Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Psicologia del funzionamento e della disabilità
4. La valutazione delle tecnologie assistive Prof. Stefano Federici – A.A

3
I Parte: Valutare I fattori personali
In the segment 3, I will present the professional functions of the psychologist in a center for technical aid. The main skills of the psychologist will be grouped into two psychological dimensions: expertise on personal factors and ability in the field of human relationships and communication.

4
Il Numero Uno dei sospettati nell’abbandono di TA: I fattori personali
Phillips & Zhao (1993) Predictors of Assistive Technology Abandonment Scherer et al (2005) Predictors of assistive technology use Dijcks et al (2006) Non-use of assistive technology Lauer et al (2006) Factors in Assistive Technology Device Abandonment Verza et al (2006) Evaluating the need for assistive technology reduces equipment abandonment Federici & Borsci (2011) The use and non-use of assistive technology For nearly two decades the scientific literature has given increasing attention to the issue of assistive technologies abandonment. The nature of the phenomenon is complex and this is one of the reasons why the abandonment has been frequently called in different ways: neglect, discard, discontinuity. Each of these terms reflects different ideas about the causes and the modalities of non-use of assistive technologies. However, a significant part of the literature on this topic identifies the lack of consideration given to personal factors as a major cause of abandonment. The early study of Philips and Zhao in 1993 found that three out of four factors significantly related to abandonment – lack of consideration of user opinion in selection, easy device procurement and change in user needs or priorities – were significantly related to personal factors. In the last 7 years, a growing number of scholars have turned their focus on the role of personal factors in the relationship between user and assistive technology. Despite of this, the most important international classification of functioning and disability, the ICF (WHO, 2001), grounded on the biopsychosocial model of disability, has never classified the personal factors.
 Predictors of Assistive Technology Abandonment. Scherer et al (2005) Predictors of assistive technology use. Dijcks et al (2006) Non-use of assistive technology. Lauer et al (2006) Factors in Assistive Technology Device Abandonment. Verza et al (2006) Evaluating the need for assistive technology reduces equipment abandonment. Federici & Borsci (2011) The use and non-use of assistive technology. For nearly two decades the scientific literature has given increasing attention to the issue of assistive technologies abandonment. The nature of the phenomenon is complex and this is one of the reasons why the abandonment has been frequently called in different ways: neglect, discard, discontinuity. Each of these terms reflects different ideas about the causes and the modalities of non-use of assistive technologies. However, a significant part of the literature on this topic identifies the lack of consideration given to personal factors as a major cause of abandonment. The early study of Philips and Zhao in 1993 found that three out of four factors significantly related to abandonment – lack of consideration of user opinion in selection, easy device procurement and change in user needs or priorities – were significantly related to personal factors. In the last 7 years, a growing number of scholars have turned their focus on the role of personal factors in the relationship between user and assistive technology. Despite of this, the most important international classification of functioning and disability, the ICF (WHO, 2001), grounded on the biopsychosocial model of disability, has never classified the personal factors.")
5
Cosa sono i fattori personali
genere razza età forma fisica ... … … … ? coping auto-stima Cosa sono i fattori personali ICF – modello biopsicosociale Condizione di Salute (disturbo o malattia) Funzioni e strutture corporee Attività Partecipazione Fattori ambientali Fattori personali The second part of the ICF covers “contextual factors”, divided into two components: environmental factors and personal factors. After more than ten years, the personal factors are not yet coded in the ICF classification, although they are heavily involved in the process of functioning and disability. Personal factors are defined in the ICF as “the particular background of an individual’s life and living and comprise features of the individual that are not part of a health condition or health states” (WHO, 2001, p. 23). [click] They include gender, race, age, other health conditions, fitness, lifestyle, habits, upbringing, coping styles, social background, education, profession, past and current experience, overall behaviour pattern and character style, individual psychological assets and other characteristics, all or any of which may play a role in disability at any level. They also include psychological, emotional and behavioral aspects, such as attribution styles, self-efficacy, self-esteem, emotion, motivation and problem-behaviors. As stated by Ueda and Okawa in 2003, personal factors belong to the objective dimension of functioning. One of the most relevant categorizations focuses on which personal factors are changeable and which are not. This distinction plays a central role since that the team of the centre for technical aid operates not only to turn environmental barriers into facilitators but also to motivate the user/client to do the same on his or her adjustable individual resources.
 Funzioni e strutture corporee. Attività. Partecipazione. Fattori ambientali. Fattori personali. The second part of the ICF covers contextual factors , divided into two components: environmental factors and personal factors. After more than ten years, the personal factors are not yet coded in the ICF classification, although they are heavily involved in the process of functioning and disability. Personal factors are defined in the ICF as the particular background of an individual’s life and living and comprise features of the individual that are not part of a health condition or health states (WHO, 2001, p. 23). [click] They include gender, race, age, other health conditions, fitness, lifestyle, habits, upbringing, coping styles, social background, education, profession, past and current experience, overall behaviour pattern and character style, individual psychological assets and other characteristics, all or any of which may play a role in disability at any level. They also include psychological, emotional and behavioral aspects, such as attribution styles, self-efficacy, self-esteem, emotion, motivation and problem-behaviors. As stated by Ueda and Okawa in 2003, personal factors belong to the objective dimension of functioning. One of the most relevant categorizations focuses on which personal factors are changeable and which are not. This distinction plays a central role since that the team of the centre for technical aid operates not only to turn environmental barriers into facilitators but also to motivate the user/client to do the same on his or her adjustable individual resources.")
6
Perché l’assistenza protesica è un processo costoso
Una riabilitazione tecnologica olistica affronta diverse variabili Una efficace riabilitazione tecnologica è un processo costoso La riabilitazione tecnologica standard trascura i fattori personali Perché l’assistenza protesica è un processo costoso La variabilità è un ostacolo perché è un costo The ICF imputes the lack of codes for the personal factors to “the large social and cultural variance associated with them.” (WHO, 2001, p. 9) We believe that the extreme variability of personal factors is certainly expensive. [click] Similarly, we know that any truly user-centered process of rehabilitation, that adopt a holistic perspective about the user, is equally expensive. But we also know that every path for an effective rehabilitation is necessarily expensive. A short term business approach to rehabilitation has led to neglect the role of personal factors due to the ignorance on their relevance for a successful outcome and for reducing economic waste. The justification of the ICF regarding the extreme variability of personal factors, therefore, is very weak. We believe that the real reason for non-coding consists in the necessity to do not introduce in the rehabilitation process too holistic variables on behalf of standardization and objectivity.
 We believe that the extreme variability of personal factors is certainly expensive. [click] Similarly, we know that any truly user-centered process of rehabilitation, that adopt a holistic perspective about the user, is equally expensive. But we also know that every path for an effective rehabilitation is necessarily expensive. A short term business approach to rehabilitation has led to neglect the role of personal factors due to the ignorance on their relevance for a successful outcome and for reducing economic waste. The justification of the ICF regarding the extreme variability of personal factors, therefore, is very weak. We believe that the real reason for non-coding consists in the necessity to do not introduce in the rehabilitation process too holistic variables on behalf of standardization and objectivity.")
7
Fattori personali e l’abbandono di TA
Abbandono nei Paesi Occidentali Il 33% degli ausili viene completamente abbandonato già nel 1° anno di utilizzo o nei primi 5 anni. 4 principali cause Cambiamento nei bisogni dell’utente; Facilità nel reperimento e nell’ottenimento della tecnologia; Basse prestazioni dell’ausilio; Mancanza di considerazione dell’opinione dell’utente. Abbandono in Italia Non abbiamo dati ufficiali né regionali né nazionali. Forse un 37% ( Un solo studio, non pubblicato e di cui non sono disponibili né dati né le procedure utilizzate per reperirli, relativo all’abbandono di ausili nella Regione Piemonte del 2001, accessibile in Internet al link riporta una percentuale di abbandono degli ausili pari al 37%.

8
Progetto MAP 2009-2010 Numero di persone intervistate
Punteggio globale servizio Punteggio globale soddisfazione Abbandono Ragioni dell’abbandono

9
L’abbandono delle tecnologie assistive in Umbria
24,34% Abbandono utenti non-in-riabilitazione Abbandono utenti in riabilitazione 12,61% L’abbandono stimato su 221 soggetti intervistati era pari a 19,10%. Tuttavia, la stima finale sull’abbandono in Umbria, riportata dal progetto MAP, è pari al 18,70%. Tale percentuale è stata ottenuta attraverso una tecnica predittiva Bootstrap su una campione simulato di utenti. Δ = 11,73% Tempo di abbandono: 1-3 anni dalla fornitura Dato reale su 221/287 utenti 19,10% Dato stimato su utenti 18,70%

10
Ritorno dell’investimento (ROI) valutando i fattori personali
Assistenza Protesica Regione Umbria Spesa protesica 2009 = € ,31 Spesa protesica = € ,93 Dispersione economica Dispersione economica 2009 ROI valutando i fattori personali nella Regione Umbria = € (annui) Popolazione Umbra = 908,000 But what is the cost of standardization and how much is the economic waste due to neglect personal factors? A research, carried out between November 2010 and January 2011 in the Umbria Italian region, has shown that in a year, the economic loss due to mismatches between users and technologies is around 1.5 million euros and that this loss amounts to about 4.5 million euros in three years. [click] Data clearly show that the users’ satisfaction of AT and of service providers are strongly correlated to the AT non-use, by suggesting that just a user-driven process of AT assignation process, centered on the user-patient needs and expectations might reasonably prevent the AT non-use and abandonment. The 18% of AT mean of non-use, estimated in this survey, is slightly lower compared to the range of percentages usually reported by international studies, that is rated from 29% to 33%. Nevertheless, the appraisal of the Italian National Health System’s economic loss for AT abandonment remains high. Data shows a strong correlation (p<.001) between AT non-use and the AT users/patients’ dissatisfaction reasons – adjustments and personalization, safety, and comfort. All these variables are codifiable as belonging to personal factors. We can conclude that the return on investment on personal factors in AT assignment in Umbria Region might amount to 2 million dollars.
 Popolazione Umbra = 908,000. But what is the cost of standardization and how much is the economic waste due to neglect personal factors A research, carried out between November 2010 and January 2011 in the Umbria Italian region, has shown that in a year, the economic loss due to mismatches between users and technologies is around 1.5 million euros and that this loss amounts to about 4.5 million euros in three years. [click] Data clearly show that the users’ satisfaction of AT and of service providers are strongly correlated to the AT non-use, by suggesting that just a user-driven process of AT assignation process, centered on the user-patient needs and expectations might reasonably prevent the AT non-use and abandonment. The 18% of AT mean of non-use, estimated in this survey, is slightly lower compared to the range of percentages usually reported by international studies, that is rated from 29% to 33%. Nevertheless, the appraisal of the Italian National Health System’s economic loss for AT abandonment remains high. Data shows a strong correlation (p<.001) between AT non-use and the AT users/patients’ dissatisfaction reasons – adjustments and personalization, safety, and comfort. All these variables are codifiable as belonging to personal factors. We can conclude that the return on investment on personal factors in AT assignment in Umbria Region might amount to 2 million dollars.")
11
Come investire nei fattori personali
Macrolivello OMS Sviluppare le categorie dei fattori personali all’interno dell’ICF Microlivello Assumere gli psicologi come esperti in fattori personali Meloni, F., Federici, S., Stella, A., Mazzeschi, C., Cordella, B., Greco, F., et al. (2012). The Psychologist. In S. Federici & M. J. Scherer (Eds.), Assistive Technology Assessment Handbook (pp ). Boca Raton, FL, US: CRC Press. Psicologo in un centro di valutazione di TA (ausilioteche, centri ausili ASL) una valutazione psicologica appropriata o un intervento clinico specifico con l’utente o con il suo contesto umano nel corso di tutto il processo di assegnazione di TA. We believe that to invest in personal factors represents an important turning point for a successful matching between person and technology. Giving the importance to personal factors would help to dramatically reduce the abandonment rate of technologies by users. The steps needed to facilitate this investment are, according to our opinion, at least two: WHO should immediately provide for the encoding of personal factors in the International Classification of Functioning, Disability and Health. The psychological variables comprised in the ICF’s personal factors can make substantial differences to the rehabilitation process and, particularly, they play a central role for a service delivery provision. The centers for technical aid should employ more psychologists as skilled professionals in the personal factors. It is reasonable to assume that the lack of importance given to the “systemic” skills of the psychologist in the process of matching the person with technology is largely due to the personal factors non-coding in the ICF. [click] Out of all the professionals comprising the multidisciplinary team, the psychologist is the one who, in terms of curriculum and training, is the greatest expert in personal factors as they are conceptualized by ICF. In an AT service delivery process, psychologist provides an appropriate psychological evaluation and a precise clinical intervention with the user/client and/or their significant human context over the course of the whole AT assignment process.
. The Psychologist. In S. Federici & M. J. Scherer (Eds.), Assistive Technology Assessment Handbook (pp ). Boca Raton, FL, US: CRC Press. Psicologo. in un centro di valutazione di TA (ausilioteche, centri ausili ASL) una valutazione psicologica appropriata o un intervento clinico specifico con l’utente o con il suo contesto umano nel corso di tutto il processo di assegnazione di TA. We believe that to invest in personal factors represents an important turning point for a successful matching between person and technology. Giving the importance to personal factors would help to dramatically reduce the abandonment rate of technologies by users. The steps needed to facilitate this investment are, according to our opinion, at least two: WHO should immediately provide for the encoding of personal factors in the International Classification of Functioning, Disability and Health. The psychological variables comprised in the ICF’s personal factors can make substantial differences to the rehabilitation process and, particularly, they play a central role for a service delivery provision. The centers for technical aid should employ more psychologists as skilled professionals in the personal factors. It is reasonable to assume that the lack of importance given to the systemic skills of the psychologist in the process of matching the person with technology is largely due to the personal factors non-coding in the ICF. [click] Out of all the professionals comprising the multidisciplinary team, the psychologist is the one who, in terms of curriculum and training, is the greatest expert in personal factors as they are conceptualized by ICF. In an AT service delivery process, psychologist provides an appropriate psychological evaluation and a precise clinical intervention with the user/client and/or their significant human context over the course of the whole AT assignment process.")
12
Cosa fa lo psicologo in un’ausilioteca
Identificare i fattori personali dell’utente, le priorità, le preferenze, ecc.; Sostenere la richiesta dell’utente; Mediare tra gli utenti che ricercano una soluzione e il team multidisciplinare di un centro ausili; Facilitare i rapporti tra i membri del team multidisciplinare; Riformulare le relazioni tra l’utente e la sua famiglia, nel quadro delle nuove sfide, limitazioni e restrizioni che si trovano ad affrontare. The international scientific literature has never given a clear definition of the role and competencies of the psychologist in the rehabilitation field. In the ATA process the psychologist’s role and the professional skills of psychologists consist of: identify the user’s personal factors, priorities, preferences, etc.; advocating the user’s request in the user-driven process through which the selection of one or more technological aids for an assistive solution is reached; acting as mediator between users seeking solutions and the multidisciplinary team of a centre for technical aid; team facilitating among members of the multidisciplinary team, and finally; reframing the relationship between the client and his or her family within the framework of the new challenges and limitations and restrictions they face.

