Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Teresa Gamucci Sora-Frosinone
Highlights in the Management of Urogenital Cancer Improving the standard of care for patients with hormone resistant prostate cancer Teresa Gamucci Sora-Frosinone Roma 9 Maggio 2008

2
Tumore della prostata ormonorefrattario
Circa l’80% dei paziente affetti da Ca della prostata metastatico che ricevono un blocco androgenico andrà in progressione entro 24 mesi Sopravvivenza mediana 12 mesi dalla progressione Sopravvivenza in relazione alla tipologia di presentazione: 18 mesi in caso di sola progressione biochimica 12 mesi in caso di progressione clinica asintomatica 6 mesi in caso di progressione clinica sintomatica

3
Tumore della prostata ormonorefrattario
Prima del 1991 : HRPC 26 studi di fase II con agenti singoli RR 8.7 % Median Survival mesi Tumore della prostata : neoplasia non chemioresponsiva Yagoda, Cancer 2003

4
Tumore della prostata ormonorefrattario
Tannok I: J Clin Oncol, 1996 Kantoff P: J Clin Oncol, 1999 Due studi randomizzati dimostrano un vantaggio in QoL ed in “pain relief “ utilizzando Mitoxantrone e Corticosteroidi vs solo Corticosteroidi (non vantaggio in sopravvivenza)
")
5
Tumore della prostata ormonorefrattario

6
Tumore della prostata ormonorefrattario
FDA approva l’impiego del Mitoxantrone nei pazienti sintomatici affetti da HRPC ma pochissimi pazienti vengono trattati

8
Tumore della prostata ormonorefrattario
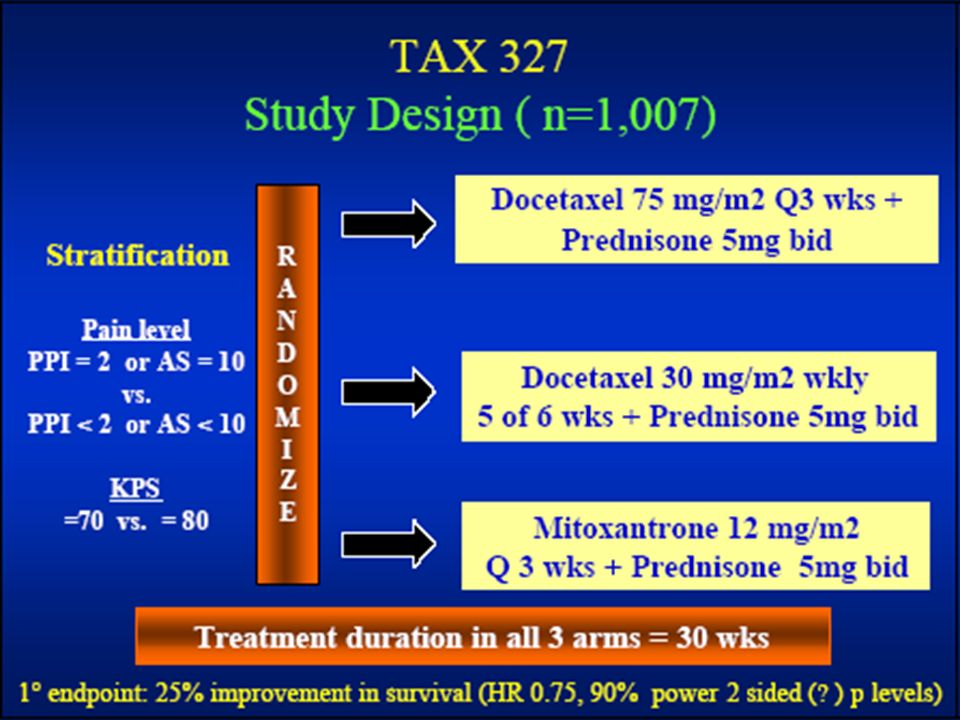
Tannok I: N Engl J Med, 2004 Petrylak D: N Engl J Med, 2004 Due grandi studi di fase tre con Docetaxel dimostrano un vantaggio in sopravvivenza per i pazienti trattati rispetto a quelli trattati con Mitoxantrone e Corticosteroidi

