Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Y. Meir, A. Poletti, R. Rolli, I. Falco
Tavola Rotonda: Diagnosi e Trattamento del Ca della Cervice Uterina nella Popolazione controllata con lo Screening Y. Meir, A. Poletti, R. Rolli, I. Falco

2
Age-standardised rates of incidence of and mortality from cervical cancer (/100 000 women-years) in 25 European Union (EU) member states, ranked by increasing mortality, estimates for 2004 (direct standardisation using the World reference population). Age-standardised rates of incidence of and mortality from cervical cancer (/100 000 women-years) in 25 European Union (EU) member states, ranked by increasing mortality, estimates for 2004 (direct standardisation using the World reference population). Arbyn M et al. Ann Oncol 2007;18: © 2007 European Society for Medical Oncology
 in 25 European Union (EU) member states, ranked by increasing mortality, estimates for 2004 (direct standardisation using the World reference population). Arbyn M et al. Ann Oncol 2007;18: © 2007 European Society for Medical Oncology.")
3
Estimated incidence, mortality and 5-year prevalence: women European Union, Globocan 2008
Incidence and mortality data for all ages. 5-year prevalence for adult population only. ASR (W) and proportions per 100,000.
 and proportions per 100,000.")
4
Estimated incidence, mortality and 5-year prevalence: women Italy, Dati Globocan 2008
Incidence and mortality data for all ages. 5-year prevalence for adult population only. ASR (W) and proportions per 100,000.
 and proportions per 100,000.")
5
Estimated age-standardised incidence and mortality rates: women Italy, Globocan 2008

6
Mortalità per Cancro della Cervice Uterina in Europa

7
Fig 2 Odds ratio for developing invasive cervical cancer stage IA or worse (in the next five year interval) in those screened in a given (three year) age band compared with those not screened in that age band (or in two previous years). Fig 2 Odds ratio for developing invasive cervical cancer stage IA or worse (in the next five year interval) in those screened in a given (three year) age band compared with those not screened in that age band (or in two previous years). Odds ratios plotted for overlapping age bands. Broken lines indicate risk of developing cervical cancer at ages and Odds ratios and confidence intervals are truncated at 1.2. Figure is based on 4012 cases (including 437 in women under age 30) and 7889 controls Sasieni P et al. BMJ 2009;339:bmj.b2968 ©2009 by British Medical Journal Publishing Group
 in those screened in a given (three year) age band compared with those not screened in that age band (or in two previous years). Odds ratios plotted for overlapping age bands. Broken lines indicate risk of developing cervical cancer at ages and Odds ratios and confidence intervals are truncated at 1.2. Figure is based on 4012 cases (including 437 in women under age 30) and 7889 controls. Sasieni P et al. BMJ 2009;339:bmj.b2968. ©2009 by British Medical Journal Publishing Group.")
8
Ca della Cervice Nel 50% dei la donna non ha mai fatto il PAP test
Nel 10% dei casi non ha fatto il PAP test negli ultimi 5 anni

9
Prevalence of high-risk HPV and incident cases of cervical cancer in the United States, 2003–2005.Surveillance Epidemiology and End Results (SEER) data for incident cases among females aged 15 to 19 years and 50 to 64 years. Prevalence of high-risk HPV and incident cases of cervical cancer in the United States, 2003–2005.Surveillance Epidemiology and End Results (SEER) data for incident cases among females aged 15 to 19 years and 50 to 64 years. Data are from references 27 and 45. HPV = human papillomavirus. Vesco K K et al. Ann Intern Med 2011;155: ©2011 by American College of Physicians
 data for incident cases among females aged 15 to 19 years and 50 to 64 years. Data are from references 27 and 45. HPV = human papillomavirus. Vesco K K et al. Ann Intern Med 2011;155: ©2011 by American College of Physicians.")
10
Age-adjusted incidence of and deaths from invasive cervical cancer in the United States, 2000–2008.Mortality rates are from 2000–2007 data. Age-adjusted incidence of and deaths from invasive cervical cancer in the United States, 2000–2008.Mortality rates are from 2000–2007 data. Data are from reference 45. Vesco K K et al. Ann Intern Med 2011;155: ©2011 by American College of Physicians

