Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Carcinoma del rene

2
AM. F: ♀, 72 aa. Anamnesi: - ipertensione (in trattamento) diverticolosi colica (episodi di diverticolite) Ipotiroidismo (in trattamento) Fumatrice sovrappeso
 Fumatrice. sovrappeso.")
3
Aprile 2005 da 2 mesi: dolore in regione lombare dx febbre, astenia, perdita di peso (6 kg) Es. ematochimici: lieve anemia (Hgb 9.5 g/dl) lieve ipercreatininemia (1.6 mg/dl) Ecografia: formazione iperecogena a carico del rene dx (Ø 6 cm).
 Ecografia: formazione iperecogena a carico del rene dx (Ø 6 cm).")
4
Aprile 2005 Rx torace: aspetto lievemente enfisematoso note di bronchite cronica TC addome: “A carico rene dx, nodulo Ø 6 cm a centro necrotico che impronta i calici renali senza sicuri segni infiltrativi o trombotici a carico della vena renale. Non linfoadenomegalie nelle stazioni iliache e pelviche” Sospetto carcinoma del rene.

5
? Quali tra i seguenti sono considerati fattori di rischio per l’insorgenza di carcinoma renale? A) obesità B) tabagismo C) ipertensione D) tutti i precedenti E) nessuno dei precedenti
 tabagismo. C) ipertensione. D) tutti i precedenti. E) nessuno dei precedenti.")
6
Dati di incidenza US per 2003-2004
(National Program of Cancer Registries) Fattori di rischio “comportamentali” nella popolazione US (Behavioral Risk Factor Surveillance System) Urology 73: , 2009
 Fattori di rischio comportamentali nella popolazione US. (Behavioral Risk Factor Surveillance System) Urology 73: ,")
8
Aprile 2005 Citologia urinaria: “Non elementi cellulari atipici.Presenza di emazie ben conservate”.

9
? E’ necessario un accertamento bioptico? A) Si B) No
 Si B) No")
10
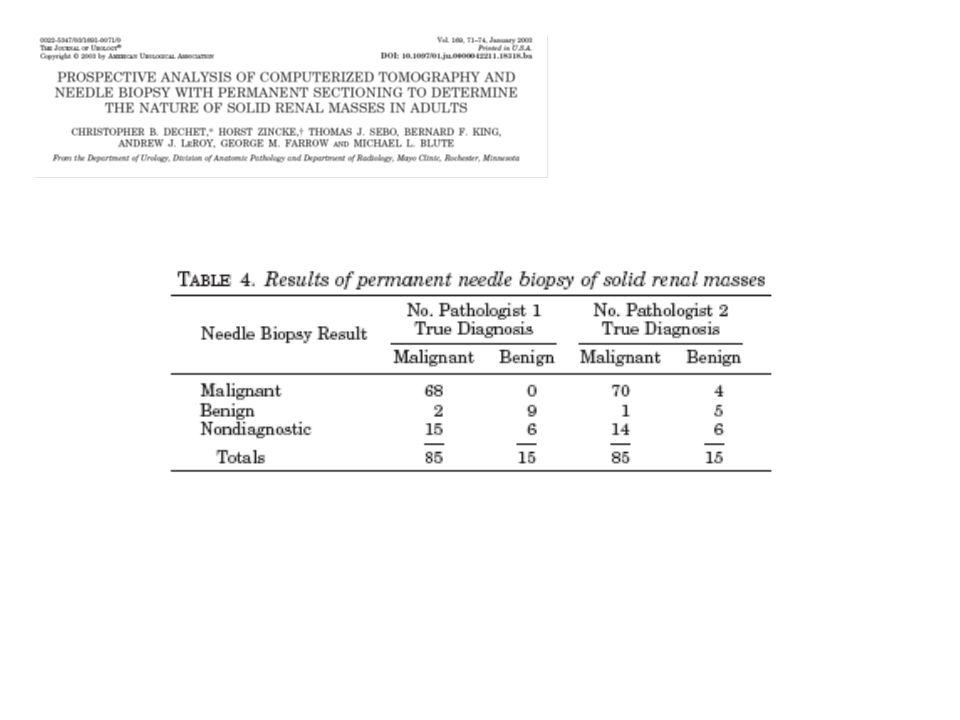
“Fine needle biopsy has been shown to have limited role in the work-up of patients with RCC, but may be considered in selected cases”.

