Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Stefano Cascinu Clinica di Oncologia Medica Università Politecnica delle Marche Ancona Toxicities of molecularly targeted agents in combination with chemotherapy

2
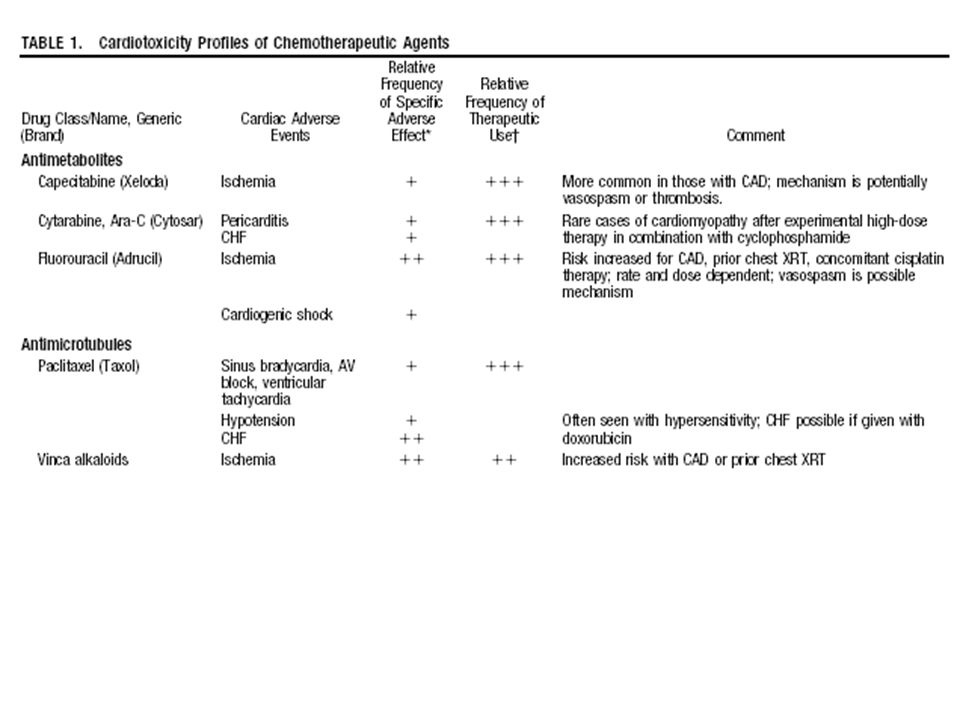
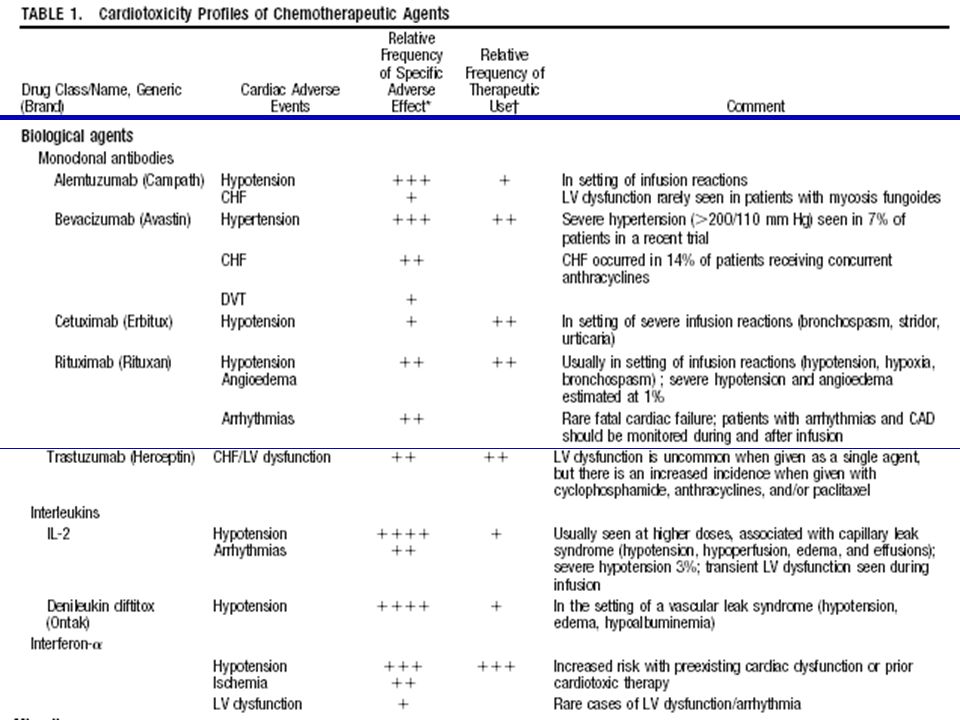
Tossicita’ dei nuovi agenti biologici
Trastuzumab Cardiotossicita’ Bevacizumab ipertensione Proteinuria Malattia tromboembolica Cetuximab Tossicita’ cutanea Sunitinib Diarrea astenia Imatinib Astenia diarrea

3
I farmaci biologici modificano o incrementano la tossicita’ dei chemioterapici ?