11
Ca della Cervice Fattori che condizionano la prognosi
Stadio del tumore Grado del tumore Tipo istologico Diffusione linfatica Invasione vascolare

12
Carcinoma della Cervice – Classificazione FIGO 2009
Stadio I Tumore confinato alla cervice IA Tumore microinvasivo con invasione stromale ≤5 mm ed estensione superficiale non > 7 mm IA1 Invasione stromale ≤3.0 mm in profondità ed estensione ≤7.0 mm IA2 Invasione stromale tra 3.0 e 5.0 mm con estensione non >7.0 mm IB Lesioni limitate alla cervice clinicamente visibili oppure lesioni precliniche maggiori di quelle per lo stadio IA2 IB1 Lesione ≤4.0 cm di dimensione IB2 Lesione >4.0 cm di dimensione

13
Carcinoma della Cervice – Classificazione FIGO 2009
Stadio II Tumore che si estende oltre la cervice ma non raggiunge la parete pelvica o il terzo inferiore della vagina IIA Senza evidente invasione dei parametri IIA1 Lesione ≤4.0 cm IIA2 Lesione >4.0 cm IIB Con evidente invasione dei parametri

14
Stadio III Il tumore si estende alla parete pelvica e/o coinvolge il terzo inferiore della vagina e/o causa idronefrosi o rene escluso IIIA Il tumore coinvolge il terzo inferiore della vagina ma no si estende alla parete pelvica IIIB Estensione alla parete pelvica e/o causa idronefrosi o rene escluso Stadio IV Il tumore si estende oltre la pelvi oppure coinvolge la vescica o retto IVA Diffusione ad organi adiacenti IVB Diffusione ad organi lontani

