Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Gli oppioidi sono indicati nel dolore neuropatico? NO
“Controversie sulla diagnosi e terapia del dolore neuropatico” Opinioni a confronto Gli oppioidi sono indicati nel dolore neuropatico? NO Marco Lacerenza Medicina del Dolore Fondazione “Opera San Camillo” Casa di Cura S. Pio X, Milano Palermo, novembre 2012, Reale Albergo delle Povere

2
O meglio….ATTENZIONE! Premessa
RCT, Linee Guida…………..artefatti della medicina moderna che danno DATI UTILISSIMI MA…………. Possono subire le influenze di forze non utili al nostro fine Possono facilitare le generalizzazioni possono facilitare la medicina della INDICAZIONE senza valutazione sedano l’ansia del giovane medico e accorciano le visite dell’esperto Proteggono dal pdv medico legale Smettiamola di parlare di “Dolore Neuropatico” Parliamo di Pazienti SOFFERENTI, con dolore spesso neuropatico, cronico, complessi, con molte comorbidità Ognuno diverso dall’altro, con scarsa QoL e problemi famigliari, lavorativi, economici

3
le sue sofferenze, nessuno è universale
Dolore - Sofferenza “Tra i rimedi che Dio Onnipotente ha voluto, bontà Sua, dare all’uomo per alleviare le sue sofferenze, nessuno è universale ed efficace come l’oppio.” Thomas Sydenham, Sumeri: IX secolo AC: oppio la pianta della gioia Omero, IV libro Odissea :….“Nel dolce Vino, di cui bevean, farmaco infuse contrario al pianto e all'ira, e che l'obblìo seco inducea d'ogni travaglio e cura”. GaspareTraversi 1753

4
Distinct roles in hedonic homeostasis and emotional control
High OPIOID RECEPTORS ROLES IN VIVO Distinct roles in hedonic homeostasis and emotional control Mu Reward Delta Kappa Low High Mood Low

5
Individuals with high reward responsiveness, a personality trait dependent on the endogenous opioid neurotransmission, experience more exogenous opioid-induced behavioral analgesia. Emerging evidence suggests that MOR polymorphism could contribute to variability in behavioral opioid analgesia by introducing variability of the MOR responsiveness to exogenous opioids. It is possible that trait RWR and the neuronal response to noxious stimuli in the endogenous opioid-rich brain reward circuitry could be useful endophenotypes of behavioral opioid analgesia.

6
Localizzazione dei recettori per gli oppioidi
Corteccia cingolata anteriore, C.prefrontale, strati superficiali della corteccia cerebrale Nuclei della base, talamo, amigdala, PAG, RMN, reticolare del tronco Corno posteriore midollare: proiezioni midollari afferenti primari Interneuroni midollari Periferia: nocicettori e afferenti viscerali

7
Recettori oppioidi Oppioidi: Meccanismi d’azione Legame Presinaptico
DRG Blocco ingresso ioni Ca++ DNIC Legame postsinaptico Recettori oppioidi Fuoriuscita di ioni K+ Fuoriuscita di ioni K+ Modificata da: A.H.Dickenson, 2000

8
I recettori per gli oppioidi

9
I recettori per gli oppioidi: binding

10
Nerve-injury neuropathy and Diabetic Neuropathy:
Perché funzionano poco???? Nerve-injury neuropathy and Diabetic Neuropathy: Functional downregulation and/or desensitization of μ-opioid receptors in the dorsal horn of the spinal cord (but not a significant decrease in number) may be related to increased production of PKC . May be due to: activation of NMDARs in postsynaptic cells, to an autophosphorylation of the TrkB receptor by BDNF. In fact, the development of the hyperalgesia and allodynia in NP states is suppressed by administration of NMDA receptor antagonists, TrkB/Fc chimera protein (sequesters endogenous BDNF) PKC inhibitors.
 may be related to increased production of PKC . May be due to: activation of NMDARs in postsynaptic cells, to an autophosphorylation of the TrkB receptor by BDNF. In fact, the development of the hyperalgesia and allodynia in NP states is suppressed by. administration of NMDA receptor antagonists, TrkB/Fc chimera protein (sequesters endogenous BDNF) PKC inhibitors.")
11
Ridotta efficacia nella pratica clinica
Dolore Neuropatico: Meccanismi che portano alla desensitizzazione di MORs Ridotta efficacia nella pratica clinica

