Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Mediterranean School of Oncology Director :Prof.Stefano Iacobelli
Impact of Patient Age on Treatment of CRC Advanced Course: Highlights in the Management of CRC Roma, 1-2 febbraio 2007 Domus Sessoriana Prof.I.Carreca Chair of Medical Oncology,Chief University of Palermo-Italy

2
Elderly people………..? Young old: years of age Older old: years of age Oldest old: over 85 years of age

3
Incidenza delle neoplasie proiezione per sesso ed età -
ITALIA 2000 proiezione per sesso ed età - Frequenza per (Verdecchia et al. EJC 2001)
")
4
Incidenza neoplasie nell’anziano Sedi più frequenti
Età aa 18,2 17,3 28,2 34,9 28,4 6,5 35,8 6,4 11,3 13 Uomini Donne Fonte: NCI SEER Program e NPCR

5
Incidenza neoplasie nell’anziano Sedi più frequenti
Età>75 aa 13,2 16,9 31,6 40 23,5 28,3 8,7 14,5 18,7 4,6 Uomini Donne Fonte: NCI SEER Program e NPCR

6
Average life expectancy 1580 - 2000
~ 30 yrs 54-84 ~ 11 yrs 43-54 ~ 7 yrs 36-43 Max Plank Institute for Demography, Rostock, Germany, Annual Report 2001

7
2003 Estimated US Cancer Cases*
Men 675,300 Women 658,800 Prostate 33% Lung & bronchus 14% Colon & rectum 11% Urinary bladder 6% Melanoma of skin 4% Non-Hodgkin lymphoma 4% Kidney 3% Oral Cavity 3% Leukemia 3% Pancreas 2% All Other Sites 17% 32% Breast 12% Lung & bronchus 11% Colon & rectum 6% Uterine corpus 4% Ovary 4% Non-Hodgkin lymphoma 3% Melanoma of skin 3% Thyroid 2% Pancreas 2% Urinary bladder 20% All Other Sites Now we will turn our attention to the number of new cancers anticipated in the US this year. It is estimated that 1.33 million new cases of cancer will be diagnosed in In men, cancers of the prostate, lung, colon & rectum, and urinary bladder will be diagnosed most often, whereas in women, cancers of the breast, lung, colon & rectum, and uterine corpus will be diagnosed most often. *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2003.

