Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

2
LESIONI ARTERIOSCLEROTICHE: PROCESSI PATOLOGICI INTERESSANTI LE
ARTERIE E AVENTI IN COMUNE L’ISPESSIMENTO, L’INDURIMENTO E LA PERDITA DI ELASTICITA’ DEI VASI INTERESSATI. ARTERIOLOSCLEROSI SCLEROSI CALCIFICA DELLA MEDIA (DI MONCKEBERG) ATEROSCLEROSI
 ATEROSCLEROSI.")
4
MEDIA INTIMA Arteriolosclerosi di tipo ialino Arteriolosclerosi di tipo iperplastico

5
ATEROSCLEROSI

7
monocito STRIA LIPIDICA foam cell SMC foam cell lipidi extracellulari fibre collagene PLACCA FIBROSA SMC cell. muscolare liscia linfocita T foam cell apoptotica SMC

8
Neovascolarizzazione
LESIONE COMPLICATA foam cell monocito foam cell apoptotica lipidi extracellulari fibre collagene piastrine linfocita T SMC cell. muscolare liscia in apoptosi Calcificazioni Neovascolarizzazione (angiogenesi) emorragie intimali SMC Atrofia della media
 emorragie intimali. SMC. Atrofia della media.")
10
APPROCCI PREVENTIVI E TERAPEUTICI
Inizio lesione: eliminazione “cause” Stabilizzazione della placca Progressione della placca: inibizione formazione di placca “instabile” Complicanze trombotiche: riduzione fattori favorenti formazione di trombi

12
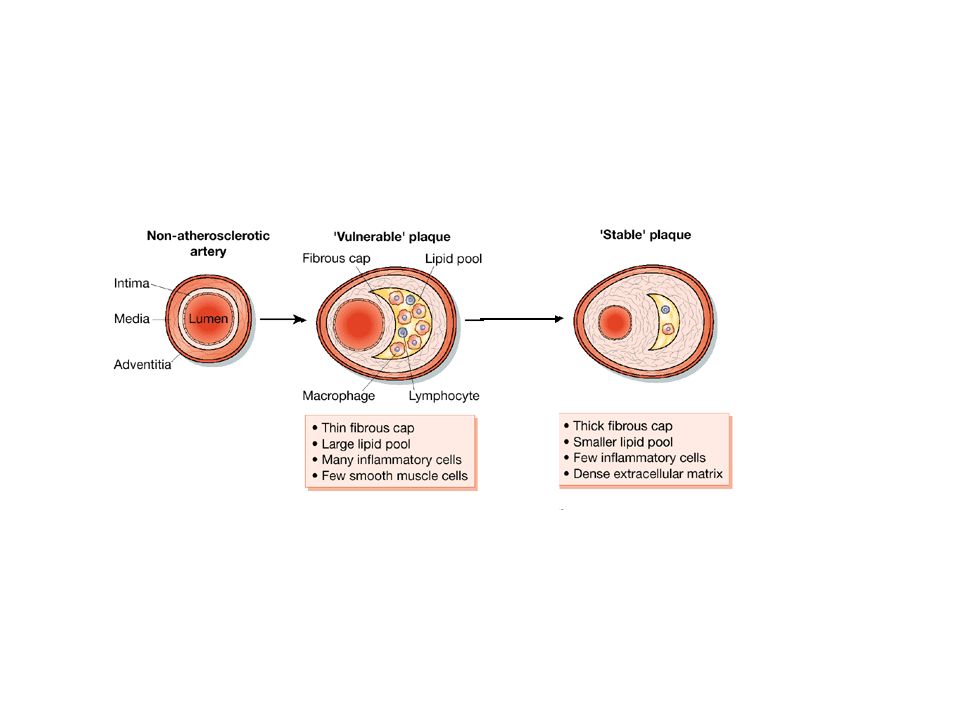
CARATTERISTICHE DELLA PLACCA
EVIDENZE DEL RUOLO DI ALTERAZIONI LIPIDICHE (DELLA COLESTEROLEMIA) NELLA PATOGENESI DELL’ATEROSCLEROSI CARATTERISTICHE DELLA PLACCA STUDIO DI PAZIENTI CON IPERCOLESTEROLEMIA FAMIGLIARE EFFETTO DI DIETE RICCHE DI COLESTEROLO IN PRIMATI E CONIGLI WATANABE HERITABLE HYPERLIPIDEMIC RABBITS (WHHL rabbits) TOPI CON INATTIVAZIONE GENICA DI APOE (Apoproteina) o RECETTORE PER LDL (LDL-R).
 NELLA PATOGENESI DELL’ATEROSCLEROSI. CARATTERISTICHE DELLA PLACCA. STUDIO DI PAZIENTI CON IPERCOLESTEROLEMIA FAMIGLIARE. EFFETTO DI DIETE RICCHE DI COLESTEROLO IN PRIMATI E CONIGLI. WATANABE HERITABLE HYPERLIPIDEMIC RABBITS (WHHL rabbits) TOPI CON INATTIVAZIONE GENICA DI APOE (Apoproteina) o RECETTORE PER LDL (LDL-R).")
13
apoproteina fosfolipide colesterolo libero esterificato

