Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Paolo Maggi Clinica delle Malattie Infettive Università degli Studi di Bari
HIV e rene

2
Prevalence of different non-AIDS related co-morbidities at different age strata in naive patients
Dec 2014 Report

3
Prevalence of different non-AIDS related co-morbidities at different age strata in ART-treated patients Dec 2014 Report

5
Giandomenico Tiepolo (1727-1804): Il mondo nuovo
: Il mondo nuovo")
8
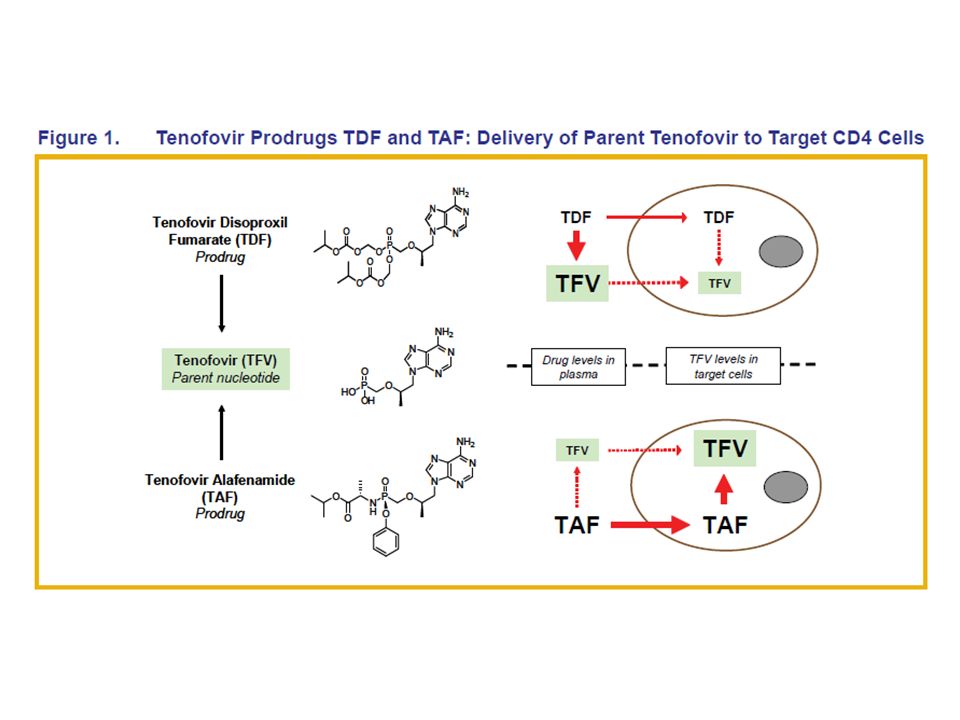
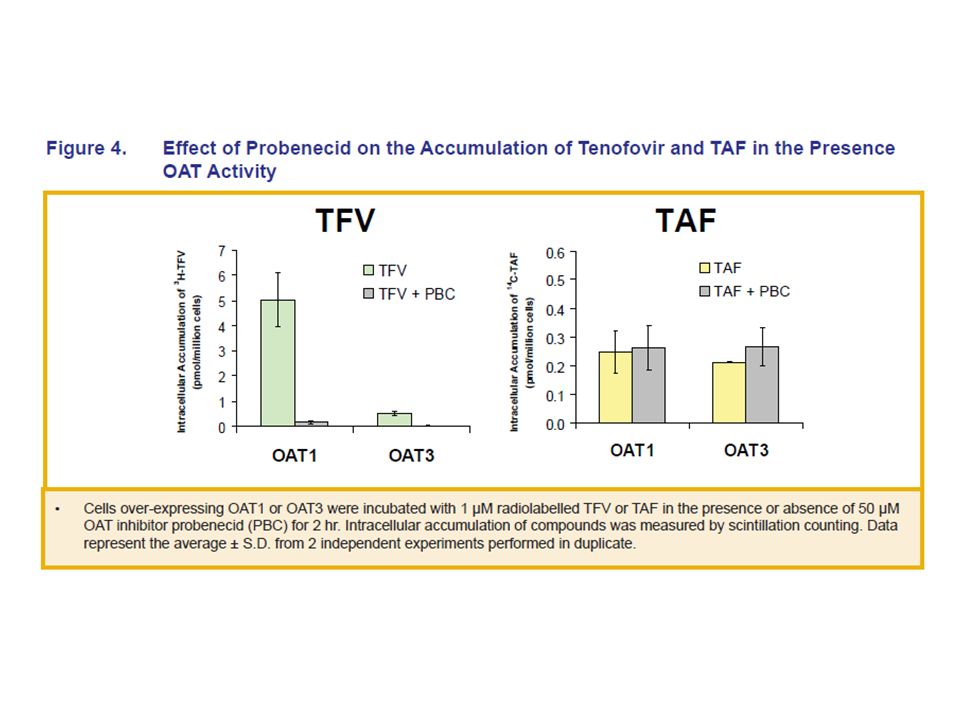
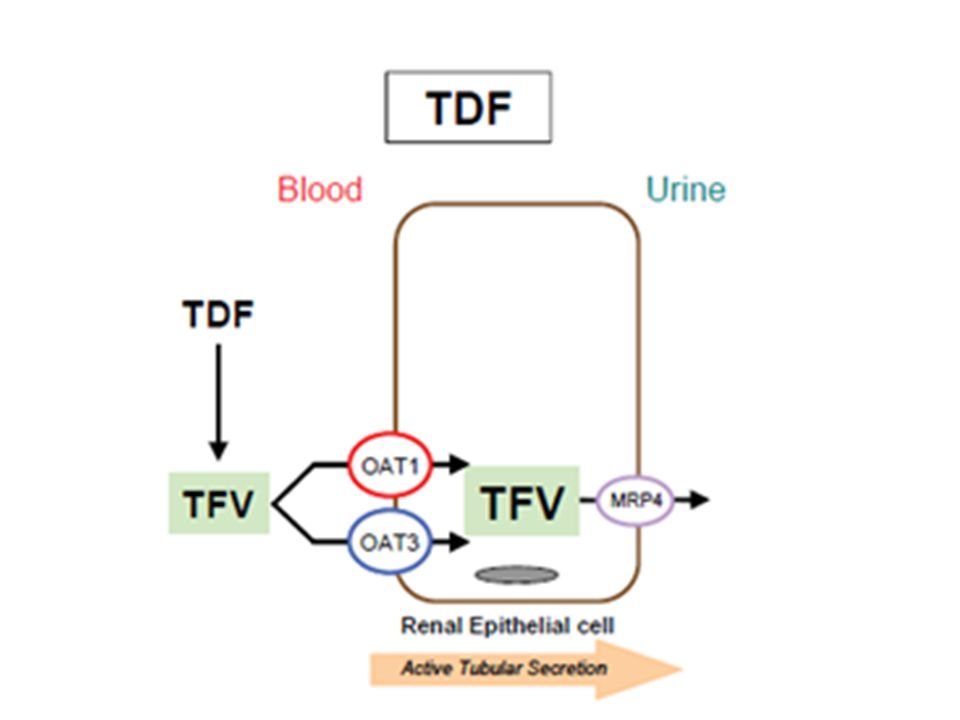
Proposed mechanism of TDF excretion
Blood Proximal tubule Tubular Renal cell Nucleotide analogues tenofovir, adefovir, cidofovir To make simple a complicated matter, this is due to a play f molecular carriers: the drug enters rapidly, but the exit is slow. This generates a selective concentration of the drug, a bottle nek that produces