8
2003 Estimated US Cancer Deaths*
Men 285,900 Women 270,600 25% Lung & bronchus 15% Breast 11% Colon & rectum 6% Pancreas 5% Ovary 4% Non-Hodgkin lymphoma 4% Leukemia 3% Uterine corpus 2% Brain/ONS 2% Multiple myeloma 23% All other sites Lung & bronchus 31% Prostate 10% Colon & rectum 10% Pancreas 5% Non-Hodgkin 4% lymphoma Leukemia 4% Esophagus 4% Liver/intrahepatic 3% bile duct Urinary bladder 3% Kidney 3% All other sites 22% Lung cancer is, by far, the most common fatal cancer in men (31%), followed by prostate (10%), and colon & rectum (10%). In women, lung (25%), breast (15%), and colon & rectum (11%) are the leading sites of cancer death. ONS=Other nervous system. *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2003.
, followed by prostate (10%), and colon & rectum (10%). In women, lung (25%), breast (15%), and colon & rectum (11%) are the leading sites of cancer death. ONS=Other nervous system. *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society,")
9
ISTAT Oct 24, 2006 Nel 2003 la speranza di vita alla nascita è pari a 77,2 anni per gli uomini e a 82,8 per le donne con uno scostamento marginale rispetto all’anno prima (+0,1 per gli uni, -0,2 per le altre). Inoltre, stime su dati provvisori permettono di prevedere per gli anni 2004 e 2005, 77,7 e 77,8 anni per gli uomini, 83,7 e 84,3 anni per le donne.
. Inoltre, stime su dati provvisori permettono di prevedere per gli anni 2004 e 2005, 77,7 e 77,8 anni per gli uomini, 83,7 e 84,3 anni per le donne.")
10
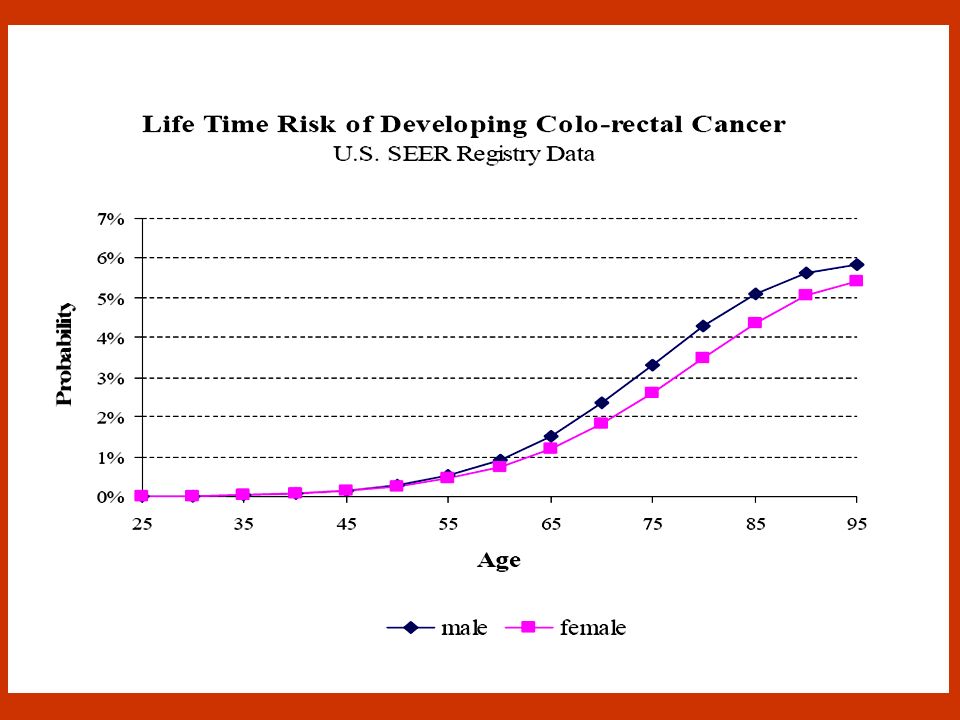
Cancer risk increases with age
30 25 20 15 10 5 Cumulative risk in European Union (%) 0–39 40–59 60–74 Age (years) Ferlay J, et al. Eucan IARC CancerBase. Lyon: IARC Press; Updated September 29, 2000.
 0–39 40–59 60–74. Age (years) Ferlay J, et al. Eucan IARC CancerBase. Lyon: IARC Press; Updated September 29,")
11
Cancer incidence and mortality + 65 vs - 65
30 20 10 –10 –20 –30 20 10 –10 –20 –30 ³65 ³65 <65 Change (%) Change (%) <65 Year Year Lyman G. Cancer Control. 1998;5:
 Change (%) < Year. Year. Lyman G. Cancer Control. 1998;5:")
12
Cancer incidence and mortality are increased in the elderly (>65 years)
Over 65 Under 65 Incidence Mortality 100 80 60 Cases (%) 40 20 Ovarian Breast NHL Lung Colorectal Ovarian Breast NHL Lung Colorectal Ferlay J, et al. Eucan IARC CancerBase. Lyon: IARC Press; Updated September 29, 2000. NHL = non-Hodgkin’s lymphoma
 Ovarian Breast NHL Lung Colorectal. Ovarian Breast NHL Lung Colorectal. Ferlay J, et al. Eucan IARC CancerBase. Lyon: IARC Press; Updated September 29, NHL = non-Hodgkin’s lymphoma.")
13
Impact of Aging on Cancer
Comorbidity Frailty Anemia Body&Metabolism Disfunctions PolyPharmacy It is an incontestable fact that most negative or neutral results are not published. Editors do not like them and readers find them boring. Thus the published results are mostly winners in the one in twenty lottery; i.e. purely accidental. Worse, there is now political censorship. Editors of once great journals, such as Nature, jump through hoops in order to prevent the publication of critiques of establishment dogma.