11
2770 Pz. sottoposti a chirurgia per masse renali solide dal 1997 al 2000
Masse ≤ 1 cm Benigne 46.3% Maligne 53.7% Masse ≥ 7 cm benigne 6.3% maligne 93.7% Benigne (12.8%) Maligne: 87.2% Frank I, J Urol 170: , 2003
 Maligne: 87.2% Frank I, J Urol 170: ,")
13
Radiology 240: 6-22, 2006 “ In other words, the positive predictive value of imaging findings is so high that a negative biopsy results does not alter management”

14
Maggio 2005 Nefroureterectomia dx
“Neoformazione di 5.5 cm aggettante nella regione dell’ilo renale. Carcinoma a cellule renali, del tipo a cellule chiare. Furhman grade: 1” T3bN0M0 (III stadio)
")
15
? E’ indicato un trattamento adiuvante? A) No B) Si
 No B) Si")
16
Frequency of post-nephrectomy recurrence
Despite the finding of pathologically confined disease at the time of nephrectomy, 20 to 30% of patients will demonstrate local recurrence or distant metastasis after nephrectomy. 1 y : 43% 2 y: 70% 3 y: 80% 5 y: 93% They have been known to occur as many as 30 yrs post-nephrectomy Kattan MW et al, J Urol 166: 63-67, Chin AI et al., Rev Urol 8: 1-7, 2006 Levy DA et al, J Urol 159: , Ljungberg B et al, BJU Int 84: , 1999 Sorbellini M et al, J Urol 173: 48-51, 2005 Zisman A et al, J Clin Oncol 20: , 2002

17
Prognostic models for predicting disease recurrence
Crispen PL, Cancer 113: , 2008

18
Prognostic models for predicting disease recurrence: the UCLA Integrated Staging System (UISS)
Based on: TNM, ECOG PS, GRADE 90.4% 61.8% 41.9% Lam JS, J Urol 174: , 2005

19
Associations between conventional prognostic indices and molecular biomarkers
lack of external validation = lack of generalizability* * J Clin Epidemiol 56: , 2003 Clin Cancer Res 10: , 2004

20
R Observation 12 cycles IFN-a q3w 283 PATIENTS
-radical nephrectomy (RCC) pT3/4 N0/1 R 12 cycles IFN-a q3w - 3 MU day 1 2 MU day 2 5 MU day 3, 4, 5 JCO 21: , 2003
 pT3/4. N0/1. R. 12 cycles IFN-a q3w. - 3 MU day 1. 2 MU day 2. 5 MU day 3, 4, 5. JCO 21: ,")
21
PFS and OS Median PFS: 3 yrs vs 2.2 yrs Median OS: 7.4 yrs vs 5.1 yrs
JCO 21: , 2003

22
R Observation 1 course IL-2 69 PATIENTS -radical nephrectomy (RCC)
pT3/4 or N1-3 R 1 course IL-2 UI/Kg q8hours On days 1-5 and 15-19 JCO 21: , 2003

23
DFS and OS Early closure occurred when an interim analysis determined that the planned 30% improvement in 2-yrs DFS could not be achieved.

24
R Observation Vitespen 819 PATIENTS - nephrectomy (RCC) pT1b/4 or N1-2
25 µg/w i.d. for 4 wks, then q2w, until progression Lancet 372: , 2008

25
RFS and OS

27
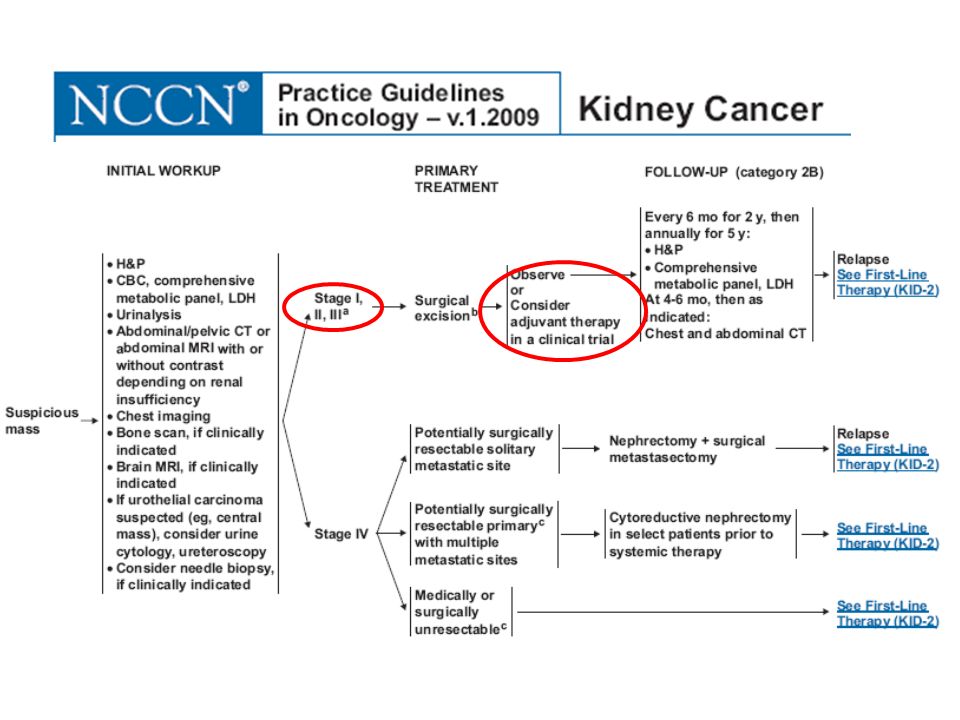
Observation remains standard care after nephrectomy, and eligible patients should be enrolled in randomized clinical trials, if available. Radiation therapy after nephrectomy is not beneficial, even in patients with nodal involvement

