Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
M.Verri U.O. Anestesia e Rianimazione Universitaria Dir.Prof.R.Alvisi

2
Valutazione della gravità
Riconoscimento che qualche cosa non va alterazione del sensorio dispnea, tachipnea, alterazione della meccanica-dinamica ventilatoria SpO2 alterazione della PA tachicardia, aritmia contrazione della diuresi T° alterazione degli esami ematochimici ecc. quanto sopra + iper-ipotermia / leucocitosi-leucopenia infezione Che fare di fronte ai segnali d’allarma che ho indicato precedentemente? Una delle cose da fare, anche se il quadro clinico (anamnesi + es.obiettivo) ci inducono a ritenere presente un quadro di sepsi, sepsi grave o, peggio, shock settico, è ricordare che esistono altre patologie che possono mimare tali quadri (anche perché ne condividono parte della patogenesi)(v dia successiva) Quanto non va ? Valutazione della gravità giudizio personale scale di gravità sepsi, sepsi grave, shock settico
 ci inducono a ritenere presente un quadro di sepsi, sepsi grave o, peggio, shock settico, è ricordare che esistono altre patologie che possono mimare tali quadri (anche perché ne condividono parte della patogenesi)(v dia successiva) Quanto non va Valutazione della gravità. giudizio personale. scale di gravità. sepsi, sepsi grave, shock settico.")
3
SOFA ? Tachicardia Ipotensione
CVP PAOP Ittero Enzimi Albumina PT Stato di coscienza alterato, confusione, psicosi FR > 20 atti/m PaO2 < 70 mm Hg SaO2 < 90% PaO2/FiO2 300 Oliguria Anuria Creatinina Piastrine PT/APTT Proteina C D-dimero SOFA ?

4
Modified Early Warning Score
Cut-off >4 Subbe CP et al Q J Med 2001; 94: Patient-At-Risk warning score Goldhill DR et al Anaesthesia 2005; 60:

5
Sequential Organ Failure Assessment (SOFA)
Vincent JL, et al. Intensive Care Med 1996;22:707-10 Score 1 2 3 4 SNC GCS 13-14 10-12 6-9 <6 RESPIRATORIO Pa/FiO2 (mmHg) < 400 < 300 < 200 con supporto resp < 100 CARDIOVASCOLARE Ipotensione MAP < 70 mmHg Dopa < 5 o DObutamina Dopa > 5 o Adr < 0,1 o Noradr < 0,1 Dopa > 15 Adr > 0,1 Noradr > 0,1 COAGULAZIONE Piastrine(103/mm3) < 150 <100 <50 <20 FEGATO Bilirubina(mg/dl) 1,2-1,9 2,0-5,9 6,0-11,9 >12 RENALE Creat (mg/dl) o Diur 2,0-3,4 3,5-4,9 o < 500 ml/24h > 5,0 < 200 ml/24 h
 < 400. < 300. < 200 con supporto resp. < 100. CARDIOVASCOLARE. Ipotensione. MAP < 70 mmHg. Dopa < 5 o DObutamina. Dopa > 5 o. Adr < 0,1 o. Noradr < 0,1. Dopa > 15. Adr > 0,1. Noradr > 0,1. COAGULAZIONE. Piastrine(103/mm3) < 150. <100. <50. <20. FEGATO. Bilirubina(mg/dl) 1,2-1,9. 2,0-5,9. 6,0-11,9. >12. RENALE. Creat (mg/dl) o Diur. 2,0-3,4. 3,5-4,9 o. < 500 ml/24h. > 5,0. < 200 ml/24 h.")
6
S.C 37 aa endocardite embolizzazione shock (settico?) coma
ascessi cerebrali ipoperfusione ipossia Riconoscimento gravità Supporto delle funzioni vitali Terapia eziologica Prevenzione complicanze insuff.respiratoria cardiopatia

