Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
UPDATE DELLA PROFILASSI ANTITROMBOTICA E MECCANICA
B. Cosmi U.O. di Angiologia e Malattie della Coagulazione “Marino Golinelli” Policlinico S. Orsola-Malpighi Bologna

2
Evolution of Venous Thromboembolism Prophylaxis
1940s Early mobilization 1940s Heparin 1950s Warfarin 1960s Dextrans 1970s Low-dose heparin (LDH) 1980s Low Molecular Weight Heparins (LMWH) 1990s Parenteral direct thrombin inhibitor (DTI) (hirudin) 2002 Fondaparinux (Pentasaccharide) 2008 Oral direct thrombin inhibitors ???? Oral Factor Xa Inhibitors
 1980s Low Molecular Weight Heparins (LMWH) 1990s Parenteral direct thrombin inhibitor (DTI) (hirudin) 2002 Fondaparinux (Pentasaccharide) 2008 Oral direct thrombin inhibitors. Oral Factor Xa Inhibitors.")
3
Profilassi del TEV nei paz
Profilassi del TEV nei paz. chirurgici con i nuovi farmaci antitrombotici Profilassi meccanica Profilassi del TEV nel paz. medico

4
Obiettivi nello sviluppo di nuovi anticoagulanti
effetto dose risposta prevedibile assenza interazioni con cibo e farmaci possibilità di somministrazione a dosi fisse senza monitoraggio di laboratorio semplificare terapia anticoagulante a lungo termine

5
Stadi della ricerca clinica con i nuovi anticoagulanti
1° stadio: profilassi del tromboembolismo venoso in chirurgia ortopedica maggiore 2° stadio: terapia del tromboembolismo venoso 3° stadio : sindromi coronariche acute e fibrillazione atriale

6
I nuovi farmaci Anticoagulanti: Indiretti (AT-mediati) Fondaparinux Idraparinux Diretti (anti IIa) Dabigatran (anti Xa) Rivaroxaban Apixaban
 Rivaroxaban Apixaban.")
7
PENTASACCHARIDES Arixtra (fondaparinux) idraparinux (SanOrg34006)
 idraparinux (SanOrg34006)")
8
Fondaparinux : The first of a new class of synthetic selective inhibitors of factor Xa
Five saccharide units Synthetic Highly selective for AT3 Factor Xa inhibition No binding with plasma proteins No effect on platelet function No thrombocytopenia Pentasaccharide* is the first of a new class of synthetic antithrombotics: the selective factor Xa inhibitors. This is highlighted by the distinct INN, fondaparinux sodium. Pentasaccharide* is a unique and novel pentasaccharide produced by total chemical synthesis. It was designed specifically to bind its agent, the protein antithrombin (ATIII), with very high affinity. The crystal structure of Pentasaccharide* is illustrated on the slide. empirical formula C31H43N3O49S8Na10 molecular weight 1728 Daltons. Pentasaccharide* is obtained exclusively by chemical synthesis from basic building blocks synthesized from glucose, glucosamine and cellobiose. guaranteed batch-to-batch consistency eliminates the risk of contamination by pathogenic agents from animal sources. *fondaparinux Herbert JM, Petitou M, Lormeau JC, Cariou R, Necciari J, Magnani HN, et al. SR90107A/Org 31540, a novel anti-factor Xa antithrombotic agent. Cardiovasc Drug Rev., 1997, 15(1): 1–26 van Boeckel CAA, Petitou M. The unique antithrombin binding domain of heparin: a lead to new synthetic antithrombotics. Angew Chem Int Ed Engl. 1993; 32:1671–1690
, with very high affinity. The crystal structure of Pentasaccharide* is illustrated on the slide. empirical formula C31H43N3O49S8Na10. molecular weight 1728 Daltons. Pentasaccharide* is obtained exclusively by chemical synthesis from basic building blocks synthesized from glucose, glucosamine and cellobiose. guaranteed batch-to-batch consistency. eliminates the risk of contamination by pathogenic agents from animal sources. *fondaparinux. Herbert JM, Petitou M, Lormeau JC, Cariou R, Necciari J, Magnani HN, et al. SR90107A/Org 31540, a novel anti-factor Xa antithrombotic agent. Cardiovasc Drug Rev., 1997, 15(1): 1–26. van Boeckel CAA, Petitou M. The unique antithrombin binding domain of heparin: a lead to new synthetic antithrombotics. Angew Chem Int Ed Engl. 1993; 32:1671–1690.")
9
Meccanismo d’azione del Pentasaccaride

