Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
CAMPAGNA EDUCAZIONALE REGIONALE ANMCO TOSCANA Difendiamo il Cuore Casciana Terme 12 Gennaio 2008 Dai grandi Trials con Statine al razionale del target terapeutico del Colesterolo in Prevenzione Secondaria Dr. Stefano Viani UO Malattie Cardiovascolari Ospedale di Pontedera USL 5 Pisa

2
La mortalità per malattia ischemica del cuore (IHD) è alta e aumenterà Mortalità per IHD (migliaia) EME=mercati con economie stabili; FSE=economia ex socialiste; OAI=altri paesi asiatici e isole del Pacifico; SSA=Africa sub-sahariana; LA=America Latina; Mid East=Medio Oriente. Yusuf S et al. Circulation. 2001;104:2746-2753. La mortalità regionale per IHD tra il 1990 e il 2020

3
… chi presenta tutti i nove fattori ha una probabilità di infarto che è più di 330 volte superiore a quella di chi non ne ha nessuno (90% probabilità) !!!!!! Studio INTERHEART (15.152 casi e 14.820 controlli) Lancet 3 settembre 2004 Nove fattori di rischio, facilmente misurabili, spiegano oltre il 90% degli infarti in tutte le regioni del mondo Lassociazione di più fattori di rischio moltiplica la probabilità di infarto: … 1.Fumo 2.Ipertensione 3.Diabete 4.Dislipidemia 5.Obesità addominale 6.Stress 7.Inattività fisica 8.Scarsa assunzione di frutta e verdura 9.Nulla assunzione di alcool
 Lancet 3 settembre 2004 Nove fattori di rischio, facilmente misurabili, spiegano oltre il 90% degli infarti in tutte le regioni del mondo Lassociazione di più fattori di rischio moltiplica la probabilità di infarto: … 1.Fumo 2.Ipertensione 3.Diabete 4.Dislipidemia 5.Obesità addominale 6.Stress 7.Inattività fisica 8.Scarsa assunzione di frutta e verdura 9.Nulla assunzione di alcool.")
5
RISCHIO CARDIOVASCOLARE E COLESTEROLEMIA

6
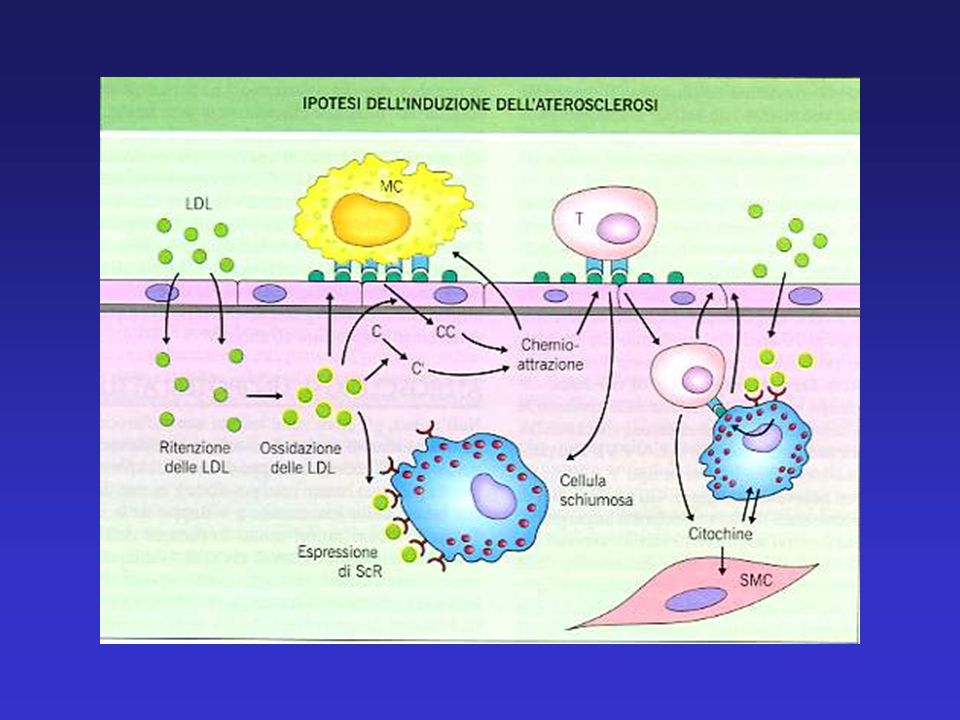
Adapted from Ray KK et al. J Am Coll Cardiol. 2005;46:1425-1433. EFFETTI NON IPOLIPEMIZZANTI (effetto precoce/rapido) EFFETTI IPOLIPEMIZZANTI (effetto lento/ritardato) Effetti delle Statine Disfunzione/attivazione endoteliale Coagulazione/ attivazione piastrine inibitorio Infiammazione/ attivazione immunologica Statine Fegato Sintesicolesteroloepatico Rottura della placca/ occlusione trombotica Placca aterosclerotica ricca di lipidi trombo Nucleo lipidico Statine Inibizione HMG-CoA reduttasi
 EFFETTI IPOLIPEMIZZANTI (effetto lento/ritardato) Effetti delle Statine Disfunzione/attivazione endoteliale Coagulazione/ attivazione piastrine inibitorio Infiammazione/ attivazione immunologica Statine Fegato Sintesicolesteroloepatico Rottura della placca/ occlusione trombotica Placca aterosclerotica ricca di lipidi trombo Nucleo lipidico Statine Inibizione HMG-CoA reduttasi.")
8
HPS 2002 TNT 2005 LIPID 1998 CARE 1996 4 S 1994 IDEAL 2005 Trials di Prevenzione Secondaria con Statine Coronaropatia Elevati valori di LDL-C Valori di LDL-C nella media Popolazione adAlto Profilo di Rischio Definizione del target LDL-C Alte dosi vs basse dosi NCEP-ATP III 2001 UPDATE 2004