a mithocondrial toxicity in spite of the relatively low mithocondrial toxicity of the drug. TDF-related nephropathy is mediated by intracellular accumulation in the proximal renal tubules that leads to mitochondrial injury and mtDNA depletion (Kohler et al., 2009). hOATP 1-3 MRP2 Nucleotide analogues excretion Animation based on Izzedine H et al., Nat Rev Nephrol. 2009;5:563-73 8
. hOATP 1-3. MRP2. Nucleotide analogues excretion. Animation based on Izzedine H et al., Nat Rev Nephrol. 2009;5:")
21
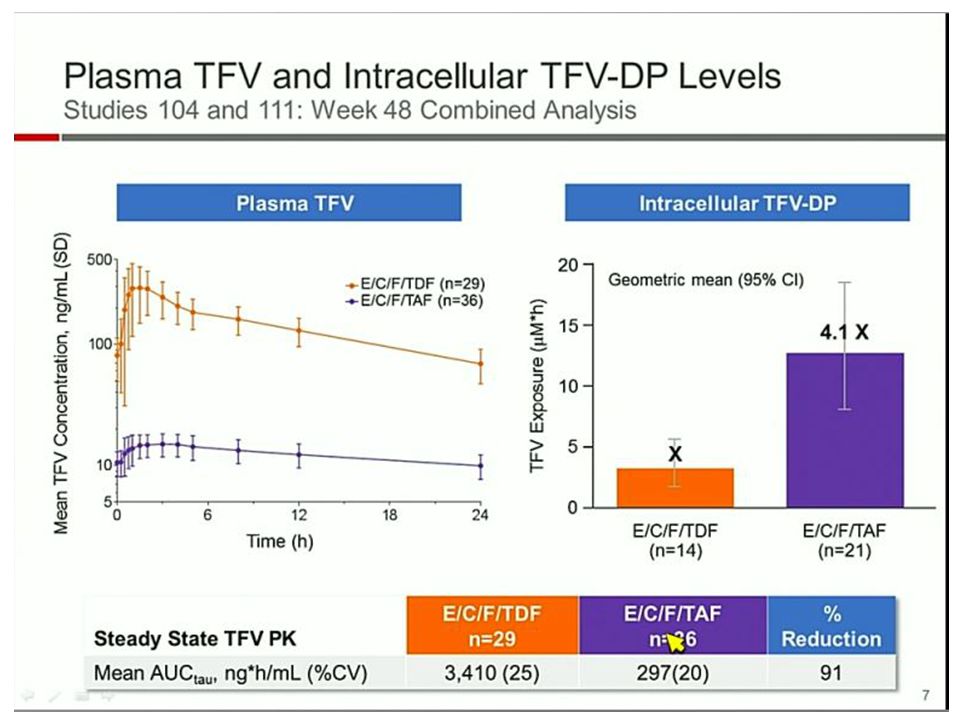
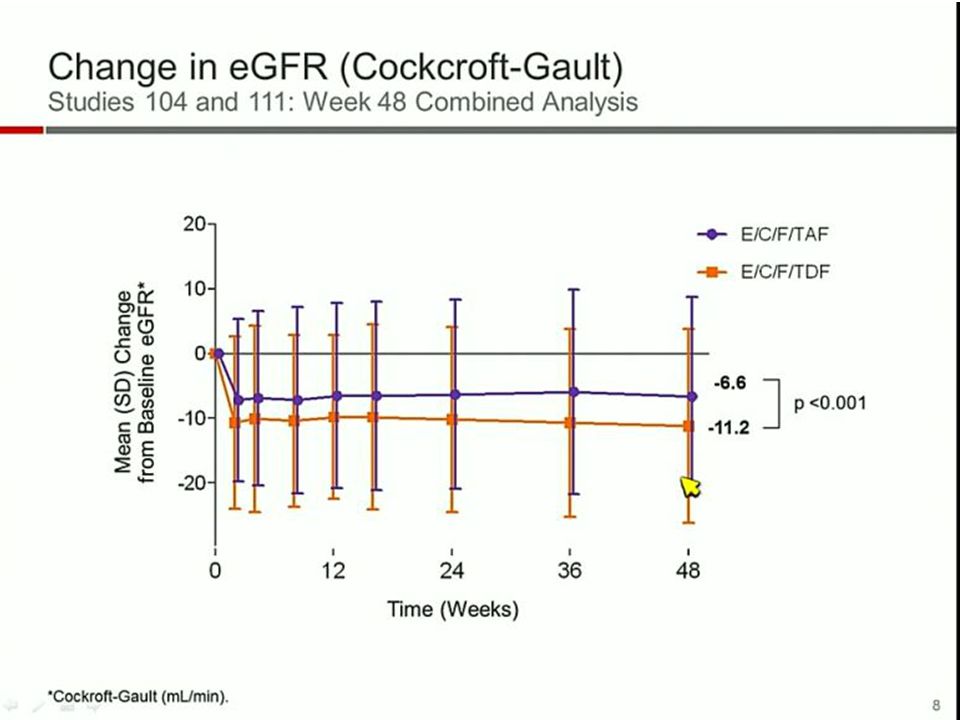
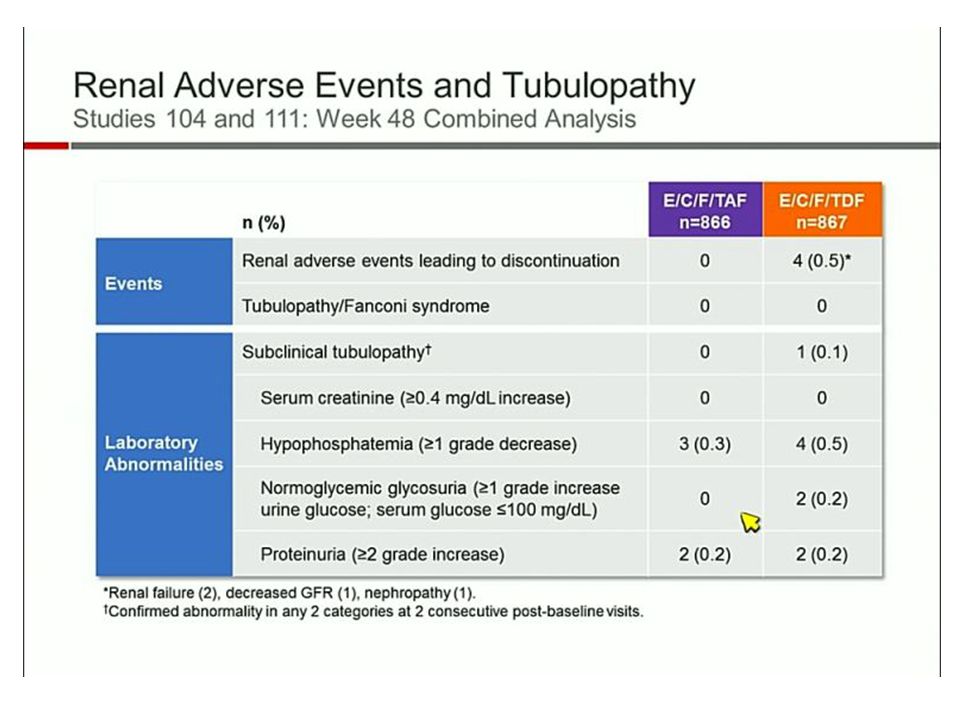
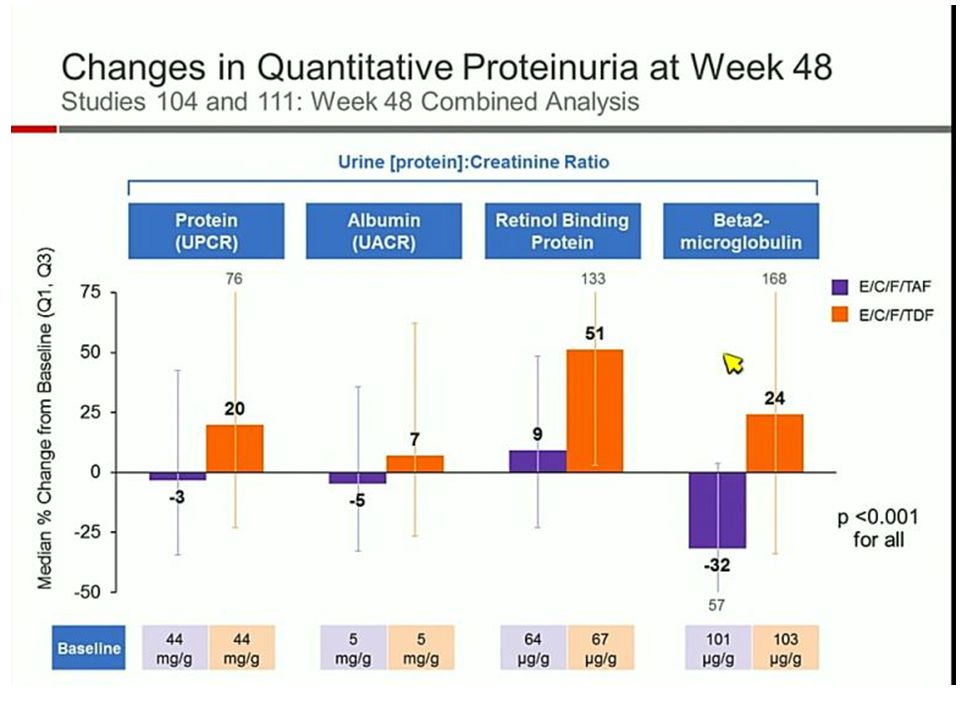
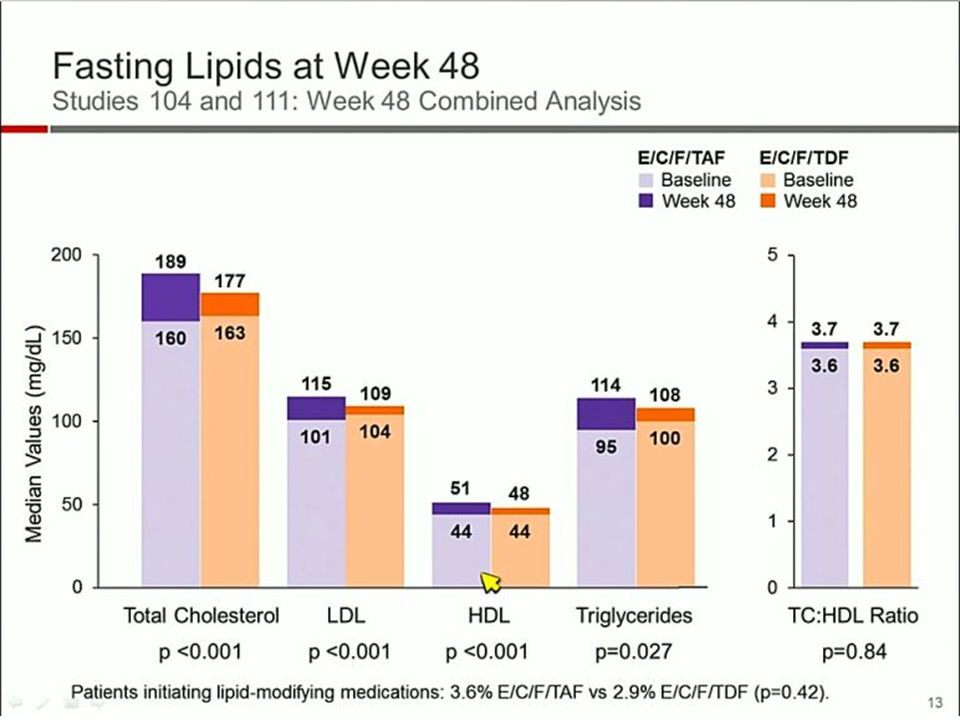
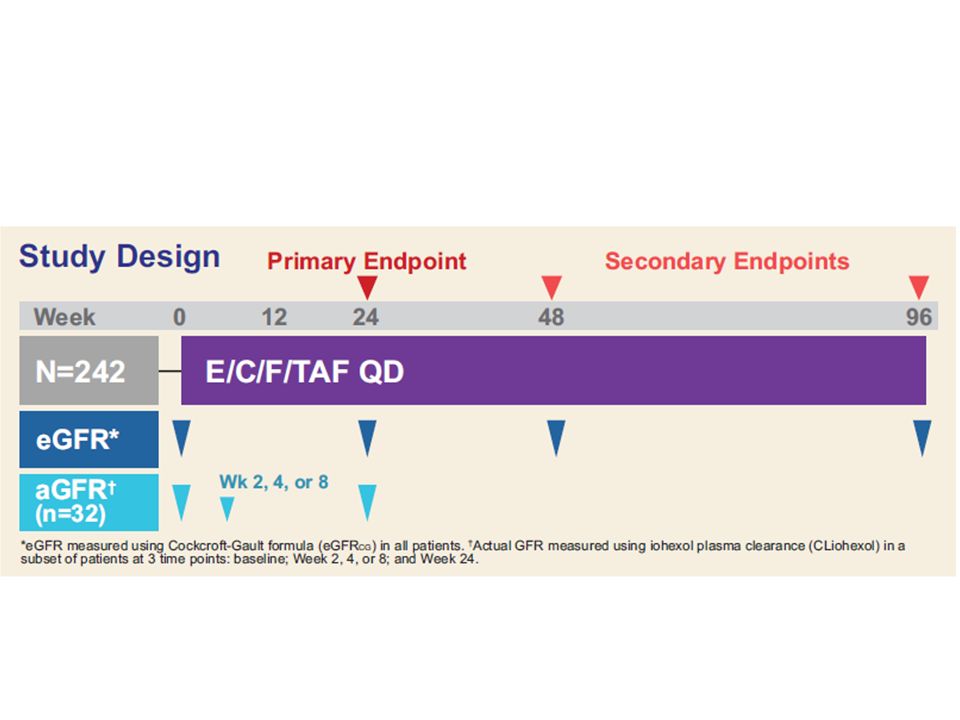
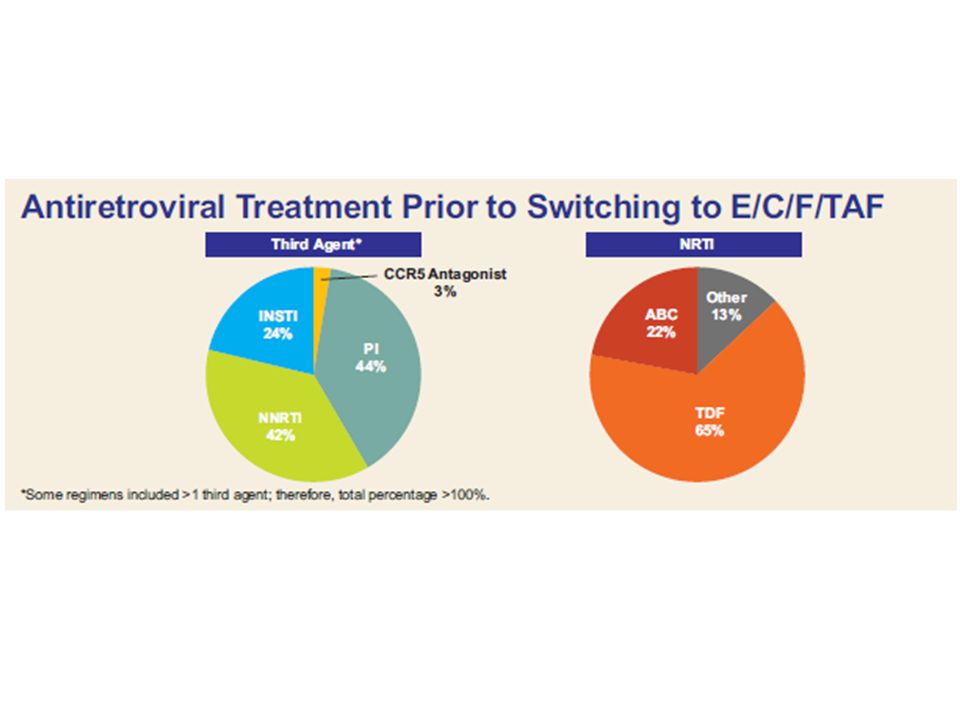
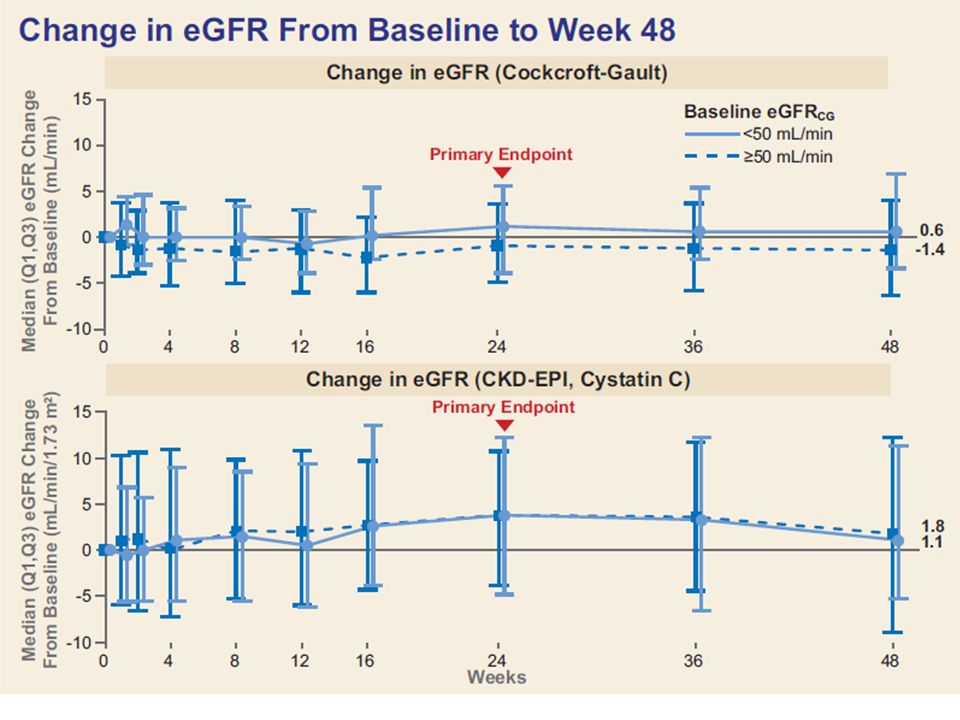
Poster # 795 Safety of Tenofovir Alafenamide in Renal Impairment Anton Pozniak