14
intestino chilomicrone microcircolo lipoproteinlipasi tessuti periferici fegato VLDL IDL LDL

15
HDL fegato a-HDL pre-b-HDL VLDL/IDL LDL Tessuti periferici LCAT
Lecitina Colesterolo Acil Transferasi HDL APO-A fegato APO-A a-HDL pre-b-HDL APO-E APO-A VLDL/IDL Tessuti periferici LDL

16
RECETTORI PER LIPOPROTEINE
APO-B100 I. LDL-Receptor APO-E ubiquitario L’espressione è regolata II. LRP (LDL-Receptor Related Protein) APO-E ubiquitario L’espressione non è regolata
 APO-E. ubiquitario. L’espressione non è regolata.")
17
III. Scavenger Receptors (SR)
LDL “modificate” altri monociti/macrofagi L’espressione non è regolata SR-A LDL “modificate” LDL “modificate” altri HDL mon./macr.; cells endo- teliali; adipociti fegato; tessuti sintetizzanti ormoni steroidei SR-B1 SR-B2

18
APO-B100 APO-E

19
coated pit Endosoma H+ Riciclaggio Lisosomi Lisosoma secondario lipidi aminoacidi colesterolo

20
- 3 2 1 NUCLEO Lisosoma secondario aminoacidi lipidi colesterolo
NEOSINTESI - 3 2 Inibizione HMGCoA REDuttasi 1 Attivazione ACAT NUCLEO Inbizione neosintesi Accumulo esterificato

21
IPERCOLESTEROLEMIA FAMIGLIARE: TIPI DI ALTERAZIONI DEL RECETTORE
I. RIDOTTA ESPRESSIONE II. SINTESI DI RECETTORI CHE RIMANGONO NEL REL/GOLGI III. RECETTORI CHE HANNO DIFETTI DI INTERNALIZZAZIONE IV. RECETTORI CHE HANNO BASSA AFFINITA’ DI LEGAME PER APO-B100

22
FEGATO - VIE BILIARI Sali biliari colestiramina acetilCoA colesterolo
HMGCoAR* *hydroxymethyl-glutaryl-CoA reductase - statine FEGATO E TESSUTI PERIFERICI

23
Lipoproteine contenenti APOE: Chilomicroni (Remnants), VLDL, IDL
LRP: LDL Receptor Related Protein Lipoproteine contenenti APOE: Chilomicroni (Remnants), VLDL, IDL
, VLDL, IDL.")
24
SCAVENGER RECEPTOR A

25
TESSUTI SINTETIZZANTI ORMONI
FEGATO APO-A APO-E esteri colesterolo SR-BI TESSUTI SINTETIZZANTI ORMONI STEROIDEI SR-BI APO-A a-HDL