9
4444 pts Pregresso Infarto del Miocardio/ Angina Stabile Colesterolo totale medio 272+23 mg/dl (in terapia dietetica) Simvastatina 20 mg/die (40 mg/die 37%) vs Placebo Riduzione LDL-C 38% nel gruppo trattato Follow-up: 5.6 anni -30% mortalità totale -34% mortalità per CHD 4S Scandinavian Simvastatin Survival Study Lancet 1994
 Simvastatina 20 mg/die (40 mg/die 37%) vs Placebo Riduzione LDL-C 38% nel gruppo trattato Follow-up: 5.6 anni -30% mortalità totale -34% mortalità per CHD 4S Scandinavian Simvastatin Survival Study Lancet 1994")
10
4159 pts (M 86%) Pregresso Infarto del Miocardio (media 10 mesi dalla randomizzazione) Colesterolo totale < 240 mg/dl (in terapia dietetica) Colesterolo LDL tra 115 e 174 mg/dl (media 139 mg/dl) Pravastatina 40 mg/die vs Placebo Follow-up: 5 anni End point I: evento coronarico fatale o infarto miocardico non fatale CARE Cholesterol and Recurrent Events Trial Sacks FM et al. NEJM 1996 Mean LDL-C level reduced by 32% 97 to 98 mg/dl throughout the 5 yr FU

11
LIPID The Long-term Intervention with Pravastatin in Ischaemic Disease Study 9014 pts (M 83%) Pregresso Infarto del Miocardio /Pregressa Angina Instabile (64%/36%) Colesterolo totale medio 218 mg/dl (in terapia dietetica) Colesterolo LDL tra 130 e 170 mg/dl (media 150 mg/dl) Pravastatina 40 mg/die vs Placebo Follow-up: 6.1 anni End point I: mortalità per evento coronarico Lipid Study Group. NEJM 1998