14
Comorbidity Prevalence in Cancer Patients by Age
60% Hypertension 50% Heart disease, moderate 40% High severity heart disease Percent 30% Diabetes Arthritis 20% Previous malignancy 10% Stroke/TIA COPD 0% 55-59 60-64 65-69 70-74 75-79 80-84 85+ Age Group Yancik R, Wesley M, Ries L, Havlik R, Edwards B, Yates, J, Effect of Age and Comorbidity in Cancer Patients, JAMA, 2001, Vol 285, No.7,

15
Curve di sopravvivenza in relazione all’indice di comorbilità di Charlson
100 % Score 0 Score 1 Score 2 Score 3 Anni di Follow-up

16
Frialty: Criteria Age > 85 years Dependence in one or more ADL
Presence of three or more comorbidities Presence of one or more geriatric syndromes

17
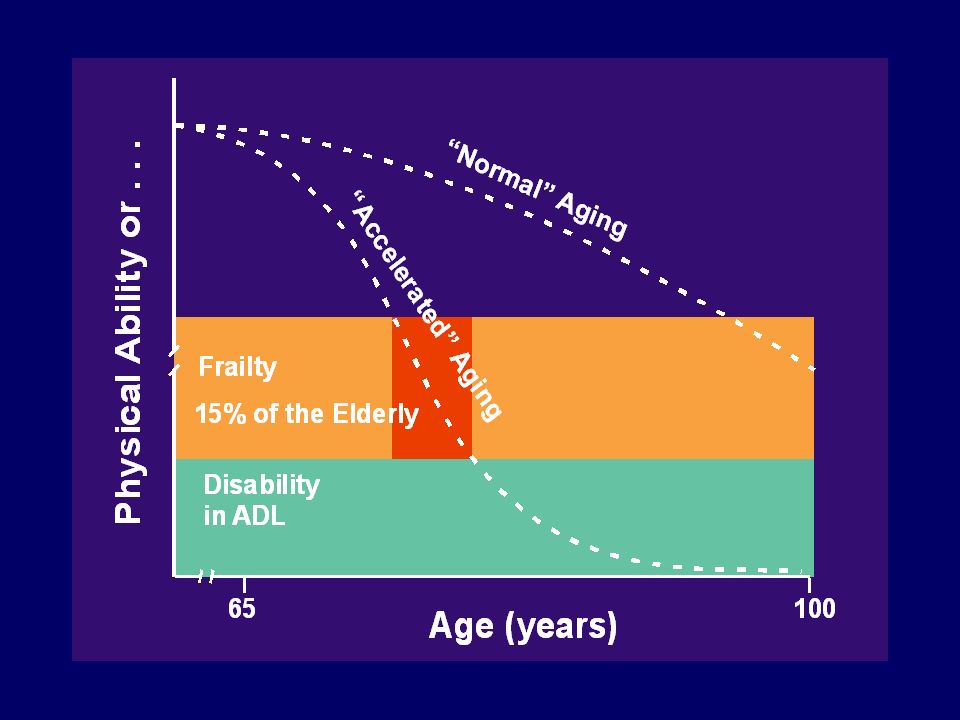
Aging, Frailty and Disease
Operational Definitions for Studies on Aging Aging Slow, Harmonic Decline of Integrity and Disability Threshold Function of Multiple Physiologic Subsystems Frailty Accelerated, Harmonic Decline of Integrity and Disability Threshold Function of Multiple Physiologic Subsystems Disease Rapid Decline of Integrity and Function Disability Threshold of Selected Physiologic Subsystems Time

19
Physiologic reserve - Hypothetical Trajectory to Illness, Functional Limitation & Disability
hip fracture pneumonia congestive heart failure Functional limitation Physiologic reserve Disability Younger age Older age Time