29
Classic risk factors: age genetic
high blood pressure diabetes

30
Prevalence of different non-AIDS related co-morbidities at different age strata in ART-treated patients Dec 2014 Report

31
Virus Drugs

32
No. of patients with events
SMART Study: Short-term CD4+ guided episodic use of ART is inferior to continuous therapy CD4+ guided drug conservation (DC) strategy was associated with significantly greater disease progression or death compared with continuous viral suppression (VS): RR 2.5 (95% CI: 1.8–3.6; p<0.001) Includes increased CVD-, liver- and renal-related deaths and non-fatal CVD events Severe complications endpoint and components Subgroups No. of patients with events Relative Risk 95% CI 1.5 Severe complications 114 1.4 CVD, liver, renal deaths 31 HIV infection , chronic inflammation is per se a major co-factor in kidney diseas and other co-morbidities, and SMART study represented, to me, an impressive proof of concept: as you will remember, paient that stopped HAART increased dramatically the odd risk of comorbidities. Many died for MI, but the higher odd was for the non fatal renal events. 1.5 Non-fatal CVD events 63 1.4 Non-fatal hepatic events 14 Non-fatal renal events 7 2.5 0.1 Favours DC Favours VS 10 El-Sadr W, et al. 13th CROI, Denver 2006, #106LB
 strategy was associated with significantly greater disease progression or death compared with continuous viral suppression (VS): RR 2.5 (95% CI: 1.8–3.6; p<0.001) Includes increased CVD-, liver- and renal-related deaths and non-fatal CVD events. Severe complications endpoint and components. Subgroups. No. of patients with events. Relative Risk. 95% CI Severe complications CVD, liver, renal deaths. 31. HIV infection , chronic inflammation is per se a major co-factor in kidney diseas and other co-morbidities, and SMART study represented, to me, an impressive proof of concept: as you will remember, paient that stopped HAART increased dramatically the odd risk of comorbidities. Many died for MI, but the higher odd was for the non fatal renal events Non-fatal CVD events Non-fatal hepatic events. 14. Non-fatal renal events Favours DC. Favours VS. 10. El-Sadr W, et al. 13th CROI, Denver 2006, #106LB.")
33
AIDS October 23, Volume 28 - Issue 16 Renal epithelial cells produce and spread HIV-1 via T-cell contact Blasi M et al. Objectives:Increasing evidence supports the role of the kidney as a reservoir for HIV-1. In-vitro co-cultivation of HIV-infected T cells with renal tubule epithelial (RTE) cells results in virus transfer to the latter, whereas cell-free virus infection is inefficient. We further characterized the fate of HIV-1 after it is internalized in renal epithelial cells. Methods:Primary or immortalized CD4+ cells were infected with a green fluorescent protein (GFP)-expressing replication competent HIV-1. HIV-1 transfer from T cells to RTE cells was carried out in a co-culture system and evaluated by fluorescence-activated cell sorting analysis. HIV-1 integration in renal cells was evaluated by Alu-PCR and the production of infectious particles was assessed by p24-ELISA and TZM-bl assay. HIV-infected renal cells were used as donor cells in a co-culture system to evaluate their ability to transfer the virus back to T cells. Results:Renal cells become productively infected by HIV-1 and multiple copies of HIV-1 can be transferred from infected T cells to renal cells. Two separate cell populations were identified among infected renal cells based on reporter gene GFP expression level (low vs. high), only the high showing sensitivity to azidothymidine and ritonavir. Co-cultivation of HIV-1-infected renal cells with noninfected T cells resulted in HIV-1 transmission to T cells, supporting bidirectional exchange of virus between T cells and kidney-derived cells. Persistent expression and generation of infectious virus in renal cells required HIV integration. Conclusion:These results support the kidney as a potential reservoir where virus is exchanged between interstitial T cells and RTE cells
 cells results in virus transfer to the latter, whereas cell-free virus infection is inefficient. We further characterized the fate of HIV-1 after it is internalized in renal epithelial cells. Methods:Primary or immortalized CD4+ cells were infected with a green fluorescent protein (GFP)-expressing replication competent HIV-1. HIV-1 transfer from T cells to RTE cells was carried out in a co-culture system and evaluated by fluorescence-activated cell sorting analysis. HIV-1 integration in renal cells was evaluated by Alu-PCR and the production of infectious particles was assessed by p24-ELISA and TZM-bl assay. HIV-infected renal cells were used as donor cells in a co-culture system to evaluate their ability to transfer the virus back to T cells. Results:Renal cells become productively infected by HIV-1 and multiple copies of HIV-1 can be transferred from infected T cells to renal cells. Two separate cell populations were identified among infected renal cells based on reporter gene GFP expression level (low vs. high), only the high showing sensitivity to azidothymidine and ritonavir. Co-cultivation of HIV-1-infected renal cells with noninfected T cells resulted in HIV-1 transmission to T cells, supporting bidirectional exchange of virus between T cells and kidney-derived cells. Persistent expression and generation of infectious virus in renal cells required HIV integration. Conclusion:These results support the kidney as a potential reservoir where virus is exchanged between interstitial T cells and RTE cells.")
34
#793 Spectrum of HIV-Associated Kidney Disease in the Era of Combination Antiretroviral Therapy John Booth We reviewed consecutive renal biopsies ( ) of HIV+ patients attending eight clinics in the UK. This is the first study to demonstrate a relationship between HIV replication and ICKD (immune complex kidney disease) . Compared to HIVAN, ICKD was associated with less advanced immunodeficiency and a lower rate of progression to ESKD. The observed association with HIV viraemia for both ‘core’ ICKD and HIVAN may imply a pathogenetic role of HIV replication and its associated immune activation; it also suggests that suppressive ART may reduce the risk of developing these types of kidney disease
 . Compared to HIVAN, ICKD was associated with less advanced immunodeficiency and a lower rate of progression to ESKD. The observed association with HIV viraemia for both ‘core’ ICKD and HIVAN may imply a pathogenetic role of HIV replication and its associated immune activation; it also suggests that suppressive ART may reduce the risk of developing these types of kidney disease.")
35
797. Kidney Dysfunction and Markers of Inflammation in the Multicenter AIDS Cohort Study Alison G. Abraham Higher circulating levels of immune activation markers among treated HIV+ individuals, despite virologic suppression, may partially explain their higher burden of kidney dysfunction compared to HIV- persons