13
The role of the psychologist in the ATA process
Multidisciplinary team meeting for: - user data valuation and - setting design START Center for Technical Aid Contact User data collection Setting set-up Matching process: - assistive solution proposal - assistive solution user-trial - assistive solution outcome Assistive solution Multidisciplinary team evaluation User Support Follow up NOT User agreement Assistive Technology Provision User/client REQUEST User Actions Request to solve activity limitations Request to solve environmental restrictions Providing history (medical, rehabilitation, support use) and psycho-socio- environmental data User subjective evaluation of technological aids User evaluation of assistive solution Short/Long-term use Effectiveness Efficiency Usability Personal, emotional, social, comfort with use Subjective well-being -Benefit Assistive Technology obtained: public health system or public/private insurance Psychologist’s role ADVOCATE IDENTIFY FACILITATE TEAM The role of the psychologist in the ATA process Identify Advocate Mediate Facilitate Reframe MEDIATE Let me show you in details what the psychologist should do within an Assistive Technology Assessment process. The psychologist should identify. During the user data collection step, the psychologist analyzes the clinical and psychosocial data in order to identify the greatest number of personal factors that are relevant in matching the user with technology. In addition, the psychologist will identify user’s preferences and priorities in relation to the objective to be achieved through assistive solution. [click] The psychologist should advocate. During the multidisciplinary meeting, the clinical psychologist’s tasks is to emphasize the unique and peculiar aspects of the case represented by the user/client in terms of personal factors and of his or her human and relational context of life. During the multidisciplinary team evaluation, the psychologist advocates the user/client’s request guaranteeing a user-driven assignation process through which the selection of one or more technological aids for an assistive solution is reached. Active listening, empathy, ability to reformulate in a shared language the user/client requirements are the main instruments employed by the clinical psychologist in this step. Advocating user’s requests is a psychologist’s task also in the follow up step. The psychologist should mediate. As Brown and Gordon (2004, p. S13) claim: “Measurement and assessment, occurring within both research and clinical service contexts, typically involve an imbalance of power between professionals and persons with disabilities. Power is evidenced in who controls decisions about measurement and whose perspective—the subjective values of the measured person or the objective or normative values of the measurer—is given primacy”. An assistive technology assessment process could amplify the relationship’s imbalance, since the presence of a multidisciplinary team, in which each professional carries out his or her values and preferences, might exponentially tend to disempower the disabled person’s point of view. Consequently, the psychologist should mediate between user seeking solution and the multidisciplinary team during the multidisciplinary team meeting and the assistive solution multidisciplinary team evaluation. The psychologist should facilitate. As an expert in human relationships, the psychologist plays a key role in making easier connections between the different perspectives of the team professionals. The psychologist should reframe. Families and caregivers also have expectations about AT assignment, overestimating or underestimating the outcomes, which will condition their relationship with the disabled user and the professionals. In fact relatives’ representations of disability can help or limit the disabled person’s independence, influencing their expectations of his or her abilities. During the user agreement step and the support and follow up phases the psychologist might help the family and/or caregivers to reframe their relationship with the user. REFRAME
 and psycho-socio- environmental data. User subjective evaluation of technological aids. User evaluation of assistive solution. Short/Long-term use. Effectiveness. Efficiency. Usability. Personal, emotional, social, comfort with use. Subjective well-being. -Benefit. Assistive Technology obtained: public health system or public/private insurance. Psychologist’s role. ADVOCATE. IDENTIFY. FACILITATE. TEAM. The role of the psychologist in the ATA process. Identify Advocate Mediate Facilitate Reframe MEDIATE. Let me show you in details what the psychologist should do within an Assistive Technology Assessment process. The psychologist should identify. During the user data collection step, the psychologist analyzes the clinical and psychosocial data in order to identify the greatest number of personal factors that are relevant in matching the user with technology. In addition, the psychologist will identify user’s preferences and priorities in relation to the objective to be achieved through assistive solution. [click] The psychologist should advocate. During the multidisciplinary meeting, the clinical psychologist’s tasks is to emphasize the unique and peculiar aspects of the case represented by the user/client in terms of personal factors and of his or her human and relational context of life. During the multidisciplinary team evaluation, the psychologist advocates the user/client’s request guaranteeing a user-driven assignation process through which the selection of one or more technological aids for an assistive solution is reached. Active listening, empathy, ability to reformulate in a shared language the user/client requirements are the main instruments employed by the clinical psychologist in this step. Advocating user’s requests is a psychologist’s task also in the follow up step. The psychologist should mediate. As Brown and Gordon (2004, p. S13) claim: Measurement and assessment, occurring within both research and clinical service contexts, typically involve an imbalance of power between professionals and persons with disabilities. Power is evidenced in who controls decisions about measurement and whose perspective—the subjective values of the measured person or the objective or normative values of the measurer—is given primacy . An assistive technology assessment process could amplify the relationship’s imbalance, since the presence of a multidisciplinary team, in which each professional carries out his or her values and preferences, might exponentially tend to disempower the disabled person’s point of view. Consequently, the psychologist should mediate between user seeking solution and the multidisciplinary team during the multidisciplinary team meeting and the assistive solution multidisciplinary team evaluation. The psychologist should facilitate. As an expert in human relationships, the psychologist plays a key role in making easier connections between the different perspectives of the team professionals. The psychologist should reframe. Families and caregivers also have expectations about AT assignment, overestimating or underestimating the outcomes, which will condition their relationship with the disabled user and the professionals. In fact relatives’ representations of disability can help or limit the disabled person’s independence, influencing their expectations of his or her abilities. During the user agreement step and the support and follow up phases the psychologist might help the family and/or caregivers to reframe their relationship with the user. REFRAME.")
14
II Parte: modellizzare un processo di valutazione delle tecnologie assistive
In this first segment I will include a presentation of a new ideal Assistive Technology Assessment process based on the biopsychosocial model of disability and used in a center for assistive technology provision.

15
Modelli di assegnazione ausili nei Paesi Occidentali
Assistenza Sanitaria Pubblica La maggior parte dei paesi europei (p.e. Italia) Assistenza Sanitaria Privata Diversi paesi anglosassoni (p.e. USA) 2 Modelli Utenti di servizi di valutazione ausili non commerciali (ad esempio le Ausilioteche in Italia) Clienti di fornitura commerciale di TA (p.e. Centri per le Tecnologie Assistive negli USA) Pazienti di centri medici di tecnologie per la riabilitazione (p.e. Dep. of Physical Medicine & Rehabilitation of University of Rochester) Destinatari Gratuiti In sistemi di assistenza sanitaria pubblica A pagamento In sistemi di assistenza sanitaria privata Prodotti Assistenza Sanitaria Pubblica Assistenza Sanitaria Privata a pagamento gratuito utente paziente cliente Modelli Destinatari Pagamento Modelling an ideal model of effective Assistive Technology Assessment process of a center for AT provision is difficult if one takes into account the extraordinary variety of systems of regional and national health and social care, both public and private in Western countries. Just to synthesize, in a schematic way, some of these differences, we have divided in 2 models the main national health systems in the Western countries: the Public and the Private health systems. According to each national health system model, the recipient of the health system can be characterized as a user of noncommercial AT service delivery, or a client of commercial provision of AT, or a patient of a medical center for technical aid. Finally, according to each national health system model, the AT will be free of charge in a public health system or by paying in a private health system. [click] This other diagram displays better as the elements of each model are often mixed rather than juxtaposed. For example, the recipient of an AT in medical center for AT could be a patient both in Private and in Public Health Systems.
 Assistenza Sanitaria Privata. Diversi paesi anglosassoni (p.e. USA) 2 Modelli. Utenti di servizi di valutazione ausili non commerciali (ad esempio le Ausilioteche in Italia) Clienti di fornitura commerciale di TA (p.e. Centri per le Tecnologie Assistive negli USA) Pazienti di centri medici di tecnologie per la riabilitazione (p.e. Dep. of Physical Medicine & Rehabilitation of University of Rochester) Destinatari. Gratuiti. In sistemi di assistenza sanitaria pubblica. A pagamento. In sistemi di assistenza sanitaria privata. Prodotti. Assistenza Sanitaria Pubblica. Assistenza. Sanitaria Privata. a pagamento. gratuito. utente. paziente. cliente. Modelli Destinatari Pagamento Modelling an ideal model of effective Assistive Technology Assessment process of a center for AT provision is difficult if one takes into account the extraordinary variety of systems of regional and national health and social care, both public and private in Western countries. Just to synthesize, in a schematic way, some of these differences, we have divided in 2 models the main national health systems in the Western countries: the Public and the Private health systems. According to each national health system model, the recipient of the health system can be characterized as a user of noncommercial AT service delivery, or a client of commercial provision of AT, or a patient of a medical center for technical aid. Finally, according to each national health system model, the AT will be free of charge in a public health system or by paying in a private health system. [click] This other diagram displays better as the elements of each model are often mixed rather than juxtaposed. For example, the recipient of an AT in medical center for AT could be a patient both in Private and in Public Health Systems.")
16
ATA process 55 Studiosi dai 5 Continenti
Institute for Matching Person & Technology Ausiliteca di Roma, Leonarda Vaccari ATA process The assistive technology assessment process is not a result of a mere academic mental exercise, but provides examples of applications of it. The theoretical view of the ATA process emerges from experimental research applied to rehabilitation and assistive technologies; the international ideal model of assistive technology assessment process is already applied in centers for technical aid. Thanks to scientific and clinical collaboration, economic and operational support of the center for Technical Aid of Rome, Leonarda Vaccari Institute – which, in turn, is part of the Italian Network of centers Advice on Computer and Electronic Aids and cooperates with the Institute for Matching Person & technology. It was possible to define the assessment model proposed in the present workshop since the model is already operative in the center of Rome. This center offers a non-commercial advisory service and support on assistive technologies and computers for communication, learning, and autonomy. The service is free of charge for users who access it through the Italian National Health Service. Several scientific projects granted by the Institute are in progress at the center to verify not only the advantages of a systematic application of the Matching Person & Technology tools in the assessment process, but also the application of the ATA process model.