10
Fondaparinux Molecular weight 1500 d Rapid onset of action
Plasma half life h 1 administration/day Renal elimination No monitoring No specific antidote available, but the effects are reversed by F. VIIa

11
EFFICACIA DEL FONDAPARINUX NELLA PROFILASSI DEL
TROMBOEMBOLISMO VENOSO IN CHIRURGIA ORTOPEDICA

12
Serious adverse events and bleeding
From first injection to day 11 - All treated patients Fondaparinux Enoxaparin NNH Patients With (N=3616) (N=3621) SAE 196 (5.4 %) 164 (4.5 %) Fatal bleeding 1 Non-fatal bleeding in 1 critical organ Bleeding leading to re-operation 12 (0.33 %) 9 (0.25 %) Bleeding with transfusion ≥ 2 units 84 (2.3%) 52 (1.4 %) and/or hemoglobin decrease ≥ 2g/dL 109 (3.01%) 99 (2.73%) Other Bleeding
 (N=3621) SAE. 196 (5.4 %) 164 (4.5 %) 111. Fatal bleeding. 1. Non-fatal bleeding in. 1. critical organ. Bleeding leading to re-operation. 12 (0.33 %) 9 (0.25 %) 125. Bleeding with. transfusion ≥ 2 units. 84 (2.3%) 52 (1.4 %) 111. and/or hemoglobin. decrease ≥ 2g/dL. 109 (3.01%) 99 (2.73%) 357. Other Bleeding.")
13
Prophylaxis in fractured hip surgery
Pentifra-plus Prophylaxis in fractured hip surgery n = 326 Arixtra 2.5 mg od INITIAL TREATMENT PERIOD (7 ± 1 DAYS) Double- Blind HFS Total Treatment Duration 21 ± 2 Days R Arixtra 2.5 mg od Placebo n = 330 Venogram Day 19–24
 Double- Blind. HFS. Total Treatment Duration. 21 ± 2 Days. R. Arixtra. 2.5 mg od. Placebo. n = 330. Venogram Day 19–24.")
15
Il Fondaparinux non provoca HIT
- Non reazione crociata di Fondaparinux con gli anticorpi associati all’HIT negli studi in vitro - Non casi di HIT negli studi clinici di fase II e III - Non casi di HIT nell’analisi dei dati di esposizione al farmaco nel periodo 07/12/2001 al 31/12/2005 riferita a pazienti (Periodic Safety Update Report di fondaparinux relativi al periodo 05Dic Dic2005)
")
16
Direct Thrombin Inhibition
Tissue Factor XIIa XIa VIIa Factor II (Prothrombin) Fibrinogen XII VII X XI IXa IX Xa Thrombin Lepirudin Bivalirudin Argatroban Ximelagatran (oral) Dabigatran (oral) This slide needs some “re-animation”: First click: To appear “intrinsic and extrinsic activation and the arrows including factor IX and VII leading to factor X” Second click: Arrow from factor X to factor Xa and all downward reactions leding to fibrin. Please delete “32 U” Third click: The three arrows on the right side (TFPI and antithrombin). Please delete “1 ug” and “1000 ug”. Fourth click: The orange text on the left side and simultaneously orange circles around II, VII, IX and X Fibrin
 Fibrinogen. XII. VII. X. XI. IXa. IX. Xa. Thrombin. Lepirudin Bivalirudin Argatroban. Ximelagatran (oral) Dabigatran (oral) This slide needs some re-animation : First click: To appear intrinsic and extrinsic activation and the arrows including factor IX and VII leading to factor X Second click: Arrow from factor X to factor Xa and all downward reactions leding to fibrin. Please delete 32 U Third click: The three arrows on the right side (TFPI and antithrombin). Please delete 1 ug and 1000 ug . Fourth click: The orange text on the left side and simultaneously orange circles around II, VII, IX and X. Fibrin.")
17
Struttura del Dabigatran etexilate
Ingelheim/Germany, 27 March 2008 Boehringer Ingelheim today announced that the European Commission has granted marketing authorisation of the novel, oral direct thrombin inhibitor, Pradaxa® (dabigatran etexilate) in all 27 EU member states. It is anticipated that Pradaxa® will be launched in Germany and the United Kingdom in the coming weeks Struttura del Dabigatran etexilate Inibitore diretto della trombina, orale
 in all 27 EU member states. It is anticipated that Pradaxa® will be launched in Germany and the United Kingdom in the coming weeks. Struttura del Dabigatran etexilate. Inibitore diretto della trombina, orale.")
19
total-hip replacement were Randomized
Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial Bengt I Eriksson BI et al RE-NOVATE Lancet 2007; 370: 949–56 3494 patients total-hip replacement were Randomized to one of two doses of dabigatran etexilate (220 mg or 150 mg once daily) or enoxaparin (40 mg sc once daily), given for one month. The primary efficacy outcome was the composite of total VTE (venographic or symptomatic) and death from all causes during treatment.