36
HCV I pazienti co-infetti hanno una prognosi renale peggiore. La presenza di crioglobuline è un fattore prognostico di aumentata mortalità Fabrizi, F. et al. Hepatitis C virus increases the risk of kidney disease among HIV-positive patients: Systematic review and meta-analysis. J Med Virol [Epub ahead of print]

37
I nuovi farmaci: Cobicistat Dolutegravir (e rilpivirina)
")
38
Recettori tubulari e farmaci:
Inibizione passiva Inibizione attiva

40
Recettori tubulari e farmaci:
Inibizione passiva Inibizione attiva

41
Recettori tubulari e farmaci:
Inibizione passiva Inibizione attiva

42
COBI Inhibits Active Tubular Secretion of Creatinine, Resulting in Increased SCr1,2
Preclinical studies indicate that COBI blocks a transport pathway used for creatinine secretion from the proximal tubule by inhibiting a transport protein called MATE1 that is responsible for transporting creatinine into the proximal tubule1-3 Other drugs have been reported to block tubular secretion of creatinine, such as ritonavir, cimetidine, and trimethoprim4-6 Creatinine Cobicistat Proximal Tubule Cell SCr ≈ 1.0 mg/dL SCr ≈ 1.14 mg/dL OCT2 MATE1 Cr Filtered From Glomerulus Blood Vessel Urinary Space For illustrative purposes only. For illustrative purposes only. For illustrative purposes only. 1 Lepist EI, et al. ICAAC Abstract A1-1724; 2 German P, et al. J Acquir Immune Defic Syndr. 2012;61:32-40; 3 Lepist EI, Ray AS. Expert Opin Drug Metab Toxicol. 2012;8: ; 4 Cohen C, et al. CROI San Francisco, CA. 58LB; 5 Andreev E, et al. J Intern Med. 1999;246: ; 6 Naderer O, et al. Antimicrob Agents Chemother. 1997;41: 42

44
In ultimo, 3 FAQ: 1) Che fare nella pratica clinica quotidiana?
 Che fare nella pratica clinica quotidiana")
45
La misurazione della funzionalità renale…

46
Formule per la stima del GFR III. CKD-EPI
eGFR = 141 * min(SCr/k, 1)a * max(SCr/k, 1)-1,209 * 0,993Età * 1,018 (F) * 1,159 (B) k = 0,7 (F), 0,9 (M) a -0,329 (F), -0,411 (M) Valutazione del GFR con metodo di riferimento Inclusi soggetti con valori normali di GFR Calcolo basato su creatininemia Non validata in altre razze Non accuratezza della misurazione della creatinina a bassa concentrazione (< 1 mg/dl)
a * max(SCr/k, 1)-1,209 * 0,993Età * 1,018 (F) * 1,159 (B) k = 0,7 (F), 0,9 (M) a -0,329 (F), -0,411 (M) Valutazione del GFR con metodo di riferimento. Inclusi soggetti con valori normali di GFR. Calcolo basato su creatininemia. Non validata in altre razze. Non accuratezza della misurazione della creatinina a bassa concentrazione (< 1 mg/dl)")
47
Performance delle formule per calcolare l’eGFR
Levey As et al. Ann Intern Med 2009; 150:

48
Bias di misurazione della Creatinina
Peake & Whiting, Clin Biochem Rev 2006;

49
2) Esistono metodiche alternative di valutazione della funzione renale?
 Esistono metodiche alternative di valutazione della funzione renale")
50
Cistatina C Pros Cons Polipeptide di 13 kD prodotto da tutte le cellule nucleate Conc. Plasmatica indipendente da massa muscolare, sesso e razza Filtrata dal glomerulo in assenza di quota di secrezione tubulare Non interferenze nei metodi analitici Aumentata produzione per: Steroidi ad alte dosi Neoplasie Stati infiammatori acuti e cronici Ipertiroidismo Carica virale sistemica (HIV) Tabacco
 Tabacco.")
51
Cistatina C e infezione da HIV
Controlli (193) p eGFR (MDRD) 104 93 < 0.001 Cocroft-Gault 118 106 eGFR (Cys) 99 120 r p Cys vs. HIV mRNA 0.33 < 0.01 Cys vs. CD4 - 0.29 Mauss S et al; Antiv Ther 2008; 13:1091-5
 p. eGFR (MDRD) < Cocroft-Gault eGFR (Cys) r. p. Cys vs. HIV mRNA < Cys vs. CD Mauss S et al; Antiv Ther 2008; 13:")
52
Accuratezza di eGFRcys e CD4
Gagneux-Brunon A et al; AIDS 2013; 27

53
Formule per eGFR in HIV Accuratezza 30% MDRD 75% CKD-EPI 82%
CDK-EPICys 80% CKD-EPImix 81% Gagneux-Brunon A et al; AIDS 2013; 27

54
Monitoraggio clinico della “funzione renale”
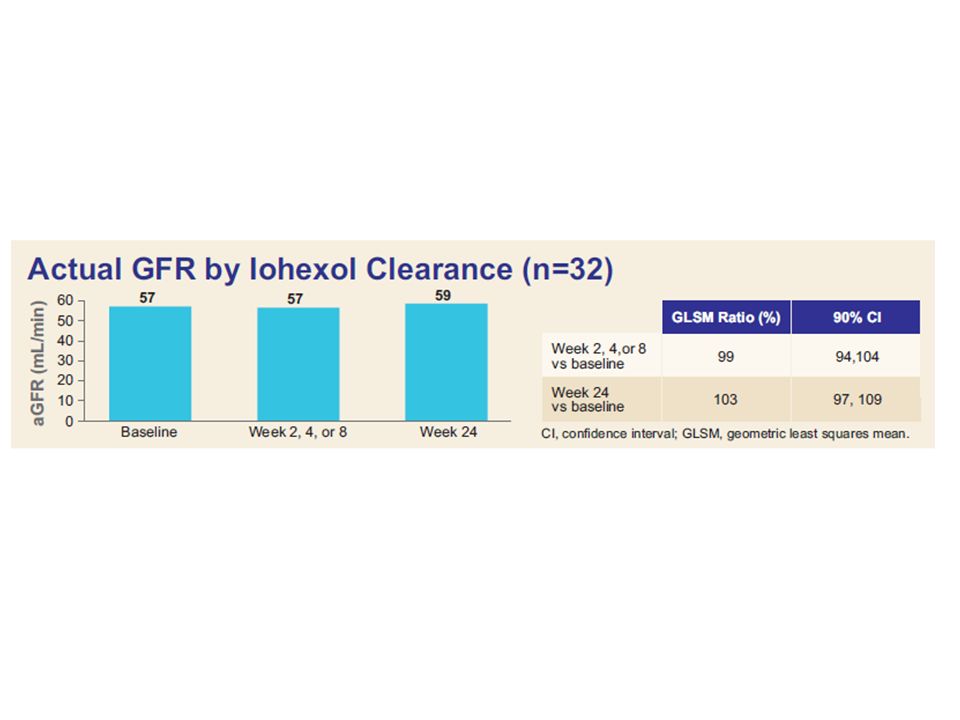
Valutazione della velocità di filtrazione glomerulare (GFR) Misurazione del GFR Clearance renale della Inulina o Iotalamato Clearance plasmatica dello Ioexolo o 51Cr-EDTA
 Misurazione del GFR. Clearance renale della Inulina o Iotalamato. Clearance plasmatica dello Ioexolo o 51Cr-EDTA.")
55
3) Qual è il ruolo della funzione tubulare?
 Qual è il ruolo della funzione tubulare")
56
proteine a basso pm fosforo glucosio acido urico