10
At a median follow-up of 32 months, 64% (217/338) of
the patients randomized to docetaxel and 70% (235/336) of the patients randomized to mitoxantrone had died. Both overall survival and disease-free survival were significantly longer with docetaxel plus estramustine than with mitoxantrone plus prednisone (Table 2). The relative risk for death was
 of. the patients randomized to mitoxantrone had died. Both overall. survival and disease-free survival were significantly longer. with docetaxel plus estramustine than with mitoxantrone. plus prednisone (Table 2). The relative risk for death was.")
11
SWOG 9916 : N Engl J Med 2004 Docetaxel 3-weekly plus Estramustine Ph
significantly improves : OS 17.5vs 15.6m p = 0.02 HR (95% CI ) PSA response vs 27 % p= Objective response vs 11 % p= 0.15 Median time to prog vs 3.2 m p= 0.001
 PSA response 50 vs 27 % p= Objective response 17 vs 11 % p= Median time to prog 6.3 vs 3.2 m p=")
12
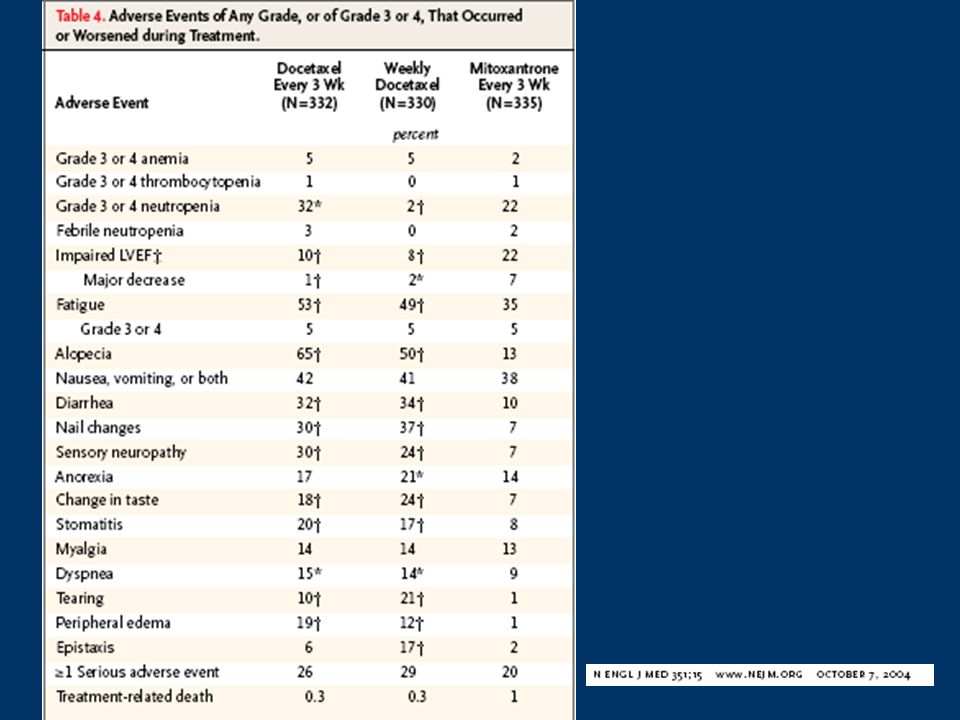
Toxicities were significantly higher in the docetaxel–
estramustine group. Sixteen percent of patients in the docetaxel–estramustine group and 10% in the mitoxantrone– prednisone group discontinued treatment as a result of adverse events. Rates of grade 3–4 neutropenia did not

13
Toxicities were significantly higher in the docetaxel–
estramustine group. Sixteen percent of patients in the docetaxel–estramustine group and 10% in the mitoxantrone– prednisone group discontinued treatment as a result of adverse events. Rates of grade 3–4 neutropenia did not differ between groups, but the incidence of severe and lifethreatening febrile neutropenia was higher with docetaxel plus estramustine (5% vs. 2%; p =.01). Gastrointestinal, neurologic, metabolic, and cardiovascular events were also significantly more common with docetaxel plus estramustine. The protocol was amended about halfway through its accrual to include prophylactic use of warfarin and aspirin; however, this did not appear to reduce the initial incidence of severe thromboembolic complications.
. Gastrointestinal, neurologic, metabolic, and cardiovascular events were also. significantly more common with docetaxel plus estramustine. The protocol was amended about halfway through its. accrual to include prophylactic use of warfarin and aspirin; however, this did not appear to reduce the initial incidence. of severe thromboembolic complications.")
16
TAX 327 : OVERALL SURVIVAL D3P vs MP + 2.9 months P =.004 HR =0.79
survival analysis was performed in August 2003 when 557 deaths had occurred. By March 2007, 310 additional deaths were recorded, resulting in a total of 867 deaths; 111 patients have been lost to follow-up, and 28 patients were alive with a last follow-up date within the previous year. Updated survival curves are shown in Figure 1, and details are listed in DR Berthold JCO 2008