 or enoxaparin (40 mg sc once daily), given for one month. The primary efficacy outcome was the composite of total VTE (venographic or symptomatic) and death from all causes during treatment.")
20
RE-NOVATE: Major results
End point Dabigatran 150 mg (%) Dabigatran 220 mg (%) Enoxaparin 40 mg (%) Total VTE and death from all causes 8.6 6.0 6.7 Major bleeding 1.3 2.0 1.6
 Dabigatran 220 mg (%) Enoxaparin 40 mg (%) Total VTE and death from all causes Major bleeding")
22
Oral dabigatran etexilate vs
Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. Eriksson BI et al. J Thromb Haemost Nov;5(11): 2076 patients dabigatran etexilate, 150 mg or 220 mg once-daily, starting with a half-dose 1-4 hours after surgery, or subcutaneous enoxaparin 40 mg once-daily, starting the evening before surgery, for 6-10 days. Follow-up for 3 months The primary efficacy outcome was a composite of total VTE (venographic or symptomatic) and mortality during treatment, and the primary safety outcome was the incidence of bleeding events
: patients. dabigatran etexilate, 150 mg or 220 mg once-daily, starting with a half-dose 1-4 hours after surgery, or subcutaneous enoxaparin 40 mg once-daily, starting the evening before surgery, for 6-10 days. Follow-up for 3 months. The primary efficacy outcome was a composite of total VTE (venographic or symptomatic) and mortality during treatment, and the primary safety outcome was the incidence of bleeding events.")
23
Oral dabigatran etexilate vs
Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. Eriksson BI et al. J Thromb Haemost Nov;5(11): End point Dabigatran 150 mg (%) Dabigatran 220 mg (%) Enoxaparin 40 mg (%) Total VTE, and all-cause mortality (primary end point) Major Bleeding 40.5% 1.3% 36.4% 1.5% 37.7%
: End point. Dabigatran 150 mg (%) Dabigatran 220 mg (%) Enoxaparin 40 mg (%) Total VTE, and all-cause mortality (primary end point) Major. Bleeding. 40.5% 1.3% 36.4% 1.5% 37.7%")
24
Combined analysis of dabigatran trials
End point Dabigatran 150 mg (%) Dabigatran 220 mg (%) Enoxaparin (%) Major VTE and VTE-related death 3.8 3.0 3.3 Major bleeding 1.1 1.4
 Dabigatran 220 mg (%) Enoxaparin (%) Major VTE and VTE-related death Major bleeding")
25
“Dabigatran etexilate”
Dose di 110 mg ( ½ cp) h dopo chirurgia 220 mg/die 10 gg dopo protesi ginocchio 28-35 gg dopo protesi anca Se età > 75 aa o IRC moderata 150 mg
 h dopo chirurgia. 220 mg/die. 10 gg dopo protesi ginocchio gg dopo protesi anca. Se età > 75 aa o IRC moderata. 150 mg.")
26
“Dabigatran etexilate”
Studi in fase III (non-inferiorità verso TAO) Re-COVER: TEV acuta, 5 gg LMWH poi random. (doppio cieco) a Dab. (150 mg x 2) o TAO x 6 mesi Re-MEDY: prev. secondaria; dopo 3-6 m. di TAO, random., cieco; Dab. (150 mg x 2) o TAO x 18 mesi
 Re-COVER: TEV acuta, 5 gg LMWH poi random. (doppio cieco) a Dab. (150 mg x 2) o TAO x 6 mesi. Re-MEDY: prev. secondaria; dopo 3-6 m. di TAO, random., cieco; Dab. (150 mg x 2) o TAO x 18 mesi.")
27
Direct Factor Xa inhibition
XIIa Tissue factor × XIa VIIa IXa Xa Rivaroxaban Apixaban DU-176b YM150 LY517717 PRT Factor II (prothrombin) Fibrinogen Fibrin clot
 Fibrinogen. Fibrin clot.")
29
Apixaban A highly potent, oral, direct FXa inhibitor (Ki 0.08 nM)
Follow-up to razaxaban (development halted due to bleeding concerns) Phase II study for VTE prevention after TKR: completed Double-blind; dose-ranging; three od and three bid apixaban doses; comparator enoxaparin and warfarin; target enrolment n=1202 Phase II pilot study for VTE prevention in patients with advanced metastatic cancer: ongoing
 Phase II study for VTE prevention after TKR: completed. Double-blind; dose-ranging; three od and three bid apixaban doses; comparator enoxaparin and warfarin; target enrolment n=1202. Phase II pilot study for VTE prevention in patients with advanced metastatic cancer: ongoing.")
30
Struttura del Rivaroxaban