Trastuzumab Antracicline Bevacizumab Oxaliplatino irinotecan Taxani carboplatino Cetuximab Irinotecan taxani

8
Effetti della introduzione di H sulla tollerabilità cardiaca
NCCTG N9831 Effetti della introduzione di H sulla tollerabilità cardiaca La differenza della incidenza degli eventi cardiaci (scompensi e morti) tra terapie con H e senza è inferiore al 4%. Analisi a 9 mesi: 500 pz per braccio con diminuzione della LVEF 15% dal basale (dopo AC) - 0,0% (95% CI, 0,0-0,7%) per il braccio di controllo - 2,2% (95% CI, %) per il controllo vs sequenziale - 3,3% (95% CI, %) per il controllo vs terapia concomitante con paclitaxel * * a 9 mesi questi pazienti hanno ricevuto ulteriori cicli di H rispetto al gruppo sequenziale. Perez et al ASCO 2005
 tra terapie con H e senza è inferiore al 4%. Analisi a 9 mesi: 500 pz per braccio con diminuzione della LVEF 15% dal basale (dopo AC) - 0,0% (95% CI, 0,0-0,7%) per il braccio di controllo. - 2,2% (95% CI, %) per il controllo vs sequenziale. - 3,3% (95% CI, %) per il controllo vs. terapia concomitante con paclitaxel * * a 9 mesi questi pazienti hanno ricevuto ulteriori. cicli di H rispetto al gruppo sequenziale. Perez et al ASCO")
10
HERA TRIAL SAFETY ANALYSIS POPULATION SAFETY ANALYSIS POPULATION
Cardiotoxicity Cardiotoxicity Observation Observation Observation Observation 1 year trastuzumab 1 year trastuzumab 1 year trastuzumab 1 year trastuzumab N=1736 N=1736 N=1736 N=1736 N=1677 N=1677 N=1677 N=1677 Decrease by Decrease by Decrease by Decrease by ? ? ? ? 10 EF points 10 EF points 10 EF points 10 EF points 2.2 % 2.2 % 2.2 % 2.2 % 7.1 % 7.1 % 7.1 % 7.1 % and LVEF < 50% and LVEF < 50% and LVEF < 50% and LVEF < 50% Same LVEF criteria Same LVEF criteria Same LVEF criteria Same LVEF criteria 0 % 0 % 0 % 0 % and and and and symptomatic symptomatic symptomatic symptomatic 0.5% 0.5% 0.5% 0.5% (95% CI: 0.00 (95% CI: 0.00 (95% CI: 0.00 (95% CI: 0.00 - - - - CHF NYHA class CHF NYHA class CHF NYHA class CHF NYHA class (95% CI: 0.25 (95% CI: 0.25 (95% CI: 0.25 (95% CI: 0.25 - - - - 1.02) 1.02) 1.02) 1.02) 0.21) 0.21) 0.21) 0.21) III/IV, confirmed III/IV, confirmed III/IV, confirmed III/IV, confirmed by cardiologist by cardiologist by cardiologist by cardiologist Cardiac death Cardiac death 0.1% 0% Cardiac death Cardiac death
 1.02) 1.02) 1.02) 0.21) 0.21) 0.21) 0.21) III/IV, confirmed. III/IV, confirmed. III/IV, confirmed. III/IV, confirmed. by cardiologist. by cardiologist. by cardiologist. by cardiologist. Cardiac death. Cardiac death. 0.1% 0% Cardiac death. Cardiac death.")