28
Contemporary adjuvant trials for high-risk localized RCC
Studi in corso da Cancer

29
Maggio 2005

30
Postnephrectomy surveillance protocol for localized RCC
Ideally based on risk stratification. Low risk Intermediate risk High risk Yearly: H&P and laboratory tests H&P, laboratory tests q 6 mos for 3 yrs then yearly through 10th yr H&P, laboratory tests q 6 mos for 3 yrs then yearly through 10th y Yearly chest CT for 5 yrs* Chest CT q 6 mos for 3 yrs then yearly through 10th y Chest CT q 6 mos for 3 yrs then yearly through 10th y Abdominal CT at year 2 and 4 Abdominal CT yearly for 2 yrs than every 2 yrs through 10th y Abdominal CT q 6 mos for 2 yrs then yearly through 5 y, then q 2 yrs through 10th y Rev Urol, 8: 1-7, 2006 Curr Urol Rep 6: 7-8, 2005 J Urol 174: , 2005 * Chest radiogram can alternate after 3y

31
Novembre 2007 RX arto sup. sx: “perdita della normale architettura della componente cortico-spugnosa del tratto prossimale omero sx che appare rigonfio e con interruzione delle limitanti corticali. Il segmento osseo presenta tipico aspetto a nido d’ape”. Frattura patologica dell’omero TAC omero sx: “estesa alterazione strutturale osteolitica della regione metafisaria…estesa erosione della corticale ossea con ampie soluzioni di continuo a tutto spessore….”

32
Novembre 2007 Intervento di osteosintesi dell’omero sx.
Istologia:” carcinoma renale a cellule chiare” TAC TORACE: negativa TAC ADDOME: area di grossolana osteolisi a carico del corpo di L1 SCINTIGRAFIA OSSEA: aree di alterata captazione del radiotracciante in corrispondenza dell’omero sx e di L1

33
Dicembre 2007 Giunge alla nostra osservazione.
Obiettivamente: apparecchio gessato arto sup sx PS 1 lieve dolenzia regione lombare C. radioterapica: indicato trattamento radiante (eseguito)
")
34
? Qual è l’aspettativa di vita a 5 anni di pazienti con RCC metastatico? A) 25% B) 40% C) 60% D) non determinato
 25% B) 40% C) 60% D) non determinato.")
35
Surveillance Epidemiology and End Results (SEER) data
Stage yrs survival rate I 96% II 82% III 64% IV 23%

36
Metodi: 670 pazienti trattati al MSKCC per mRCC dal 1975 al 1996
Obiettivo: identificazione di caratteristiche pre-trattamento con significato prognostico Metodi: 670 pazienti trattati al MSKCC per mRCC dal al 1996 Analisi sopravvivenza (Kaplan-Meier e Cox multivaiate analysis) JCO 17: , 1999
 JCO 17: ,")
37
INDEPENDENT PROGNOSTIC FACTORS
- Low Karnofsky PS (< 80) - High serum LDH (> 1.5 x ULN) - Low Hb (below the LLN) - High “corrected” Ca (> 10 mg/dl) - No prior nephrectomy JCO 17: , 1999
 - High serum LDH (> 1.5 x ULN) - Low Hb (below the LLN) - High corrected Ca (> 10 mg/dl) - No prior nephrectomy. JCO 17: ,")
38
RISK STRATIFICATION Low 0 19.9 71 31 Intermediate 1 or 2 10.3 42 7
STRATA No. Risk factors Median OS y OS (%) y OS (%) Low Intermediate or High > JCO 17: , 1999
 3-y OS (%) Low Intermediate 1 or High > JCO 17: ,")
39
Dicembre 2007 Intermediate risk
Performance Status: ECOG =1, Karnofsky= 80-90 Hgb: 12.2 g/dl (LLN= 12 g/dl) LDH: 642 U/L (ULN= 618 U/L) Calcio corretto: 10.5 mg/dl Intermediate risk
 LDH: 642 U/L (ULN= 618 U/L) Calcio corretto: 10.5 mg/dl. Intermediate risk.")
40
Dicembre 2007 SCELTA DEL TRATTAMENTO OTTIMALE Efficacia e tossicità
Precedenti trattamenti Fattori prognostici Co-morbidità Possibilità “burocratiche”

