Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Metastatic CRC: recent therapeutic developments
Dott. Carlo Garufi Oncologia Medica A Istituto Regina Elena, Roma

2
CRC Background Colorectal cancer is the fourth most common cancer in men and the third most common in women worldwide About 50% of patients will eventually die of their disease At diagnosis: the stage of the disease is the most important prognostic factor: five year survival for stage I: > 85%, stage IV: only 5-30% approximately 25% of patients will present with metastatic disease Around 50% of patients treated with current first-line chemotherapy regimens will develop progressive disease within months

3
Diferent Stage IV Disease in Different Patients
Disseminated Disease Local Recurrences Peritoneal Carcinosis Non-measurable Disease Lung Metastases Liver Metastases Resected Resectable Non-resectable

4
Strategia di Trattamento nelle Neoplasie del Colon-Retto
Malattia Incurabile Trattamento a lungo termine Tossicità accettabile Più linee di Terapia Malattia Curabile Massimo effetto antitumorale Tossicità maggiore Possibilità di resezione radicale Questo sembra essere il concetto portante del trattamento del ca colorettale in fase avanzata: identificare i pazienti che possono giovarsi di un trattamento aggressivo verso quelli nei quali bisogna pensare ad una continuità di cura. Nella malattia incurabile si pone il quesito dell’utilizzo di un regime di monoterapia. 4

5
Malattia Incurabile C’è un chiaro vantaggio in sopravvivenza nell’uso della chemioterapia di combinazione rispetto alla monochemioterapia? (± irinotecan; ± oxaliplatino) all’uso sequenziale dei farmaci? (FOCUS 2007, CAIRO 2007) Non è chiaro se tutti i pazienti in fase avanzata debbano essere trattati con una polichemioterapia. Saltz L, et al: NEJM 343: ,2000, Douillard JY et al: Lancet 355: , 2000, Giacchetti S et al: JCO 18:136-47, 2000, De Gramont A et al: JCO 18: , 2000 Seymour MT Lancet 370: , 2007; Koopman M et al. Lancet 370:135-42, 2007 5
 all’uso sequenziale dei farmaci (FOCUS 2007, CAIRO 2007) Non è chiaro se tutti i pazienti in fase avanzata debbano essere trattati con una polichemioterapia. Saltz L, et al: NEJM 343: ,2000, Douillard JY et al: Lancet 355: , 2000, Giacchetti S et al: JCO 18:136-47, 2000, De Gramont A et al: JCO 18: , Seymour MT Lancet 370: , 2007; Koopman M et al. Lancet 370:135-42,")
6
Trials di polichemioterapia vs monochemioterapia: Sopravvivenza
Saltz L. et al NEJM, 2000 Giacchetti S. et al, JCO 2000 Gli studi con la combinazione 5-fluorouracile-leucovorin-irinotecan hanno dimostrato aumento di sopravvivenza nei pazienti con cancro del colon-retto in fase avanzata di malattia rispetto alla stessa combinazione senza l’irinotecan (Saltz e Douillard) mentre ciò non è avvenuto con la combinazione 5-fluorouracile-leucovorin-oxaliplatino rispetto alla stessa combinazione senza l’oxaliplatino (Giacchetti e De Gramont). Douillard JY. et al The Lancet 2000 De Gramont A. et al JCO 2000
 mentre ciò non è avvenuto con la combinazione 5-fluorouracile-leucovorin-oxaliplatino rispetto alla stessa combinazione senza l’oxaliplatino (Giacchetti e De Gramont). Douillard JY. et al The Lancet De Gramont A. et al JCO")
7
Questo studio confronta 3 strategie differenti: monochemioterapia con 5-FU seguita da monochemioterapia con IRI versus 5-FU con aggiunta di OXA o IRI in 2° linea versus iniziale chemioterapia di combinazione 7

8
Non vi è nessuna differenza significativa nella sopravvivenza tra le tre strategie. Soltanto il gruppo trattato con irinotecan in combinazione con fluorouracile ha un vantaggio che diventa statisticamente significativo nella sopravvivenza. Si conferma che l’uso dell’oxaliplatino in prima linea aumenta il tasso di risposte ma non la sopravvivenza come dimostrato negli studi di De Gramont e Giacchetti. 30% dei pazienti dello studio nel braccio A non ha ricevuto un trattamento di seconda linea. FOCUS TRIAL 8