13
Significantly Higher Pathologic Complete Remission Rate After Neoadjuvant Therapy With Trastuzumab, Paclitaxel, and Epirubicin Chemotherapy: Results of a Randomized Trial in Human Epidermal Growth Factor Receptor 2–Positive Operable Breast Cancer Buzdar et al JCO 2005 Event P>FEC alone n = 19 P>FEC +H n = 23 Grade 4 neutropenia 11 21 Neutropenic fever 8 Neutropenic infections 3 5 Hospitalization 1 Chemotherapy dose reduction as a result of neutropenia 10 Cardiac safety data CHF 10% decrease in ejection fraction Decrease on P Decrease on FEC 7 4 Improvement in ejection fraction on follow-up evaluation 2 Abnormal troponin-T

16
Trastuzumab + Docetaxel (n=92)
Efficacy and Safety of Trastuzumab Combined With Docetaxel in Patients With Human Epidermal Growth Factor Receptor 2–Positive Metastatic Breast Cancer Administered As First-Line Treatment: Results of a Randomized Phase II Trial by the M77001 Study Group Marty et al, JCO 2005 Toxicity Trastuzumab + Docetaxel (n=92) Docetaxel alone (n=94) Anemia 1 Thrombocitopenia Leukopenia 20 15 Neutropenia 32 22 Febrile neutropenia / Neutropenic sepsis 23 17 Alopecia 10 6 Astenia
 Docetaxel alone (n=94) Anemia. 1. Thrombocitopenia. Leukopenia Neutropenia Febrile neutropenia / Neutropenic sepsis Alopecia Astenia.")
19
I farmaci biologici modificano o incrementano la tossicita’ dei chemioterapici
Trastuzumab Antracicline Bevacizumab Oxaliplatino irinotecan Taxani carboplatino Cetuximab Irinotecan taxani

20
Unusual chemotherapy-related toxicity
Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Adverse events in the phase III trial that may be attributable to bevacizumab therapy are shown in this slide. Neither grade 3/4 bleeding nor grade 3/4 proteinuria were increased with bevacizumab. The most common adverse event was hypertension, which was easily managed using oral antihypertensive medication. Data were not been adjusted for differences in time on therapy between the two arms. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. NB: not adjusted for different time on therapy *p<0.05 Hurwitz H, et al. N Engl J Med 2004;350:2335–42

21
Hypertension: incidence
This slide shows the incidence of hypertensive events in clinical trials of bevacizumab in patients with CRC. Hypertension is the most common grade 3/4 adverse event seen in trials of bevacizumab plus chemotherapy and is consistent irrespective of the chemotherapy regimen to which bevacizumab is added. Grade 3 hypertension requires introduction of standard oral antihypertensives. Hypertension is easily managed in this way, but bevacizumab should be discontinued if hypertension remains uncontrolled. Study discontinuations, hospitalisations or deaths due to hypertension are rare. Giantonio BJ, Catalano PJ, Meropol NJ, et al. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): An updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November 2004. Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. NR = not reported
 to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): An updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. NR = not reported.")
22
Proteinuria: incidence
Proteinuria is a common event reported in approximately 20–40% of patients with CRC treated with bevacizumab. Grade 1 and 2 proteinuria are asymptomatic and are more common that grade 3 proteinuria (≤1%). In general, proteinuria improves after patients stop taking bevacizumab. Grade 4 proteinuria (nephrotic syndrome) has not been reported but would require discontinuation of bevacizumab. Similar results have been reported across all trials of bevacizumab. Giantonio BJ, Catalano PJ, Meropol NJ, et al. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): An updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November 2004. Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press.
. In general, proteinuria improves after patients stop taking bevacizumab. Grade 4 proteinuria (nephrotic syndrome) has not been reported but would require discontinuation of bevacizumab. Similar results have been reported across all trials of bevacizumab. Giantonio BJ, Catalano PJ, Meropol NJ, et al. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): An updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press.")
23
Thromboembolic events during first-line therapy (AVF2192)
Trial AVF2192g was a blinded, randomised phase II trial of 5-FU/LV with or without bevacizumab 5mg/kg every 2 weeks in patients with previously untreated metastatic CRC who were not optimal candidates for first-line irinotecan. In trial AVF2192g,1 the incidence of any thromboembolic event was not increased in patients receiving 5-FU/LV plus bevacizumab compared with chemotherapy plus placebo (18.0% vs 18.3%).2 Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. Novotny WF, Holmgren E, Nelson B, et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) does not increase the incidence of venous thromboembolism when added to first-line chemotherapy to treat metastatic colorectal cancer. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 3529. Novotny W, et al. J
.2. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. Novotny WF, Holmgren E, Nelson B, et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) does not increase the incidence of venous thromboembolism when added to first-line chemotherapy to treat metastatic colorectal cancer. J Clin Oncol 2004;22(July 15 Suppl.): Abstract Novotny W, et al. J.")