7
Sapere Sapere fare (efficacia?) Efficienza Economicità sicurezza
Etica Allocazione risorse sicurezza Economicità: Utilizza in modo efficiente le proprie risorse raggiungendo in modo efficace i propri obiettivi EFFICACIA = Grado di raggiungimento di un obiettivo (sia qualitativo che quantitativo) EFFICIENZA = COSTO DELLE RISORSE / OUTPUT OUTPUT???: N. Prestazioni sanitarie N. Pazienti partecipanti ad un trattamento N. Sperimentazioni
 EFFICIENZA = COSTO DELLE RISORSE / OUTPUT. OUTPUT : N. Prestazioni sanitarie. N. Pazienti partecipanti ad un trattamento. N. Sperimentazioni.")
8
riconoscimento shock settico valutazione-monitoraggio
sono guarito !!! riconoscimento shock settico sua gravità diagnosi differenziale microbiologia antibioticoterapia rimozione sorgente Coupled Plasma Filtration Adsorption CPFA Ottimizzazione perfusione volemia cristalloidi colloidi emocomponenti emoderivati tono vascolare vasocostrittori vasodilatatori ?? contrattilità miocardica dobutamina (dopamina) ECMO CPFA (Coupled Plasma Filtration Adsorption) è un trattamento extracorporeo per pazienti con multi-organ failure (MOF) o sepsi attuato utilizzando una cartuccia sorbente dedicata. La resina messa a punto per questa specifica indicazione consente di adsorbire i principali mediatori infiammatori coinvolti. La tecnica, mediante un plasmafiltro, separa dal sangue il plasma, e questo attraversa successivamente una cartuccia in grado di adsorbire un ampio range di mediatori pro e anti infiammatori. Il plasma così purificato viene restituito al paziente. A questo primo stadio segue, in serie, un emofiltro che provvede alla depurazione per convezione e al bilancio idrico e a quello dell’equilibrio acido-base steroidi ? supporto respiratorio sostituz.funzione renale controllo glicemico nutrizione sedazione prevenzione complicanze ecc. valutazione-monitoraggio
 ECMO. CPFA (Coupled Plasma Filtration Adsorption) è un trattamento extracorporeo per pazienti con multi-organ failure (MOF) o sepsi attuato utilizzando una cartuccia sorbente dedicata. La resina messa a punto per questa specifica indicazione consente di adsorbire i principali mediatori infiammatori coinvolti. La tecnica, mediante un plasmafiltro, separa dal sangue il plasma, e questo attraversa successivamente una cartuccia in grado di adsorbire un ampio range di mediatori pro e anti infiammatori. Il plasma così purificato viene restituito al paziente. A questo primo stadio segue, in serie, un emofiltro che provvede alla depurazione per convezione e al bilancio idrico e a quello dell’equilibrio acido-base. steroidi supporto respiratorio. sostituz.funzione renale. controllo glicemico. nutrizione. sedazione. prevenzione complicanze. ecc. valutazione-monitoraggio.")
9
Special admission paths: sepsis
