. MTX mg/w. DAS-guided therapy. Change if DAS > 2.4. Tight control. Evaluation every 2 months for 6. months then every 3 months thereafter. MTX 20 mg/w. MTX 25 mg/w.")
10
P-EAC: treatment protocol
Pavia early arthritis clinic P-EAC: treatment protocol UPA RA (ACR/EULAR) HCQ 200mg/day MTX mg/w DAS-guided therapy Change if DAS > 2.4 Tight control Evaluation every 2 months for 6 months then every 3 months thereafter MTX 20 mg/w MTX 25 mg/w MTX +biologic agent
 HCQ 200mg/day. MTX mg/w. DAS-guided therapy. Change if DAS > 2.4. Tight control. Evaluation every 2 months for 6. months then every 3 months thereafter. MTX 20 mg/w. MTX 25 mg/w. MTX +biologic agent.")
11
Pavia early arthritis clinic
46% 34% DAS 20% 20% 80% Data on file

12
Cosa sono i farmaci biologici ?
Farmaci biologici = farmaci biotecnologici Grandi molecole (proteine) Prodotti con procedure biotecnologiche Elevati costi di produzione Altamente selettivi verso un preciso e stabilito bersaglio terapeutico
 Prodotti con procedure biotecnologiche. Elevati costi di produzione. Altamente selettivi verso un preciso e stabilito bersaglio terapeutico.")
13
TARGETED THERAPIES

14
Quali bersagli terapeutici nell’AR ?
Anti-CD20 Anti-TNFα abatacept IL1-RA Tocilizumab denosumab Choy EHS. NEJM 2001;344:907-12 Choy EHS. NEJM 2001

15
Come agiscono i farmaci biotecnologici
Come agiscono i farmaci biotecnologici ? 1) Inibizione delle citochine infiammatorie Interazione normale CK infiammatoria Antagonista recettoriale recettore Segnale di attivazione della infiammazione Neutralizzazione della CK Anticorpo monoclonale Recettore solubile Nessun segnale Adapted with permission from Choy EHS, Panayi GS. N Engl J Med. 2001;344:907–916. Copyright © 2001 Massachusetts Medical Society. All rights reserved.
 Inibizione delle citochine infiammatorie. Interazione normale. CK infiammatoria. Antagonista. recettoriale. recettore. Segnale di attivazione della infiammazione. Neutralizzazione della CK. Anticorpo monoclonale. Recettore solubile. Nessun segnale. Adapted with permission from Choy EHS, Panayi GS. N Engl J Med. 2001;344:907–916. Copyright © 2001 Massachusetts Medical Society. All rights reserved.")
16
Come agiscono I farmaci biotecnologici
Come agiscono I farmaci biotecnologici ? 2) Inibizione dell’interazione tra cellule antigene MHC II TCR attivazione proliferazione T-Linfocito Recettore solubile modified from Kremer JM, et al. J Clin Rheumatol 2005.
 Inibizione dell’interazione tra cellule. antigene. MHC II. TCR. attivazione. proliferazione. T-Linfocito. Recettore solubile. modified from Kremer JM, et al. J Clin Rheumatol")
17
Come agiscono I farmaci bioptecnologici
Come agiscono I farmaci bioptecnologici ? 3) distruzione mirata delle cellule attivazione del complemento e lisi della membrana cellulare anticorpo monoclonale CD 20 B-linfocito membrana cellulare attivazione di segnali di “autodistruzione”
 distruzione mirata delle cellule. attivazione del complemento e lisi della membrana cellulare. anticorpo. monoclonale. CD 20. B-linfocito. membrana cellulare. attivazione di segnali. di autodistruzione")
18
Quali sono i farmaci biotecnologici per l’AR oggi disponibili ?
TNF alpha inhibition (MoAbs) Infliximab IV Adalimumab SC certolizumab pegol SC Golimumab SC TNF alpha inhibition (soluble receptor) Etanercept SC IL1 inhibition (receptor antagonist) anakinra SC IL6 receptor inhibition (MoAb) Tocilizumab IV CTLA4-Ig (soluble receptor) Abatacept IV Anti-CD20 (MoAb) Rituximab IV FIRST LINE BIOLOGIC AGENTS 2nd LINE
 Infliximab IV. Adalimumab SC. certolizumab pegol SC. Golimumab SC. TNF alpha inhibition (soluble receptor) Etanercept SC. IL1 inhibition (receptor antagonist) anakinra SC. IL6 receptor inhibition (MoAb) Tocilizumab IV. CTLA4-Ig (soluble receptor) Abatacept IV. Anti-CD20 (MoAb) Rituximab IV. FIRST LINE BIOLOGIC AGENTS. 2nd LINE.")
19
Da quanto tempo sono disponibili i farmaci biotecnologici per l’AR?
Certolizumab 2010 Etanercept 2000 Rituximab TNF failure 2006 Adalimumab 2003 Golimumab 2009 Infliximab 2000 Abatacept TNF failure 2007 Tocilizumab 2009 #### PLEASE DO NOT DELETE CONTENT BELOW THIS LINE ! #### ########### Presentation 'CBV-SEM3756-MACT-RA005_Golimumab LT data and labelchanges_ r01_January ptt' created on Friday, 14 January, 2011 ########### Author: FRTA Purpose: MA Training Slides (Introduction & Continuous) QA: N/A Review By: N/A Review Type: Scientific Slide: 6/ Golimumab-Specific Deck: Yes Adapted from European Medicines Agency website )(EPARs ( 19
 QA: N/A Review By: N/A. Review Type: Scientific Slide: 6/48 Golimumab-Specific Deck: Yes. Adapted from European Medicines Agency website )(EPARs. ( curl=pages/medicines/landing/epar_search.jsp&murl=menus/medicines/medicines.jsp&mid=WC0b01ac058001d125) 19.")
21
Quanto sono efficaci ? EFFICACIA CLINICA
Sono efficaci quanto il MTX in pazienti non trattati (1) Sono efficaci nei pazienti non responsivi al MTX L’efficacia è maggiore se associati al MTX o ad altro DMARD 1 Tocilizumab è risultato maggiormente efficace del MTX in uno studio
 Sono efficaci nei pazienti non responsivi al MTX. L’efficacia è maggiore se associati al MTX o ad altro DMARD. 1 Tocilizumab è risultato maggiormente efficace del MTX in uno studio.")
22
Quanto sono efficaci ? Efficacia clinica Efficacia radiologica