24
Thromboembolic events during first-line therapy (AVF2107)
Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. The overall incidence of thromboembolic events was similar across the two arms (IFL plus bevacizumab, 19.4% vs IFL plus placebo, 16.2%; p=0.26).1 The incidence of venous thromboembolic events was similar in both arms (16.6% vs 15.2%); the incidence of arterial thromboembolic events was increased in the IFL plus bevacizumab arm compared with the IFL plus placebo arm (3.3% vs 1.0%, respectively).1 Novotny WF, Holmgren E, Nelson B, et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) does not increase the incidence of venous thromboembolism when added to first-line chemotherapy to treat metastatic colorectal cancer. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 3529. Novotny W, et al. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 3529
.1. The incidence of venous thromboembolic events was similar in both arms (16.6% vs 15.2%); the incidence of arterial thromboembolic events was increased in the IFL plus bevacizumab arm compared with the IFL plus placebo arm (3.3% vs 1.0%, respectively).1. Novotny WF, Holmgren E, Nelson B, et al. Bevacizumab (a monoclonal antibody to vascular endothelial growth factor) does not increase the incidence of venous thromboembolism when added to first-line chemotherapy to treat metastatic colorectal cancer. J Clin Oncol 2004;22(July 15 Suppl.): Abstract Novotny W, et al. J Clin Oncol 2004;22(July 15 Suppl.): Abstract")
25
IFL/bevacizumab (n=150) n (%)
Bevacizumab does not increase wound healing/bleeding complications when given 28–60 days following cancer surgery Wound healing complications Complication IFL/placebo (n=155) (%) IFL/bevacizumab (n=150) n (%) 5-FU/LV/bevacizumab (n=37) (%) Abscess Perforated large intestine 1 (0.67) Perforated stomach ulcer All types (total) 2 (1.3) Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. A subgroup of patients in the phase III trial AVF2107 was treated with IFL plus placebo (n=155), IFL plus bevacizumab (n=150) and 5-FU/LV plus bevacizumab (n=37) 28–60 days after cancer surgery. Only two (1.3%) patients treated with IFL plus bevacizumab had a wound healing complication. No such complications were reported in patients treated with IFL plus placebo or 5-FU/LV plus bevacizumab. These data suggest that initiation of bevacizumab therapy 28–60 days after surgery does not increase the incidence of wound healing/bleeding complications. Scappaticci F, Fehrenbacher L, Cartwright T, Hainsworth J, et al. Lack of effect of bevacizumab on wound healing/bleeding complications when given days following primary cancer surgery. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 3530.
 (%) IFL/bevacizumab (n=150) n (%) 5-FU/LV/bevacizumab. (n=37) (%) Abscess. Perforated large intestine. 1 (0.67) Perforated stomach ulcer. All types (total) 2 (1.3) Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. A subgroup of patients in the phase III trial AVF2107 was treated with IFL plus placebo (n=155), IFL plus bevacizumab (n=150) and 5-FU/LV plus bevacizumab (n=37) 28–60 days after cancer surgery. Only two (1.3%) patients treated with IFL plus bevacizumab had a wound healing complication. No such complications were reported in patients treated with IFL plus placebo or 5-FU/LV plus bevacizumab. These data suggest that initiation of bevacizumab therapy 28–60 days after surgery does not increase the incidence of wound healing/bleeding complications. Scappaticci F, Fehrenbacher L, Cartwright T, Hainsworth J, et al. Lack of effect of bevacizumab on wound healing/bleeding complications when given days following primary cancer surgery. J Clin Oncol 2004;22(July 15 Suppl.): Abstract")
26
Bleeding complications
Bevacizumab does not increase wound healing/bleeding complications when given 28–60 days following cancer surgery (cont’d) Bleeding complications Haemorrhage IFL/placebo (n=155) n (%) IFL/bevacizumab (n=150) 5-FU/LV/bevacizumab (n=37) (%) GI 1 (0.65) Rectal 1 (0.67) All types Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Two patients (one in each of the IFL-containing arms) had bleeding complications when treated days after surgery. These results indicate that the addition of bevacizumab to IFL does not increase bleeding complications in patients with metastatic CRC when given 28–60 days after surgery. Scappaticci F, Fehrenbacher L, Cartwright T, Hainsworth J, et al. Lack of effect of bevacizumab on wound healing/bleeding complications when given days following primary cancer surgery. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 3530.