R Ferrer, A.Navas, ML Martinez, A.Artigas The key to success involves the implementation of a hospital wide system that recognizes septic patients early, and at the same time rapidly administers effective therapy ( sepsis-rapid response team)(?) The results of the meta-analysis are very consistent in showing that sepsis bundles improve survival by improving the way sepsis treatments are delivered Health care organizations traditionally favour investing in new technology and drugs, but are reluctant to invest in organizational development. For sepsis care bundles to succeed, this must change elementi del bundle probabilmente correlati a sopravvivenza: antibioticoterapia, rapido riconoscimento della sorgente d’infezione, volemia e pressione, supporto respiratorio, proteina C attivata (?), controllo della glicemia (?) Barochia AV, Cui X, Vitberg D, Suffredini AF, O’Grady NP, Banks SM. Bundled care for septic shock: an analysis of clinical trial. Crit Care Med 2010; 38(2) Ferrer R, Artigas A, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med 2009; 180(9):861-6 Levy MM, Dellinger RP, Bion J. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med 2010;36(2):222-31
( ) The results of the meta-analysis are very consistent in showing that sepsis bundles improve survival by improving the way sepsis treatments are delivered. Health care organizations traditionally favour investing in new technology and drugs, but are reluctant to invest in organizational development. For sepsis care bundles to succeed, this must change. elementi del bundle probabilmente correlati a sopravvivenza: antibioticoterapia, rapido riconoscimento della sorgente d’infezione, volemia e pressione, supporto respiratorio, proteina C attivata ( ), controllo della glicemia ( ) Barochia AV, Cui X, Vitberg D, Suffredini AF, O’Grady NP, Banks SM. Bundled care for septic shock: an analysis of clinical trial. Crit Care Med 2010; 38(2) Ferrer R, Artigas A, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med 2009; 180(9): Levy MM, Dellinger RP, Bion J. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med 2010;36(2):")
10
Signal pathway activation
Sepsis is very complex! Da EMC 2010 Infectious agent? Other factors? Pro inflammatory mediator early inhibitors Receptor activation Signal pathway activation Coagulation cascade Inflammatory cascade mini trattato di biochimica e patologia generale fallimento delle terapie rivolte ad un solo mediatore cytokine storm (tempesta) ROS Pro- inflammatory mediators Anti- inflammatory mediators inhibitors Protein synthesis
 ROS. Pro- inflammatory. mediators. Anti- inflammatory. mediators. inhibitors. Protein synthesis.")
11
Immunoinflammatory response of three hypothetical patients
Immunoinflammatory response of three hypothetical patients with sepsis. The individual immune response in sepsis is determined by many factors, including pathogen virulence characteristics, size of the bacterial inoculum, patient comorbidities. The initial immune response is hyperinflammatory, but the response rapidly progresses to hypoinflammatory. In the healthy individual who experiences meningococcemia, there is a robust hyperinflammatory response. Death may occur rapidly because of a hyperinflammatory state, and antiinflammatory treatments may improve survival. If infection resolves, there is only a