57
Valutazione qualitativa della proteinuria
Proteinuria glomerulare Danno della MBG (strutturale, funzionale) Prevalentemente Albumina Albumina/Proteine urinarie > 0,4 Proteinuria tubulare Polipeptidi a basso peso molecolare (< 25 kD) Scarsa quantità di Albumina Albumina/Proteine urinarie < 0,4 Dosaggio immunometrico di proteine a basso peso molecolare [Retinol-binding protein, b2-microglobulina, a1-microglobulina, Cistatina C, NGAL]
 Prevalentemente Albumina. Albumina/Proteine urinarie > 0,4. Proteinuria tubulare. Polipeptidi a basso peso molecolare (< 25 kD) Scarsa quantità di Albumina. Albumina/Proteine urinarie < 0,4. Dosaggio immunometrico di proteine a basso peso molecolare [Retinol-binding protein, b2-microglobulina, a1-microglobulina, Cistatina C, NGAL]")
58
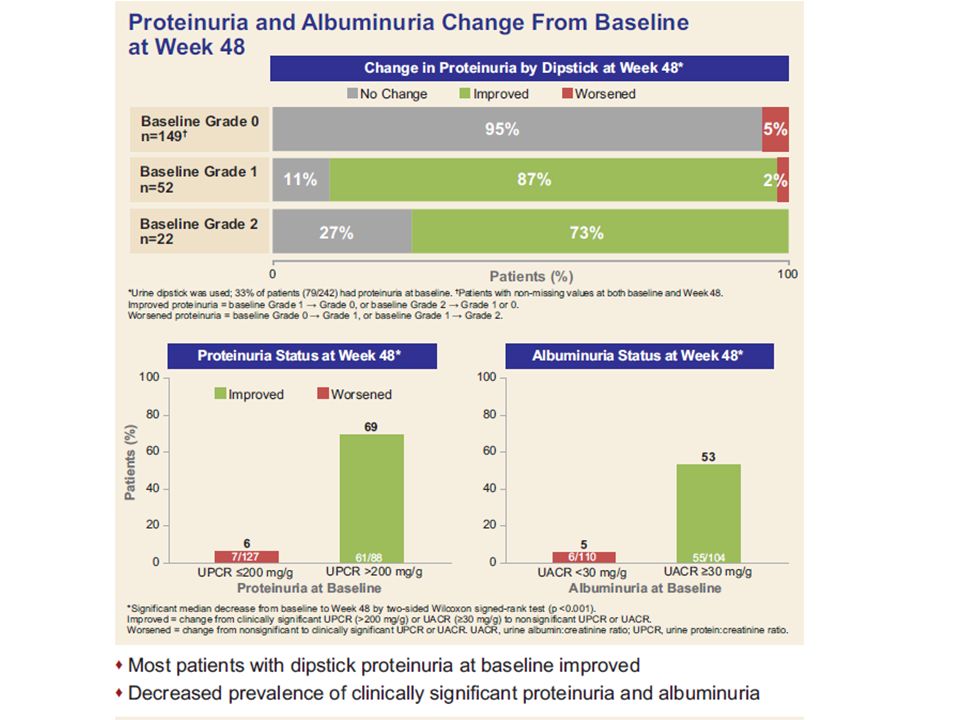
Valutazione della proteinuria
Dipstick (Screening) [0 – 4 +; 0 – 300 mg/dl] Proteinuria quantitativa su raccolta urine 24 h [0 – 0,3 g/24h] Rapporto Proteine/Creatinina (PCR) [0 – 0,2 g/g]⌘ Rapporto Albumina/Creatinina (ACR) [0 – 30 mg/g] ⌘ ⌘ Esame su campioni spot della mattina
 [0 – 4 +; 0 – 300 mg/dl] Proteinuria quantitativa su raccolta urine 24 h [0 – 0,3 g/24h] Rapporto Proteine/Creatinina (PCR) [0 – 0,2 g/g]⌘ Rapporto Albumina/Creatinina (ACR) [0 – 30 mg/g] ⌘ ⌘ Esame su campioni spot della mattina.")
59
Gradi di Proteinuria Microalbuminuria ACR > 30 < 200 mg/g
Proteinuria franca ACR > 200 mg/g PCR > 0,2 g/g Proteinuria lieve: PCR 0,2 – 1,0 g/g Proteinuria moderata: PCR 1,0 – 3,0 g/g Proteinuria grave: PCR > 3,0 g/g

60
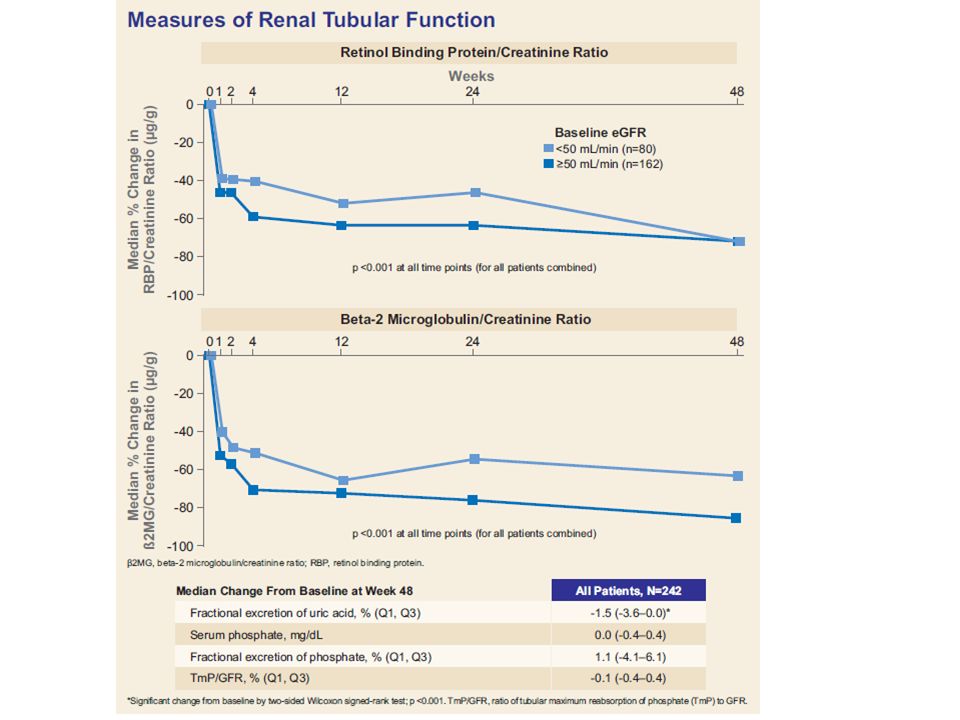
Dosaggio immunometrico di proteine a basso peso molecolare
-Retinol-binding protein -b2-microglobulina - a1-microglobulina - NGAL

61
Glomerulosclerosi Tubulo Glomerulo Sovraccarico tubulare

62
Grazie per l’attenzione

Presentazioni simili











 tel 339/1619488 Studi clinici veterinari in-field una nuova opportunita.>")




, 29-30 maggio 2013 PERCEZIONE DEI CAMPI.>")