41
The cytokine era Garcia and Rini, CA Cancer J Clin 57: , 2007

42
Molecular Pathways and Targeted Therapies in Renal-Cell Carcinoma
Brugarolas J. N Engl J Med 2007;356:

43
? Quale trattamento ritenete indicato nella prima linea metastatica?
A) Sunitinib B) Bevacizumab+ IFN C) Temsirolimus D) tutti i precedenti
 Sunitinib. B) Bevacizumab+ IFN. C) Temsirolimus. D) tutti i precedenti.")
44
First-line Second-line Third-line
Current treatment options for mRCC based on data from randomized phase III trials SETTING THERAPY First-line Low-intermediate risk Sunitinib, bevacizumab + IFN Citokines High risk Temsirolimus Second-line Prior cytokine or TKI Sorafenib Prior bevacizumab Sunitinib Third-line Prior TKI Clinical trial?

45
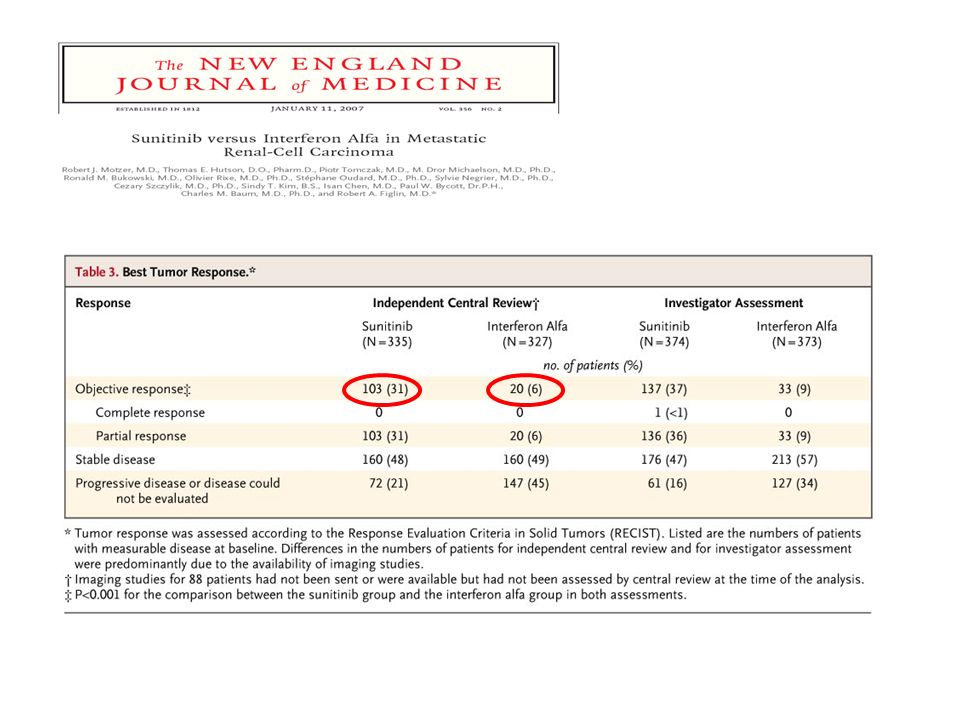
R N= 750 pts CC histology no prior systemic tx ECOG PS 0-1
measurable disease SUNITINIB 50 mg PO qD 4wON – 2wOFF R IFN-a 9 MU SC TIW Crossover allowed after interim analysis Motzer et al, NEJM 356:

47
NEJM 356: , 2007 ASCO 2008 Motzer R et al. N Engl J Med 2007;356:

48
Relevant Sunitinib side effects
Fatigue Hypertension Mucositis Hand-foot syndrome Neutropenia Hypothyroidism

49
R N= 649 pts CC histology no prior systemic tx ECOG PS 0-1
measurable disease IFN-a 9MU 3 times/w +Placebo R IFN-a 9MU 3 times/w + Bevacizumab 10mg/kg q2w Lancet 370: , 2007