minimal hypoimmune state. In the elderly patient with malnutrition who experiences diverticulitis, the initial response is limited, and if the infection persists, a prolonged hypoinflammatory response develops, followed by recovery or death. In the patient with diabetes, chronic renal failure, and pneumonia, the initial response is blunted, and there is a prolonged depression of immune function. (Modified from Hotchkiss RS, Karl IE: The pathophysiology and treatment of sepsis. N Engl J Med 2003; 348:138–50. Used with permission. Copyright © Massachusetts Medical Society 2003.) Immunosoppressione Immunoinflammatory response of three hypothetical patients with sepsis.
 Immunosoppressione. Immunoinflammatory response of three hypothetical patients. with sepsis.")
12
riconoscimento shock settico valutazione-monitoraggio
sua gravità diagnosi differenziale microbiologia antibioticoterapia rimozione sorgente Coupled Plasma Filtration Adsorption CPFA Ottimizzazione perfusione volemia cristalloidi colloidi emocomponenti emoderivati tono vascolare vasocostrittori vasodilatatori ?? contrattilità miocardica dobutamina (dopamina) ECMO CPFA (Coupled Plasma Filtration Adsorption) è un trattamento extracorporeo per pazienti con multi-organ failure (MOF) o sepsi attuato utilizzando una cartuccia sorbente dedicata. La resina messa a punto per questa specifica indicazione consente di adsorbire i principali mediatori infiammatori coinvolti. La tecnica, mediante un plasmafiltro, separa dal sangue il plasma, e questo attraversa successivamente una cartuccia in grado di adsorbire un ampio range di mediatori pro e anti infiammatori. Il plasma così purificato viene restituito al paziente. A questo primo stadio segue, in serie, un emofiltro che provvede alla depurazione per convezione e al bilancio idrico e a quello dell’equilibrio acido-base steroidi ? supporto respiratorio sostituz.funzione renale controllo glicemico nutrizione sedazione prevenzione complicanze ecc. valutazione-monitoraggio
 ECMO. CPFA (Coupled Plasma Filtration Adsorption) è un trattamento extracorporeo per pazienti con multi-organ failure (MOF) o sepsi attuato utilizzando una cartuccia sorbente dedicata. La resina messa a punto per questa specifica indicazione consente di adsorbire i principali mediatori infiammatori coinvolti. La tecnica, mediante un plasmafiltro, separa dal sangue il plasma, e questo attraversa successivamente una cartuccia in grado di adsorbire un ampio range di mediatori pro e anti infiammatori. Il plasma così purificato viene restituito al paziente. A questo primo stadio segue, in serie, un emofiltro che provvede alla depurazione per convezione e al bilancio idrico e a quello dell’equilibrio acido-base. steroidi supporto respiratorio. sostituz.funzione renale. controllo glicemico. nutrizione. sedazione. prevenzione complicanze. ecc. valutazione-monitoraggio.")
18
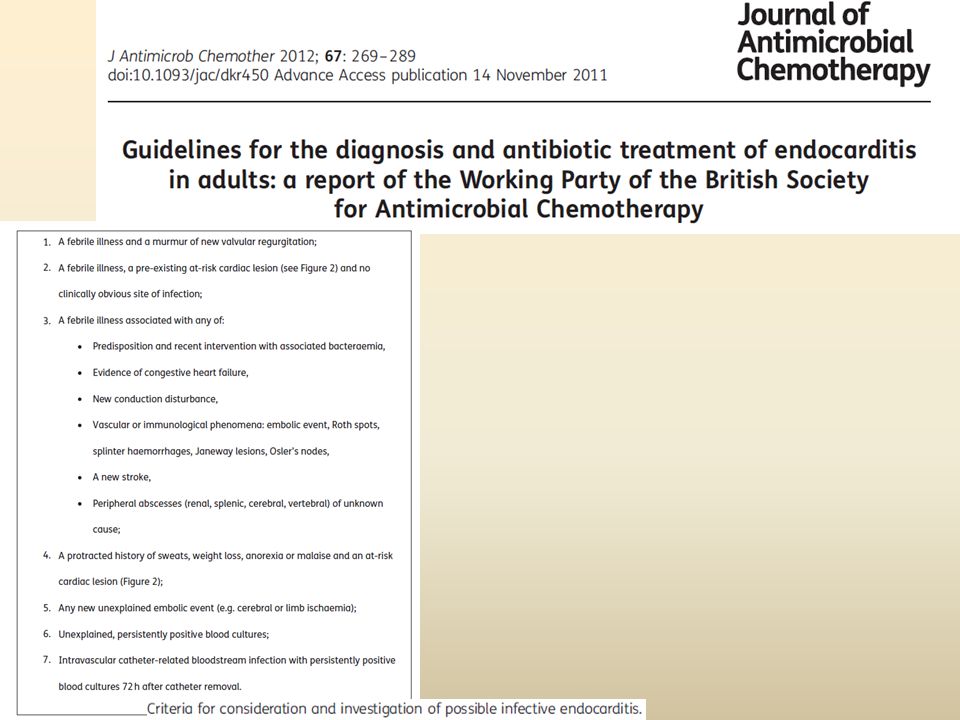
Cardiac conditions considered to increase a patient’s risk of developing infective endocarditis, i.e. ‘at risk’ heart valve lesions.