12
NCEP-ATP III Risk Categories High Risk CHD, PVD, Diabetes 2 + RF (10 yr risk > 20%) LDL-C goal < 100 mg/dl Moderately High Risk 2 + RF (10 yr risk 10-20%) LDL-C goal < 130 mg/dl Moderate Risk 2 + RF (10 yr risk > 10%) LDL-C goal < 130 mg/dl Lower Risk 0-1 RF (10 yr risk > 20%) LDL-C goal < 160 mg/dl JAMA 2001 (www.cuore.iss.it/valutazione/carte.asp)
 LDL-C goal < 100 mg/dl Moderately High Risk 2 + RF (10 yr risk 10-20%) LDL-C goal < 130 mg/dl Moderate Risk 2 + RF (10 yr risk > 10%) LDL-C goal < 130 mg/dl Lower Risk 0-1 RF (10 yr risk > 20%) LDL-C goal < 160 mg/dl JAMA 2001 (")
13
NCEP-ATP III Treatment Algorithm In High Risk Patients 2001 LDL-C > 130 LDL-C 100-129 LDL C < 100 TLC and Statin TLC/Statin/ Fibrates/ Nicotinic Acid No Lowering Therapy Therapeutic Indication Therapeutic Options LDL-C Goal JAMA 2001

14
60100 LDL-C mg/dl Threshold: unnecessary to go very low Curvilinear: the lower the better with diminishing returns Linear: the lower the better Possible Relationship between LDL-C and CHD Risk (2001) CHD Risk
 CHD Risk")
15
HPS Study (Heart Protection Study Investigators) 20536 UK pts (40-80 yr) High Risk pts CHD, PVD, Diabetes Variable LDL-C at baseline (TLC) Simvastatin 40 mg/die vs Placebo (also vitamins arm) Follow-up: 5 yr Results 13% reduction all cause death 24% reduction major vascular events 27% reduction major coronary events 25% reduction stroke 24% reduction revascularization Lancet 2002
 UK pts (40-80 yr) High Risk pts CHD, PVD, Diabetes Variable LDL-C at baseline (TLC) Simvastatin 40 mg/die vs Placebo (also vitamins arm) Follow-up: 5 yr Results 13% reduction all cause death 24% reduction major vascular events 27% reduction major coronary events 25% reduction stroke 24% reduction revascularization Lancet 2002")
16
P<0.00001 HPS: Reduction of Major Cardiovascular Events according to baseline LDL-C (mg/dl) Lancet 2002
 Lancet 2002")
17
60100 Log CVD Risk LDL-C mg/dl 22% reduction CVD 26% reduction CVD HPS Study: CVD Risk reduction according to LDL-C level The lower the better Lancet 2002

18
*In high-risk patients with high TG (>200 mg/dl) or low HDL-C consider fibrates/nicotinic acid High Risk CHD or CHD risk equivalents ACS LDL-C level 100 - 160 - 130 - 190 - Lower Risk Moderately High Risk Target <160 mg/dL Target <130 mg/dL 70 - Target <100 mg/dL Optional goal <70 mg/dL* Moderate Risk Target <130 mg/dL Optional goal <100 mg/dL NCEP ATP III: LDL-C Goals (2004 proposed modifications) Grundy SM et al. Circulation 2004

19
Considerations and Limitations for achieving very low LDL-C levels Dangers from very low LDL-C (unlikely) High baseline LDL-C levels (> 150 mg/dl, max drug lowering about 50%) Side effects of high drug doses
 High baseline LDL-C levels (> 150 mg/dl, max drug lowering about 50%) Side effects of high drug doses")
20
10001 pts (M 81%) Clinically evident, stable CHD (58.5% previous myocardial infarction) LDL-C < 130 mg/dl ( mean 98+18/97+18 mg/dl, after a 8 w open-label treatment with Atorva 10 mg/die) Atorvastatin 10 mg/die vs Atorvastatin 80 mg/die Follow-up: 4.9 yrs End point I: occurrence of a first major CV event (death from CHD non fatal myocardial infarction, resuscitation after cardiac arrest, fatal or nonfatal stroke) TNT Study (Treating to New Targets Investigators) La Rosa JC et al. NEJM 2005

24
8888 pts (M 81%) Previous Myocardial Infarction LDL-C < 130 mg/dl (mean 121.4+0.5/121.6+0.5 mg/dl) Simvastatin 20 mg/die vs Atorvastatin 80 mg/die Follow-up: 4.8 yrs End point I: occurrence of a first major CV event (death from CHD non fatal myocardial infarction, resuscitation after cardiac arrest) IDEAL Study (Incremental Decrease in End Points Through Aggressive Lipid Lowering) Pedersen TR et al. JAMA 2005