12
Central Glutamatergic system
Genetic mechanisms Sensitiz. of primary afferent N. Central Glutamatergic system Descending facilitation (in RVM on-cells and CCK) leading to up-regulation of Spinal dynorphin and enhanced primary afferent neurotransmitter release (CGRP) and pain. Decreased reuptake of neurotransmitters from the primary afferent fibers Pain that has become more diffuse and less defined in quality and has a wider spatial distribution than the pre-existing pain. NMDA receptors become activated and when inhibited, prevent the development of tolerance and OIH The glutamate transporter system is inhibited, (increasing the amount of glutamate available to NMDAR) Ca regulated intracellular PKC is likely a link between cellular mechanisms of tolerance and OIH Prolonged morphine administration induces neurotoxicity via NMDA receptor mediated apoptotic cell death in the dorsal horn
 leading to up-regulation of Spinal dynorphin and enhanced primary afferent neurotransmitter release (CGRP) and pain. Decreased reuptake of neurotransmitters from the primary afferent fibers. Pain that has become more diffuse and less defined in quality and has a wider spatial distribution than the pre-existing pain. NMDA receptors become activated and when inhibited, prevent the development of tolerance. and OIH. The glutamate transporter system is inhibited, (increasing the amount of glutamate available to NMDAR) Ca regulated intracellular PKC is likely a link between cellular mechanisms of tolerance and OIH. Prolonged morphine administration induces neurotoxicity via NMDA receptor mediated apoptotic cell death in the dorsal horn.")
13
Smith HS, 2012

14
Il risveglio americano dall’oppiofobia
“Opioid maintenance therapy can be a safe salutary and more humane alternative…..in those patients with intractable non-malignant pain and non history of drug abuse”

15
The reason ………..is unknown.
The dichotomous classification of nociceptive and neuropathic pain is not yet fully recognized in the pain literature or among physicians dealing with pain. ..comon narcotic analgesics, administered in a double-blind fashion and in doses which effectively control acute and chronic nociceptive pain, are inefficient for relief of neuropathic (including deafferentation) pain….. The reason ………..is unknown.
 pain….. The reason ………..is unknown.")
16
Opioids for neuropathic pain (Review), 2009
Eisenberg E, McNicol ED, Carr DB Short-term studies: equivocal evidence regarding the efficacy of opioids in neuropathic pain. Intermediate-term studies demonstrated significant efficacy of opioids over placebo for neuropathic pain. The difference in outcomes does not support the use of short-term opioid administration as a predictive tool to decide whether to initiate intermediate-term opioid therapy. …the participants in the included studies may not reflect those commonly seen in practice. Therefore, issues such as abuse of medication, or conversely, non-compliance due to participants’ unwillingness to tolerate side effects may not be accurately reflected in our results.

17
Studi epidemiologici documentano nel LBP dolore misto nel 20-35% dei casi
1/3 della popolazione ha LBP, quindi il 6% ha una componente neuropatica Il costo dei pazienti con LBP e componente neuropatica è il 70% > rispetto a LBP nocicettivo