50
ORR 31% vs 13% Median PFS: 10.2 vs 5.4 mos (HR 0.63) Median OS
(251 of 445 deaths required) NR vs 19.8mos (HR 0.79)
 NR vs 19.8mos (HR 0.79)")
51
R N= 626 pts HIGH RISK LDH 1.5 X ULN Low hemoglobin
C. calcium >10 mg/dl diagnosis-R> 1yr PS 60-70 metastasis multi organs IFN-a 3-18MU 3 times/w R Temsirolimus 25 mg/w IFN-a 3-18MU 3 times/w + Temsirolimus 25 mg/w NEJM 356: , 2007

52
ORR TEM 8.6% IFN 4.8% TEM+IFN 8.1 Median OS TEM: 10.9 mos (HR 0.73) IFN: 7.3 mos (HR 1) TEM+IFN: 8.4 mos (HR 0.96) Median PFS TEM 5.5 mos IFN 3.1 mos TEM+IFN 4.7 mos

53
Novembre 2007 Inizia trattamento con Sunitinib 50 mg/die PO per 4 settimane seguite da 2 di riposo. Dopo primo ciclo: mucosite G3, Dose ridotta a 37.5 mg Dopo il secondo ciclo: Hgb 9.5 g/d MCV femtolitri Inizia Epoetina- U/w

54
Marzo 2008 TAC torace-addome-braccio: SD Continua Sunitinib a 37.5 mg
Dopo il III ciclo: Hgb 10.5 g/dl (sospende epoetina) MCV femtolitri Dopo il IV ciclo: Hgb 11 g/dl MCV femtolitri B12 folati nella norma reticolociti TSH, FT3, FT4
 MCV femtolitri. Dopo il IV ciclo: Hgb 11 g/dl. MCV femtolitri. B12. folati nella norma. reticolociti. TSH, FT3, FT4.")
55
NEJM 356: 23330, 2007

56
Non correlata a B12 o folati
Macrocitosi in 67 pazienti trattati con Sunitinib, ma non in 31 trattati con Sorafenib Non correlata a B12 o folati Probabile effetto della inibizione di cKit Cancer 113: , 2008

57
Luglio 2008 TAC torace: multiple formazioni nodulari parenchimali di carattere secondario, bilateralmente (comprese tra 5 e 13 mm). TAC addome-pelvi: zone di osteolisi a livello del corpo di L5 e D8. Grossolana zona di osteolisi interessante l’ala sacrale dx con superamento della sincondrosi sacro-iliaca omolaterale ed estensione ai tessuti molli contigui

58
? Quale tra i seguenti farmaci ritenete indicato come trattamento di II-linea? A) Sorafenib C) Temsirolimus D) Bevacizumab + IFN
 Bevacizumab + IFN.")
59
R N= 903 pts IFN-refractory Crossover allowed after interim analysis
SORAFENIB 400mg twice/d N= 903 pts IFN-refractory R PLACEBO Crossover allowed after interim analysis NEJM 356: , 2007

60
INTERIM ANALYSIS Median OS Placebo mos Sorafenib NR (HR 0.72) Median PFS Placebo mos Sorafenib mos (HR 0.44) FINAL ANALYSIS Placebo mos Sorafenib mos (HR 0.77) Sorafenib mos (HR 0.51)
 FINAL ANALYSIS. Placebo 15.9 mos. Sorafenib 19.3mos (HR 0.77) Sorafenib 5.5 mos (HR 0.51)")
61
Luglio 2008 Nuovo trattamento radioterapico
Inizia Sorafenib (400 mg/die)
")
62
Ottobre 2008 La paziente lamenta dispnea ed astenia
TAC torace-addome: abbondante versamento pleurico sx. Quadro di linfangite carcinomatosa

63
? Ritenete che la sola BSC sia una giustificata in questo caso? A) Si
B) No
 No.")
64
410 con mRCC progrediti dopo Sunitinib, Sorafenib o entrambi
Median PFS Everolimus 4.0 mos Placebo: mos HR 0.3 Lancet 372: , 2008

65
Novembre 2008 Everolimus (RAD001) extended access trial 2 cycles
 extended access trial 2 cycles")
66
FDA Approves Everolimus for Renal Cell Cancer When Sunitinib or Sorafenib Fail
NEW YORK -- March 30, The US Food and Drug Administration (FDA) has approved everolimus (Afinitor) for patients with advanced renal cell carcinoma (RCC) after failure of treatment with sunitinib (Sutent) or sorafenib (Nexavar).
 has approved everolimus (Afinitor) for patients with advanced renal cell carcinoma (RCC) after failure of treatment with sunitinib (Sutent) or sorafenib (Nexavar).")
Presentazioni simili












>")







