Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Antiaggregazione nel diabetico: Credenze ed evidenze
Antonio Nicolucci Department of Clinical Pharmacology and Epidemiology Consorzio Mario Negri Sud S. Maria Imbaro (CH) Italy
 Italy.")
2
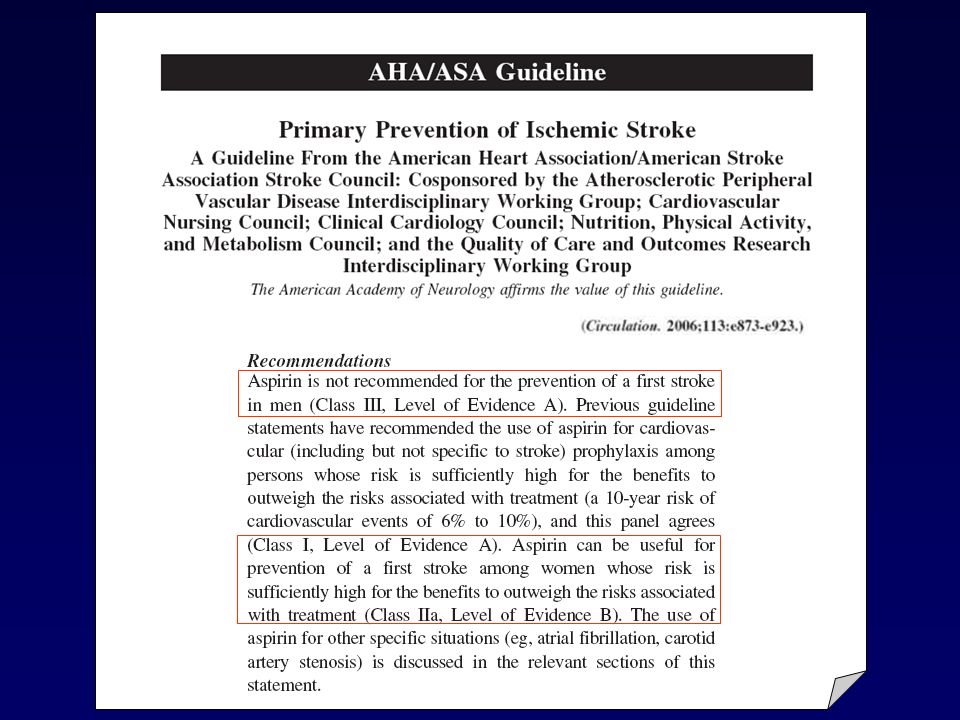
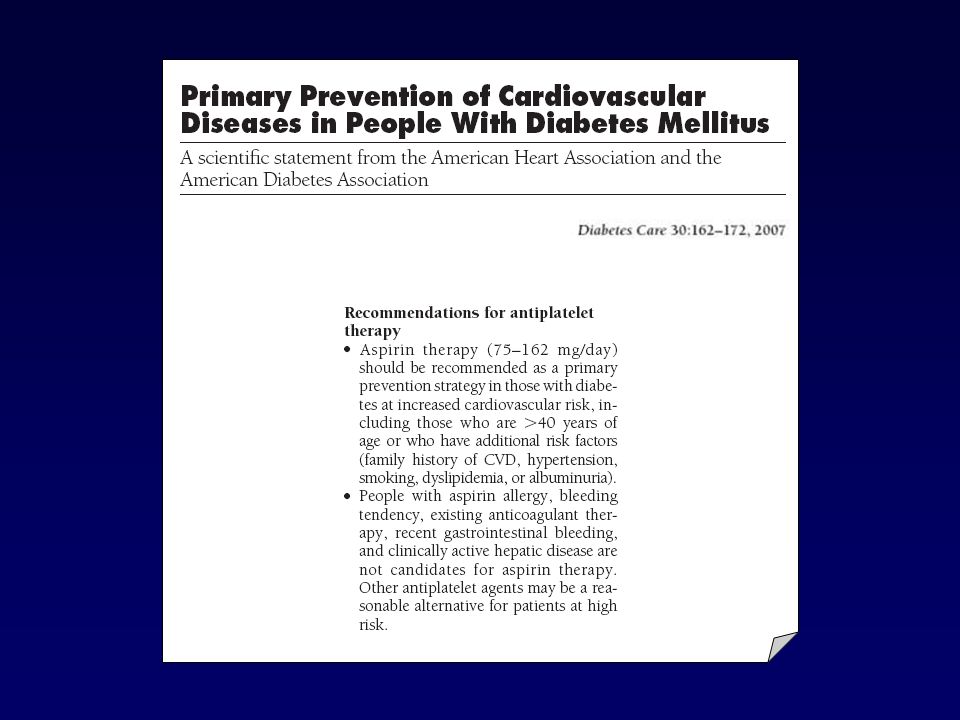
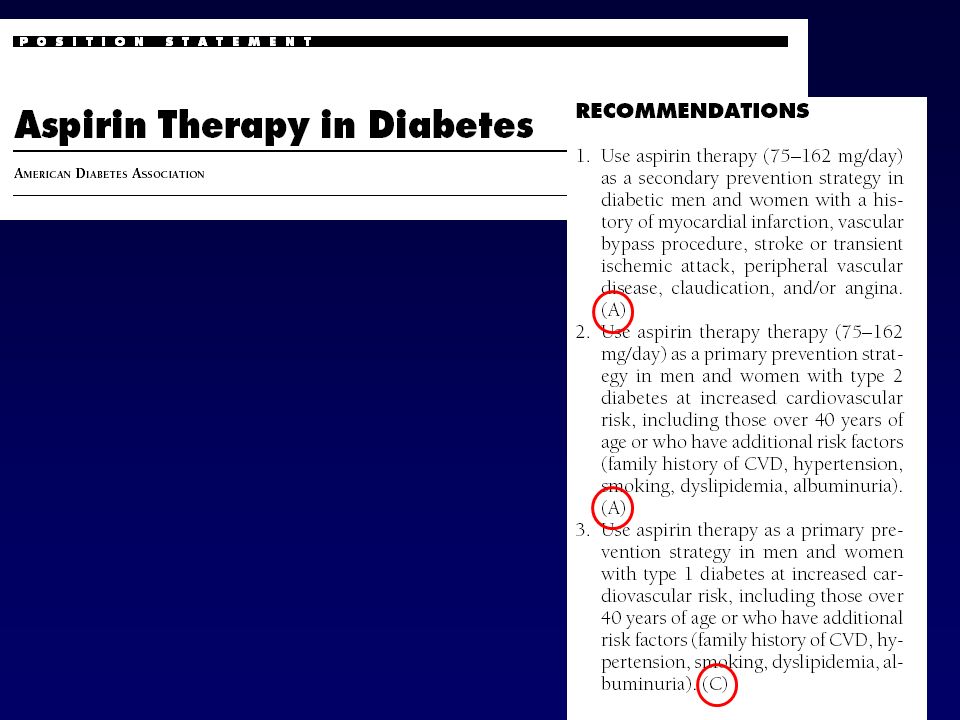
L’aspirina è efficace nei pazienti ad alto rischio cardiovascolare
I pazienti con DM presentano un alto rischio cardiovascolare L’aspirina è efficace nei pazienti con DM

7
EVIDENCE BASED MEDICINE EMINENCE BASED MEDICINE?
o EMINENCE BASED MEDICINE?

8
Studio attivato agli inizi degli anni ‘80
Pazienti con diabete: 2,4% Number of myocardial infarctions Aspirin Group Placebo group 11/275 (4.0%) /258 (10.1%) p=0.22 N Engl J Med 1989
 26/258 (10.1%) p=0.22. N Engl J Med")
9
Dato presente solo nella discussione dell’articolo!