17
5 pilastri del modello dell’ATA process
5. Il ruolo dello psicologo 4. Lo psicotecnologo 3. La definizione di soluzione assistive (AAATE – ’03) 2. Il modello MPT 1. Il modello biopsicosociale dell’ICF The ATA process model is built on five pillars of the disability study and rehabilitation research: The ICF: International Classification of Functioning, Disability and Health biopsychosocial model [4]. Activities and social participation are strictly related to the body functions and structures, so that the individual’s functioning is the outcome of a triadic reciprocal relationship among health condition, environmental factors, and personal factors. According to this outlook of human functioning, the ATA process models service delivery provision in such a way that all dimensions affecting the user’s functioning (health condition and contextual factors) must be evaluated when the analysis of the user’s request and the selection of the AT is carried out by a centre. These dimensions are also criteria to verify the success of a good assignment and AT solution. The MPT model [2, 3]. It contends that the characteristics of the person, milieu/environment, and technology should be considered as interacting when selecting the most appropriate AT solution for a particular person’s use. Moreover, the MPT model overcame the traditional one-way process from provider to consumer involving, for the first time, the user in AT selection. The ATA process borrows a user-driven and collaborative working methodology from the MPT model, fostering a continuous dialogue between user and professional or team of professionals to make manifest different perspectives of the person’s needs and appropriate supports. It models a user-driven process guaranteeing that any activity in AT service delivery centre must find a correspondence to a user action and vice-versa; The definition of an assistive solution stated by the AAATE (Association for the Advancement of Assistive Technology in Europe) from 2003 [5]. The solution for a user provided by an AT service delivery centre must “involve something more than just a device, it often requires a mix of mainstream and assistive technologies whose assembly is different from one individual and another, and from one context to another. We may label it assistive solution” [5]. The assistive solution is the goal of the entire ATA process that, hypothetically, might not require any technological aid, but, e.g., just changes to fit the environment or a blend of use of a device and personal assistance [6]. It is also crucial when pursuing the goal of the assistive solution that the user’s request is taken seriously, often having to explore the user’s request of just a device to capture the user’s real needs. For this reason, the ATA process to relaunch the figure of the psychologist as essential, a pillar of the model, will help guarantee a user-centered evaluation and empower users to make their own choices. The role of the psychotechnologist. The psychotechnologist [7-9] is an expert in both psychology and AT, in particular in Human-Computer Interaction (HCI) and human factors, and he or she analyses the relations emerging from the person-technology interaction by taking into account all the psychological and cognitive components, and the possibilities of adapting and designing systems and services in an adaptable and accessible manner. Because of the characteristics of his or her professional background and training, the psychotechnologist is an ideal professional to coordinate the ATA process in an AT service delivery centre. The role of the psychologist. Although the structure, level of intensity, and services available for rehabilitation vary widely from one area to another whether comparing facilities, cities, states, or countries, nevertheless, there is considerable cross-cultural consistency in the view of the composition of the rehabilitation team [10], from Singapore [11] to the USA [12] and Europe [13, 14]. In this framework the role of the psychologist and psychiatrist is well and universally recognized. The psychologist in an AT service delivery process provides an appropriate psychological evaluation or a precise clinical intervention with the users and/or their significant human context over the course of the whole AT assignment process. We believe that to invest in personal factors represents an important turning point for a successful match between person and technology. Assigning greater importance to personal factors would help dramatically to reduce the abandonment rate of technologies by users [3, 15-24]. ATA PROCESS
 2. Il modello MPT. 1. Il modello biopsicosociale dell’ICF. The ATA process model is built on five pillars of the disability study and rehabilitation research: The ICF: International Classification of Functioning, Disability and Health biopsychosocial model [4]. Activities and social participation are strictly related to the body functions and structures, so that the individual’s functioning is the outcome of a triadic reciprocal relationship among health condition, environmental factors, and personal factors. According to this outlook of human functioning, the ATA process models service delivery provision in such a way that all dimensions affecting the user’s functioning (health condition and contextual factors) must be evaluated when the analysis of the user’s request and the selection of the AT is carried out by a centre. These dimensions are also criteria to verify the success of a good assignment and AT solution. The MPT model [2, 3]. It contends that the characteristics of the person, milieu/environment, and technology should be considered as interacting when selecting the most appropriate AT solution for a particular person’s use. Moreover, the MPT model overcame the traditional one-way process from provider to consumer involving, for the first time, the user in AT selection. The ATA process borrows a user-driven and collaborative working methodology from the MPT model, fostering a continuous dialogue between user and professional or team of professionals to make manifest different perspectives of the person’s needs and appropriate supports. It models a user-driven process guaranteeing that any activity in AT service delivery centre must find a correspondence to a user action and vice-versa; The definition of an assistive solution stated by the AAATE (Association for the Advancement of Assistive Technology in Europe) from 2003 [5]. The solution for a user provided by an AT service delivery centre must involve something more than just a device, it often requires a mix of mainstream and assistive technologies whose assembly is different from one individual and another, and from one context to another. We may label it assistive solution [5]. The assistive solution is the goal of the entire ATA process that, hypothetically, might not require any technological aid, but, e.g., just changes to fit the environment or a blend of use of a device and personal assistance [6]. It is also crucial when pursuing the goal of the assistive solution that the user’s request is taken seriously, often having to explore the user’s request of just a device to capture the user’s real needs. For this reason, the ATA process to relaunch the figure of the psychologist as essential, a pillar of the model, will help guarantee a user-centered evaluation and empower users to make their own choices. The role of the psychotechnologist. The psychotechnologist [7-9] is an expert in both psychology and AT, in particular in Human-Computer Interaction (HCI) and human factors, and he or she analyses the relations emerging from the person-technology interaction by taking into account all the psychological and cognitive components, and the possibilities of adapting and designing systems and services in an adaptable and accessible manner. Because of the characteristics of his or her professional background and training, the psychotechnologist is an ideal professional to coordinate the ATA process in an AT service delivery centre. The role of the psychologist. Although the structure, level of intensity, and services available for rehabilitation vary widely from one area to another whether comparing facilities, cities, states, or countries, nevertheless, there is considerable cross-cultural consistency in the view of the composition of the rehabilitation team [10], from Singapore [11] to the USA [12] and Europe [13, 14]. In this framework the role of the psychologist and psychiatrist is well and universally recognized. The psychologist in an AT service delivery process provides an appropriate psychological evaluation or a precise clinical intervention with the users and/or their significant human context over the course of the whole AT assignment process. We believe that to invest in personal factors represents an important turning point for a successful match between person and technology. Assigning greater importance to personal factors would help dramatically to reduce the abandonment rate of technologies by users [3, 15-24]. ATA PROCESS.")
18
Lo Assistive Technology Assessment process
Utente/cliente RICHIESTA Azioni dell’utente Richiesta di risolvere limitazioni nell’attività Richiesta di risolvere restrizioni ambientali Fornire dati anamnestici (medici, riabilitazione, uso di supporti) e psico-socio- ambientali Valutazione soggettiva dell’utente degli ausili tecnologici Valutazione dell’utente della soluzione assistiva Utilizzo di breve o lungo periodo: Efficacia Efficienza Usabilità Personale, emotivo, sociale, comfort d’uso Benessere soggettivo Benefici NO Tecnologia assistiva ottenuta: sistema sanitario pubblico o pubblica/privata assicurazione USCITA temporanea o permanente AVVIO Azioni del centro ausili Contatto Raccolta dati utente Allestimento del setting Processo di abbinamento: - proposta della soluzione assistiva - prova utente della soluzione assistiva - esito della soluzione assistiva Valutazione del team multidisciplinare della soluzione assistiva Supporto all’utente Follow up NO Consenso dell’utente Fornitura della tecnologia assistiva USCITA Meeting del team multidisciplinare per: - valutare i dati utente e – creazione del setting Processo di valutazione ambientale (vedi il diagramma della valutazione dell’usabilità e dell’accessibilità) Fase 1: L’utente cerca una soluzione Fase 1: Raccolta dei dati dell’utente Lo Assistive Technology Assessment process Fase 2: Valutazione dei dati forniti dall’utente Fase 2: L’utente verifica la soluzione Fase 3: Processo di abbinamento The ATA process can be read both from the perspective of the user or from the perspective of the center for Technical Aid. [click] Since the ATA is a user-driven process any activity of the staff must to find a correspondence to a user action and vice-versa. The users’ actions of the ATA process can be grouped in three phases. Phase 1 The user seeks a solution for one or more own activity limitations or participation restrictions and seeks assistance from a center. Phase 2 [click] The user checks the solution. The user tries and checks one or more technological aids provided by the professionals in an suitable evaluation setting (Center, house, hospital, school, rehabilitation center, etc.) Phase 3 [click] The user adopts the solution after obtaining the technological aid(s) from the public health system or public/private insurance, receives training for the daily use of the AT and follow-up. The actions of the center can be grouped in four phases. When the user provides data to the center, data are collected and the case is opened and transmitted to the multidisciplinary team. The multidisciplinary team evaluates the data and user’s request and arranges a suitable setting for the matching assessment. The multidisciplinary team, along with the user, assesses the assistive solution proposed, tries the solution and gathers outcome data. The multidisciplinary team evaluates the outcome of the matching assessment, then proposes the assistive solution to the user. When the assistive solution proposed requires an environmental evaluation, the team initiates the Environmental Assessment Process that we will deepen in the segment 3 of this workshop. Phase 4 [click] When the technological aid is delivered to the user a follow-up and on-going user support is activated and the assistive solution is verified in the daily life context of the user. Fase 3: L’utente adotta la soluzione Fase 4: Fornitura della Tecnologia Assistiva e follow up della soluzione assistiva nel contesto d’uso
 e psico-socio- ambientali. Valutazione soggettiva dell’utente degli ausili tecnologici. Valutazione dell’utente della soluzione assistiva. Utilizzo di breve o lungo periodo: Efficacia. Efficienza. Usabilità. Personale, emotivo, sociale, comfort d’uso. Benessere soggettivo. Benefici. NO. Tecnologia assistiva ottenuta: sistema sanitario pubblico o pubblica/privata assicurazione. USCITA. temporanea o permanente. AVVIO. Azioni del centro ausili. Contatto. Raccolta dati utente. Allestimento del setting. Processo di abbinamento: - proposta della soluzione assistiva - prova utente della soluzione assistiva - esito della soluzione assistiva. Valutazione del team multidisciplinare della soluzione assistiva. Supporto all’utente. Follow up. NO. Consenso dell’utente. Fornitura della tecnologia assistiva. USCITA. Meeting del team multidisciplinare per: - valutare i dati utente e – creazione del setting. Processo di valutazione ambientale (vedi il diagramma della valutazione dell’usabilità e dell’accessibilità) Fase 1: L’utente cerca una soluzione. Fase 1: Raccolta dei dati dell’utente. Lo Assistive Technology Assessment process. Fase 2: Valutazione dei dati forniti dall’utente. Fase 2: L’utente verifica la soluzione. Fase 3: Processo di abbinamento. The ATA process can be read both from the perspective of the user or from the perspective of the center for Technical Aid. [click] Since the ATA is a user-driven process any activity of the staff must to find a correspondence to a user action and vice-versa. The users’ actions of the ATA process can be grouped in three phases. Phase 1 The user seeks a solution for one or more own activity limitations or participation restrictions and seeks assistance from a center. Phase 2 [click] The user checks the solution. The user tries and checks one or more technological aids provided by the professionals in an suitable evaluation setting (Center, house, hospital, school, rehabilitation center, etc.) Phase 3 [click] The user adopts the solution after obtaining the technological aid(s) from the public health system or public/private insurance, receives training for the daily use of the AT and follow-up. The actions of the center can be grouped in four phases. When the user provides data to the center, data are collected and the case is opened and transmitted to the multidisciplinary team. The multidisciplinary team evaluates the data and user’s request and arranges a suitable setting for the matching assessment. The multidisciplinary team, along with the user, assesses the assistive solution proposed, tries the solution and gathers outcome data. The multidisciplinary team evaluates the outcome of the matching assessment, then proposes the assistive solution to the user. When the assistive solution proposed requires an environmental evaluation, the team initiates the Environmental Assessment Process that we will deepen in the segment 3 of this workshop. Phase 4 [click] When the technological aid is delivered to the user a follow-up and on-going user support is activated and the assistive solution is verified in the daily life context of the user. Fase 3: L’utente adotta la soluzione. Fase 4: Fornitura della Tecnologia Assistiva. e follow up della soluzione assistiva. nel contesto d’uso.")
19
L’ATA process alla luce del modello biopsicosociale dell’ICF
Condizioni di salute (disturbo o malattia) Funzioni e Strutture corporee Attività Partecipazione Fattori ambientali Fattori personali Benessere MPT Diagnosi medica Processo condotto dall’utente Supporto e follow-up Soluzione Assistiva The ATA process is embedded in the ICF model and the process describes the complexity of the biopsychosocial model. The ATA process means to guide a multidisciplinary team to provide not just devices but much more: assistive solutions; in order to empower the user and improve the well-being. [click] Now, let me show you how the ICF model fits to the ATA process. The individual functioning and disability of the user are taken into account by the multidisciplinary team that evaluates health conditions of the user. The matching process then aims to support activity limitations and enhance individual functioning. Finally, overcoming a disablement may involve something more than just a device, it often requires a mix of mainstream and assistive technologies whose matching is different from one individual and another, and from one context to another. Therefore, the multidisciplinary team has to take in a serious account the participation restrictions. ICF – modello biopsicosociale
 Funzioni e Strutture corporee. Attività. Partecipazione. Fattori ambientali. Fattori personali. Benessere. MPT. Diagnosi medica. Processo condotto dall’utente. Supporto e follow-up. Soluzione Assistiva. The ATA process is embedded in the ICF model and the process describes the complexity of the biopsychosocial model. The ATA process means to guide a multidisciplinary team to provide not just devices but much more: assistive solutions; in order to empower the user and improve the well-being. [click] Now, let me show you how the ICF model fits to the ATA process. The individual functioning and disability of the user are taken into account by the multidisciplinary team that evaluates health conditions of the user. The matching process then aims to support activity limitations and enhance individual functioning. Finally, overcoming a disablement may involve something more than just a device, it often requires a mix of mainstream and assistive technologies whose matching is different from one individual and another, and from one context to another. Therefore, the multidisciplinary team has to take in a serious account the participation restrictions. ICF – modello biopsicosociale.")
20
Limiti e vantaggi di un modello ideale di ATA process
La difficoltà di definire un unico AT system delivery La straordinaria varietà di sistemi sanitari influenza in differenti modi le specifiche caratteristiche che delineano ogni singolo Centro. La comunità scientifica sta perseguendo un AT system delivery che sia sempre più individualizzato. Come si usa dire Centrato sulla persona. Vantaggi Emerge come una sintesi di esperienze di modelli regionali. Si condivide un modello teorico e criteri di valutazione. Permette di condividere dati essenziali alla ricerca scientifica. Aiuta a pianificare e valutare politiche nazionali e internazionali. Può aiutare a valutare la qualità dei servizi. This model, therefore, intends to express, in an idealized and essential form, an assessment process carried out in a center for assistive technology provision, since it provides such tools for assessment and the professional skill set that we define “psychotechnological.” However, one of the unsolved problems is the difficulty, already met several times, of defining the features of a center for technical aid. The modelling process of a center for technical aid is difficult if one takes into account the extraordinary variety of systems of regional and national health and social care, both public and private (Müller, 2012). Because of the difficulty of finding an adequate and effective synthesis of the various models proposed by specific national systems of public health and welfare, the scientific community is facing an assistive technology delivery system which will be increasingly individualized, due to the social and cultural diversity of users and the necessary adjustment of the center’s functioning to the local health system. However, it should be noted that this particularization of the model is to clash with some trends that are aimed at promoting, instead, globalization (for example, this occurs both in social and health policies of the European Community and in those of the World Health Organization). The internationalization of a model, indeed, is advantageous since it often emerges as a synthesis of experiences of regional models. Moreover, it offers the opportunity, by sharing a theoretical model and evaluation criteria, to share data essential to scientific research, planning, and evaluation of national and international policies and the verification of the quality of public services.
. Because of the difficulty of finding an adequate and effective synthesis of the various models proposed by specific national systems of public health and welfare, the scientific community is facing an assistive technology delivery system which will be increasingly individualized, due to the social and cultural diversity of users and the necessary adjustment of the center’s functioning to the local health system. However, it should be noted that this particularization of the model is to clash with some trends that are aimed at promoting, instead, globalization (for example, this occurs both in social and health policies of the European Community and in those of the World Health Organization). The internationalization of a model, indeed, is advantageous since it often emerges as a synthesis of experiences of regional models. Moreover, it offers the opportunity, by sharing a theoretical model and evaluation criteria, to share data essential to scientific research, planning, and evaluation of national and international policies and the verification of the quality of public services.")
21
III Parte: Analisi di un caso
In this first segment I will include a presentation of a new ideal Assistive Technology Assessment process based on the biopsychosocial model of disability and used in a center for assistive technology provision.