20
Overlap of Frailty with chronic diseases: a role for subclinical disease ?
Disability Comorbidity Frailty

21
Anemia: An Indipendent Risk Factor for Death
Mortality risk is significantly increased in individuals aged >70 years with anemia1 This increased risk is indipendent of diseases at baseline, or functional impairment1 Other data indicate that mortality is also increased in elderly individuals >65 years2 Izaks G, et al JAMA. 1999;281: Ania B, et al. J Am Geriatr Soc 1997;45:

22
Marrow reserves 70% fat - elderly Cellularity 30% fat - young
50% fat - normal 70% fat - elderly

23
Aging affects chemotherapy toxicity and effectiveness
Pharmacokinetic changes that increase toxicity decreased volume of distribution (Vd) decreased glomerular filtration rate (GFR) decreased hepatic metabolism decreased intestinal absorption Pharmacodynamic changes that limit effectiveness increased expression of multidrug resistance (MDR) gene decreased apoptosis increased tumour anoxia decreased cell proliferation Balducci L, Carreca I, et al Oncologist. 2000;5:
 decreased glomerular filtration rate (GFR) decreased hepatic metabolism. decreased intestinal absorption. Pharmacodynamic changes that limit effectiveness. increased expression of multidrug resistance (MDR) gene. decreased apoptosis. increased tumour anoxia. decreased cell proliferation. Balducci L, Carreca I, et al Oncologist. 2000;5:")
24
Drug distribution and absorption
Marrow reserves

25
Physiological Aging-related Changes (20 to 80 yrs)
test change Body weight/fat + 35% Plasmatic volume - 8% Albumine - 10% globulins Total body water - 17% Extracellular fluids - 40% Cardiac electric stym/velocity - 20% Cardiac capacity Ejection fraction - 35% Vital capacity - 60% glomerular filtration - 50% Renal/GI ematic circulation

30
Survival of colorectal cancer elderly patients following surgical resection by serum IL-6 concentration But not an independent prognostic indicator – correlated with tumor size, stage, & metastasis From Chung & Chang, J Surg Oncol, 2003

31
A NEGLECTED ISSUE: POLYPHARMACY
RISK OF DRUG INTERACTIONS INCREASES BY ABOUT 7-13%% PER DRUG USED, i.e. 100% risk at the 8th drug Karas S Ann Emerg Med, 2001;10:627–30

32
Polifarmacia L’impiego di piu’ farmaci per pazienti con una o piu’ patologie. Somministrazione di piu’ farmaci spesso concomitante per il trattamento della stessa patologia. Utilizzazione di formulazioni farmaceutiche che comprendono piu’ principi attivi. L’impiego di farmaci senza una apparente indicazione terapeutica. Trattamento degli effetti collaterali come una “nuova” patologia.

33
Other Factors Influencing Toxicities:
Polypharmacy: On average, adults over the age of 65 use 2-6 prescribed medications and 1-3 non-prescribed medications Drugs used to treat other health problems may interfere with chemotherapy regimens

34
BMJ, 2002, 324:1497

35
Fattori che contribuiscono alla polifarmacia
Numero di patologie croniche Sesso Terapie prescritte da piu’ medici ad es. specialisti. Automedicazione con farmaci prescritti e OTC. Aumentata mobilita’ degli anziani. Messaggi pubblicitari diretti al consumatore. Richieste da parte dei caregivers o personale infermieristico. Prescrizioni telefoniche del medico. I medici sono riluttanti a sospendere terapie prescritte da altri medici. Raramente la terapia farmacologica e’ sottoposta a revisioni periodiche. "Start slow, Go slow" puo’ portare a somministrazioni sottodosate di farmaci con insuccesso terapeutico.