Studio condotto fra il 1980 e il 1985 3711 pazienti con diabete, di cui quasi la metà con storia pregressa di CVD CV death, MI, RR=0.90 ( ) Stroke Fatal and non-fatal MI RR=0.82 ( ) JAMA 1992 Dato presente solo nella discussione dell’articolo!
 Stroke. Fatal and non-fatal MI RR=0.82 ( ) JAMA Dato presente solo nella discussione dell’articolo!")
10
I risultati non si riferiscono ai pazienti con diabete
Pazienti con diabete: 8% (previous MI? Previous stroke?) “The relative benefit of ASA on major cardiovascular events and all myocardial infarction was about the same in the group of patients with diabetes mellitus as in the whole HOT population”. Lancet. 1998;351(9118): I risultati non si riferiscono ai pazienti con diabete
 The relative benefit of ASA on major cardiovascular events and all myocardial infarction was about the same in the group of patients with diabetes mellitus as in the whole HOT population . Lancet. 1998;351(9118): I risultati non si riferiscono ai pazienti con diabete.")
12
LO STUDIO PPP Probability 1.00 0.99 0.98 0.97 0.96 0.95 0.94 0.93 0.92
Main end point (cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke) according to aspirin and diabetes status 1.00 0.99 0.98 0.97 0.96 Probability 0.95 0.94 0.93 Aspirin No Diabetes No Aspirin No Diabetes 0.92 Aspirin Diabetes Log-Rank Test No Diabetes c2=4.98 p-value=0.03 0.91 No Aspirin Diabetes Log-Rank Test Diabetes c2=0.13 p-value=0.71 0.90 1 2 3 4 5 Time Diabetes Care 2003; 26:
 according to aspirin and diabetes status Probability Aspirin No Diabetes. No Aspirin No Diabetes Aspirin Diabetes. Log-Rank Test No Diabetes c2=4.98 p-value= No Aspirin Diabetes. Log-Rank Test Diabetes c2=0.13 p-value= Time. Diabetes Care 2003; 26:")
13
LO STUDIO PPP Diabetes yes ( ) Diabetes no ( ) RR (95%CI) ASA Ctr . .
0.59 ( ) Main combined end-point 20 (3.9%) 22 (4.3%) 30 (1.6%) 51 (2.7%) 0.90 ( ) 0.69 ( ) Total CV events 53 (10.2%) 59 (11.5%) 98 (5.3%) 142 (7.5%) 0.89 ( ) 0.70 ( ) All deaths 25 (4.8%) 20 (3.9%) 42 (2.3%) 61 (3.2%) 1.23 ( ) 0.32 ( ) Cardiovascular 10 (1.9%) 8 (1.6%) 8 (0.4%) 25 (1.3%) 1.23 ( ) 0.97 ( ) Non-cardiovascular 15 (2.9%) 12 (2.3%) 34 (1.9%) 36 (1.9%) 1.23 ( ) 0.69 ( ) All myocardial infarction 5 (1.0%) 10 (2.0%) 15 (0.8%) 22 (1.2%) 0.49 ( ) 0.59 ( ) All stroke 9 (1.7%) 10 (2.0%) 11 (0.6%) 19 (0.1%) 0.89 ( ) 0.85 ( ) Angina pectoris 13 (3.1%) 16 (3.9%) 42 (2.7%) 51 (3.1%) 0.80 ( ) 0.71 ( ) TIA 7 (1.7%) 10 (2.4%) 22 (1.4%) 32 (2.0%) 0.69 ( ) 0.38 ( ) Peripheral artery disease 11 (2.6%) 13 (3.2%) 6 (0.4%) 16 (1.0%) 0.83 ( ) 0.70 ( ) Revasculatisation proced . . 8 (1.9%) 10 (2.4%) 15 (1.0%) 22 (1.4%) 0.79 ( ) 0.10 1.00 1.00 10.00 Diabetes Care 2003; 26: Aspirin better Aspirin worse