23
Quando vanno impiegati nell’AR ?
FAILURE OF MTX

24
In case of failure of MTX (or other DMARDs), the following scenarios should represent indications for the use of TNF antagonists: High disease activity for at least one month, as defined by the 28- joint count disease activity score (DAS28) >5.1 (Ia, A). Moderate disease activity (DAS 28 >3.2 and ≤5.1) in the presence of unfavourable prognostic factors: • a positive test for ACPA or RF; elevated ESR or CRP (Ib, B); • clinical markers: persistence of at least 1 swollen joint (Ib, B); • early occurrence of bone erosions on x-rays (III, C); detection of active synovitis with power Doppler signal (III, C). 3. New erosions regardless of disease activity (III, C).
 >5.1 (Ia, A). Moderate disease activity (DAS 28 >3.2 and ≤5.1) in the presence of unfavourable prognostic factors: • a positive test for ACPA or RF; elevated ESR or CRP (Ib, B); • clinical markers: persistence of at least 1 swollen joint (Ib, B); • early occurrence of bone erosions on x-rays (III, C); detection of active synovitis with power Doppler signal (III, C). 3. New erosions regardless of disease activity (III, C).")
25
The Lombardy Rheumatology Network
Caporali R et al. Autoimm Rev 2008 TNF alpha inhibitor

26
… e se la risposta è insufficiente ?
First failure: In patients with inefficacy or adverse events to the first anti-TNF agent, either a treatment with a second TNF antagonists or with biologics with a different mechanism of action is recommended (1a,A)
")
27
Switching to a second TNF blocker
EULAR Response Autoimmun Rev. 2010

28
Switching to Rituximab
A- patients previously treated with tumor necrosis factor (TNF) inhibitors (n 155) B- patients who had never taken TNF inhibitors (n 99) Keystone E, et al. A&R 2007
 inhibitors (n 155) B- patients who had never taken TNF inhibitors (n 99) Keystone E, et al. A&R")
29
The Lombardy Rheumatology Network
Caporali R et al. Autoimm Rev 2008 TNF alpha inhibitor

30
Sono farmaci sicuri ? Post Marketing Warnings Infection risks TB
Congestive heart failure Cytopenia Demyelinating disease Malignancies (lymphoma)
")
31
INFEZIONI GRAVI NELLO STUDIO LORHEN
Favalli EG et al. Autoimm Rev 2009