9
CAIRO TRIAL Koopman M et al. Lancet vol 370:135-142, 2007
Nel CAIRO una chemioterapia di combinazione con Capecitabina + IRI viene confrontata con Capecitabina da sola in prima linea. In questo studio il braccio di confronto con la monoterapia è rappresentato da un regime poco utilizzato per la scarsa tollerabilità. Koopman M et al. Lancet vol 370: , 2007 9

10
Monochemioterapia o Terapia di combinazione?
I risultati degli studi FOCUS e CAIRO possono giustificare l’uso iniziale di una monochemioterapia con Fluoropirimidine nei pazienti nei quali non vi sia indicazione ad un atteggiamento aggressivo Questi due studi randomizzati non escludono un trattamento sequenziale in pazienti per i quali la malattia è incurabile. 10

11
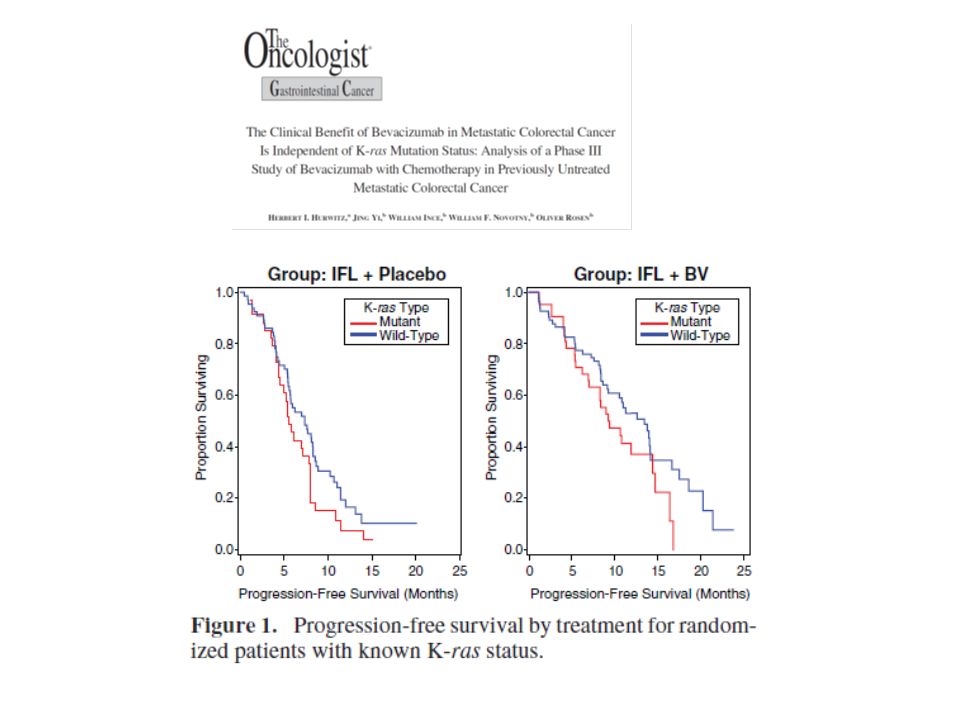
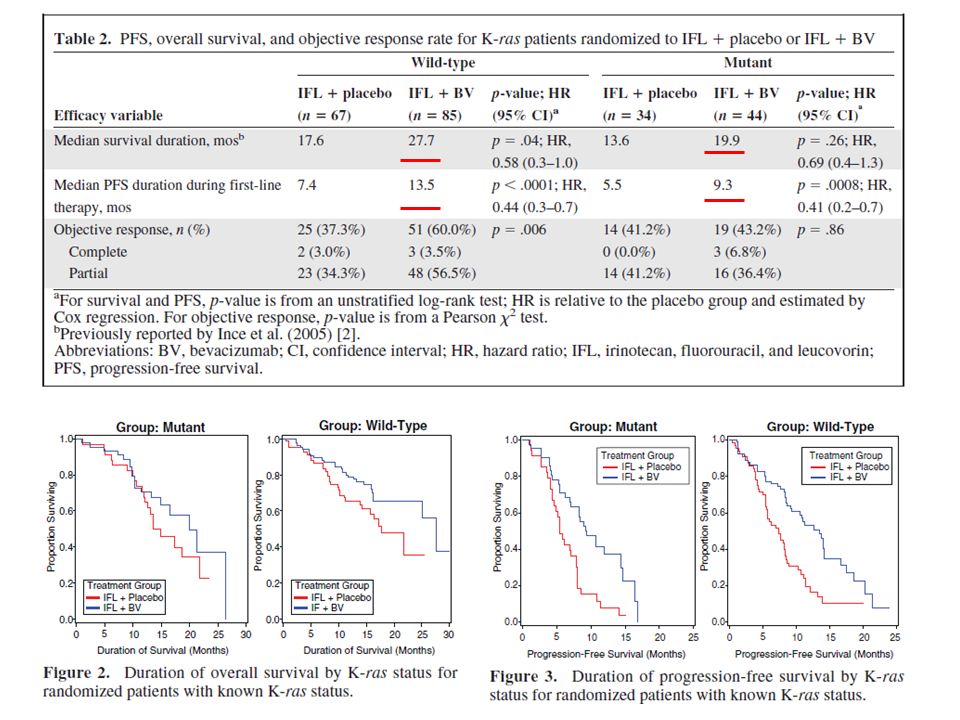
Cosa Aggiunge Bevacizumab?
In pazienti “unfit” Beva +5-FU/LV aumenta significativamente RR e PFS ed aumenta la OS da 12.9 a 16.6 mesi (Kabbinavar JCO 23:3697, 2005) In pazienti “fit” Beva +5-FU/LV è equivalente ad un regime come IFL in termini di RR, PFS ed OS (Hurwitz JCO 23:3502, 2005) Il Bevacizumab + 5-FU/LV migliora i risultati rispetto al 5-FU/LV da solo ed è equivalente all’IFL. 11
 In pazienti fit Beva +5-FU/LV è equivalente ad un regime come IFL in termini di RR, PFS ed OS (Hurwitz JCO 23:3502, 2005) Il Bevacizumab + 5-FU/LV migliora i risultati rispetto al 5-FU/LV da solo ed è equivalente all’IFL. 11.")
12
Kabbinavar F et al: JCO 23:3706-3712, 2005
L’aggiunta di Beva a 5-FU/LV aumenta significativamente la OS da 14.6 a 17.9 mesi, HR 0.74 p=0.008), PFS da 5.6 a 8.8 mesi, HR 0.63 con p≤ .0001, (Kabbinavar, JCO 23:3706, 2005). Dalla valutazione complessiva di questi studi si può dedurre che l’aggiunta del bevacizumab alla monoterapia con fluorofolato può rappresentare una ragionevole scelta terapeutica in questo setting di ammalati. Kabbinavar F et al: JCO 23: , 2005 12
, PFS da 5.6 a 8.8 mesi, HR 0.63 con p≤ .0001, (Kabbinavar, JCO 23:3706, 2005). Dalla valutazione complessiva di questi studi si può dedurre che l’aggiunta del bevacizumab alla monoterapia con fluorofolato può rappresentare una ragionevole scelta terapeutica in questo setting di ammalati. Kabbinavar F et al: JCO 23: ,")
13
Saltz L. et al: IFL NEJM 2004 Sobrero A et al: FOLFIRI Oncology 2009