31
A Once-Daily, Oral, Direct Factor Xa Inhibitor, Rivaroxaban (BAY ), for Thromboprophylaxis After Total Hip Replacement Eriksson et al. Circulation. 2006;114:

32
Rivaroxaban bid (THR/TKR pooled):
10 20 30 40 50 60 Enoxaparin DVT, PE, and all-cause mortality Major bleeding Estimated incidence rate* (%) Rivaroxaban (mg total daily dose) 5 Efficacy: p=0.39 The highlighted section demonstrates the wide therapeutic window of rivaroxaban – where the observed efficacy and safety of rivaroxaban were similar to those of enoxaparin. Turpie AGG et al. Thromboprophylaxis after orthopaedic surgery with an oral, direct Factor Xa inhibitor: pooled results of two phase IIb clinical trials. Blood 2005;106(11):Abstract 277. Oral presentation at the 47th American Society of Hematology meeting, Atlanta, GA, 9–13 December 2005 Safety: p<0.0001 *Estimated rates calculated by logistic regression adjusted for study, age, and gender
 Rivaroxaban (mg total daily dose) 5. Efficacy: p=0.39. The highlighted section demonstrates the wide therapeutic window of. rivaroxaban – where the observed efficacy and safety of rivaroxaban were. similar to those of enoxaparin. Turpie AGG et al. Thromboprophylaxis after orthopaedic surgery with an oral, direct Factor. Xa inhibitor: pooled results of two phase IIb clinical trials. Blood 2005;106(11):Abstract 277. Oral presentation at the 47th American Society of Hematology meeting, Atlanta, GA, 9–13. December Safety: p< *Estimated rates calculated by logistic regression adjusted for study, age, and gender.")
33
Rivaroxaban

34
RECORD – REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
Rivaroxaban 10 mg od will be compared with enoxaparin in over 10,000 patients worldwide RECORD 1: THR, 5 weeks therapy RECORD 2: THR, 5 weeks vs 10–14 days enoxaparin RECORD 3: TKR, 10–14 days therapy RECORD 4: TKR, 10–14 days therapy

35
Rivaroxaban

36
Rivaroxaban

37
Rivaroxaban

38
RECORD 3: Major efficacy end points
Rivaroxaban (%) Enoxaparin (%) Relative risk reduction (%) p DVT, nonfatal PE, all-cause mortality 9.6 18.9 49 <0.001 Major VTE (proximal DVT, nonfatal PE, and VTE-related death) 1.0 2.6 62 0.01 Lassen M et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.
 Enoxaparin (%) Relative risk reduction (%) p. DVT, nonfatal PE, all-cause mortality < Major VTE (proximal DVT, nonfatal PE, and VTE-related death) Lassen M et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.")
39
RECORD 3: Major safety end points
Outcome Rivaroxaban (%) Enoxaparin (%) p Major bleed 0.6 0.5 NS Any bleed 4.9 4.8 Lassen M et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.
 Enoxaparin (%) p. Major bleed NS. Any bleed Lassen M et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.")
40
Nuovi anticoagulanti: potenziali vantaggi
Fondapar. Idrapar. rapida azione; no controllo no HIT 1 somm./die o 1/sett Altri anti-Xa o anti-IIa orali; no controllo rapida azione