15
Ca Cervice: Sopravvivenza per stadio

17
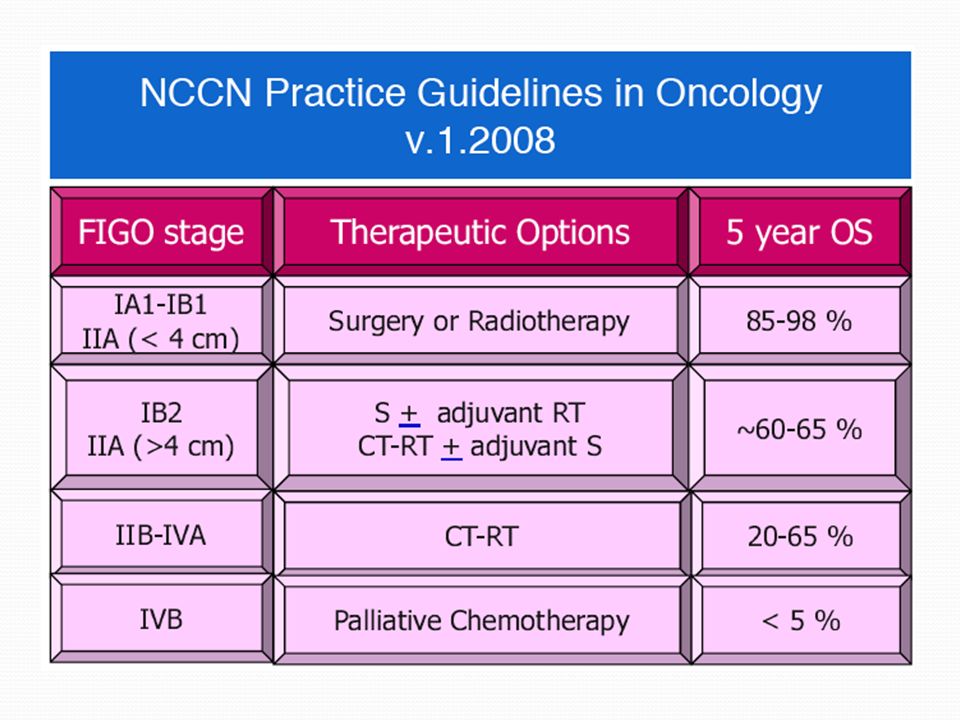
Ca Cervice – LG trattamento
Stadio FIGO IA1 Il trattamento standard consiste in una conizzazione con margini liberi oppure isterectomia semplice (a seconda dell’età della donna) Stadio FIGO IA2 La chirurgia è lo standard. Le opzioni consistono in conizzazione o trachelectomia in pazienti giovani e in isterectomia semplice o radicale in altre pazienti. E’ richiesta la linfadenectomia pelvica. Nelle pazienti con linfonodi positivi, il trattamento standard consiste in Chemio-radio concomitante complementare.
 Stadio FIGO IA2. La chirurgia è lo standard. Le opzioni consistono in conizzazione o trachelectomia in pazienti giovani e in isterectomia semplice o radicale in altre pazienti. E’ richiesta la linfadenectomia pelvica. Nelle pazienti con linfonodi positivi, il trattamento standard consiste in Chemio-radio concomitante complementare.")
18
Isterectomia radicale: Stadi IA2 – IIA (< 4 cm)
Utilizzata per trattare il Ca della Cervice con invasione > 3 mm ma confinati alla cervice e alla vagina (Stadi IA2 – IIA) Vengono rimossi i parametri e la parte superiore della vagina.
 Vengono rimossi i parametri e la parte superiore della vagina.")
19
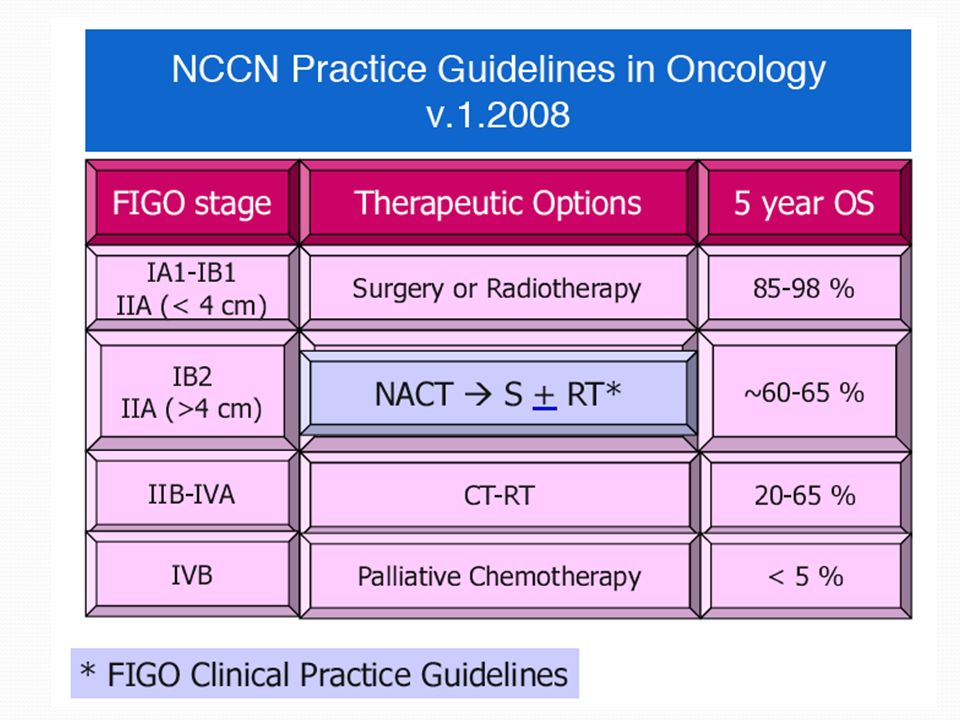
Ca Cervice – LG trattamento
Stadio FIGO IB1 Non esiste un trattamento standard. Le opzioni consistono in chirurgia, radioterapia esterna più brachiterapia oppure Chirurgia-radioterapia combinate. Stadio FIGO IB2 – IVA Chemio-Radio concomitante rappresenta lo standard La radioterapia esterna è combinata con la brachiterapia L’isterectomia extrafasciale è un’opzione Il ricorso alla terapia neoadiuvante è tuttora controverso.