14
Bevacizumab PRO CONTRO BEVA non ha attività come agente singolo
Regimi tipo FOLFIRI + BEVA o 5-FU/FA + BEVA aumentano il PFS e la OS in prima linea Efficacia indipendente da biomarkers Profilo di sicurezza ben definito Migliore utilizzo clinico quando usato fino a progressione BEVA può essere usato con sicurezza nei pazienti candidati a resezione di metastasi epatiche BEVA non ha attività come agente singolo Regimi tipo FOLFOX/XELOX + BEVA aumentano il PFS ma non OS in I linea (aumentano PFS e OS in II linea) I dati sull’uso della terapia di mantenimento con BEVA e dopo progressione devono essere confermati
 I dati sull’uso della terapia di mantenimento con BEVA e dopo progressione devono essere confermati.")
17
Clinical Anti-EGF Receptor Therapies
Anticorpi Monoclonali (Trastuzumab, Cetuximab, Panitumumab) Ligand R R Inibitori di Tirosin Kinasi “Piccole Molecole” (Imatinib, Sutinib, Sorafenib, Erlotinib) K K Signal Transduction
 Ligand. R. R. Inibitori di Tirosin Kinasi. Piccole Molecole (Imatinib, Sutinib, Sorafenib, Erlotinib) K. K. Signal Transduction.")
20
EGF down-stream signaling
courtesy by Vincenzi B.