 Main combined end-point. 20 (3.9%) 22 (4.3%) 30 (1.6%) 51 (2.7%) 0.90 ( ) 0.69 ( ) Total CV events. 53 (10.2%) 59 (11.5%) 98 (5.3%) 142 (7.5%) 0.89 ( ) 0.70 ( ) All deaths. 25 (4.8%) 20 (3.9%) 42 (2.3%) 61 (3.2%) 1.23 ( ) 0.32 ( ) Cardiovascular. 10 (1.9%) 8 (1.6%) 8 (0.4%) 25 (1.3%) 1.23 ( ) 0.97 ( ) Non-cardiovascular. 15 (2.9%) 12 (2.3%) 34 (1.9%) 36 (1.9%) 1.23 ( ) 0.69 ( ) All myocardial infarction. 5 (1.0%) 10 (2.0%) 15 (0.8%) 22 (1.2%) 0.49 ( ) 0.59 ( ) All stroke. 9 (1.7%) 10 (2.0%) 11 (0.6%) 19 (0.1%) 0.89 ( ) 0.85 ( ) Angina pectoris. 13 (3.1%) 16 (3.9%) 42 (2.7%) 51 (3.1%) 0.80 ( ) 0.71 ( ) TIA. 7 (1.7%) 10 (2.4%) 22 (1.4%) 32 (2.0%) 0.69 ( ) 0.38 ( ) Peripheral artery disease. 11 (2.6%) 13 (3.2%) 6 (0.4%) 16 (1.0%) 0.83 ( ) 0.70 ( ) Revasculatisation proced (1.9%) 10 (2.4%) 15 (1.0%) 22 (1.4%) 0.79 ( ) Diabetes Care 2003; 26: Aspirin better. Aspirin worse.")
15
Sanderson, S. et. al. Ann Intern Med 2005;142:370-380

16
We included 34 full-text articles and 8 meeting abstracts
We included 34 full-text articles and 8 meeting abstracts. The mean prevalence of aspirin resistance was 24% (95% CI 20%-28%). After adjustment for differences in definition, used dosage, and population, a statistically significant higher prevalence was found in studies with aspirin dosage V100 mg compared with z300 mg (36% [95% CI 28%-43%] vs 19% [95% CI 11%-26%], P b .0001). Studies measuring platelet aggregation using light aggregometry with arachidonic acid as an agonist had a pooled unadjusted prevalence of 6% (95% CI 0%-12%). In studies using point-of-care platelet function–analyzing devices, the unadjusted prevalence was significantly higher, at 26% (95% CI 21%-31%).
. After adjustment for differences in definition, used dosage, and population, a statistically significant higher prevalence was found in studies with aspirin dosage V100 mg compared with z300 mg (36% [95% CI 28%-43%] vs 19% [95% CI 11%-26%], P b .0001). Studies measuring platelet aggregation using light aggregometry with arachidonic acid as an agonist had a pooled unadjusted prevalence of 6% (95% CI 0%-12%). In studies using point-of-care platelet function–analyzing devices, the unadjusted prevalence was significantly higher, at 26% (95% CI 21%-31%).")