36
Comprehensive geriatric assessment reveals stages of aging
Group 1 functionally independent, no serious comorbidity standard cancer treatment Group 2 partially dependent, £2 comorbid conditions modified cancer treatment Group 3 dependent, ³3 comorbid conditions, any geriatric syndrome palliative treatment Balducci L, et al. Oncologist. 2000;5:

37
Comprehensive Geriatric Assessment (CGA)
Dependence ADL IADL Bathing Dressing Toileting Transfer Continence Feeding Using telephone Shopping Cooking House keeping Laundry Trasportation Medication Handling finances Comorbidity (Charlson scale) Cardiovascular diseases Respiratory diseases Hepatic impairment Renal impairment Other major organ failures Hematological malignancies Metastatic solid tumors AIDS Cognition (Mini Mental Status Examination) Memory Orientation Comprehension Logical thinking Geriatric Syndromes Dementia Delirium Severe depression Frequent falls Spontaneous fractures Poor Nutrition (causes) Anorexia/cachexia Depression Bad dentition Cognitive impairment Functional impairment Lack of caregivers Toxicity of chemotherapy Polipharmacy (causes) Long-term medications Unecessary prescriptions Increased risk of interactions
 Cardiovascular diseases. Respiratory diseases. Hepatic impairment. Renal impairment. Other major organ failures. Hematological malignancies. Metastatic solid tumors. AIDS. Cognition. (Mini Mental Status Examination) Memory. Orientation. Comprehension. Logical thinking. Geriatric Syndromes. Dementia. Delirium. Severe depression. Frequent falls. Spontaneous fractures. Poor Nutrition. (causes) Anorexia/cachexia. Depression. Bad dentition. Cognitive impairment. Functional impairment. Lack of caregivers. Toxicity of chemotherapy. Polipharmacy. (causes) Long-term medications. Unecessary prescriptions. Increased risk of interactions.")
38
Comprehensive Geriatric Assessment (CGA) Life-prolonging treatment
Group 1 Group 2 Group 3 (frial elderly) Life expectancy >Cancer <Cancer Treatment tolerance Life-prolonging treatment Yes Palliation No Balducci L, et al. Oncologist. 2000;5: AlphaMed Press
 Life expectancy. >Cancer. <Cancer. Treatment tolerance. Life-prolonging treatment. Yes. Palliation. No. Balducci L, et al. Oncologist. 2000;5: AlphaMed Press")
39
To Treat or Not To Treat ELDERLY PATIENTS ?

40
Proporzione di pazienti anziani (>65 aa) arruolati in studi clinici controllati su terapie di diversi tipi di cancro, rispetto alla proporzione di anziani con la stessa patologia nella popolazione generale (Hutchins LF, NEJM 1999)
")
41
EVIDENCE-BIASED MEDICINE
Elderly are almost systematically excluded from controlled studies. Even if included, these studies show comparative efficacy of only some types of treatment, for an “average” randomized patient. Sir John Grimley Evans University of Oxford Il grande vecchio è davvero un buco nero per la farmacologia clinica? Gambassi et al. Giornale di Gerontologia 1999;47:51-5 The exclusion of older cancer patients from clinical trials Gambassi et al. RAYS 1999;24:26-31