21
EGFR GENE COPY NUMBER, FISH/CISH: MAIN STUDIES
Author Method N pts Correl. with Cet Outcome % ICN Notes Shia et al. CISH 147 NA 11.5% NDR Sauer et al. FISH 48 (15%) Not stated how many ICN Moroni et al. 30 Positive Enrichment strategy Lievre et al. 10% Amplification for 6 or > signals/nucleus in >50% of cells Garufi et al. 101 83% Only 4% amplified; Correlation with RR - PFS Romagnani et al. 27 Positive??? 89% Not clear definition of ICN Personeni et al. 70 Negative 92% Multiple centile cut-offs Sartore-Bianchi A. et al 58 Increased EGFR copy number associated with disease control and better PFS Finocchiaro et al. 85 48% Multiple criteria Only Moroni’s valid 21 21
 Not stated how many ICN. Moroni et al. 30. Positive. Enrichment strategy. Lievre et al. 10% Amplification for 6 or > signals/nucleus. in >50% of cells. Garufi et al % Only 4% amplified; Correlation with RR - PFS. Romagnani et al. 27. Positive 89% Not clear definition of ICN. Personeni et al. 70. Negative. 92% Multiple centile cut-offs. Sartore-Bianchi A. et al. 58. Increased EGFR copy number associated with disease control. and better PFS. Finocchiaro et al % Multiple criteria Only Moroni’s valid")
22
Campanella C et al. 2010

23
Campanella C et al. 2010

24
Tossicità cutanea ed Abs Anti-EGFR

25
Phase III CRYSTAL study: Design
ERBITUX + FOLFIRI ERBITUX IV 400 mg/m2 on day 1, then 250 mg/m2 weekly + irinotecan 180 mg/m2 + 5-FU/LV every 2 weeks EGFR-expressing mCRC R Stratification factors: Region ECOG performance status Populations: Randomized patients (n=1217) Safety population (n=1202) ITT population (n=1198) FOLFIRI Irinotecan 180 mg/m2 + 5-FU/LV every 2 weeks Van Cutsem E, et al. New Engl J Med 2009;360:1408–1417 25 25
 Safety population (n=1202) ITT population (n=1198) FOLFIRI. Irinotecan 180 mg/m FU/LV every 2 weeks. Van Cutsem E, et al. New Engl J Med 2009;360:1408–")
26
Overall survival in KRAS wt patients
Van Cutsem E, et al. ECCO/ESMO Congress 2009; Abstract No: 6077 Van Cutsem E, et al. ECCO/ESMO Congress 2009; Abstract No: 6077

27
WT KRAS: Overall Survival (Interim Analysis)
Events n (%) Median (95% CI) months Panitumumab + FOLFOX 106 (33) NE (20.3, NE) FOLFOX 124 (37) 18.8 (17.2, NE) HR = 0.83 (95% CI: 0.64–1.08) P-value = 0.16 Douillard - PRIME
 Median (95% CI) months. Panitumumab + FOLFOX. 106 (33) NE (20.3, NE) FOLFOX. 124 (37) 18.8 (17.2, NE) HR = 0.83 (95% CI: 0.64–1.08) P-value = Douillard - PRIME.")
28
COIN: Study design Patients with mCRC;
03/15/2007 Patients with mCRC; no prior CT for advanced disease; fit for combination CT; no prior testing for EGFR status 2445 randomized Arm A: Continuous CT (control) Continued until progression, cumulative toxicity, or patient choice Arm B: Continuous CT + ERBITUX (ERBITUX 400 mg/m2 day 1, then 250 mg/m2 weekly) Continued until progression, cumulative toxicity, or patient choice Arm C: Intermittent CT Treat for 12 weeks then stop CT and monitor. Restart same CT on progression for a further 12 weeks Second-line chemotherapy: After completion of trial therapy, patients will be eligible for treatment with irinotecan or entry into another clinical trial Maughan T. J Clin Oncol 2007;25(Suppl. 18):Abstract No. 4070 28
 Continued until progression, cumulative toxicity, or patient choice. Arm B: Continuous CT + ERBITUX. (ERBITUX 400 mg/m2 day 1, then 250 mg/m2 weekly) Continued until progression, cumulative toxicity, or patient choice. Arm C: Intermittent CT. Treat for 12 weeks then stop CT and monitor. Restart same CT on progression for a further 12 weeks. Second-line chemotherapy: After completion of trial therapy, patients will be eligible for treatment with irinotecan or entry into another clinical trial. Maughan T. J Clin Oncol 2007;25(Suppl. 18):Abstract No")
29
COIN: first efficacy analysis
xx/xx/xxxx % Erbitux + XELOX/OxMdG KRAS wt XELOX/OxMdG p OS months 17 17,9 NS PFS months 8.6 ORR 59% 50% 0.015 *Abs. 7LBA 29 Editor: Presentation name here