27
Figure 1 Mononuclear phagocytes in atherogenesis
Figure 1 Mononuclear phagocytes in atherogenesis. This figure schematizes steps in the recruitment of mononuclear phagocytes to the nascent atherosclerotic plaque and some of the functions of these cells in the mature atheroma. The steps are depicted in an approximate time sequence proceeding from left to right. The normal arterial endothelium resists prolonged contact with leukocytes including the blood monocyte. When endothelial cells undergo inflammatory activation, they increase their expression of various leukocyte adhesion molecules. In the context of monocyte recruitment to the atheroma, vascular cell adhesion molecule-1 (VCAM-1) seems to have a major role. Once adherent to the activated endothelial layer, the monocyte diapedeses between intact endothelial cells to penetrate into the tunica intima, or innermost layer of the arterial wall. This directed migration requires a chemoattractant gradient. Various chemokines seem to participate in this process, particularly interaction of monocyte chemoattractant protein-1 (MCP-1) with its receptor CCR2. Once resident in the intima the monocyte acquires characteristics of the tissue macrophage. In the atheroma in particular, the macrophage expresses scavenger receptors that bind internalized lipoprotein particles modified for example by oxidation or glycation. These processes give rise to the arterial foam cell, a hallmark of the arterial lesion, so named because of the foamy appearance under the microscope, which is the result of accumulation of lipid droplets within the cytoplasm. Within the arterial intima, the macrophage serves many functions related to atherosclerosis and its complications. Notably, the foam cell secretes pro-inflammatory cytokines that amplify the local inflammatory response in the lesion, as well as reactive oxygen species. The activated mononuclear phagocyte has a key role in the thrombotic complications of atherosclerosis by producing matrix metalloproteinases (MMPs) that can degrade extracellular matrix that lends strength to the plaque's fibrous cap. When the plaque ruptures as a consequence, it permits the blood to contact another macrophage product, the potent pro-coagulant protein tissue factor. Eventually the macrophages congregate in a central core in the typical atherosclerotic plaque. Macrophages can die in this location, some by apoptosis, hence producing the so-called 'necrotic core' of the atherosclerotic lesion.
 seems to have a major role. Once adherent to the activated endothelial layer, the monocyte diapedeses between intact endothelial cells to penetrate into the tunica intima, or innermost layer of the arterial wall. This directed migration requires a chemoattractant gradient. Various chemokines seem to participate in this process, particularly interaction of monocyte chemoattractant protein-1 (MCP-1) with its receptor CCR2. Once resident in the intima the monocyte acquires characteristics of the tissue macrophage. In the atheroma in particular, the macrophage expresses scavenger receptors that bind internalized lipoprotein particles modified for example by oxidation or glycation. These processes give rise to the arterial foam cell, a hallmark of the arterial lesion, so named because of the foamy appearance under the microscope, which is the result of accumulation of lipid droplets within the cytoplasm. Within the arterial intima, the macrophage serves many functions related to atherosclerosis and its complications. Notably, the foam cell secretes pro-inflammatory cytokines that amplify the local inflammatory response in the lesion, as well as reactive oxygen species. The activated mononuclear phagocyte has a key role in the thrombotic complications of atherosclerosis by producing matrix metalloproteinases (MMPs) that can degrade extracellular matrix that lends strength to the plaque s fibrous cap. When the plaque ruptures as a consequence, it permits the blood to contact another macrophage product, the potent pro-coagulant protein tissue factor. Eventually the macrophages congregate in a central core in the typical atherosclerotic plaque. Macrophages can die in this location, some by apoptosis, hence producing the so-called necrotic core of the atherosclerotic lesion.")
30
FATTORI DI RISCHIO PER ATEROSCLEROSI: IMPLICAZIONI FISIOPATOLOGICHE
Forte evidenza di causalità Buona evidenza di causalità Ipercolesterolemia Ridotta espressione LDL-R, Aumento LDL circolanti, Aumentata probabilità ossidazione e deposito nell’intima Ipertensione Alterazioni endoteliali e aumentato adsorbimento di LDL nell’intima Genere maschile Mancata protezione da parte di ormoni sessuali femminili (vedi poi), Abitudini di vita, Altri (??) Diabete mellito Glicosilazione di proteine della superficie endoteliale e dell’intima vascolare, Alterazioni metaboliche (Tipo II) Storia famigliare di prematura CAD Alterazioni recettori per LDL, Alterazioni Apoproteine, Neosintesi ed eliminazione colesterolo (??) Elevati livelli di lipoproteina (a) Aumentate complicanze trombotiche Fumo da sigaretta Alterazioni endoteliali ed aumentata ossidazione LDL Stato post-menopausale Regressione di alto rapporto HDL/VLDL tipico di donne in età fertile Iperfibrinogenemia (e aumento coagu-labilità del sangue) Aumentate complicanze trombotiche Inattività fisica Riduzione HDL, Ridotto utilizzo colesterolo, Altri Obesità Ipertensione ealterazioni metaboliche Iperomocisteinemia Alterazioni endoteliali
, Abitudini di vita, Altri ( ) Diabete mellito. Glicosilazione di proteine della superficie endoteliale e dell’intima vascolare, Alterazioni metaboliche (Tipo II) Storia famigliare di prematura CAD. Alterazioni recettori per LDL, Alterazioni Apoproteine, Neosintesi ed eliminazione colesterolo ( ) Elevati livelli di lipoproteina (a) Aumentate complicanze trombotiche. Fumo da sigaretta. Alterazioni endoteliali ed aumentata ossidazione LDL. Stato post-menopausale. Regressione di alto rapporto HDL/VLDL tipico di donne in età fertile. Iperfibrinogenemia (e aumento coagu-labilità del sangue) Aumentate complicanze trombotiche. Inattività fisica. Riduzione HDL, Ridotto utilizzo colesterolo, Altri. Obesità. Ipertensione ealterazioni metaboliche. Iperomocisteinemia. Alterazioni endoteliali.")
Presentazioni simili






 is a disease state characterized by airflow limitation that is not fully reversible. The.>")






>")




>")