42
Percentuale di articoli originali su studi clinici (tot
Percentuale di articoli originali su studi clinici (tot. 1012) pubblicati su BMJ, Gut, Lancet, Thorax in 12 mesi riportanti dati ottenuti su pazienti anziani Specifico su anziani (>75 aa) % Esclude anziani in maniera giustificabile % Esclude anziani in maniera non giustificabile % Non specifica i limiti di età % Tra il 1966 ed il 1996 sono stati pubblicati solo 50 studi clinici specificamente disegnati per il paziente anziano, soprattutto nell’ipertensione (13), neuropsichiatria (11) e patologie cardiologiche (7)
 pubblicati su BMJ, Gut, Lancet, Thorax in 12 mesi riportanti dati ottenuti su pazienti anziani. Specifico su anziani (>75 aa) 3% Esclude anziani in maniera giustificabile 8% Esclude anziani in maniera non giustificabile 35% Non specifica i limiti di età 54% Tra il 1966 ed il 1996 sono stati pubblicati solo 50 studi clinici specificamente disegnati per il paziente anziano, soprattutto nell’ipertensione (13), neuropsichiatria (11) e patologie cardiologiche (7)")
43
UNDER-REPRESENTATION OF ELDERLY PTS WITH ADV. CRC IN CT TRIALS
8.0 yrs 6.4 yrs The median age of CRC pts enrolled in RCT remained constant (62.0 and 62.2 yrs), whilst the median age of the CRC population increased from 68.4 to 70.2 yrs Jennens RR et al., Intern Med J Apr;36(4):
, whilst the median age of the CRC population increased from 68.4 to 70.2 yrs. Jennens RR et al., Intern Med J Apr;36(4):")
44
Undertreatment in elderly patients
Aggressive lymphoma older patients less likely to be treated for cure, less likely to survive for 5 years Breast cancer older women less likely to be invited into clinical trials Stage III colon cancer older patients less likely to receive chemotherapy Lung cancer older patients receive delay in diagnosis and less aggressive treatment Chen C, et al. Leuk Lymphoma. 2000;38: Kemeny M, et al. Proc Am Soc Clin Oncol. 2000; 19:602a, Abstract 237I. Mahoney T, et al. Arch Surg. 2000;135: Peake M. Presentation at 96th International Conference of Am Thoracic Soc, Toronto, May 2000.