22
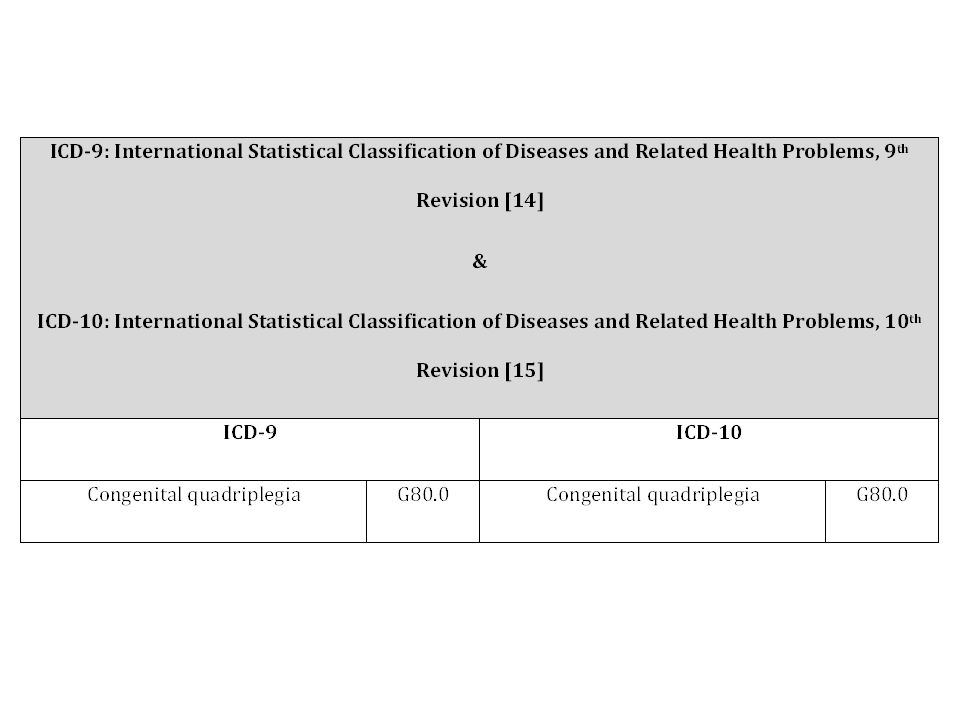
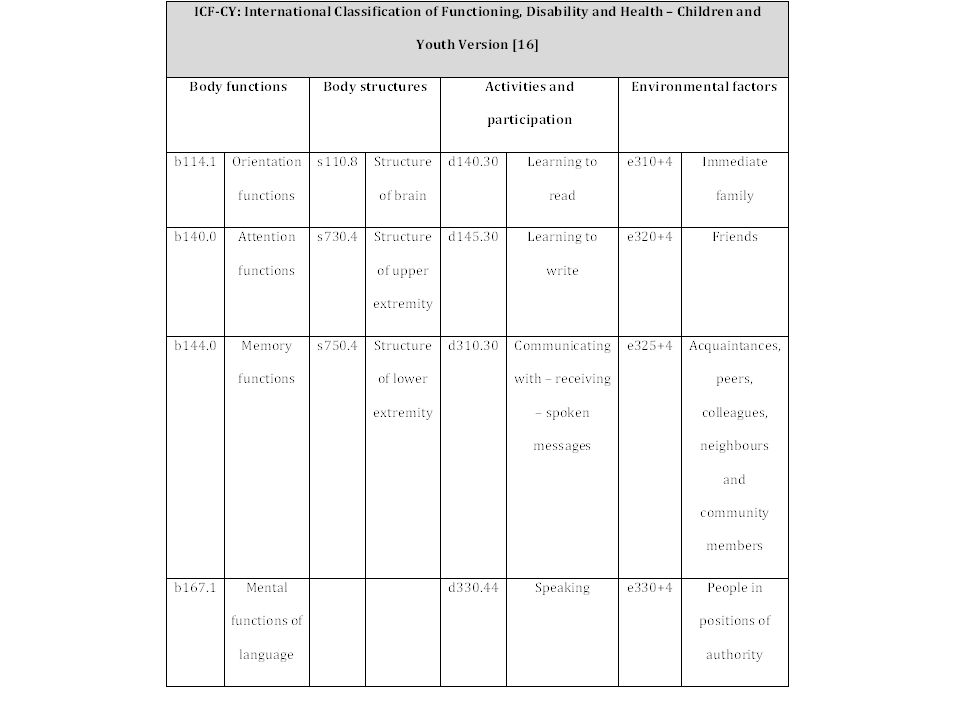
Arianna: diagnosi La diagnosi di Arianna
6,5 anni, grave tetraparesi spastica con una componente distonica come esito di una paralisi cerebrale neonatale. Le funzioni visive e percettive buone. Sono stati utilizzati i Lea Test della Hyvärinen. Buona acuità visiva (OD = 910/10 Dip.; OS = 10/10 D.; OU = 11/10 Dip.) e un normale senso del colore, sensibilità al contrasto e del campo visivo. Buona percezione e localizzazione di oggetti a una distanza sia prossimale sia distale, con una buona capacità di fissazione e tracciamento. --> La paralisi cerebrale infantile rappresenta l'esito di una lesione del sistema nervoso centrale che abbia comportato una perdita più o meno estesa di tessuto cerebrale. Le manifestazioni della lesione sono caratterizzate prevalentemente, ma non esclusivamente, da un'alterazione delle funzioni motorie. L'evento lesivo può aver avuto origine in epoca prenatale, perinatale o postnatale, ma in ogni caso entro i primi tre anni di vita del bambino, periodo di tempo in cui vengono completate le principali fasi di crescita e sviluppo della funzione cerebrale nell'essere umano. Il disturbo è definito come persistente, in quanto la lesione a carico del cervello non è suscettibile di "guarigione" in senso stretto, ma la patologia non tende al peggioramento spontaneo perché la lesione stessa, sostituita da tessuto cicatriziale, non va incontro a fenomeni degenerativi. Le manifestazioni della malattia, comunque, non sono fisse, perché i sintomi mutano nel corso del tempo, e possono beneficiare di un trattamento di tipo riabilitativo o, nei casi più gravi, anche chirurgico (v. chirurgia funzionale). Classificazione in base alla sede del disturbo motorio (classificazione topografica) Tetraplegia (disturbo del controllo motorio del tronco e dei quattro arti) Emiplegia (disturbo del controllo motorio di un emilato, ovvero del lato sinistro o del lato destro del corpo) Diplegia (disturbo del controllo motorio di due arti, ma prevalente degli arti inferiori) Il termine paraplegia, talvolta erroneamente utilizzato al posto di quello di diplegia, non indica un tipo di paralisi cerebrale infantile, ma un disturbo del controllo motorio degli arti inferiori causato da lesione del midollo spinale. La triplegia (disturbo del controllo motorio di tre arti) e la monoplegia (disturbo del controllo motorio di un solo arto) rappresentano forme lievi, rispettivamente, di diplegia e di emiplegia[2]. Classificazione in base alle caratteristiche del movimento (classificazione motoria) Forme spastiche: aumento costante del tono in alcuni gruppi muscolari e dei riflessi da stiramento. Sono presenti alcuni atteggiamenti posturali tipici (arto superiore addotto e intra-ruotato, gomito, polso e dita flessi, piede equino.) Forme ipotoniche: diminuzione costante del tono di alcuni gruppi muscolari. Noto anche col nome di "bambino floppy". Forme atassiche: disturbi della coordinazione e dell'equilibrio, con frequente presenza di ipotono dei muscoli distali. Forme discinetiche o distoniche: fluttuazione continua del tono muscolare, e presenza di movimenti parassiti influenzabili dalle emozioni e dalla fatica, ma che scompaiono nel sonno. Forme miste: sintomatologia combinata di due o più forme. Hyvärinen, L., & Jacob, N. (2011). What and How Does This Child See?: Assessment of Visual Functioning for Development and Learning. Moscow, RU: Vistest.
 e un normale senso del colore, sensibilità al contrasto e del campo visivo. Buona percezione e localizzazione di oggetti a una distanza sia prossimale sia distale, con una buona capacità di fissazione e tracciamento. --> La paralisi cerebrale infantile rappresenta l esito di una lesione del sistema nervoso centrale che abbia comportato una perdita più o meno estesa di tessuto cerebrale. Le manifestazioni della lesione sono caratterizzate prevalentemente, ma non esclusivamente, da un alterazione delle funzioni motorie. L evento lesivo può aver avuto origine in epoca prenatale, perinatale o postnatale, ma in ogni caso entro i primi tre anni di vita del bambino, periodo di tempo in cui vengono completate le principali fasi di crescita e sviluppo della funzione cerebrale nell essere umano. Il disturbo è definito come persistente, in quanto la lesione a carico del cervello non è suscettibile di guarigione in senso stretto, ma la patologia non tende al peggioramento spontaneo perché la lesione stessa, sostituita da tessuto cicatriziale, non va incontro a fenomeni degenerativi. Le manifestazioni della malattia, comunque, non sono fisse, perché i sintomi mutano nel corso del tempo, e possono beneficiare di un trattamento di tipo riabilitativo o, nei casi più gravi, anche chirurgico (v. chirurgia funzionale). Classificazione in base alla sede del disturbo motorio (classificazione topografica) Tetraplegia (disturbo del controllo motorio del tronco e dei quattro arti) Emiplegia (disturbo del controllo motorio di un emilato, ovvero del lato sinistro o del lato destro del corpo) Diplegia (disturbo del controllo motorio di due arti, ma prevalente degli arti inferiori) Il termine paraplegia, talvolta erroneamente utilizzato al posto di quello di diplegia, non indica un tipo di paralisi cerebrale infantile, ma un disturbo del controllo motorio degli arti inferiori causato da lesione del midollo spinale. La triplegia (disturbo del controllo motorio di tre arti) e la monoplegia (disturbo del controllo motorio di un solo arto) rappresentano forme lievi, rispettivamente, di diplegia e di emiplegia[2]. Classificazione in base alle caratteristiche del movimento (classificazione motoria) Forme spastiche: aumento costante del tono in alcuni gruppi muscolari e dei riflessi da stiramento. Sono presenti alcuni atteggiamenti posturali tipici (arto superiore addotto e intra-ruotato, gomito, polso e dita flessi, piede equino.) Forme ipotoniche: diminuzione costante del tono di alcuni gruppi muscolari. Noto anche col nome di bambino floppy . Forme atassiche: disturbi della coordinazione e dell equilibrio, con frequente presenza di ipotono dei muscoli distali. Forme discinetiche o distoniche: fluttuazione continua del tono muscolare, e presenza di movimenti parassiti influenzabili dalle emozioni e dalla fatica, ma che scompaiono nel sonno. Forme miste: sintomatologia combinata di due o più forme. Hyvärinen, L., & Jacob, N. (2011). What and How Does This Child See : Assessment of Visual Functioning for Development and Learning. Moscow, RU: Vistest.")
23
LEA Test di Lea Hyvärinen
Lea test è una serie di prove di visione pediatrici progettato specificamente per i bambini che non sanno leggere le lettere dell’alfabeto. Possono essere utilizzati per valutare le capacità visive di da vicino e a distanza, così come la sensibilità al contrasto, al campo visivo, ai colori, la percezione del movimento. Hyvärinen, L., & Jacob, N. (2011). What and How Does This Child See?: Assessment of Visual Functioning for Development and Learning. Moscow, RU: Vistest.
. What and How Does This Child See : Assessment of Visual Functioning for Development and Learning. Moscow, RU: Vistest.")
24
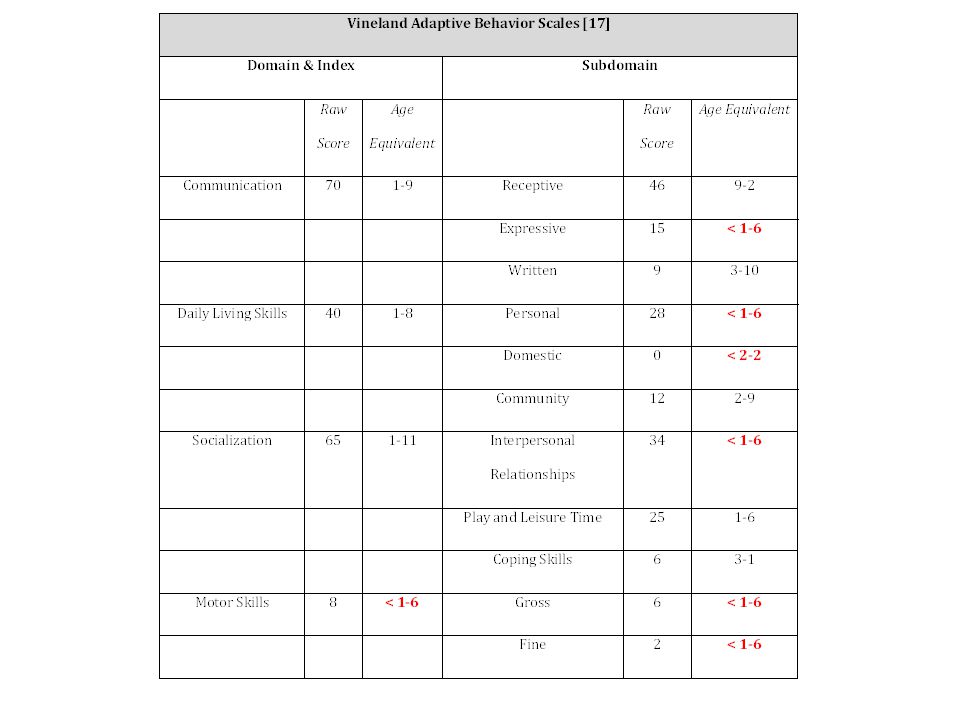
Arianna: funzionamento
Il comportamento di Arianna Difficoltà a separarsi dalla madre. Ottime risorse cognitive, molto comunicativa e partecipativa. Usava una ACC in modo adeguato e appropriato, sia in risposta a una richiesta che dichiarativa. Buona comunicazione di stati d’animo molto complessi con un sorriso motivato e contestuale, rispondendo alle domande chiuse “sì” con anti-flessione della testa e del “no” con leggeri movimenti laterali della testa. Mostrava di capire ogni richiesta, in modo che l’operatore poteva sempre spiegarle quello che avrebbe fatto e chiederle che cosa preferiva. Interessata a oggetti che le sono stati presentati e che ha tentato in tutti i modi di raggiungere e afferrare, non riuscendovi a causa della presenza di una significativa distonia. Si muoveva volontariamente all’interno della stanza con una sedia a rotelle motorizzata.