17
TAX 327: JCO 2008 Docetaxel 3-weekly significantly improves :
OS vs 16.3 m p =.0009 HR (95% CI ) PSA response vs 32 % p= Objective response vs 7 % p= 0.11 Pain response vs 22 % p= .01 QoL (FACT.P) vs 13 % p= .009
 PSA response 45 vs 32 % p= Objective response 12 vs 7 % p= Pain response 35 vs 22 % p= .01. QoL (FACT.P) 22 vs 13 % p=")
18
When compared with the previous analysis,
the difference in median survival between the D3P and MP arms has increased slightly to 2.9 months, the hazard ratio (HR) has changed minimally, and the P value is slightly stronger (P.004). The difference in survival between the D1P and MP arms remains nonsignifi- cant (P .09). The percentages of patients who survived for more than 3 years in the D3P, D1P, and MP arms were 18.6%, 16.8%, and 13.5%, respectively (Table 1). Subgroup Analyses Median survival times and 95% CIs for the defined subgroups as
 has changed. minimally, and the P value is slightly stronger (P.004). The difference. in survival between the D1P and MP arms remains nonsignifi- cant (P .09). The percentages of patients who survived for more. than 3 years in the D3P, D1P, and MP arms were 18.6%, 16.8%, and. 13.5%, respectively (Table 1). Subgroup Analyses. Median survival times and 95% CIs for the defined subgroups as.")
19
Similar trends in survival between treatment arms were seen for patients
greater than and less than the median age of 68 years. The HRs for younger and older patients were 0.81 and 0.77, respectively, for D3P compared with MP. Similar results were found when using a more extreme age cutoff of 75 years (HR0.80 for older patients).(20% del totale)
.(20% del totale)")
20
In the TAX 327 study, the median serum PSA at baseline was 115ng/mL
In the TAX 327 study, the median serum PSA at baseline was 115ng/mL. Among patients with lower and higher PSA levels at baseline, theHRs were 0.83 and 0.73, respectively, indicating similar benefits of D3Pcompared withMPfor patients with a greater or lesser burden of disease. The presence of visceral involvement is a known adverse prognostic factor for men with metastatic prostate cancer when compared with patients with only bone and/or nodal disease. In the present study, the 22% of patients with visceral disease died on average 6 months earlier than those without visceral metastases. The HR was 0.87 for the subgroup of men with visceral metastases when comparing D3P with MP compared withMPfor patients with a greater or lesser burden of disease. The presence of visceral involvement is a known adverse prognostic factor for men with metastatic prostate cancer when compared with patients with only bone and/or nodal disease. In the present

21
There were 456 patients with substantial pain at baseline (defined
by PPI2 and/or AS10), and survival time was shorter for those with pain. The HRs for patients without and with pain were 0.73 and 0.85, respectively, for D3P compared with MP.
, and survival time was shorter for those. with pain. The HRs for patients without and with pain were 0.73 and. 0.85, respectively, for D3P compared with MP.")
22
Patients with a KPS 90% lived approximately 8 months longer
than patients with aKPS80%; however, theHRsfor these groups were similar at 0.75 and 0.82, respectively, for D3P compared with MP.

23
Men with better or worse QOL, as indicated by their FACT-P
score at baseline, had HRs of 0.92 and 0.66, respectively, when treated with D3P compared with MP. For minimally symptomatic patients

24
For minimally symptomatic patients
(FACT-P score128, PPI2, and AS10), the trend for survival benefit was maintained for D3P compared with MP.
, the trend for survival. benefit was maintained for D3P compared with MP.")
25
Therefore, the earlier mentioned factors are indicators of poor prognosis but not predictors of response

27
HRCP: confronto fra gli studi
SWOG 99-16 TAX 327 Soprav. Docet 18 mesi 19.2 mesi Soprav. Mitox 16 mesi 16.3 mesi Miglioramento OS 2 mesi 2.5 mesi HR 0.80 0.79 RR PSA Docetax 50 % 45.4 % RR PSA Mitox 27 % 32 %