45
PFS/DFS by STUDY and AGE GROUP
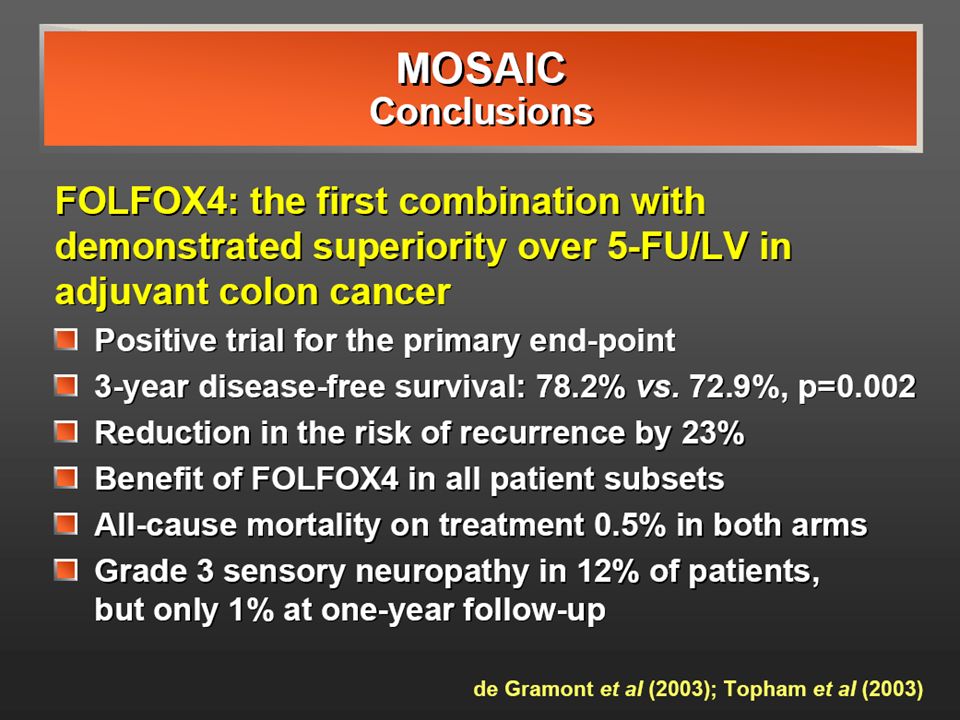
<70 yrs >=70 yrs CONCLUSION: FOLFOX4 maintains its efficacy and safety ratio in selected elderly pts with colorectal cancer. Its judicious use should be considered without regard to age, although scant data are available among pts older than 80 yrs. (Goldberg R et al., JCO 2006; 2:4: , modif.)
")
46
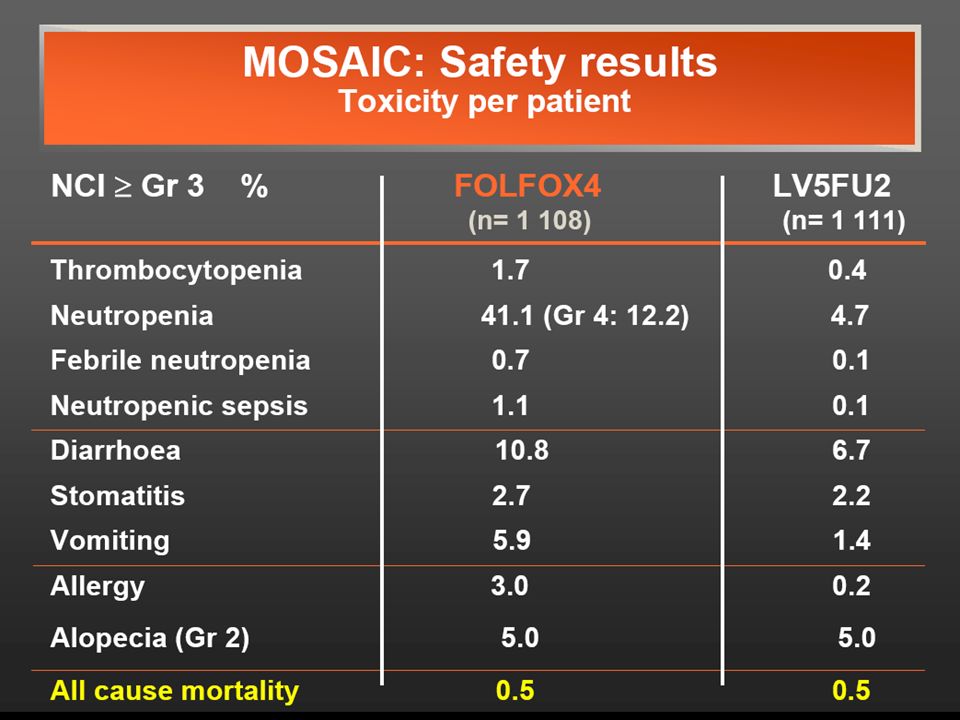
Incidenza di mucosite CHEMIOTERAPIA *(%) High-dose 75-100
Standard-dose 40 RADIOTERAPIA frequente nel corso di cure palliative comune in pazienti pediatrici e anziani (incidenza 3-5 volte superiore che nell’adulto)
")
47
Renal function Cockcroft-Gault equation: Kintzel and Dorr formula:

56
In clinical practice….. Selezione del paziente mediante valutazione
geriatrica completa. Adattamento della dose iniziale ( funzionalità renale e cardiaca ). Mantenimento dei livelli di Hb > 12g/dL con Epo Attuazione tempestiva di adeguata idratazione per controllare la mucosite. In età > 65 anni uso profilattico dei CSF per tossicità ematologica moderata-intensa.
. Mantenimento dei livelli di Hb > 12g/dL con Epo. Attuazione tempestiva di adeguata idratazione per. controllare la mucosite. In età > 65 anni uso profilattico dei CSF per tossicità. ematologica moderata-intensa.")
57
To Treat or Not To Treat ELDERLY PATIENTS ?

58
To Treat or Not To Treat ELDERLY PATIENTS YES,WE DO..

60
…Message to take home.. Age is not a contraindication to full-dose therapy Main limiting factors poor overall health and function presence of comorbidities Elderly are more susceptible to myelotoxicity In elderly with good performance status, equal treatment yields equal benefit Prophylactic use of G-CSF helps maintain chemotherapy dose intensity

Presentazioni simili




 Brussels, 26 settembre 2013.>")

