19
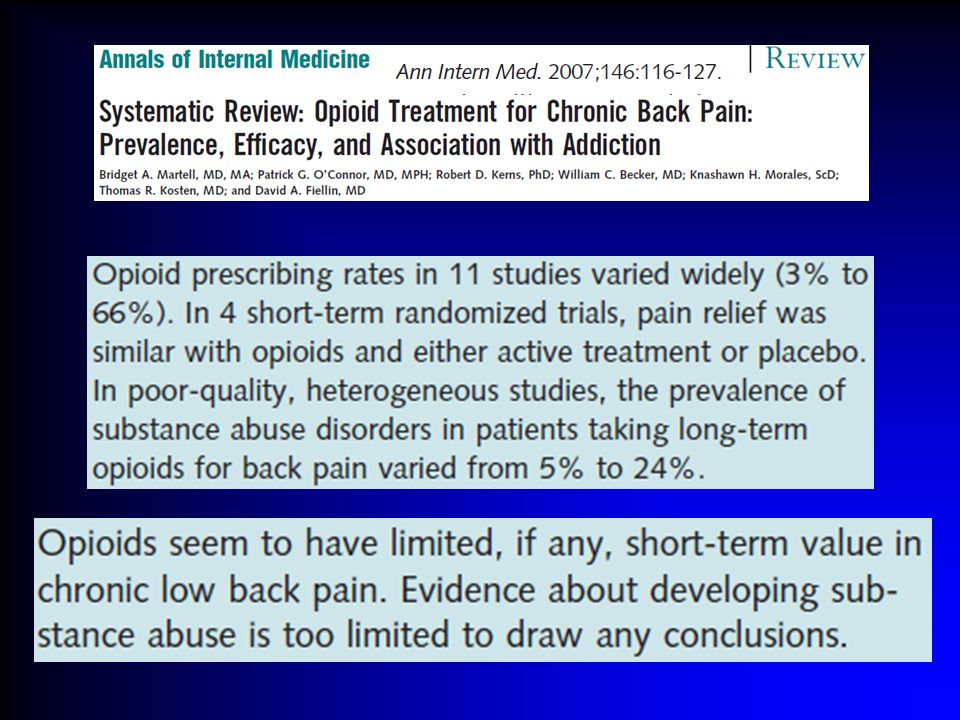
The meta-analysis of Martell et al
The meta-analysis of Martell et al identifies also a number of relevant issues: patients were more likely to be prescribed opioids if they reported greater distress and suffering. The prevalence of substance abuse disorders was in the range of 40% to 50% in these patients and up to 24% showed aberrant medication-taking behaviour Long-term trials of opioid efficacy for chronic back pain are lacking, and there is other evidence that indicates that the long-term efficacy of opioids for chronic pain may be limited

20
Opioids and opioid combinations were exceeding NSAIDs in proportion of patients and number of prescriptions. Short-acting opioids are frequently used as rescue medication…. high prescribing..(36.5%). Although the frequency of use of long-acting opioids was low (3.8%), the median (7.0) number of prescriptions were higher than for any other medication. Opioids continue to be recommended and used, despite evidence of a negative association with outcomes in CLBP, including function and productivity and an increased likelihood of substance use disorders.
. Although the frequency of use of long-acting opioids was low (3.8%), the median (7.0) number of prescriptions were higher than for any other medication. Opioids continue to be recommended and used, despite evidence of a negative association with outcomes in CLBP, including function and productivity and an increased likelihood of substance use disorders.")
21
Several investigations have identified drug abuse in 18%
In such “pathological pain states”, nociception is not the sole target, but also suffering, dysfunction, mood states, psychosocial factors and dependence on the health system. Then opioid use is less likely to improve analgesia and even less to yield psychological or functional improvement. Several investigations have identified drug abuse in 18% to 41% of patients receiving opioids for chronic pain The prevalence of lifetime substance use disorders range from 36% to 56%, with an estimate of 43% current substance use disorders and 5% to 24% of the patients with aberrant medication taking behaviours.

22
Fattori di Rischio per l’Abuso e la Dipendenza
Storia di abuso di sostanze Disturbi mentali Storia di dolori multipli Genere maschile Giovani adulti Prescrizioni di > 90gg ATTENZIONE Programma multidisciplinare Valutazione dolore, QoL, funzionamento Supporto psicologico-occupazionale Educativo-motivazionale Fisioterapico Contratto Spiegazioni esaustive dei rischi A breve e lungo termine