28
Azioni del centro ausili
E-Tran. Schede di comunicazione. Sistema di scansione Clicker. Sistema posturale. E-Tran non usato perché a bassa tecnologia. Schede di comunicazione non usate autonomamente. Riproposta dell’E-Tran. Clicker configurato in modalità manuale. E-Tran usato molto efficacemente. Schede di comunicazione non più pratiche. Sistema di Eye tracking. TA di supporto allo studio. TA per la comunicazione. 1° ciclo 2° ciclo 3° ciclo A B C E F D AVVIO Azioni del centro ausili Contatto Raccolta dati utente Allestimento del setting Processo di abbinamento: - proposta della soluzione assistiva - prova utente della soluzione assistiva - esito della soluzione assistiva Valutazione del team multidisciplinare della soluzione assistiva Supporto all’utente Follow up Consenso dell’utente Fornitura della tecnologia assistiva Meeting del team multidisciplinare per: - valutare i dati utente e – creazione del setting Figure 7. ATA process cycles. The flow chart shows the three cycles of the ATA process for Arianna’s case. In the middle of the figure the AT Service Delivery process for each cycle is drawn. Each cycle has a duration of about 12 months. In step A of the first cycle, the two user’s requests are reported. In steps B, D and F the assistive solutions proposed by the multidisciplinary team in each cycle are summarized. Finally, in steps C and E the outcome of the follow-up regarding the first and second cycles are displayed.

29
Richiesta di Arianna La madre contattò l’Istituto Leonarda Vaccari nel 2008 per una valutazione di strategie tecnologiche che migliorassero la comunicazione di Arianna.

30
Composizione del meeting del teem multidisciplinare
ATA process – 1° ciclo: Meeting del teem multidisciplinare: composizione Composizione del meeting del teem multidisciplinare Psicotecnologo, psicologo, pediatra, neuropsicomotricista, terapista occupazionale, ortopedico, fisiatra, architetto e ingegnere.

31
Psicologo: relazione sui fattori di salute e personali
ATA process – 1° ciclo: Meeting del teem multidisciplinare: relazione dello psicologo sui fattori di salute e personali Psicologo: relazione sui fattori di salute e personali Arianna, 6,5 anni di età, frequenta la prima classe della scuola primaria, con un programma individualizzato. La sua prognosi è favorevole per quanto riguarda la lettura e la scrittura. Usa, quando richiesto, un libro con delle immagini per raccontare le sue esperienze. Chiaramente esprime “sì” e “no” con i movimenti della testa e degli occhi. Per comunicare, utilizza un codice di mimica facciale e sguardi condiviso dai caregiver, ma non comprensibile a persone non familiari. Intelligente, motivata, vivace, allegra, attenta e molto comunicativa.

32
Psicologo: relazione sui fattori ambientali
ATA process – 1° ciclo: Meeting del teem multidisciplinare: relazione dello psicologo sui fattori ambientali Psicologo: relazione sui fattori ambientali Usa AAC: quaderno ad anelli con le sue esperienze, figure, immagini e icone create dalla famiglia tramite Boardmaker. Per muoversi, utilizza una carrozzina elettrica con comando a joystick e un passeggino pediatrico posturale. L’MPT test for Child (MATCH) ha evidenziato una buona predisposizione all’uso di TA.
 ha evidenziato una buona predisposizione all’uso di TA.")
33
Psicotecnologo: Soluzioni per la comunicazione (AAC)
ATA process – 1° ciclo: Meeting del teem multidisciplinare: proposte di soluzioni dello psicotecnologo per la comunicazione Psicotecnologo: Soluzioni per la comunicazione (AAC) E-Tran Permette una rapida comunicazione con un facilitatore. Tale soluzione è stata proposta a causa dei movimenti involontari molto marcati che impediscono l’uso degli arti superiori in modo funzionale, ma con un controllo della testa sufficiente e una buona funzionalità visiva. Schede di comunicazione riorganizzate per temi, facilmente ricercabili, e integrate stampando nuove immagini attraverso l’utilizzo del software Boardmaker già in uso.
 E-Tran. Permette una rapida comunicazione con un facilitatore. Tale soluzione è stata proposta a causa dei movimenti involontari molto marcati che impediscono l’uso degli arti superiori in modo funzionale, ma con un controllo della testa sufficiente e una buona funzionalità visiva. Schede di comunicazione. riorganizzate per temi, facilmente ricercabili, e integrate stampando nuove immagini attraverso l’utilizzo del software Boardmaker già in uso.")
34
Psicotecnologo: Soluzioni per l’apprendimento e la vita indipendente
ATA process – 1° ciclo: Meeting del teem multidisciplinare: proposte di soluzioni dello psicotecnologo per l’apprendimento e la vita indipendente Psicotecnologo: Soluzioni per l’apprendimento e la vita indipendente Sistema di scansione automatica Il sistema è costituito da uno switch Jelly Bean e il software Clicker, personalizzabile dagli insegnanti, impostato per la scansione automatica.