41
Nuovi anticoagulanti: potenziali svantaggi
No antidoti (eccetto SSR126517E) Difficile monitorare l’effetto (se emorragia) Non escludibili altri negativi effetti Breve tempo di emivita (vantaggi/svantaggi) Difficile controllare la compliance Costi
 Difficile monitorare l’effetto (se emorragia) Non escludibili altri negativi effetti. Breve tempo di emivita (vantaggi/svantaggi) Difficile controllare la compliance. Costi.")
42
PROFILASSI MECCANICA Calze elastiche :
prevenzione distensione venosa con riduzione stasi venosa nel polpaccio con miglioramento ritorno venoso CPI (compressione pneumatica intermittente; arto o solo piede) con manicotti gonfiabil ad intermittenza: solo paz. ospedalizzati Stimolano e mantengono flusso pulsatile nel circolo venoso profondo CPI aumentano velocità flusso in v. femorale comune dal 50 al 250% dei valori a riposo
 con manicotti gonfiabil ad intermittenza: solo paz. ospedalizzati. Stimolano e mantengono flusso pulsatile nel circolo venoso profondo. CPI aumentano velocità flusso in v. femorale comune dal 50 al 250% dei valori a riposo.")
43
ELASTIC COMPRESSION STOCKINGS FOR PREVENTION OF DEEP VEIN THROMBOSIS (Amaragiri SV, Lees TA, Cochrane Review, Cochrane Library Issue 3, 2002) Nove studi clinici randomizzati ( sia paz. Chirurgici che medici) CE da sole vs. controllo: TVP 13% vs. 27% RRR : 66% Sette studi clinici randomizzati (paz. Chirurgici) CE con altro metodo farmacologico: TVP 2% vs. 15% RRR: 76% Nessuno studio ha incluso paz a basso rischio In associazione alla profilassi farmacologica se: - sindrome varicosa - insufficienza venosa cronica - alto rischio
 CE da sole vs. controllo: TVP 13% vs. 27% RRR : 66% Sette studi clinici randomizzati (paz. Chirurgici) CE con altro metodo farmacologico: TVP 2% vs. 15% RRR: 76% Nessuno studio ha incluso paz a basso rischio. In associazione alla profilassi farmacologica se: - sindrome varicosa - insufficienza venosa cronica - alto rischio.")
44
Intermittent pneumatic compression and deep vein thrombosis prevention
Intermittent pneumatic compression and deep vein thrombosis prevention. A meta-analysis in postoperative patients. Urbankova et al. T& H, 2005; 2005 Dec;94(6):1181-5 RCT of IPC versus no prophylaxis, 2,270 patients in 15 eligible studies: 1,125 and 1,145 in the IPC and no prophylaxis group, respectively. The included studies formed a total of 16 treatment groups and were conducted in orthopedic (5), general surgical (4),oncologic (3), neurosurgical (3) and urologic (1) patient populations. In comparison to no prophylaxis, IPC devices reduced the risk of DVT by 60% (relative risk 0.40, 95% CI ; p < 0.001).
: RCT of IPC versus no prophylaxis, 2,270 patients in 15 eligible studies: 1,125 and 1,145 in the IPC and no prophylaxis group, respectively. The included studies formed a total of 16 treatment groups and were conducted in orthopedic (5), general surgical (4),oncologic (3), neurosurgical (3) and urologic (1) patient populations. In comparison to no prophylaxis, IPC devices reduced the risk of DVT by 60% (relative risk 0.40, 95% CI ; p < 0.001).")
45
Foot pump livelli di compressione maggiori per aumentare flusso in v
Foot pump livelli di compressione maggiori per aumentare flusso in v. femorale, più efficaci se utilizzate in combinazione con CE vs. CE sole Pochi confronti tra i vari apparecchi Non chiaro momento inizio e durata ottimali Compliance del paz. CPI > efficacia di CE in pz. A alto rischio in combinazione con anticoagulanti o se anticoagulanti controindicati