 Bleeding complications. Haemorrhage. IFL/placebo. (n=155) n (%) IFL/bevacizumab. (n=150) 5-FU/LV/bevacizumab. (n=37) (%) GI. 1 (0.65) Rectal. 1 (0.67) All types. Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without bevacizumab 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Two patients (one in each of the IFL-containing arms) had bleeding complications when treated days after surgery. These results indicate that the addition of bevacizumab to IFL does not increase bleeding complications in patients with metastatic CRC when given 28–60 days after surgery. Scappaticci F, Fehrenbacher L, Cartwright T, Hainsworth J, et al. Lack of effect of bevacizumab on wound healing/bleeding complications when given days following primary cancer surgery. J Clin Oncol 2004;22(July 15 Suppl.): Abstract")
27
Bleeding: incidence *Epistaxis + GI haemorrhage
Clinical trials have shown that minor bleeding (in the form of epistaxis) is increased in patients with CRC who are receiving bevacizumab. Bevacizumab-associated epistaxis is generally manageable and usually lasts less than 5 minutes. Grade 3/4 bleeding events are reported in ≤5% of patients receiving bevacizumab 5mg/kg every 2 weeks. The addition of bevacizumab to chemotherapy does not appear to increase the incidence of grade 3/4 bleeding.2–4 Giantonio BJ, Catalano PJ, Meropol NJ, O'Dwyer PJ, Benson AB. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): an updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November 2004. Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al, Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. *Epistaxis + GI haemorrhage
 is increased in patients with CRC who are receiving bevacizumab. Bevacizumab-associated epistaxis is generally manageable and usually lasts less than 5 minutes. Grade 3/4 bleeding events are reported in ≤5% of patients receiving bevacizumab 5mg/kg every 2 weeks. The addition of bevacizumab to chemotherapy does not appear to increase the incidence of grade 3/4 bleeding.2–4. Giantonio BJ, Catalano PJ, Meropol NJ, O Dwyer PJ, Benson AB. The addition of bevacizumab (anti-VEGF) to FOLFOX4 in previously treated advanced colorectal cancer (advCRC): an updated interim toxicity analysis of the Eastern Cooperative Oncology Group (ECOG) study E3200. Presented at: 2004 Gastrointestinal Cancers Symposium; 22–24 January 2004; San Francisco, Ca. Abstract 241. Available at: Accessed 15 November Kabbinavar F, Hurwitz HI, Fehrenbacher L, et al. Phase II, randomized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin (LV) with FU/LV alone in patients with metastatic colorectal cancer. J Clin Oncol 2003;21:60–5. Hurwitz H, Fehrenbacher L, Novotny W, et al, Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004,350:2335–42. Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus 5-FU/leucovorin in first-line metastatic colorectal cancer: results of a randomized phase II trial. J Clin Oncol In Press. *Epistaxis + GI haemorrhage.")
30
I farmaci biologici modificano o incrementano la tossicita’ dei chemioterapici
Trastuzumab Antracicline Bevacizumab Oxaliplatino irinotecan Taxani carboplatino EGFR inibitori (Cetuximab/TKI) Irinotecan gemcitabina taxani
 Irinotecan. gemcitabina. taxani.")
33
CRYSTAL trial: Safety: Grade 3/4 AE
FOLFIRI n=602, % Cetuximab + FOLFIRI n=600, % Any 59.5 78.0 Neutropenia 23.3 26.7 - Febrile neutropenia 2.2 2.7 Diarrhea 10.5 15.2 Vomiting 5.0 4.5 Fatigue Skin reactionsa 0.2 18.7 Hypomagnesemiab 1.8 Infusion-related reactions 2.3 aThere were no grade 4 skin reactions bAvailable only from a subset of patients (at least one measurement in 20% of population)
")
34
Tossicita’ dei nuovi agenti biologici
Trastuzumab Cardiotossicita’ Bevacizumab ipertensione Proteinuria Malattia tromboembolica Cetuximab Tossicita’ cutanea Sunitinib Diarrea astenia Imatinib Astenia diarrea

Presentazioni simili









>")