17
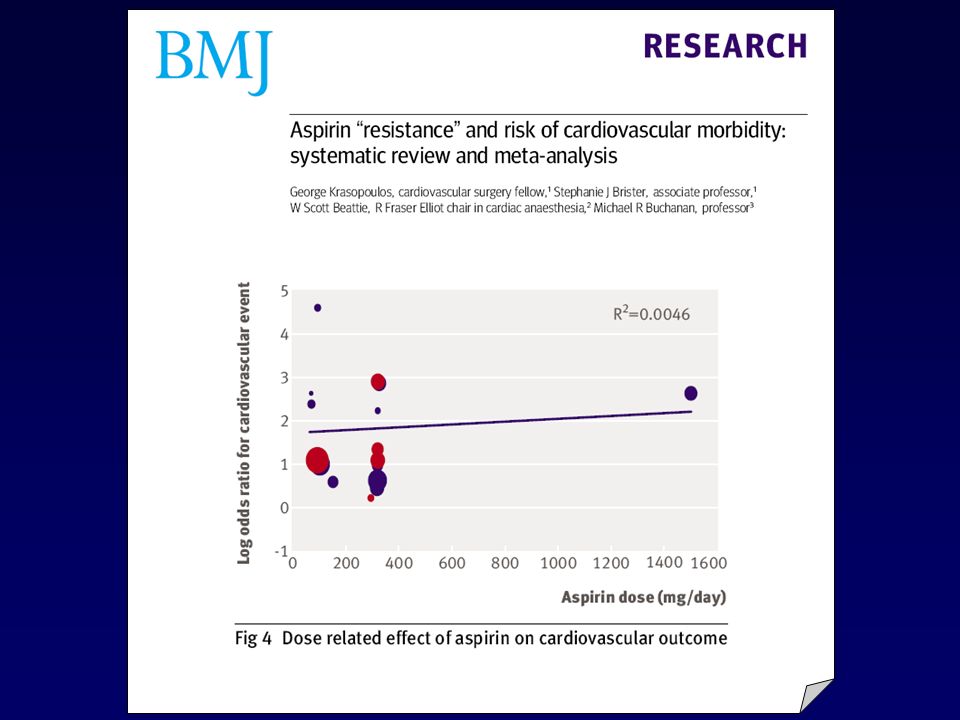
20 studies totalling 2930 patients with cardiovascular disease were identified.
Overall, 810 patients (28%) were classified as aspirin resistant. A cardiovascular related event occurred in 41% of patients (odds ratio 3.85, 95% confidence interval 3.08 to 4.80), death in 5.7%(5.99, 2.28 to 15.72),and an acute coronary syndrome in 39.4% (4.06, 2.96 to 5.56). Aspirin resistant patients did not benefit from other antiplatelet treatment.
 were classified as aspirin resistant. A cardiovascular related event occurred in 41% of patients (odds ratio 3.85, 95% confidence interval 3.08 to 4.80), death in 5.7%(5.99, 2.28 to 15.72),and an acute coronary syndrome in 39.4% (4.06, 2.96 to 5.56). Aspirin resistant patients did not benefit from other antiplatelet treatment.")
19
RIDOTTA EFFICACIA DELL’ASPIRINA:
POSSIBILI MECCANISMI Presenza di un ambiente pro-infiammatorio e pro-trombotico con attivazione piastrinica attraverso vie alternative che non richiedono il coinvolgimento del TXA2 Sintesi di TXA2 non sensibile all’azione dell’ASA Cause genetiche: polimorfismi del gene del COX-1, del recettore della Glicoproteina IIb/IIIa (PIA2) o di altri geni.
 o di altri geni.")
20
Inflammatory reaction
REAZIONE INFIAMMATORIA NELLA PLACCA E EFFICACIA ANTI-TROMBOTICA DELL’ASPIRINA cytokines CD40L Inflammatory reaction MMP TF COX-1 TxA2 Thrombin ASA-insensitive platelet activation ASA-sensitive TxA2 synthesis TxA2 synthesis Platelets AGEs ROS Hyperglycemia Hyperinsulinemia Insulin Resistance Dyslipidemia Hypertension DIABETES Platelet reactivity Leukocyte adhesion TF expression TF expressing microparticles ROS production Endothelial dysfunctions Adhesive molecules Chemokines COX-2 TxA2 PgI2 NO PAI-1 Circulating cells dysfunctions Atherosclerotic plaque Plaque instability COX-2 Evangelista V. Thromb Haemost. 2005;93:8-16

21
Urinary 11-dehydro-TXB2, plasma sCD40 L, and sP-selectin were measured, together with indices of low-grade inflammation, glycemic control, and lipid profile, in 82 patients with type-2 diabetes and 39 without diabetes, treated with low doses of aspirin.

