Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
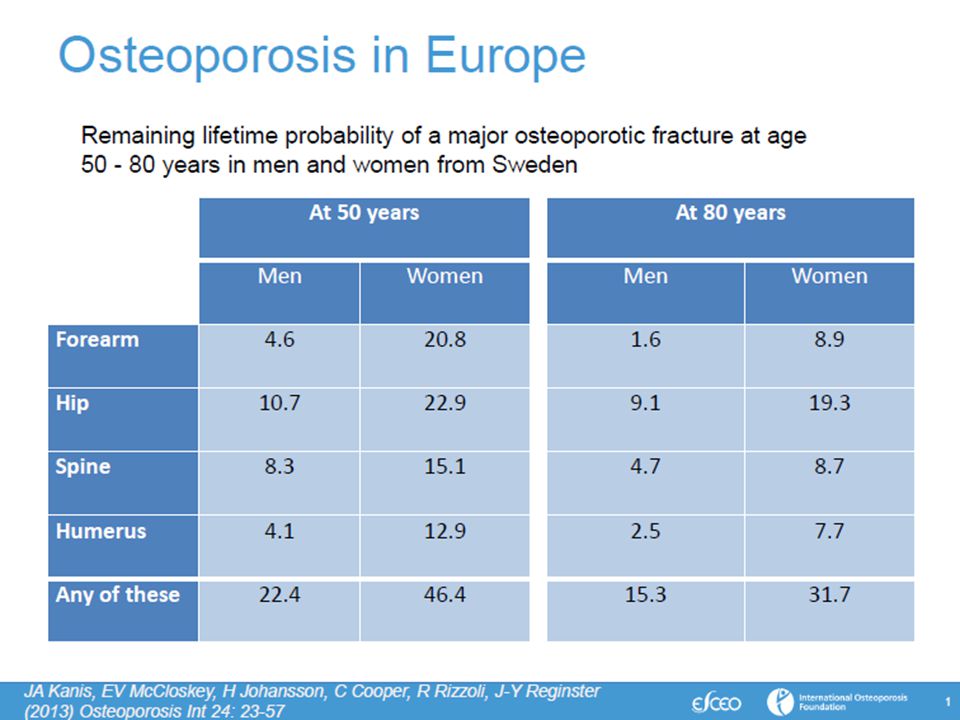
Terapia e prevenzione dell’osteoporosi
Stefania Maggi CNR Sezione Invecchiamento Padova

5
increase exponentially
As trabecular and cortical bone loss progresses, vertebral and hip fracture rates increase exponentially Hip fractures Vertebral fractures 400 Early increased incidence of vertebral fracture correlating with early trabecular bone loss Later increased incidence of hip fracture correlating with accumulation of trabecular and cortical bone loss 300 Incidence per 10,000 women per year 200 100 Key Points In women after menopause fractures occur throughout the skeleton and the incidence accelerates with ageing.1 Vertebral fracture incidence is high early on after menopause correlating with early trabecular bone loss Later increased incidence of hip fracture correlate with the accumulation of trabecular and cortical bone loss Supplemental Information Osteoporotic fractures occur throughout the skeleton; the most common fractures are those of the hip, spine and wrist.2 The incidence of all osteoporotic fractures increases with age.1,3 Epidemiological studies have shown, for women aged >50 years, the most common fractures are hip (26% of all fractures) and vertebral (15%).3 In women, the incidence of hip fracture (a bone site comprised of >75% cortical bone)4 – the most devastating result of osteoporosis in terms of hospitalization, disability and mortality – increases exponentially from the age of approximately 70 years.1 The incidence of vertebral fractures (a site comprised of ~70% trabecular bone)4 is high following the menopause and accelerates beyond the age of 50 years.1 References 1. Sambrook P & Cooper C. Lancet 2006;367:2010–2018. 2. Johnell O & Kanis JA. Osteoporos Int 2006;17:1726–1733. 3. Kanis JA et al. Osteoporos Int 2005;16:229–238. 4. Dempster DW. Primer on the metabolic bone diseases and disorders of bone metabolism. 6th ed. 2006; p.7–11. 50−54 55−59 60−64 65−69 70−74 75−79 80−84 85+ Age (years) Adapted from: Sambrook P & Cooper C. Lancet 2006;367:2010–2018.
 and vertebral (15%).3. In women, the incidence of hip fracture (a bone site comprised of >75% cortical bone)4 – the most devastating result of osteoporosis in terms of hospitalization, disability and mortality – increases exponentially from the age of approximately 70 years.1. The incidence of vertebral fractures (a site comprised of ~70% trabecular bone)4 is high following the menopause and accelerates beyond the age of 50 years.1. References. 1. Sambrook P & Cooper C. Lancet 2006;367:2010– Johnell O & Kanis JA. Osteoporos Int 2006;17:1726– Kanis JA et al. Osteoporos Int 2005;16:229– Dempster DW. Primer on the metabolic bone diseases and disorders of bone metabolism. 6th ed. 2006; p.7–11. 50−54. 55−59. 60−64. 65−69. 70−74. 75−79. 80− Age (years) Adapted from: Sambrook P & Cooper C. Lancet 2006;367:2010–2018.")
6
Decrease Fracture Risk
Multiple Factors May Mitigate Fracture Risk Therapeutic Interventions Lifestyle Modifications Slowing/Stopping Bone Loss Minimizing Factors that Contribute to Falls Maintaining or Increasing Bone Density and Strength Decrease Fracture Risk Maintaining or Improving Bone Microarchitecture Modification of Risk Factors (diet, exercise) Improving Medication Adherence NAMS Position Statement. Menopause. 2006;13: Heaney, RP. Bone. 2003;33: Siris ES, et al. Mayo Clin Proc. 2006;81:
 Improving Medication. Adherence. NAMS Position Statement. Menopause. 2006;13: Heaney, RP. Bone. 2003;33: Siris ES, et al. Mayo Clin Proc. 2006;81:")
10
Effective Treatment Is Based on Efficacy, Safety/Tolerability and Adherence
+ Safety/Tolerability + Adherence The capacity for beneficial change, or therapeutic effect of a given intervention Defined as freedom from undesirable side- effects/adverse events, and decrease in susceptibility to the effects of a medication resulting from continued administration Reflects a combination of behaviours determining the extent to which patients take medications as prescribed Payer J, et al. Biomed Pharmacother 2007;61:

11
+ Adherence Encompasses Both Persistence and Compliance Adherence
Reflects a combination of behaviours determining the extent to which patients take medications as prescribed Adherence Persistence Compliance + The length of time from beginning to completion or discontinuation of therapy The consistency and accuracy with which a prescribed regimen is followed Payer J, et al. Biomed Pharmacother 2007;61:

12
Osteoporosis Therapies and Patient Adherence
Less than 50% of patients persist with their osteoporosis therapy for more than 1 year Patients initiating therapy Side effects Safety concerns Health problems Lack of results Lack of motivation Cost Inconvenient dosing Withdrawn by others Adherence Patients continuing therapy Siris E.S. et al. Am. J. Med. 2009; 122: S3-S13

13
Increased Risk of Fracture
Poor Adherence is Associated with Increased Fracture Risk Fracture Risk by Adherence Level low high p < p = p = 0.12 1.21 1.18 1.09 1 Increased Risk of Fracture high Adherence Level low Huybrechts KF, et al. Bone. 2006;38: Data from 38,000 women in a managed care database

14
Denosumab lega il RANK Ligando inibendo la formazione, la funzione e la sopravvivenza degli osteoclasti RANKL RANK OPG Denosumab CFU-M Pre- Osteoclasti Ormoni Fattori di crescita Citochine Inibizione della formazione, funzione e sopravvivenza degli osteoclasti Denosumab is the first fully human monoclonal antibody in clinical development that specifically targets RANK ligand, an essential mediator of osteoclast formation, function, and survival.1,2 Lewiecki EM. RANK ligand inhibition with denosumab for the management of osteoporosis. Exper Opin Biol Ther. 2006;6: McClung MR, Lewiecki EM, Cohen SB, et al. Denosumab in postmenopausal women with low bone mineral density. N Engl J Med. 2006;354: Osteoblasti Formazione ossea Inibizione del riassorbimento osseo In presenza di M-CSF CFU-M= unità formante colonie macrofagiche M-CSF= fattore stimolante le colonie macrofagiche Adattato da: Boyle WJ, et al. Nature. 2003;423: 14

15
Proprietà farmacologiche di denosumab
Anticorpo monoclonale completamente umano – isotipo IgG2 Elevata affinità per il RANK Ligando umano Elevata specificità per il RANK Ligando Legame con TNF-α, TNF-β, TRAIL, o CD40L non rilevabile Ad oggi non è stata osservata la formazione di anticorpi neutralizzanti nel corso degli studi clinici Struttura di denosumab Ig = immunoglobuline; TNF = tumor necrosis factor; TRAIL = TNF-α–related apoptosis-inducing ligand. Bekker PJ, et al. J Bone Miner Res. 2004;19: Elliott R, et al. Osteoporos Int. 2007;18:S54. Abstract P149. McClung MR, et al. N Engl J Med. 2006;354:

16
Pharmacokinetic and Pharmacodynamic Properties of Denosumab
Administered via subcutaneous (SC) injection Reduction in bone turnover markers within 3 days and sustained for up to 6 months The maximum denosumab serum concentration (Cmax) occurred in 10 days for the 60 mg SC dose (range: 2–28 days) Mean half-life is 25.4 days (SD 8.5 days) with 60 mg SC dosing Serum denosumab concentrations declined over 4–5 months No accumulation or change in denosumab pharmacokinetics with time was observed upon multiple dosing Dosing schedule: every 6 months At the end of each dosing interval, CTX reductions were partially attenuated from a maximal reduction of ≥ 87% to ≥ 45% (range 45% to 80%), as serum denosumab levels diminished, reflecting the reversibility of the effects of denosumab on bone remodeling. These effects were sustained with continued treatment. Upon reinitiation, the degree of inhibition of CTX by denosumab was similar to that observed in patients initiating denosumab treatment.1 The half-life of denosumab is similar to that reported for some monoclonal antibodies and for purified antiviral antibodies, total IgG, IgG1, or IgG2.2 Denosumab Summary of Product Characteristics, Amgen. 2010 Jang G, et al. J Bone Miner Res. 2006;21(suppl 1):S190. Abstract SA403 and poster. SD = standard deviation Denosumab Summary of Product Characteristics, 2012
 injection. Reduction in bone turnover markers within 3 days and sustained for up to 6 months. The maximum denosumab serum concentration (Cmax) occurred in 10 days for the 60 mg SC dose (range: 2–28 days) Mean half-life is 25.4 days (SD 8.5 days) with 60 mg SC dosing. Serum denosumab concentrations declined over 4–5 months. No accumulation or change in denosumab pharmacokinetics with time was observed upon multiple dosing. Dosing schedule: every 6 months. At the end of each dosing interval, CTX reductions were partially attenuated from a maximal reduction of ≥ 87% to ≥ 45% (range 45% to 80%), as serum denosumab levels diminished, reflecting the reversibility of the effects of denosumab on bone remodeling. These effects were sustained with continued treatment. Upon reinitiation, the degree of inhibition of CTX by denosumab was similar to that observed in patients initiating denosumab treatment.1. The half-life of denosumab is similar to that reported for some monoclonal antibodies and for purified antiviral antibodies, total IgG, IgG1, or IgG2.2. Denosumab Summary of Product Characteristics, Amgen Jang G, et al. J Bone Miner Res. 2006;21(suppl 1):S190. Abstract SA403 and poster. SD = standard deviation. Denosumab Summary of Product Characteristics,")
17
Studio DAPS Disegno dello studio
V I S T A D C R E N G F I N E D L O S T U V I S T A G O R N 1 N = 250 Denosumab 60 mg SC Q6M Alendronato mg orale QW Anno 1 Anno 2 Alendronato mg orale QW Denosumab 60 mg SC Q6M Crossover Randomizzazione 1:1 6 mesi 12 mesi 18 mesi 24 mesi Visite dello studio 0-35 giorni 24 mesi Multicentrico, randomizzato, in aperto, di crossover Tutti i soggetti hanno ricevuto una supplementazione quotidiana con 1000 mg di calcio e ≥ 400 UI di vitamina D Kendler DL et al. Osteoporos Int 2011; 22:

18
Non-aderenza, non-compliance e non-persistenza maggiori per alendronato al primo anno
Denosumab (N = 126) Alendronato (N = 124) 5 10 15 20 25 Non Aderenza Compliance Persistenza RRR = 46% P = 0.026 RRR = 52% P = 0.014 RRR = 50% P = 0.029 Percentuale di soggetti RRR = riduzione rischio relativo Kendler DL et al. Osteoporos Int 2011; 22: Freemantle N et al. Osteoporos Int 2012;23:
 Alendronato (N = 124) Non. Aderenza. Compliance. Persistenza. RRR = 46% P = RRR = 52% P = RRR = 50% P = Percentuale di soggetti. RRR = riduzione rischio relativo. Kendler DL et al. Osteoporos Int 2011; 22: Freemantle N et al. Osteoporos Int 2012;23:")
19
Non-aderenza, non-compliance e non-persistenza maggiori per alendronato anche al 2° anno
Denosumab (N = 106) Alendronato (N = 115) Non Aderenza Compliance Persistenza RRR = 80% P < 0.001 RRR = 91% 10 20 30 40 Percentuale di soggetti RRR = riduzione rischio relativo Kendler DL et al. Osteoporos Int 2011; 22: Freemantle N et al. Osteoporos Int 2012;23:
 Alendronato (N = 115) Non. Aderenza. Compliance. Persistenza. RRR = 80% P < RRR = 91% Percentuale di soggetti. RRR = riduzione rischio relativo. Kendler DL et al. Osteoporos Int 2011; 22: Freemantle N et al. Osteoporos Int 2012;23:")
20
Maggiore soddisfazione e preferenza per denosumab rispetto ad alendronato
Per niente/scarsa/moderata Compressa Abbastanza/Molto Iniezione 20 40 60 80 100 Convenienza Modalità: Compressa vs Iniezione DMab ALN Frequenza di somministrazione Percentuale di soggetti 38% 62% 7% 93% 31% 69% 9% 91% 37% 63% 5% 95% 20 40 60 80 100 Percentuale di soggetti 92% 91% 8% 9% Preferita Preferita nel lungo termine Kendler DL et al. Osteoporos Int 2011; 22: Freemantle N et al. Osteoporos Int 2012;23:

21
CONCLUSIONI L’Osteoporosi è un problema di salute pubblica molto rilevante e resterà tale nei prossimi anni Gli interventi di prevenzione e di trattamento ad oggi implementati non riflettono le profonde conoscenze scientifiche raggiunte sull’efficacia degli stessi

Presentazioni simili


 Brussels, 26 settembre 2013.>")











>")