19
The endocarditis risk in GUCH patients is substantially higher than in the general population, with marked variation between lesions. It has to be emphasized that good oral hygiene and regular dental review have an essential role in reducing the risk of IE. Aseptic measures are mandatory during manipulation of venous catheters and during any invasive procedure in order to reduce the rate of healthcare-associated IE. GUCH patients should also be discouraged from getting piercings and tattoos.

20
The approach to antibiotic endocarditis prophylaxis has changed for several reasons.
In short, transient bacteraemia occurs not only after dental procedures but frequently in the context of daily routine activities such as tooth brushing, flossing, or chewing. Due to the lack of scientific evidence for the efficacy of antibiotic prophylaxis, the estimated huge number of patients that may need to be treated to prevent one single case of IE, the small but existing risk of anaphylaxis, and the general problem of emergence of resistant microorganisms resulting from widespread, often inappropriate use of antibiotics, it is currently recommended by expert consensus to limit antibiotic prophylaxis to patients with the highest risk of IE undergoing the highest risk procedures (IIaC).
.")
21
This recommendation includes the following patient groups:
Patients with a prosthetic valve or a prosthetic material used for cardiac valve repair Patients with previous IE Patients with CHD: a cyanotic CHD, without surgical repair, or with residual defects, palliative shunts, or conduits a CHD after repair with prosthetic material whether placed by surgery or by percutaneous technique, up to 6 months after the procedure (until endothelialization) a when a residual defect persists at the site of implantation of a prosthetic material or device by cardiac surgery or percutaneous technique. The recommendation is limited to dental procedures requiring manipulation of the gingival or periapical region of the teeth or perforation of the oral mucosa. Antibiotics are not recommended for respiratory tract, gastrointestinal, genitourinary, dermatological, or musculoskeletal procedures unless there is an established infection.
 a when a residual defect persists at the site of implantation of a prosthetic material or device by cardiac surgery or percutaneous technique. The recommendation is limited to dental procedures requiring manipulation of the gingival or periapical region of the teeth or perforation of the oral mucosa. Antibiotics are not recommended for respiratory tract, gastrointestinal, genitourinary, dermatological, or musculoskeletal procedures unless there is an established infection.")
27
Steroids ◦ Consider intravenous hydrocortisone for adult septic shock when hypotension remains poorly responsive to adequate fluid resuscitation and vasopressors. (2C) ◦ ACTH stimulation test is not recommended to identify the subset of adults with septic shock who should receive hydrocortisone. (2B) ◦ Hydrocortisone is preferred to dexamethasone. (2B) ◦ Fludrocortisone (50μg orally once a day) may be included if an alternative to hydrocortisone is being used which lacks significant mineralocorticoid activity. Fludrocortisone is optional if hydrocortisone is used. (2C) ◦ Steroid therapy may be weaned once vasopressors are no longer required. (2D) • Hydrocortisone dose should be ≤300 mg/day. (1A) • Do not use corticosteroids to treat sepsis in the absence of shock unless the patient’s endocrine or corticosteroid history warrants it. (1D) Strength of recommendation and quality of evidence have been assessed using the GRADE criteria, presented in brackets after each guideline. For added clarity: • Indicates a strong recommendation or “we recommend”; ◦ indicates a weak recommendation or “we suggest” CIRCI = Critical Illness-related corticosteroid insufficiency
 ◦ ACTH stimulation test is not recommended to identify the subset of adults with septic shock who should receive hydrocortisone. (2B) ◦ Hydrocortisone is preferred to dexamethasone. (2B) ◦ Fludrocortisone (50μg orally once a day) may be included if an alternative to hydrocortisone is being used which lacks significant mineralocorticoid activity. Fludrocortisone is optional if hydrocortisone is used. (2C) ◦ Steroid therapy may be weaned once vasopressors are no longer required. (2D) • Hydrocortisone dose should be ≤300 mg/day. (1A) • Do not use corticosteroids to treat sepsis in the absence of shock unless the patient’s endocrine or corticosteroid history warrants it. (1D) Strength of recommendation and quality of evidence have been assessed using the GRADE criteria, presented in brackets after each guideline. For added clarity: • Indicates a strong recommendation or we recommend ; ◦ indicates a weak recommendation or we suggest CIRCI = Critical Illness-related corticosteroid insufficiency.")
28
Nov.2008 Steroids Negli ultimi anni l’uso dei corticosteroidi nello shock settico è risultato controverso Pro: miglioramento emodinamico con più rapida sospensione dei vasopressori > rapidità di risoluzione della disfunzione d’organo < mortalità (?) Con: mortalità tra responder e non responder = rapidità nella sospensione dei vasopressori > superinfezioni debolezza neuromuscolare intolleranza glucidica cortisone provoca, nell’ambito del processo infiammatorio innescato nella sepsi: IL-6, espressione di NF- NO
 Con: mortalità tra responder e non responder. = rapidità nella sospensione dei vasopressori. > superinfezioni. debolezza neuromuscolare. intolleranza glucidica. cortisone provoca, nell’ambito del processo infiammatorio innescato nella sepsi: IL-6, espressione di NF- NO.")
29
Steroids Annane D, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002;288: Sì steroidi nello shock settico che richiede vasopressori SprungCL, et al. The CORTICUS randomized, double-blind, placebo-controlled study of hydrocortisone therapy in patients with septic shock. N Engl J Med 2008;358: NO steroidi nello shock settico ... Queste differenze sono state sintetizzate in questi due studi...