20
Rapporti tra componenti nel programma di Screening
Screening spontaneo I Livello Ambulatorio Colposcopia S.C. Ginecologia II Livello diagnostico Consultorio CIN Colposcopia e prelievi bioptici Follow-up Conizzazioni Escissioni DTC Colposcopia e prelievi bioptici Follow-up Cancro Cervice Cancro Cervice Stadiazione e Chirurgia S.C. Ginecologia Stadiazione post-Chirurgia S.C. Anatomia Patologica Trattamento Post-op S.C. Oncologia

21
Attività S.C. OST/GIN - 2011 Bassano del Grappa
Ambulatorio Colposcopia Conizzazioni con Radiofrequenza 25 Escissioni lesioni con ansa a RF 3 Ablazioni lesioni con RF 3 Sala Operatoria Conizzazioni con RF (Day Surgery) 24 Escissioni con ansa a RF 4 Totale CIN trattate 59
 24. Escissioni con ansa a RF 4. Totale CIN trattate 59.")
22
Successo della prevenzione del Ca della Cervice: Elementi chiave
Copertura dello Screening Collegamento tra Screening e trattamento Efficacia del trattamento

23
Grazie per l’attenzione

24
Storia naturale della delle anomalie citologiche e della CIN
ASCUS 68% regressione a normale 7,3% progressione ad HSIL in 24 mesi 21% progressione a LSIL in 24 mesi 0,25% progressione a Ca invasivo LSIL 47% regressione a normale 0,15% progressione a Ca HSIL 35% regressione a normale 1,44% progressione a Ca CIN 1 60% regressione 10% progressione a CIS 1% progressione a Ca invasivo CIN 3 33% regressione a normale 12% progressione a Ca invasivo