22
ASPIRINO RESISTENZA: ASPETTI CLINICI
Reduced sensitivity of platelets from type 2 diabetic patients to acetylsalicylic acid (aspirin) – its relation to metabolic control The reduced response of platelets from diabetic subjects to aspirin was associated with a higher level of HbA1c, lower concentration of HDL-cholesterol and a higher total cholesterol concentration. 48 control healthy volunteers and 31 type 2 DM patients. In majority of control subjects (69%) and minority of diabetic patients (29%, p=0.0006), the use of 150 mg aspirin daily for 1 week significantly reduced platelet adhesiveness and reactivity (by 14.1% in diabetes vs. 78.6% in control, p=0.0035, as expressed by the relative changes in CTCEPI). Curves of the inhibition by ASA of the collagen (a) or arachidonic acid-induced aggregation in platelet-rich plasma from diabetic patients ( ) and control healthy subjects ( ). Watala C. Thrombosis Research 2004; 113:
 – its relation to metabolic control. The reduced response of platelets from diabetic subjects to aspirin was associated with a higher level of HbA1c, lower concentration of HDL-cholesterol and a higher total cholesterol concentration. 48 control healthy volunteers and 31 type 2 DM patients. In majority of control subjects (69%) and minority of diabetic patients (29%, p=0.0006), the use of 150 mg aspirin daily for 1 week significantly reduced platelet adhesiveness and reactivity (by 14.1% in diabetes vs. 78.6% in control, p=0.0035, as expressed by the relative changes in CTCEPI). Curves of the inhibition by ASA of the collagen (a) or arachidonic acid-induced aggregation in platelet-rich plasma from diabetic patients ( ) and control healthy subjects ( ). Watala C. Thrombosis Research 2004; 113:")
23
A total of 201 T2DM and 65 nondiabetic patients with coronary artery disease in a steady phase of aspirin and clopidogrel treatment were studied.

24
RIDUZIONE DEL POTENZIALE INFIAMMATORIO NELLA PLACCA E MIGLIORAMENTO DELLA EFFICACIA ANTI-TROMBOTICA DELL’ASPIRINA ACE - I TZDs STATINS x Hyperinsulinemia Insulin Resistance Endothelium Û Adhesive molecules Û Chemokines Û Hyperglycemia Û COX - 2 TxA 2 INFLAMMATION Ü PgI Û PAI - 1 2 Ü NO Dyslipidemia DIABETES Circulating cells Aspirin Resistance Û Leukocyte adhesion Û TF expression Hypertension Û TF expressing microparticles Atherosclerotic plaque THROMBOSIS AGEs Û TF Û MMPs Û TxA ROS 2 Evangelista V. Thromb Haemost. 2005;93:8-16

26
CONCLUSIONI La terapia antiaggregante con ASA potrebbe essere meno efficace nei soggetti con DM per la presenza di un contesto trombogenico poco influenzabile dall’inibizione della COX-1 piastrinica Non è chiaro se il DM possa rappresentare un caso particolare di “aspirino-resistenza” A tutt’oggi esistono controversie riguardo il fenomeno dell’aspirino resistenza: Mancanza di una definizione standard Prevalenza del fenomeno non chiara Assenza di un meccanismo biologico chiaramente definito Incertezza riguardo la sua rilevanza per la prevenzione CV Assenza di provate strategie terapeutiche per le persone affette Gli studi in corso, che coinvolgono numeri importanti di pazienti con DM, potranno contribuire a chiarire il ruolo dell’ASA nella prevenzione degli eventi CV

Presentazioni simili