26
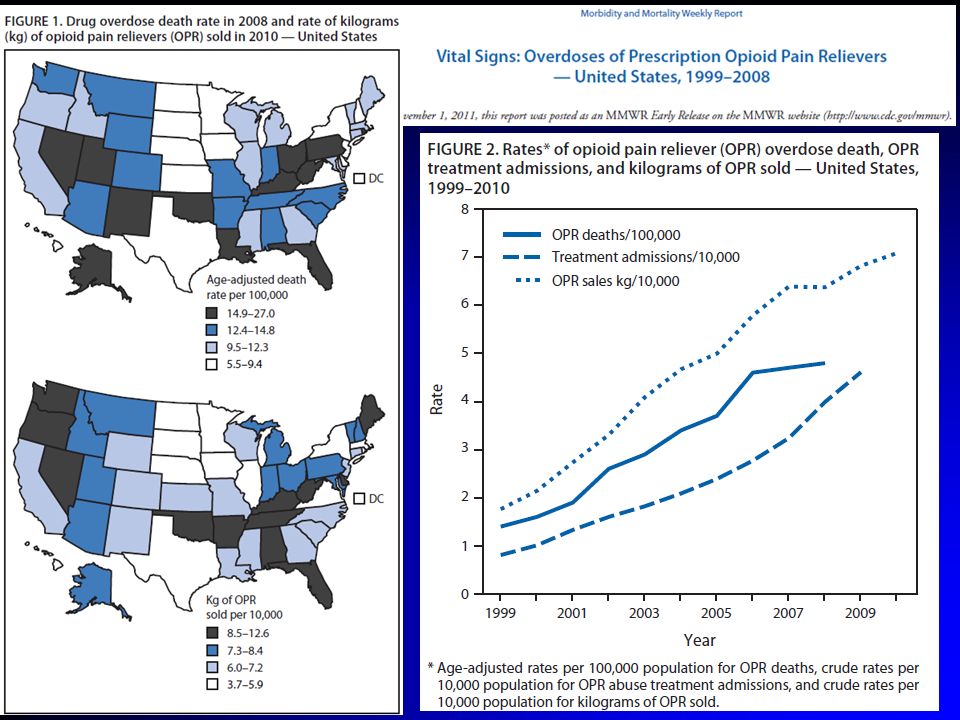
461 report nonmedical uses of opioid analgesics
Unintentional overdose death related to an opioid analgesic 9 persons are admitted for substance abuse treatment 35 visit ER 161 report drug abuse or dependence report nonmedical uses of opioid analgesics

27
It has been shown that from 1997 through 2007, there was a seven fold increase in the number of prescriptions for opioids. The pharmaceutical industry aggressively marketed long-acting opioids for chronic pain relying on 2 erroneous facts: That medical management with opioids is the recommended solution for undertreated chronic pain That the use of long-acting formulations decreases incidences of prescription opioid abuse. The principles of opioid management in acute pain and cancer pain were transferred to the chronic pain arena. JAMA 2000, 283: : ”Increased opioid use is not associated with deleterious health consequences”.

28
Approximately two-thirds of the panel responsible for writing guidelines for the use of opioids for chronic pain for the American Academy of Pain Medicine (AAPM) and American Pain Society (APS) had conflicts of interest with the opioid pharmaceutical industry. The investigation announced by the Senate in reference to conflicts of interest in preparation of opioid guidelines and promotion of opioid usage, have resulted in abandonment of the American Pain Foundation on May 10, 2012, which was a pivotal organization in promoting opioid use.

29
Rischi del trattamento con oppioidi nel lungo termine:
Dipendenza fisica Sviluppo di tolleranza Iperalgesia indotta da oppioidi Abuso e Dipendenza Deficit cognitivi Ipogonadismo (Disfunzioni sessuali, osteoporosi, depressione, fatica) Alterazioni del sistema immunitario (attraverso il sistema ipotalamo-ipofisi-surrene) riduce la produzione di anticorpi riduce l’attività delle cellule Natural Killer riduce l’espressione di citochine riduce l’attività fagocitaria
 Alterazioni del sistema immunitario (attraverso il sistema ipotalamo-ipofisi-surrene) riduce la produzione di anticorpi. riduce l’attività delle cellule Natural Killer. riduce l’espressione di citochine. riduce l’attività fagocitaria.")
31
Opioid use for the management of pain in fibromyalgia is strongly discouraged and is not recommended by any current guideline.

33
women could be at higher risk for the negative medical and psychological effects of opioids because they have more persistent pain than men, and may be prescribed opioids more often and at higher doses than men multiple psychophysiological factors may contribute to certain risks and consequences of chronic opioid therapy risks in pregnancy and breast-feeding as in men, risks that are unique to women may increase concomitantly with greater exposure to opioids (in terms of frequency and dosage) as in men, risks for women appear to vary at different ages.
 as in men, risks for women appear to vary at different ages.")
34
GRAZIE PER LA VOSTRA ATTENZIONE

Presentazioni simili


















>")


>")