28
Tumore della prostata ormonorefrattario
The HRs for death similar in the TAX327 and SWOG 9916 The secondary endpoints (PSA response, pain response, and QoL response) The docetaxel–prednisone regimen appeared to be better tolerated Docetaxel plus prednisone is the appropriate choice for the first-line treatment of HRPC The regimen approved for use in HRPC in the U.S. and Europ Oudard and colleagues [6] conducted a meta-analysis using the data from all three trials to determine if the schedule of docetaxel treatment affected survival. They assessed overall survival at 12, 18, 24, 30, and 36 months and evaluated the impact of weekly and Q3W therapy on overall survival. Using combined data from 1,807 patients, they found that overall survival was significantly greater with docetaxel at all time points evaluated. The relative risk for death ranged from 8%–21% lower. As in TAX327, the difference in survival was significant for the comparison of Q3W docetaxel with MP but not for weekly docetaxel compared with MP. Second, the utility of estramustine and its associated toxicity is another important consideration. Because the HRs for death and the secondary end points (PSA response, pain response, and QoL response) were similar in the TAX327 and SWOG 9916 trials, yet the docetaxel–prednisone regimen appeared to be better tolerated, it is reasonable to conclude at this time that treatment with docetaxel plus prednisone alone is the appropriate choice for the first-line treatment of HRPC. The regimen approved for use in HRPC in the U.S. and Europ
 The docetaxel–prednisone regimen appeared to be better tolerated. Docetaxel plus prednisone is the appropriate. choice for the first-line treatment of HRPC. The regimen approved for use in HRPC in the U.S. and Europ. Oudard and colleagues [6] conducted a meta-analysis. using the data from all three trials to determine if the. schedule of docetaxel treatment affected survival. They. assessed overall survival at 12, 18, 24, 30, and 36 months. and evaluated the impact of weekly and Q3W therapy on. overall survival. Using combined data from 1,807 patients, they found that overall survival was significantly greater. with docetaxel at all time points evaluated. The relative risk. for death ranged from 8%–21% lower. As in TAX327, the. difference in survival was significant for the comparison. of Q3W docetaxel with MP but not for weekly docetaxel. compared with MP. Second, the utility of estramustine. and its associated toxicity is another important consideration. Because the HRs for death and the secondary end. points (PSA response, pain response, and QoL response) were similar in the TAX327 and SWOG 9916 trials, yet the. docetaxel–prednisone regimen appeared to be better tolerated, it is reasonable to conclude at this time that treatment. with docetaxel plus prednisone alone is the appropriate. choice for the first-line treatment of HRPC. The regimen. approved for use in HRPC in the U.S. and Europ.")
29
Tumore della prostata ormonorefrattario : quando trattare
In contrast to the earlier Canadian study1 that evaluated mitoxantrone, the TAX 327 trial has included patients with and without symptoms. In general, the chances of prolonging survival with D3P seemed similar among patients with higher and lower disease burden as indicated by level of serum PSA, the presence or absence of substantial pain, and the QOL or performance score. This analysis does not address whether docetaxel should be used in patients with minimal symptoms or whether it is appropriate to defer treatment until more symptoms occur. However, considering the similar benefit among subgroups and the potential for QOL to deteriorate as a result of disease progression, it seems reasonable to offer treatment to patients with symptoms and to those who are likely to develop symptoms in the near future, based on the burden of disease and the PSA doubling Sternberg CN, ASCO Education ,June 2006

30
Tumore della prostata ormonorefrattario : quando trattare
TAX 327 ha incluso pazienti con e senza sintomi La probabilità di prolungare la sopravvivenza sembra uguale nei pazienti con alto o basso “disease burden” Ragionevole offrire il trattamento ai pazienti sintomatici e a quelli che svilupperanno sintomi nel prossimo futuro basandosi sulla clinica e sul “PSA doubling “ In contrast to the earlier Canadian study1 that evaluated mitoxantrone, the TAX 327 trial has included patients with and withoutsymptoms. In general, the chances of prolonging survival with D3P seemed similar among patients with higher and lower disease burden as indicated by level of serum PSA, the presence or absence of substantial pain, and the QOL or performance score. This analysis does not address whether docetaxel should be used in patients with minimal symptoms or whether it is appropriate to defer treatment until more symptoms occur. However, considering the similar benefit among subgroups and the potential for QOL to deteriorate as a result of disease progression, it seems reasonable to offer treatment to patients with symptoms and to those who are likely to develop symptoms in the near future, based on the burden of disease and the PSA doubling

32
HRPC : Trattare tutti nello stesso modo ?
Il TAX327, ha dimostrato che la somministrazione settimanale di Docetaxel è attiva anche se non dimostra un vantaggio significativo in sopravvivenza verso il Mitoxantrone HR median survivals 17.8 m PSA % (p ) QoL % (p 0.005) Trattamento indicato per l’anziano frail
 QoL 23% (p 0.005) Trattamento indicato per l’anziano frail.")
34
Tumore della prostata ormonorefrattario
Dal 2004 il trattamento chemioterapico standard dell’HRPC è il Docetaxel SWOG 9916 e TAX 327 Complessivamante 1600 pazienti trattati SWOG 9916: Docetaxel + Estramustina vs Mitoxantrone + Prednisone ↑ 2 mesi in OS TAX 326: Docetaxel q21 + Prednisone vs Mitoxantrone + Prednisone ↑ 2.5 mesi in OS

Presentazioni simili















>")