47
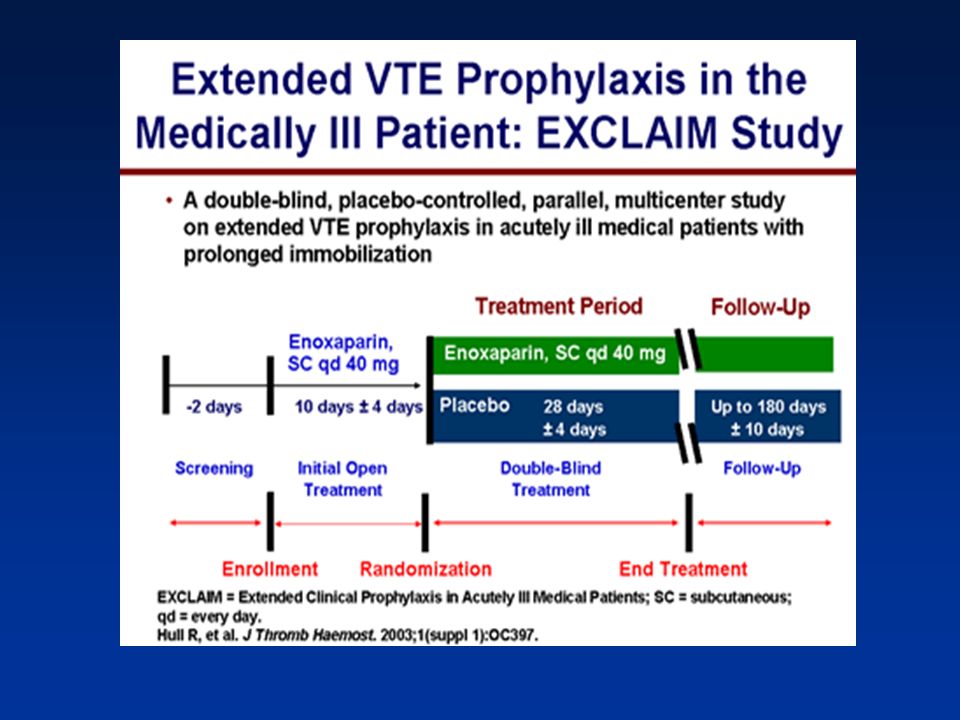
Outcome, extended prophylaxis, n=2052 (%) Outcome, placebo, n=2062 (%)
Efficacy outcomes during extended-duration enoxaparin therapy in high-risk nonsurgical patients End points Outcome, extended prophylaxis, n=2052 (%) Outcome, placebo, n=2062 (%) RR reduction (%) p VTE events* 2.8 4.9 44 0.0011 Symptomatic VTE 0.3 1.1 73 0.0044 Asymptomatic VTE 2.5 3.7 34 0.0319 *Primary efficacy end point: composite of asymptomatic DVT, symptomatic DVT, symptomatic pulmonary embolism, or fatal pulmonary embolism. Asymptomatic DVT was defined by compression ultrasonography, which was routinely performed. VTE=venous thromboembolism RR=relative risk Hull RD et al. EXCLAIM 2007 Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.
 Outcome, placebo, n=2062 (%) RR reduction (%) p. VTE events* Symptomatic VTE Asymptomatic VTE *Primary efficacy end point: composite of asymptomatic DVT, symptomatic DVT, symptomatic pulmonary embolism, or fatal pulmonary embolism. Asymptomatic DVT was defined by compression ultrasonography, which was routinely performed. VTE=venous thromboembolism. RR=relative risk. Hull RD et al. EXCLAIM 2007 Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.")
48
Safety outcomes during extended-duration randomized therapy in high-risk nonsurgical patients
End point Extended enoxaparin prophylaxis, n=2052 (%) Placebo, n=2062 (%) p Total bleeding events* 5.7 3.8 0.007 Major bleeding events 0.6 0.15 0.019 Minor bleeding events 5.2 3.7 0.024 *Primary safety end point Hull RD et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.
 Placebo, n=2062 (%) p. Total bleeding events* Major bleeding events Minor bleeding events *Primary safety end point. Hull RD et al Congress of the International Society on Thrombosis and Hemostasis; July 7-13, 2007; Geneva, Switzerland.")
Presentazioni simili




 Brussels, 26 settembre 2013.>")














>")