35
Psicotecnologo: Soluzioni per la postura e la mobilità
ATA process – 1° ciclo: Meeting del teem multidisciplinare: proposte di soluzioni dello psicotecnologo per la postura e la mobilità Psicotecnologo: Soluzioni per la postura e la mobilità Sistema posturale Junior della Jenx Dopo aver visto il video prodotto dalla madre, il fisiatra ha trovato che sistema di postura in uso fosse inadeguato. Il nuovo sistema oltre a migliorare la postura, supporta la TA per l’apprendimento e la comunicazione.

36
ATA process – 1° ciclo: Processo di abbinamento: Relazione dello psicotecnologo
Comportamento e personalità Il SOTU fornisce la prova che Arianna generalmente sembra: felice a casa e a scuola, disponibile, espressiva, impaziente, motivatia, coinvolta nelle attività, flessibile, curiosa, cooperativa. E-Tran Capisce immediatamente la modalità d’uso; controlla i movimenti oculari in modo preciso e veloce; allungare il tempo di fissazione dell’occhio su richiesta. Il matching test è molto positivo. Schede di comunicazione riorganizzate Comprende adeguatamente i simboli e le loro funzioni. Il matching test è positivo. Il sistema di scansione Clicker Capisce bene la modalità di utilizzo, anche se non è in grado di gestirlo autonomamente, con riferimento al tempo e presenta difficoltà a mantenere la pressione sul sensore in modo coerente. Ha una dismetria nel toccare il sensore.

37
Le schede di comunicazione riorganizzate e il sistema Clicker
ATA process – 1° ciclo: Processo di abbinamento: Relazione dello psicologo E-Tran Ne è entusiasta, consapevole del suo potenziale comunicativo, attraverso cui può soddisfare sia la necessità di una maggiore autonomia nella comunicazione sia il suo desiderio di interagire con un numero maggiore di persone. Le schede di comunicazione riorganizzate e il sistema Clicker Manifesta diverse difficoltà come riportato dalla psicotecnologo. Tuttavia, la madre e gli insegnanti apprezzano il potenziale educativo di entrambe le tecnologie.

38
ATA process – 1° ciclo: Valutazione ambientale: Relazioni dell’ingegnere e dell’architetto
Ingegnere e architetto valutazione della casa e la classe sulla base di 3 dimensioni ambientali: accessibilità, usabilità e sostenibilità. Accessibilità: non si sono riscontrati problemi di accessibilità. Usabilità e sostenibilità: il sistema Clicker può essere utilizzato solo in uno spazio sicuro e ben illuminato (usabilità) e se vicino a una presa elettrica (sostenibilità). Questo ha richiesto una valutazione ambientale in loco e non solo tramite video e mappa.
 e se vicino a una presa elettrica (sostenibilità). Questo ha richiesto una valutazione ambientale in loco e non solo tramite video e mappa.")
39
ATA process – 1° ciclo: Valutazione ambientale: Relazioni dell’ingegnere e dell’architetto – Metodo
Metodo – Valutazione ambientale del sistema di scansione Clicker (ICF = e1251) adattato con un joystick e cloche (ICF = E1201) utilizzando sia la carrozzina elettrica sia il nuovo sistema posturale Junior in due posizioni in aula. Con Arianna seduta nella solita scrivania, in posizione centrale. Con Arianna seduta in una nuova posizione più periferica dal centro della classe e più vicino alla parete; riducendo il rischio di danneggiamento involontario del sistema; migliore illuminazione (ICF = E2400); vicina a una presa elettrica (ICF = E1501). La valutazione della performance si è basata sui tempi di esecuzione di 5 compiti diversi per ogni prova comparati su quelli ottenuti presso il Centro (M = 14.46s; DS = 5.55s).
 adattato con un joystick e cloche (ICF = E1201) utilizzando sia la carrozzina elettrica sia il nuovo sistema posturale Junior in due posizioni in aula. Con Arianna seduta nella solita scrivania, in posizione centrale. Con Arianna seduta in una nuova posizione. più periferica dal centro della classe e più vicino alla parete; riducendo il rischio di danneggiamento involontario del sistema; migliore illuminazione (ICF = E2400); vicina a una presa elettrica (ICF = E1501). La valutazione della performance si è basata sui tempi di esecuzione di 5 compiti diversi per ogni prova comparati su quelli ottenuti presso il Centro (M = 14.46s; DS = 5.55s).")
40
Risultati della valutazione ambientale in carrozzina elettrica
ATA process – 1° ciclo: Valutazione ambientale: Relazioni dell’ingegnere e dell’architetto – Risultati 1 Risultati della valutazione ambientale in carrozzina elettrica In posizione centrale e in carrozzina elettrica l’interazione con il sistema molto lenta (M = 23,53s, DS = 4,68s). Il sistema di scansione in questa posizione non è stato considerato come un facilitatore (ICF = e1251+0) né la carrozzina elettrica (ICF = E1201+0); la scarsa illuminazione e la distanza dalla presa elettrica sono stati gravi ostacoli ambientali (ICF = e // e1501.3). In posizione periferica e in carrozzina elettrica l’interazione più veloce ma ancora non ottimale (M = 21,49s; DS = 2,09s). L’illuminazione e l’accesso alle prese sono stati facilitatori (ICF = e // e1501+4), mentre la sedia a rotelle elettrica e il software Clicker non erano ancora adeguati (ICF = e e E1201+0).
. Il sistema di scansione in questa posizione non è stato considerato come un facilitatore (ICF = e1251+0) né la carrozzina elettrica (ICF = E1201+0); la scarsa illuminazione e la distanza dalla presa elettrica sono stati gravi ostacoli ambientali (ICF = e // e1501.3). In posizione periferica e in carrozzina elettrica. l’interazione più veloce ma ancora non ottimale (M = 21,49s; DS = 2,09s). L’illuminazione e l’accesso alle prese sono stati facilitatori (ICF = e // e1501+4), mentre la sedia a rotelle elettrica e il software Clicker non erano ancora adeguati (ICF = e e E1201+0).")
41
ATA process – 1° ciclo: Valutazione ambientale: Relazioni dell’ingegnere e dell’architetto – Risultati 2 Risultati della valutazione ambientale nel sistema posturale Junior solo in posizione periferica Il tempo della performance molto vicino alle prestazioni al Centro (M = 15,11s; DS = 2,07s ). Al termine delle prove, è stato somministrato tramite E-Tran la scala di soddisfazione QUEST 2.0 (Device = 28; Servizi = 16; Soddisfazione media = 3,17). L’interazione con il software di sistema di scansione Clicker è auto- valutato come soddisfacente (M = 3.11; DS = 0,44 ). Conclusioni Il sistema di scansione Clicker risulta un facilitatore completo (ICF = e ) solo quando associato al sistema posturale Junior (ICF = E ). Si raccomanda l’utilizzo del sistema posturale in casa al fine di ottimizzare le competenze di Arianna nell’uso.
. Al termine delle prove, è stato somministrato tramite E-Tran la scala di soddisfazione QUEST 2.0 (Device = 28; Servizi = 16; Soddisfazione media = 3,17). L’interazione con il software di sistema di scansione Clicker è auto- valutato come soddisfacente (M = 3.11; DS = 0,44 ). Conclusioni. Il sistema di scansione Clicker risulta un facilitatore completo (ICF = e ) solo quando associato al sistema posturale Junior (ICF = E ). Si raccomanda l’utilizzo del sistema posturale in casa al fine di ottimizzare le competenze di Arianna nell’uso.")
42
ATA process – 1° ciclo: Supporto e follow-up
E-Tran Non utilizzato a casa e poco a scuola perché considerato come troppo low-tech. Schede di comunicazione Utilizzate spontaneamente in tutti gli ambienti. I compagni di classe hanno svolto il ruolo di facilitatori. Restano problemi relative alla sua gestione autonoma. Sistema di scansione Clicker Gestito in modo completamente indipendente, in casa per adattare i libri e a scuola per la creazione di unità di apprendimento personalizzati. Sistema posturale Junior ha risposto alle richieste del contesto.

43
ATA process – 1° ciclo: Supporto e follow-up Relazione psicologo
Lo psicologo La bassa attrattiva tecnologica dell’E-Tran ha determinato il suo non-uso, dimostrando il ruolo centrale che il contesto ha nell’utilizzo delle TA. Il non-uso dell’E-Tran ha comportato il mantenimento di una forte dipendenza di Arianna dalla madre per i suoi bisogni comunicativi, necessaria per la gestione dei sistemi tecnologici più avanzati. Gli insegnanti hanno espresso la necessità di ridurre gradualmente il sostegno di Arianna nell’uso delle TA.

44
ATA process – 1° ciclo: Supporto e follow-up Relazione psicotecnologo
Lo psicotecnologo Ritiene di riproporre l’E-Tran e di continuare l’utilizzo del sistema di scansione Clicker per ottenere una maggiore autonomia. Programma un nuovo processo di abbinamento e convoca il team multidisciplinare per descrivere la nuova situazione.

45
IV Parte: modellizzare una fase di follow-up
In this first segment I will include a presentation of a new ideal Assistive Technology Assessment process based on the biopsychosocial model of disability and used in a center for assistive technology provision.

46
1 PROCESSO DI FOLLOW-UP

47
PERCORSI PRESCRITTIVI PROTESI ACUSTICHE
2 PERCORSI PRESCRITTIVI PROTESI ACUSTICHE

48
PRESCRIZIONE E FOLLOW-UP
3 PRESCRIZIONE E FOLLOW-UP

49
MISURE SOGGETTIVE FOLLOW-UP
WHODAS 2.0 APHAB ATUFS & QUEST OPERATORI MISURE SOGGETTIVE FOLLOW-UP

50
V PARTE: GESTIRE UN ata process: LO psICOTECNOLOGO
In this segment I will present the professional figure of the psychotechnologist with particular reference to the specific contexts of application of the assistive technology assessment process in a center for technical aids.

51
Tra l’utente e la tecnologia: Lo psicotecnologo
autonomia interazione participazione Caratteristiche della tecnologia Bisogni dell’utente The assessment process is critical to future success for assistive solutions, it involves a wide range of disciplines and in some cases the emergence of new interdisciplinary approaches. [click] The psychotechnologist is an expert of Information and Communication Technologies, in particular in Human-Computer Interaction and human factors and analyses the relations emerging from the person-technology interaction. The psychotechnologist analyzes the interaction between the User and the Assistive Technology. The analysis aims to reach a level of autonomy of the person in need. psicologo tecnologo