30
Diferent Stage IV Disease in Different Patients
Disseminated Disease Local Recurrences Peritoneal Carcinosis Non-measurable Disease Lung Metastases Liver Metastases Resected Resectable Non-resectable

31
POCHER STUDY Patients with unresectable liver metastases +/- extrahepatic disease RESECTION Adjuvant therapy for 4-6 courses (same schedule as pre-operatively) Technically resectable ERBITUX + CPT-FFL ~ (n=43) for 4-6 courses Technically unresectable 4 further treatment cycles Primary endpoint: Response rate 8 cycles (~4 months) Garufi C et al ECCO-ESMO, Berlin 2009
 Technically resectable. ERBITUX. + CPT-FFL ~ (n=43) for 4-6 courses. Technically unresectable. 4 further treatment cycles. Primary endpoint: Response rate. 8 cycles (~4 months) Garufi C et al ECCO-ESMO, Berlin")
32
PreOperative Chemotherapy Hepatic Resection POCHER STUDY
Cetuximab mg/m2 day1 CPT-11: 130 mg/m2day 1 peak 13:00 PreOperative Chemotherapy Hepatic Resection Istituto Regina Elena Roma Ospedale S Maria degli Angeli Pordenone Garufi C. et al ECCO/ESMO 2009

33
A B C D E F Pre-treatment (Fig. A-B-C) and after 6 courses (Fig. D-E-F) spiral TC-scan of SP patient. She was submitted to a two-step hepatectomy and she is free of disease after 36 months of follow-up.
 and after 6 courses (Fig. D-E-F) spiral TC-scan of SP patient. She was submitted to a two-step hepatectomy and she is free of disease after 36 months of follow-up.")
34
Figure 3. Kaplan-Meier curves of progression-free survival (PFS) and overall survival.
overall survival in the entire population (n = 43);B)PFS in the entire population (n = 43); (C) PFS in patients with resected liver metastases (n = 26)
;B)PFS in the entire population (n = 43); (C) PFS in patients with resected liver metastases (n = 26)")
35
ERBITUX and Liver Metastases
Doublets Triplet CT CT + ERBITUX Unselected population Selected population (liver metastases) LLD * ** * 10 20 30 40 50 60 70 80 10 20 30 40 50 60 70 80 80 10 20 30 40 50 60 70 80 79 * 70 79 P<0.0001 77 p=0.0027 60 57.3 57.3 50 Response (%) 40 39.7 34 30 20 10 CRYSTAL OPUS CELIM POCHER Van Cutsem E, et al. ECCOESMO 2009 Abs 6077 Van Cutsem E, et al. N Engl J Med 2009;360:1408–1417 Van Cutsem E, et al. Ann Oncol 2008;19(Suppl.8):viii4 [Update to 710] Bokemeyer C, et al. J Clin Oncol 2009;27:663–671 Bechstein WO, et al. J Clin Oncol 2009;27(Suppl. 15): Abstract No. 4091 Garufi C, et alECCO/ESMO, Berlin, 2009 *KRAS wt, **ITT LLD=liver-limited disease
 LLD. * ** * * P< p= Response (%) CRYSTAL. OPUS. CELIM. POCHER. Van Cutsem E, et al. ECCOESMO 2009 Abs Van Cutsem E, et al. N Engl J Med 2009;360:1408–1417. Van Cutsem E, et al. Ann Oncol 2008;19(Suppl.8):viii4 [Update to 710] Bokemeyer C, et al. J Clin Oncol 2009;27:663–671. Bechstein WO, et al. J Clin Oncol 2009;27(Suppl. 15): Abstract No Garufi C, et alECCO/ESMO, Berlin, *KRAS wt, **ITT. LLD=liver-limited disease.")
36
ERBITUX improves resections
60