25
Linee Guida ACOG 2009 Revised Guidelines Specific ACOG recommendations in the updated guidelines, based on good and consistent scientific evidence (level A), are as follows: Cervical cancer screening should begin at age 21 years and should be avoided at younger ages, when it may result in unnecessary and harmful workup and treatment in women who are at very low risk for cancer. For women aged 21 to 29 years, cervical cytology screening is recommended every 2 years. The interval between cervical cytology examinations may be extended to every 3 years for women at least aged 30 years who have had 3 consecutive negative cervical cytology screening test results and who have no history of CIN 2 or CIN 3, HIV infection, immunocompromised state, or DES exposure in utero. Acceptable screening techniques are liquid-based and conventional cervical cytology methods. Routine cytology testing should be discontinued in women who have had a total hysterectomy for benign conditions and who have no history of high-grade CIN. For women older than 30 years, an appropriate screening test is cytology combined with HPV DNA testing. When both these test results are negative in a low-risk woman 30 years or older, rescreening should be performed no sooner than 3 years later.
, are as follows: Cervical cancer screening should begin at age 21 years and should be avoided at younger ages, when it may result in unnecessary and harmful workup and treatment in women who are at very low risk for cancer. For women aged 21 to 29 years, cervical cytology screening is recommended every 2 years. The interval between cervical cytology examinations may be extended to every 3 years for women at least aged 30 years who have had 3 consecutive negative cervical cytology screening test results and who have no history of CIN 2 or CIN 3, HIV infection, immunocompromised state, or DES exposure in utero. Acceptable screening techniques are liquid-based and conventional cervical cytology methods. Routine cytology testing should be discontinued in women who have had a total hysterectomy for benign conditions and who have no history of high-grade CIN. For women older than 30 years, an appropriate screening test is cytology combined with HPV DNA testing. When both these test results are negative in a low-risk woman 30 years or older, rescreening should be performed no sooner than 3 years later.")
26
Linee Guida ACOG 2009 Specific ACOG recommendations in the updated guidelines, based on limited and inconsistent scientific evidence (level B), are as follows: Sexually active women younger than 21 years should be counselled and tested for sexually transmitted infections and should be counselled regarding safe sex and contraception. Cervical cytology testing is not necessary, and speculum examination need not be performed in asymptomatic women. Cervical cancer screening can be discontinued between the ages of 65 and 70 years in women who have 3 or more consecutive negative cytology test results and no abnormal test results in the past 10 years because cervical cancer develops slowly, and risk factors decrease with age. Women previously treated for CIN 2, CIN 3, or cancer remain at risk for persistent or recurrent disease for at least 20 years after treatment and after initial posttreatment surveillance. This group should therefore continue to be screened annually for at least 20 years. Even after the period of posttreatment surveillance, screening should continue for women status post hysterectomy with removal of the cervix who have a history of CIN 2 or CIN 3, or in whom a negative history cannot be documented. In this patient group, there are no good data to support or refute discontinuing screening.
, are as follows: Sexually active women younger than 21 years should be counselled and tested for sexually transmitted infections and should be counselled regarding safe sex and contraception. Cervical cytology testing is not necessary, and speculum examination need not be performed in asymptomatic women. Cervical cancer screening can be discontinued between the ages of 65 and 70 years in women who have 3 or more consecutive negative cytology test results and no abnormal test results in the past 10 years because cervical cancer develops slowly, and risk factors decrease with age. Women previously treated for CIN 2, CIN 3, or cancer remain at risk for persistent or recurrent disease for at least 20 years after treatment and after initial posttreatment surveillance. This group should therefore continue to be screened annually for at least 20 years. Even after the period of posttreatment surveillance, screening should continue for women status post hysterectomy with removal of the cervix who have a history of CIN 2 or CIN 3, or in whom a negative history cannot be documented. In this patient group, there are no good data to support or refute discontinuing screening.")
27
Linee Guida ACOG 2009 Revised ACOG recommendations, based primarily on consensus and expert opinion (level C), are as follows: Physicians should inform their patients that annual gynecologic examinations may still be appropriate regardless of the frequency of cervical cytology screening, even if cervical screening is not performed at each visit. Women who were vaccinated against HPV-16 and HPV-18 should follow the same screening guidelines as nonvaccinated women.

28
Geographical distribution of the world age-standardised mortality from cervical cancer in 28 European countries, estimates for 2004. Geographical distribution of the world age-standardised mortality from cervical cancer in 28 European countries, estimates for 2004. Arbyn M et al. Ann Oncol 2007;18: © 2007 European Society for Medical Oncology

29
Geographical distribution of the mortality from uterine cancer among women younger than 45 years in 40 European countries, estimates for 2004. Geographical distribution of the mortality from uterine cancer among women younger than 45 years in 40 European countries, estimates for 2004. Arbyn M et al. Ann Oncol 2007;18: © 2007 European Society for Medical Oncology

30
Prevalence of high-risk HPV and incidence of CIN3 or worse
Prevalence of high-risk HPV and incidence of CIN3 or worse.High-risk HPV types are 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 68. Prevalence of high-risk HPV and incidence of CIN3 or worse.High-risk HPV types are 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 68. Data are from reference 25. Reproduced with permission from Macmillan Publishers, British Journal of Cancer, copyright CIN = cervical intraepithelial neoplasia; HPV = human papillomavirus. Vesco K K et al. Ann Intern Med 2011;155: ©2011 by American College of Physicians

Presentazioni simili

 Brussels, 26 settembre 2013.>")

