52
Cos’è e non è uno psicotecnologo
Perché no? Lo psicotecnologo non è uno Psicologo clinico. Lo psicotecnologo ha una formazione in psicologia (della riabilitazione e salute). Cognitive ergonomist Valuta l’interazione secondo una reciprocità dualistica tra due poli: il sistema dell’utente e il sistema manufatto (Norman 1983). Perché no? Lo psicotecnologo valuta l’interazione secondo un modello olistico utente-AT-ambiente. Lo psicotecnologo è un esperto in soluzioni assitive. Psicologo (in un Centro ausili) è un esperto in fattori personali; relazioni umane e comunicazione; valutazione psicologica e intervento; dinamiche e variabili biopsicosociali. The main role of cognitive ergonomics is to analyze person-artifact interaction in the working environment by taking into account: Both the cognitive and behavioral effects arising from the interaction system; The activities and skills needed to improve productivity and effectiveness; and, at the same time To avoid any cognitive or physical overload. [click] The psychotechnologist evaluates the interaction between a person and a technology by following a user-AT-milieu holistic model. Moreover, the psychotechnologist values the importance of one or more technological aids selected for an assistive solution. As dr. Fabio Meloni explained in the segment 2, the professional role of the psychologist in assistive technology service provision focuses on personal factors, human relationships, and communication, connecting the “bio-”, “psycho-” and “social” components affecting the assistive technology assessment process. Psychotechnologist is not a clinic/dynamic psychologist, is not the so called “shrink”, but he or she has a background in psychology, especially in rehabilitation.
. Cognitive ergonomist. Valuta l’interazione secondo una reciprocità dualistica tra due poli: il sistema dell’utente e il sistema manufatto (Norman 1983). Perché no Lo psicotecnologo valuta l’interazione secondo un modello olistico utente-AT-ambiente. Lo psicotecnologo è un esperto in soluzioni assitive. Psicologo (in un Centro ausili) è un esperto in. fattori personali; relazioni umane e comunicazione; valutazione psicologica e intervento; dinamiche e variabili biopsicosociali. The main role of cognitive ergonomics is to analyze person-artifact interaction in the working environment by taking into account: Both the cognitive and behavioral effects arising from the interaction system; The activities and skills needed to improve productivity and effectiveness; and, at the same time. To avoid any cognitive or physical overload. [click] The psychotechnologist evaluates the interaction between a person and a technology by following a user-AT-milieu holistic model. Moreover, the psychotechnologist values the importance of one or more technological aids selected for an assistive solution. As dr. Fabio Meloni explained in the segment 2, the professional role of the psychologist in assistive technology service provision focuses on personal factors, human relationships, and communication, connecting the bio- , psycho- and social components affecting the assistive technology assessment process. Psychotechnologist is not a clinic/dynamic psychologist, is not the so called shrink , but he or she has a background in psychology, especially in rehabilitation.")
53
Cosa fa lo psicotecnologo
Strumenti: ATD-PA QUEST, SUMI, IPDA… Sistema Tecnologico Barriere e facilitatori “How does the Psychotechnologist work?” Being a psychotechnologist, I introduce a new mark: “the socio-environment-system” by following the biopsychosocial perspective. In this way, the psychotechnologist aims to analyze barriers and facilitators to obtain the best combination possible. Specifically, the psychotechnologist analyzes the interaction between three different systems: [click] the Person, the Technology and the Environmental factors. The analysis aims to reach a level of autonomy of the person in need (related to contextual factors and technological features and functions). The psychotechnologist verifies if the environmental expectations (such as: family, health and educational’ operators) can meet the user’s possibilities to benefit from the technology. In order words, I explore the related material to find the user’s needs by seeking a proper assistive solution (in cooperation with the multidisciplinary team). With the use of different tools (ATD-PA, QUEST, SUMI, IPDA, etc.), the psychotechnologist leads the team by observing critical issues and problems. This analysis it’s important because the psychotechnology: facilitates the human being’s adaptation to the environment system; forces the users to a cognitive, cultural modification and adaptation; increases the information taken by the human technology interaction; modifies the characteristics and functions of the mind; allows a different synthesis of the information; And re-organizes the relations between the elements of the experience. Sistema-utente Sistema socio-ambientale Prospettiva biopsicosociale
. The psychotechnologist verifies if the environmental expectations (such as: family, health and educational’ operators) can meet the user’s possibilities to benefit from the technology. In order words, I explore the related material to find the user’s needs by seeking a proper assistive solution (in cooperation with the multidisciplinary team). With the use of different tools (ATD-PA, QUEST, SUMI, IPDA, etc.), the psychotechnologist leads the team by observing critical issues and problems. This analysis it’s important because the psychotechnology: facilitates the human being’s adaptation to the environment system; forces the users to a cognitive, cultural modification and adaptation; increases the information taken by the human technology interaction; modifies the characteristics and functions of the mind; allows a different synthesis of the information; And re-organizes the relations between the elements of the experience. Sistema-utente. Sistema socio-ambientale. Prospettiva biopsicosociale.")
54
Valutazione dati utente e organizzazione del setting;
Preparazione del setting; Processo di abbinamento; Valutazione della soluzione assistiva; Supporto e follow-up. START Centro Ausili Contact User data collection Setting set-up Matching process: - assistive solution proposal - assistive solution user-trial - assistive solution outcome Assistive solution Multidisciplinary team evaluation User Support Follow up NOT User agreement EXIT Multidisciplinary team meeting for: - user data valuation and - setting design Environmental assessment process (see the Usability and Accessibility evaluation diagram) Assistive Technology Provision 1 2 3 4 5 As you can see in detail in the figure 4 of the supplementary material, [click] the psychotechnologist acts in the following steps. The psychotechnologist analyzes the related material and emphasis any environmental, personal and technological issue (phase 1). In agreement with the multidisciplinary team, I also study the medical case by considering: the individual predisposition to the assistive solutions; previous experiences with AT; the current motivation to use AT; the environmental factors that may affect the matching process of the Matching Persons and Technology (SOTU and ATD-PA). The psychotechnologist prepares the setting and checks if the technologies are working (phase 2). More specifically, the psychotechnologist: checks if the social environment is going to support the solution; checks the equipment that will be part of tests (during the assessment to select some ATs, such as keyboard supports, mouse emulators and communication software, etc.) for example selects portable communicators designed for wheelchair use. The multidisciplinary team, along with the user assesses the assistive solution proposed, tries the solution and gathers outcome data (phase 3-4). Assistive solution proposal: the psychotechnologist offers the user the tested technologies by explaining functions and features. Assistive solution user trial: while the user tests the assistive solutions, the psychotechnologist supervises the interaction (between the user and the assistive technology) by collecting any critical situation. Assistive solution outcome: in this phase, the psychotechnologist discusses with the multidisciplinary team about the observations made during the interaction of the user and technology. When the Assistive Technology is delivered to the user, follow up and ongoing user support is activated. The psychotechnologist, in according by the multidisciplinary team, evaluates the outcome of the assistive solution in the context of use (phase 5). When the assistive solution requires an environmental evaluation, the team starts the Environmental Assessment Process to respect the eAccessibility requirements.
 Assistive Technology Provision As you can see in detail in the figure 4 of the supplementary material, [click] the psychotechnologist acts in the following steps. The psychotechnologist analyzes the related material and emphasis any environmental, personal and technological issue (phase 1). In agreement with the multidisciplinary team, I also study the medical case by considering: the individual predisposition to the assistive solutions; previous experiences with AT; the current motivation to use AT; the environmental factors that may affect the matching process of the Matching Persons and Technology (SOTU and ATD-PA). The psychotechnologist prepares the setting and checks if the technologies are working (phase 2). More specifically, the psychotechnologist: checks if the social environment is going to support the solution; checks the equipment that will be part of tests (during the assessment to select some ATs, such as keyboard supports, mouse emulators and communication software, etc.) for example selects portable communicators designed for wheelchair use. The multidisciplinary team, along with the user assesses the assistive solution proposed, tries the solution and gathers outcome data (phase 3-4). Assistive solution proposal: the psychotechnologist offers the user the tested technologies by explaining functions and features. Assistive solution user trial: while the user tests the assistive solutions, the psychotechnologist supervises the interaction (between the user and the assistive technology) by collecting any critical situation. Assistive solution outcome: in this phase, the psychotechnologist discusses with the multidisciplinary team about the observations made during the interaction of the user and technology. When the Assistive Technology is delivered to the user, follow up and ongoing user support is activated. The psychotechnologist, in according by the multidisciplinary team, evaluates the outcome of the assistive solution in the context of use (phase 5). When the assistive solution requires an environmental evaluation, the team starts the Environmental Assessment Process to respect the eAccessibility requirements.")
55
Assistec – Austria (Miesenberger, 2006)
University courses Assistec – Austria (Miesenberger, 2006) Corso e-learning; 4 moduli e 17 seminari; Diploma in Esperto in Tecnologie Assistive. Modulo 1: Fondamenti Modulo 2: Conoscenze specifiche sulle Tecnologie Assistive In 2006 Miesemberger and colleagues proposed an online e-learning course called Assistec focused on Assistive Technologies, e-Accessibility and e-Inclusion with the aim to provide methods, techniques and guidelines to improve the interaction between disabled users and Information and Communication Technologies by means of Assistive Psychotechnologies. The university course was open to people from different academic backgrounds and provided a graduation as experts in the area of Assistive Technologies. [click] The course has been divided into 4 modules 7 seminars as illustrated: The first module described the fundamentals such as e-learning, medicine and physiology, legislative framework and rehabilitation technologies; The second module focused on assistive technologies for special knowledge; The third module illustrated the process of assortment and provision of assistive technologies related to information and communication technologies; The fourth module showed examples in practice and application related to assistive technologies. Modulo 3: Processi di Assortimento e Fornitura di TA e ICT Modulo 4: Tecnologie Assistive in Pratica e Applicazioni
 Corso e-learning; 4 moduli e 17 seminari; Diploma in Esperto in Tecnologie Assistive. Modulo 1: Fondamenti. Modulo 2: Conoscenze specifiche sulle Tecnologie Assistive. In 2006 Miesemberger and colleagues proposed an online e-learning course called Assistec focused on Assistive Technologies, e-Accessibility and e-Inclusion with the aim to provide methods, techniques and guidelines to improve the interaction between disabled users and Information and Communication Technologies by means of Assistive Psychotechnologies. The university course was open to people from different academic backgrounds and provided a graduation as experts in the area of Assistive Technologies. [click] The course has been divided into 4 modules 7 seminars as illustrated: The first module described the fundamentals such as e-learning, medicine and physiology, legislative framework and rehabilitation technologies; The second module focused on assistive technologies for special knowledge; The third module illustrated the process of assortment and provision of assistive technologies related to information and communication technologies; The fourth module showed examples in practice and application related to assistive technologies. Modulo 3: Processi di Assortimento e Fornitura di TA e ICT. Modulo 4: Tecnologie Assistive in Pratica e Applicazioni.")
56
Master in Psicotecnologie per Soluzioni Assistive
University course Master in Psicotecnologie per Soluzioni Assistive Corso universitario; 4 moduli, 1000 h di insegnamento frontale, 500 h tirocinio and workshop; Diploma in Esperto in psicotecnologie. Modulo 1: Fondamenti Modulo 2: Introduzione alla Psicotecnologia Furthermore, we propose here an example of a Bachelor of Science university course in Psychotechnology for Assistive Solutions, aiming at providing theoretical and methodological skills that are necessary for the analysis, the evaluation and the intervention on the processes involved in the interaction system between persons and technologies, with a particular attention to disabled persons. Students who successfully complete the Psychotechnology for Assistive Solutions course will obtain a Bachelor of Psychotechnologist. [click] The course is divided in 4 module for a total of 1500 hours including training and workshops, and it will focus on: basics in psychology, healthcare, design principles and legislation; theoretical background of psychotechnology and overview of the evaluation techniques of person-technology interaction; different Assistive Technologies and different application fields; phases and actions for the Assistive Technology assessment process. Please, find further information in the supplementary material. Modulo 3: Elementi di base e avanzati su Tecnologie Assistive Modulo 4: Soluzioni Assistive

57
VI PARTE: VALUTARE I FATTORI AMBIENTALI IN UN’AUSILIOTECA
In this fourth segment I will present a model for evaluating the impact of the environment within the Assistive Technology Assessment process. This model adopts a holistic outlook that integrates the three dimensions of accessibility, sustainability, and universal design.