37
Chemioterapia + Abs Anti-EGFR
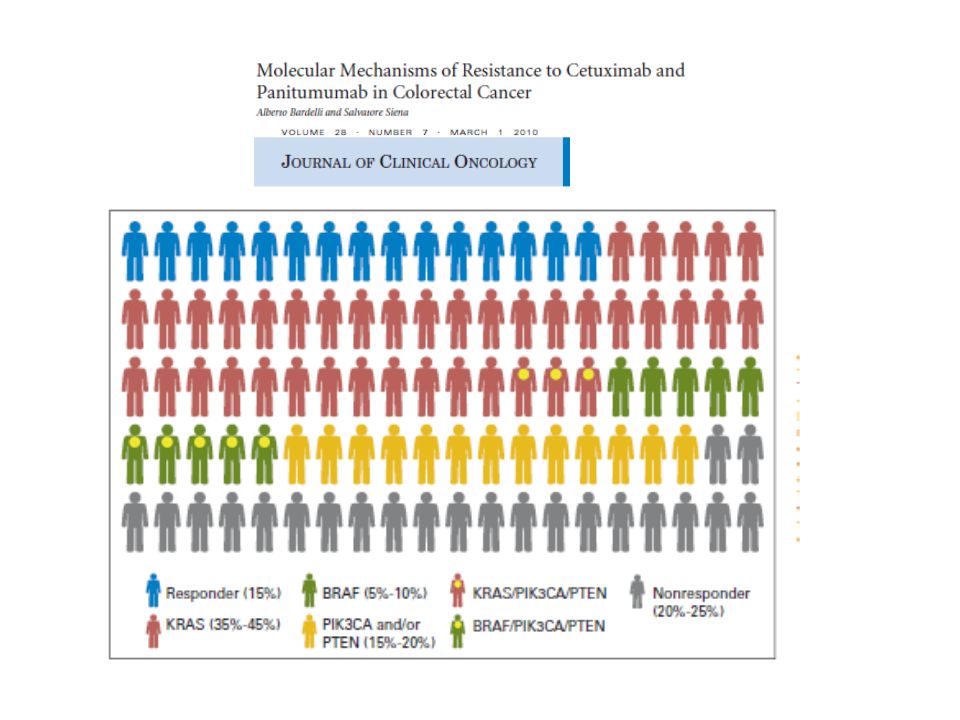
Abs (Cetuximab e Panitumumab) possono essere usati solo nei pazienti k-ras wild-type B-RAF, P-TEN, PI3-PK sono target in corso di valutazione Abs hanno attività come agenti singoli nei pazienti pretrattati indipendentemente dalla linea di trattamento Regimi tipo FOLFIRI+ Cetuximab aumentano il PFS e la OS in prima linea (CRYSTAL) Regimi tipo FOLFOX + Panitumumab aumentano il PFS in prima linea ma non OS (PRIME) I pazienti con metastasi epatiche sembrano essere quelli che traggono il maggior beneficio dagli ABs Regimi con Tripletta (5-FU/FA/CPT-11/OXA) + Cetuximab sembrano essere particolarmente promettenti come regime neoadiuvante nei pazienti candidati a resezione di metastasi epatiche
 possono essere usati solo nei pazienti k-ras wild-type. B-RAF, P-TEN, PI3-PK sono target in corso di valutazione. Abs hanno attività come agenti singoli nei pazienti pretrattati indipendentemente dalla linea di trattamento. Regimi tipo FOLFIRI+ Cetuximab aumentano il PFS e la OS in prima linea (CRYSTAL) Regimi tipo FOLFOX + Panitumumab aumentano il PFS in prima linea ma non OS (PRIME) I pazienti con metastasi epatiche sembrano essere quelli che traggono il maggior beneficio dagli ABs. Regimi con Tripletta (5-FU/FA/CPT-11/OXA) + Cetuximab sembrano essere particolarmente promettenti come regime neoadiuvante nei pazienti candidati a resezione di metastasi epatiche.")
38
Algoritmo Ideale di Trattamento CRC Avanzato nel 2009

39
Grazie per l’Attenzione

Presentazioni simili





>")