30
Steroids Recommendation 6:
Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American College of Critical Care Medicine Crit Care Med 2008; 36:1937–1949 Recommendation 6: Hydrocortisone should be considered in the management strategy of patients with septic shock, particularly those patients who have responded poorly to fluid resuscitation and vasopressor agents. Strength of Recommendations: 2B

31
Corticosteroids in the Treatment of Severe Sepsis and Septic Shock in Adults Annane D, Bellissant E, Bollaert PE, et al. JAMA. 2009; 301: 28-day mortality was modestly reduced (relative risk [RR] = 0.84, P = .05) and was also modestly reduced in the subset of studies reporting prolonged corticosteroid administration (RR = 0.84, P = .02). Treatment increased the proportion of patients achieving reversal of shock and reduced the length of intensive care unit stay without a detectable increase in gastrointestinal bleeding, superinfection, or neuromuscular complications. Corticosteroids did increase the risk for hyperglycemia and hypernatremia. The authors concluded that the prolonged use of corticosteroids safely reduces short-term mortality in patients with severe sepsis or septic shock. Until a definitive clinical trial answers this question, corticosteroid use will continue to be highly variable and at the discretion of intensivists worldwide metaanalisi
 and was also modestly reduced in the subset of studies reporting prolonged corticosteroid administration (RR = 0.84, P = .02). Treatment increased the proportion of patients achieving reversal of shock and reduced the length of intensive care unit stay without a detectable increase in gastrointestinal bleeding, superinfection, or neuromuscular complications. Corticosteroids did increase the risk for hyperglycemia and hypernatremia. The authors concluded that the prolonged use of corticosteroids safely reduces short-term mortality in patients with severe sepsis or septic shock. Until a definitive clinical trial answers this question, corticosteroid use will continue to be highly variable and at the discretion of intensivists worldwide. metaanalisi.")
32
Conclusions: Based on clinically meaningful thresholds (RRR[15–25%) for mortality reduction in severe sepsis or septic shock, the Bayesian approach to all three meta-analyses consistently showed that low-dose steroids were not associated with survival benefits. The probabilities of developing steroid- induced side effects (superinfections, bleeding, and hyperglycemia) were high for all analyses.
 were high for all analyses.")
33
R. Moreno C. L. Sprung D. Annane S. Chevret J. Briegel D. Keh M. Singer Y. G. Weiss D. Payen B. H. Cuthbertson J.-L. Vincent Conclusion Patients randomized to treatment with hydrocortisone demonstrated a faster decrease in total organ dysfunction/failure determined by the SOFA score, primarily driven by a faster improvement in cardiovascular organ dysfunction/failure. This organ dysfunction/failure improvement was not accompanied by a decreased mortality.

34
Ideal therapy for sepsis
Plasma “bad molecules” SIRS = Systemic inflammatory response syndrome CARS = Compensatory anti-inflammatory response syndrome Hyper-inflammation Normal Immunoparalysis “good molecules” We also adapted the use of resins for acute patients. Note that this technique is different from the previous technique in that we use plasma instead of ultrafiltrate and a much greater quantity of resin. UF out Reinfusate in

35
CPFA used successfully in non-ARF patients
Hemodynamic response to coupled plasmafiltration-adsorption in human septic shock Marco Formica, Carlo Olivieri, Sergio Livigni, Giulio Cesano, Antonella Vallero, Mariella Maio and Ciro Tetta Intensive Care Med (2003) 29: Objective: The objective was to examine the effect of repeated applications of coupled plasmafiltration-adsorption on the hemodynamic response in septic shock patients hospitalized in intensive care units (ICUs). entusiati Conclusion: Coupled plasmafiltration-adsorption was a feasible and safe extracorporeal treatment and exerted a remarkable improvement in the hemodynamics, the pulmonary function, and the outcome in septic shock patients with or without concomitant ARF.
 29: Objective: The objective was to examine the effect of repeated applications of coupled plasmafiltration-adsorption on the hemodynamic response in septic shock patients hospitalized in intensive care units (ICUs). entusiati. Conclusion: Coupled plasmafiltration-adsorption was a feasible and safe extracorporeal treatment and exerted a remarkable improvement in the hemodynamics, the pulmonary function, and the outcome in septic shock patients with or without concomitant ARF.")
36
Anne-Corne´lie J. M. de Pont, MD, PhD Adult Intensive Care Unit Academic Medical Center University of Amsterdam Amsterdam, The Netherlands …The improvement of blood purification techniques and membranes has generated new opportunities for the use of extracorporeal techniques in sepsis. Removal of both pro- and anti-inflammatory mediators by means of these new techniques is feasible and might add to the restoration of homeostasis by controlling excessive cytokine production (the so-called peak concentration hypothesis). Whether this approach will result in a better clinical outcome for patients with severe sepsis remains to be investigated. più prudenti da definire: metodica, tipologia di filtri utilizzati, volumi trattati, tempo di applicazione
. Whether this approach will result in a better clinical outcome for patients with severe sepsis remains to be investigated. più prudenti. da definire: metodica, tipologia di filtri utilizzati, volumi trattati, tempo di applicazione.")
37
tecnica clinica organizzazione gestione

38
tecnica clinica organizzazione gestione

39
tecnica clinica organizzazione economicità gestione

41
Overall Conclusions CPFA appears to be a safe and well-tolerated treatment for treatment of septic patients CPFA improved hemodynamics, reduced some pro- and anti- inflammatory cytokines and restored immune balance More clinical studies are needed to determine target septic patient population and treatment indications