58
Why assess the environment
Health conditions are affected by environmental factors (WHO, 2011, World report on Disability) AT abandonment is affected by environmental factors (Philips & Zhao, 1994; Scherer et al. 2005; Federici & Borsci, 2011) The first World Report on Disability recently published by the WHO (2011) states that “Data on all aspects of disability and contextual factors are important for constructing a complete picture of disability and functioning. Without information on how particular health conditions in interaction with environmental barriers and facilitators affect people in their everyday lives, it is hard to determine the scope of disability.” [click] Moreover, several surveys on assistive technology abandonment collected a large amount of data about the importance and effect of personal and psychosocial factors on the non-use and discontinuance of assistive technology use.
 AT abandonment is affected by environmental factors. (Philips & Zhao, 1994; Scherer et al. 2005; Federici & Borsci, 2011) The first World Report on Disability recently published by the WHO (2011) states that Data on all aspects of disability and contextual factors are important for constructing a complete picture of disability and functioning. Without information on how particular health conditions in interaction with environmental barriers and facilitators affect people in their everyday lives, it is hard to determine the scope of disability. [click] Moreover, several surveys on assistive technology abandonment collected a large amount of data about the importance and effect of personal and psychosocial factors on the non-use and discontinuance of assistive technology use.")
59
What the environment is in the ATA process
Any context in which the AT is used by a person Social and natural environment and artifacts Personal Factors ICF - biopsychosocial model Health condition (disorder or disease) Body Functions and Structures Activities Participation Environmental Factors Personal Definition Environmental Factors Personal ICF Contextual Factors According to the ICF biopsychosocial model of disability, shown in the slide, [click] the environment and the personal factors belong to the Contextual Factors. Therefore, we define the environment in the Assistive Technology Assessment process as any context in which the AT is used by a person. According to this definition the environment refers to the world in which people with different levels of functioning must live and act (WHO, 2011, p. 5). The dimensions of the context in which the AT is used are: The social and natural environments and human artifacts (i.e., products and technology, the natural and built environment, support and relationships, attitudes and services, systems, and policies). Personal factors, such as age, sex, race, motivation, and self-esteem, influence how much a person participates in society. These dimensions can be either considered as facilitators or barriers. Dimensions
 Body Functions. and Structures. Activities. Participation. Environmental. Factors. Personal. Definition. Environmental. Factors. Personal. ICF. Contextual Factors. According to the ICF biopsychosocial model of disability, shown in the slide, [click] the environment and the personal factors belong to the Contextual Factors. Therefore, we define the environment in the Assistive Technology Assessment process as any context in which the AT is used by a person. According to this definition the environment refers to the world in which people with different levels of functioning must live and act (WHO, 2011, p. 5). The dimensions of the context in which the AT is used are: The social and natural environments and human artifacts (i.e., products and technology, the natural and built environment, support and relationships, attitudes and services, systems, and policies). Personal factors, such as age, sex, race, motivation, and self-esteem, influence how much a person participates in society. These dimensions can be either considered as facilitators or barriers. Dimensions.")
60
How to assess environment
Environment of use Facilitator (AT) Barriers ICF Constructs Output User’s Performance According to the ICF, “facilitator” and “barrier” provide a way to weight how much elements of the environment of use (context) fostering or preventing person’s performance. Of course any AT should be considered as a facilitator since it should be improve the user’s performance.
 Barriers. ICF Constructs. Output. User’s Performance. According to the ICF, facilitator and barrier provide a way to weight how much. elements of the environment of use (context) fostering or preventing person’s performance. Of course any AT should be considered as a facilitator since it should be improve the user’s performance.")
61
How to improve the user’s performance AT facilitator
Measures of Environment and AT impact Mirza, Gosset, & Borsci 2012 Decisions for Improving User’s Performance Modify Environment Modify AT Modify AT and Environment Environment of use Access Use Sustainable Mirza, Gosset, and Borsci (2012) have pointed out three measures of environment and assistive technology impact on the user’s performance: Accessibility (Access): It measures the level of environmental characteristics to permit entrance, exit, and internal movements. This measure also predicts how many changes are needed for rendering accessible the environment in use. Universal design (Use): It measures how much an environment and a human product are designed for all. Sustainability (Sustainable): It measures how much an environment and AT are adaptable over the time to person’s changing needs, with minimal impact on natural environment and economic maintenance. [click] These three measures guide professionals to make decisions in order to: Modify the environment; Modify the AT, or change the current AT with another one; Modify both AT and the Environment.
 have pointed out three measures of environment and assistive technology impact on the user’s performance: Accessibility (Access): It measures the level of environmental characteristics to permit entrance, exit, and internal movements. This measure also predicts how many changes are needed for rendering accessible the environment in use. Universal design (Use): It measures how much an environment and a human product are designed for all. Sustainability (Sustainable): It measures how much an environment and AT are adaptable over the time to person’s changing needs, with minimal impact on natural environment and economic maintenance. [click] These three measures guide professionals to make decisions in order to: Modify the environment; Modify the AT, or change the current AT with another one; Modify both AT and the Environment.")
62
Assess the match between AT and environment
Accessibility The three measures of the accessibility, universal design, and sustainability capture three perspectives on the interaction between person and assistive technology in an environment of use. [click] The goal of practitioners (e.g., architecture, engineer, psychotechnologist, ergonomist, etc.) is to reach an “ideal fit”, that is, matching these three dimensions. Nevertheless, previous researches (Gossett et al., 2009) has shown that a “perfect fit” remains a ideal goal. Instead, in most situations there exists a tenuous relationship between these three desired features pulling the design solution in divergent directions (e.g., more accessible than usable and sustainable). The adopted final solution eventually reflects a trade off between the three dimensions of accessibility, sustainability, and universal design as the following slide shows. Ideal fit Universal Design Sustainability
 is to reach an ideal fit , that is, matching these three dimensions. Nevertheless, previous researches (Gossett et al., 2009) has shown that a perfect fit remains a ideal goal. Instead, in most situations there exists a tenuous relationship between these three desired features pulling the design solution in divergent directions (e.g., more accessible than usable and sustainable). The adopted final solution eventually reflects a trade off between the three dimensions of accessibility, sustainability, and universal design as the following slide shows. Ideal fit. Universal. Design. Sustainability.")
63
Assess the match between AT and environment
The dimensions of accessibility, sustainability, and universal design each exists along their own continuum. Each decision about the environment or about the AT (or both) can be evaluated in terms of universal design, accessibility, and sustainability, falling into various places on the three continua. The evaluation on the three continua can help to focus a decision on a critical deciding factor for improving the person performance. [click]
 can be evaluated in terms of universal design, accessibility, and sustainability, falling into various places on the three continua. The evaluation on the three continua can help to focus a decision on a critical deciding factor for improving the person performance. [click]")
64
How to assess accessibility
General guidelines Physical access laws Local policies The practitioners may assess accessibility by using general guidelines and national physical access laws for analysing the barriers that prevent the interaction between AT and users in the environment of use. A knowledge of local policies governing accessibility will also help determine whether the AT and environmental modifications will be publicly or privately funded, that is a key factor in determining the feasibility of the proposed assistive solution.

65
How to assess Universal Design
Principle of UD Effectiveness, efficiency and satisfaction The practitioners may assess universal design by using the design principle (e.g., as the seven principles of universal design of the Center for Universal Design, 1997) for considering the users’ needs who may require assistive solutions to fully participate in a given space. At the same time practitioners have to consider how to assess the effectiveness, the efficiency, and the satisfaction perceived by the persons when they use AT in different environments. This is especially important when an assistive solution is proposed for communal settings, such as schools, and it involves multiple users in various capacities, such as students, parents, administrators.
 for considering the users’ needs who may require assistive solutions to fully participate in a given space. At the same time practitioners have to consider how to assess the effectiveness, the efficiency, and the satisfaction perceived by the persons when they use AT in different environments. This is especially important when an assistive solution is proposed for communal settings, such as schools, and it involves multiple users in various capacities, such as students, parents, administrators.")
66
How to assess sustainability
Sustainable standards / principles Person’s needs over the time (changing) Impact AT-Environment (cost of maintenance) Practitioners assess the sustainability of the physical, social, economical, ecological and temporal contexts during the Environmental Assessment process. The sustainability can be assessed by using specific standards for physical environments, as the Leadership Energy and Environmental Design (LEED; U.S. Green Building Council, 2011). At the same time, it is important to consider not only how much the solution is ecologically sound and environmentally-friendly, but also on how much the solution will meet the user’s changing needs over a period of time, ideally a life span.
 Impact AT-Environment (cost of maintenance) Practitioners assess the sustainability of the physical, social, economical, ecological and temporal contexts during the Environmental Assessment process. The sustainability can be assessed by using specific standards for physical environments, as the Leadership Energy and Environmental Design (LEED; U.S. Green Building Council, 2011). At the same time, it is important to consider not only how much the solution is ecologically sound and environmentally-friendly, but also on how much the solution will meet the user’s changing needs over a period of time, ideally a life span.")
67
Environmental Assessment Process Change the environment
Center for Technical Aid Check the match Environment data collecting START Environment Universal design Accessibility Sustainability AT/end user Contact User data collection MATCH END EXIT TO YES Multidisciplinary team meeting for: - user data valuation and - setting design NOT NOT Check the impact Modify the environment in use (Mod–Env) Proposal of a new matching process or strong personalization (Prop–nMP) IF IF Setting set-up Matching process: - assistive solution proposal - assistive solution user-trial - assistive solution outcome Impact of environment modification Impact of a new matching process Climate Impact Assistive solution Multidisciplinary team evaluation Mod–Env Results Prop–nMP Results In the ATA process a specific Environment Assessment procedure guides multidisciplinary team to effectively evaluate and determine a best assistive solution for the user’s needs. We can identify three main phases of the environment assessment process: [click] The first phase consists in Checking the match: The practitioners assess the environment impact in supporting or obstructing full participation for the user. IF there is a match between the environment, the user, and the AT, the assistive solution is achieved and the environment assessment process ends. While, IF a match does not occur, it is necessary to estimate the impact of the possible modification to the environment or to the AT. In the phase two, practitioners have to check the economical and socio-cultural impact of the modifications to the climate. The modifications can regard the environment, the assistive technology or both. [Click] On the base of the impact analysis, in the phase three, practitioners can take one of the following decisions: Suggest the modification of the environment Click] – In this case, the ATA process restarts from the multidisciplinary team’s evaluation for a new or the modified assistive technology. The match between the assistive technology and the user only requires a minimal environmental adaptation. But the practitioners can decide do not modify the environment by the modification of assistive technology. – In this case, the ATA process restarts with a new multidisciplinary team meeting in order to discuss: The cost-benefit of assistive technology modifications; The cost-benefit for identifying another assistive technology. In this case the process restarts from the beginning of the assistive technology assessment process. Finally the practitioners could decide to modify both the assistive technology and the environment. – Also in this case, the ATA process needs to restart with a new multidisciplinary team meeting in order to discuss costs-benefits of the proposed modifications. NOT Take a decision Mod–Env < Prop–nMT MATCH Prop–nMP < Mod–Env IF IF EXIT User agreement IF Prop–nMP = Mod–Env NOT NOT Assistive Technology Provision Results Change the AT END EXIT TO Change both User Support Change the environment Change AT and environment Change the AT Change Environment Follow up
 Proposal of a new. matching process. or strong. personalization (Prop–nMP) IF. IF. Setting set-up. Matching process: - assistive solution proposal - assistive solution user-trial - assistive solution outcome. Impact of environment modification. Impact of a new matching process. Climate. Impact. Assistive solution Multidisciplinary team evaluation. Mod–Env Results. Prop–nMP Results. In the ATA process a specific Environment Assessment procedure guides multidisciplinary team to effectively evaluate and determine a best assistive solution for the user’s needs. We can identify three main phases of the environment assessment process: [click] The first phase consists in Checking the match: The practitioners assess the environment impact in supporting or obstructing full participation for the user. IF there is a match between the environment, the user, and the AT, the assistive solution is achieved and the environment assessment process ends. While, IF a match does not occur, it is necessary to estimate the impact of the possible modification to the environment or to the AT. In the phase two, practitioners have to check the economical and socio-cultural impact of the modifications to the climate. The modifications can regard the environment, the assistive technology or both. [Click] On the base of the impact analysis, in the phase three, practitioners can take one of the following decisions: Suggest the modification of the environment. Click] – In this case, the ATA process restarts from the multidisciplinary team’s evaluation for a new or the modified assistive technology. The match between the assistive technology and the user only requires a minimal environmental adaptation. But the practitioners can decide do not modify the environment by the modification of assistive technology. – In this case, the ATA process restarts with a new multidisciplinary team meeting in order to discuss: The cost-benefit of assistive technology modifications; The cost-benefit for identifying another assistive technology. In this case the process restarts from the beginning of the assistive technology assessment process. Finally the practitioners could decide to modify both the assistive technology and the environment. – Also in this case, the ATA process needs to restart with a new multidisciplinary team meeting in order to discuss costs-benefits of the proposed modifications. NOT. Take. a decision. Mod–Env < Prop–nMT. MATCH. Prop–nMP. < Mod–Env. IF. IF. EXIT. User agreement. IF. Prop–nMP. = Mod–Env. NOT. NOT. Assistive Technology Provision. Results. Change the AT. END EXIT TO. Change both. User Support. Change the environment. Change. AT and. environment. Change the AT. Change Environment. Follow up.")
Presentazioni simili