25
…intensive lowering of LDL-C did not result in a significant reduction of the primary outcome of major coronary events, but did reduce the risk of other secondary end points and nonfatal acute MI. Pts with MI may benefit from intensive lowering of LDL-C without an increase in non-CV mortality or other serious adverse reaction

26
Adverse Events resulting in 5.8 8.1 p<.001 4.2 9.6 p<.001 permanent discontinuation of study drug (%) ALT > 3 ULN on 2 consecutive 0.2 1.2 p<.001 0.11 0.97 p<.001 measurements (%) Myalgia (%) 4.7 4.8 p: NS 1.1 2.2 p<.001 Rhabdomyolysis (%) 0.06 0.04 p: NS 0.07 0.05 p: NS A10 A80 S A80 TNTIDEAL
 ALT > 3 ULN on 2 consecutive p< p<.001 measurements (%) Myalgia (%) p: NS p<.001 Rhabdomyolysis (%) p: NS p: NS A10 A80 S A80 TNTIDEAL")
27
Low-density lipoprotein cholesterol (LDL-C) levels of trials comparing high-dose to standard-dose statin therapy Cannon C. P. et al. J Am Coll Cardiol 2006

28
Individual trials and pooled analysis showing a highly significant 16% reduction in the risk of coronary death or any cardiovascular event (myocardial infarction, stroke, hospitalization for unstable angina, or revascularization) (p < 0.0001) Cannon C. P. et al. J Am Coll Cardiol 2006

29
Individual trials and pooled analysis showing a highly significant 16% reduction in the risk of coronary death or myocardial infarction (p < 0.0001)
")
30
Individual and pooled analyses showing: A) non-significant trend in reduction of cardiovascular death B) no increased risk of non- cardiovascular mortality C) a non-significant trend toward decreased overall mortality with high-dose statins Cannon C. P. et al. J Am Coll Cardiol 2006

31
High dose vs Standard doseStatin standard dose vs Placebo Stroke Risk reduction in High Risk Patients

32
Prevenzione con Statine nei Soggetti ad Alto Rischio (= Prevenzione Secondaria) Le modificazioni terapeutiche dello stile di vita sono una componente essenziale del trattamento di questi pazienti La riduzione del LDL-C determina un significativo beneficio in termini di mortalità e morbilità cardiovascolare Tanto più si riducono i valori di LDL-C tanto maggiore è il beneficio in termini di riduzione del rischio (the lower the better). In particolare la terapia con statine è ragionevole anche in soggetti ad alto rischio con LDL-C < 100 mg/dl con un target terapeutico < 70 mg/dl La terapia con alte dosi conferisce un significativo vantaggio se confrontata con quella a dosi standard particolarmente nella prevenzione degli eventi cardiovascolari non fatali (ogni milione di pts trattati con alte dosi si eviterebbero 35000 eventi CV, più di 14000 morti coronariche o infarto del miocardio, con un NNT di 29 per 2 aa nei pazienti con SCA, per 5 aa nei pazienti con coronaropatia stabile)
.")
35
Ford ES et al. NEJM 2007;356:2388-2398 Special Article Explaining the Decrease in U.S. Deaths from Coronary Disease, 1980-2000 Approximately half the decline in U.S. deaths from coronary heart disease from 1980 through 2000 may be attributable to reductions in major risk factors and approximately half to evidence- based medical therapies Remember……. Guidelines that are not followed are of no value !

36
Risk CategoryGoalInitiation levelConsideration level for for TLCdrug therapy High Risk 100> 100 (optional < 70)(optional < 100) Moderately High Risk 130> 130 (optional < 100)(optional 100-129) Moderate Risk 130> 160 Low Risk 160> 190 (optional 160-189) LDL-C mg/dl Updated ATP III LDL-C Goals and Cutpoints for Therapy Grundy SM et al. Circulation 2004

Presentazioni simili



















 Guidelines May 2001 Ipercolesterolemie famigliari Ipercolesterolemie e rischio cardio vascolare globale.>")
>")