42
riconoscimento shock settico valutazione-monitoraggio
sono guarito !!! riconoscimento shock settico sua gravità diagnosi differenziale microbiologia antibioticoterapia rimozione sorgente proteina C attivata ricombinante ? (Drotrecogin) Ottimizzazione perfusione volemia cristalloidi colloidi emocomponenti emoderivati tono vascolare vasocostrittori contrattilità miocardica dobutamina monitoraggio microperfusione attraverso doppler laser near-infrared spectroscopy altro mediatore dell’infiammazione pentraxina-3 (PTX3) azioni tra loro coordinate, qualche volta contemporanee qualche volta in rapida successione steroidi ? supporto respiratorio sostituz.funzione renale controllo glicemico nutrizione sedazione prevenzione complicanze ecc. valutazione-monitoraggio
 Ottimizzazione perfusione. volemia. cristalloidi. colloidi. emocomponenti. emoderivati. tono vascolare. vasocostrittori. contrattilità miocardica. dobutamina. monitoraggio microperfusione attraverso doppler laser near-infrared spectroscopy. altro mediatore dell’infiammazione pentraxina-3 (PTX3) azioni tra loro coordinate, qualche volta contemporanee qualche volta in rapida successione. steroidi supporto respiratorio. sostituz.funzione renale. controllo glicemico. nutrizione. sedazione. prevenzione complicanze. ecc. valutazione-monitoraggio.")
43
Da Intensive Care Med 2010;36(12): 2019-2029
:")
44
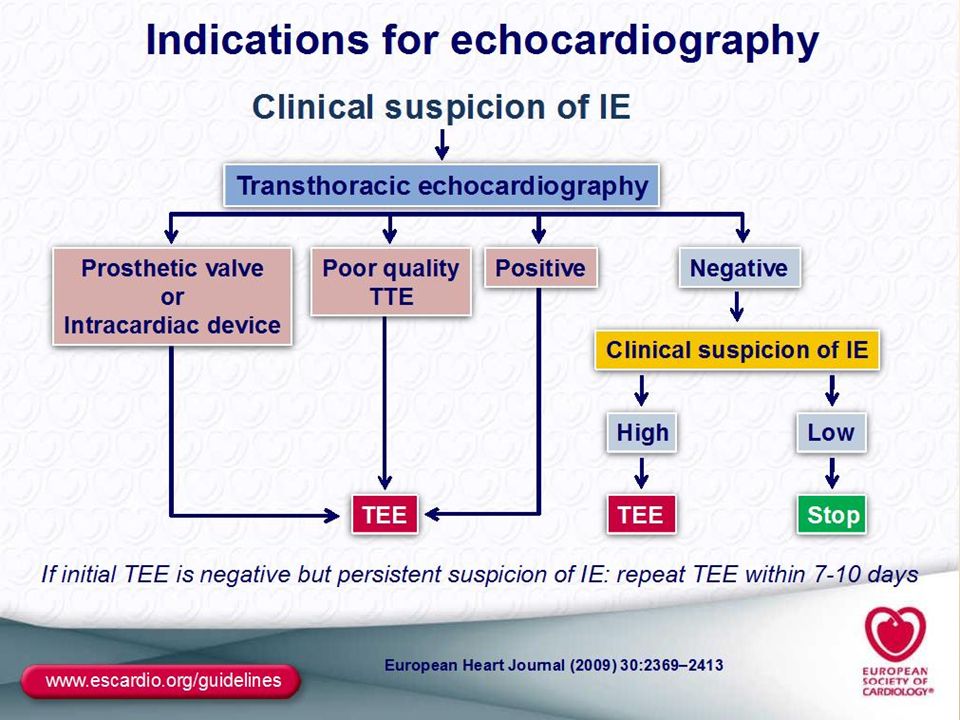
Indications for echocardiography in suspected infective endocarditis.
IE, infective endocarditis; TTE, transthoracic echocardiography; TOE, transoesophageal echocardiography. TOE is not mandatory in isolated right-sided native valve IE with good quality TTE examination and unequivocal echocardiographic findings.

Presentazioni simili



 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")


 is a disease state characterized by airflow limitation that is not fully reversible. The.>")


>")








>")