32
DMARDS e infezioni nella AR
Increased risk in RA vs non-RA (RR 1.33) Doran MF et al Arthritis Rheum 2002 Factors associated with higher risk Age Extraarticular disease Rheumatoid factor ESR Cyclophosphamide Corticosteroids MTX not associated with a significant risk Caporali R et al Autoimm Rev 2008
 Doran MF et al Arthritis Rheum Factors associated with higher risk. Age. Extraarticular disease. Rheumatoid factor. ESR. Cyclophosphamide. Corticosteroids. MTX not associated with a significant risk. Caporali R et al Autoimm Rev")
33
Riattivazione della TBC in studi italiani
MONITORNET cases / 8787 p-y LORHEN 5 cases / 2069 p-y

34
Neoplasie nell’AR Symmons D PM, Silman AJ. Arthritis Rheum2004

35
Cancer type Observed Expected SIR (95% CI) Lymphomas^ 4 0.80 4.98 ( ) Hematologic* 5 1.23 4.07 ( ) Solid** 13 15.33 0.85 ( ) Overall 18 16.56 1.09 ( ) a) SIRs of cancer in RA patients treated with TNF blockers in comparison with general population living in Milan (a) and Varese (b). Cancer type Observed Expected SIR (95% CI) Lymphomas^ 4 0.67 5.99 ( ) Hematologic* 5 1.23 4.08 ( ) Solid** 13 17.99 0.72 ( ) Overall 18 19.22 0.94 ( ) b)
 Solid** ( ) Overall ( ) a) SIRs of cancer in RA patients treated with TNF blockers in comparison with general population living in Milan (a) and Varese (b). Cancer type. Observed. Expected. SIR (95% CI) Lymphomas^ ( ) Hematologic* ( ) Solid** ( ) Overall ( ) b)")
36
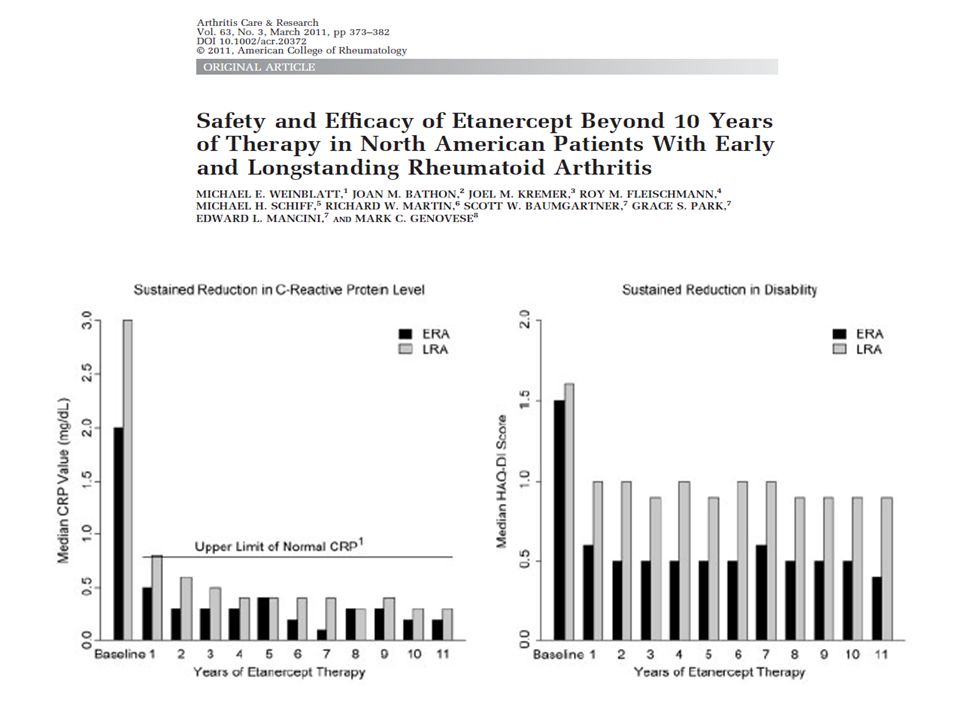
In conclusione ? Si tratta di farmaci efficaci ma non miracolosi, costosi e non privi di effetti collaterali, in particolare di natura infettiva Il loro impiego va valutato attentamente seguendo linee guida codificate a livello nazionale ed internazionale Queste riguardano sia la tipologia dei casi da trattare che raccomandazioni in merito a controindicazioni ed eventi avversi Nei casi in cui vanno somministrati, l’impiego non va procrastinato, pena una progressione della malattia e della conseguente invalidità permanente I pazienti vanno seguiti e monitorati per quanto concerne la risposta al trattamento e la possibile insorgenza di eventi avversi I timori legati all’impiego prolungato di questi farmaci sembrano fugati, almeno per gli anti-TNFalfa che sono in commercio da oltre 12 anni

Presentazioni simili

















>")

>")
