Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
La trombosi arteriosa: cosa deve sapere il medico non specialista
La trombosi arteriosa: cosa deve sapere il medico non specialista. Il ruolo del cardiologo Renato Rosiello Laboratorio di Cardiologia Interventistica U.O. di Cardiologia Azienda Ospedaliera Carlo Poma Mantova

3
Tombosi arteriosa Il comune denominatore in tutti i pazienti ricoverati per SCA è un evento coronarico o tromboembolico nel quale gioca un ruolo determinante la trombosi: la rottura di una placca aterosclerotica, l’attivazione della cascata emocoagultiva e delle piastrine e la conseguente formazione di un trombo

4
Fibrinolytic ineffective Antiplatelet effective
Ruolo delle piastrine e della fibrina nella instabilizzazione di placca Fibrinolytic ineffective Antiplatelet effective Platelet-Rich Thrombus Antiplatelet Effective Fibrinolytic Ineffective Unstable Angina Platelets Platelet-Fibrin Thrombus Fibrinolytic Effective Acute MI Fibrin

5
“Targets” della trombosi mediata dalle piastrine
Abciximab, eptifibatide, tirofiban ticlopidine clopidogrel prasugrel ticagrelor ADP (P2Y12) Receptor GP IIb/IIIa Receptor Intact Endothelium Endothelial Damage Collagen vWF (Α2β3 Integrin) Platelet Collagen Receptor (GPIa) Platelet vWF Receptor (GP1b) TXA2 Receptor ADP TXA2 aspirin Concentrerò la presentazione sull’aspirina (inibitore della COX1) e sugli inibitori dell’attivazione piastrinica ADP mediata (inibitori del recettore P2Y12). I primi 3 sono tienopiridine di 1,2,3 generazione, il ticagrelor è un inibitore non tienopiridinico. Adhesion Activation Aggregation GP = glycoprotein; vWF = von Willebrand factor; ADP = adenosine diphosphate; TX = thromboxane. Meadows et al. Circulation Res. 2007;100: 5 5
 Receptor. GP IIb/IIIa Receptor. Intact Endothelium. Endothelial Damage. Collagen. vWF. (Α2β3 Integrin) Platelet Collagen Receptor (GPIa) Platelet vWF Receptor (GP1b) TXA2 Receptor. ADP. TXA2. aspirin. Concentrerò la presentazione sull’aspirina (inibitore della COX1) e sugli inibitori dell’attivazione piastrinica ADP mediata (inibitori del recettore P2Y12). I primi 3 sono tienopiridine di 1,2,3 generazione, il ticagrelor è un inibitore non tienopiridinico. Adhesion. Activation. Aggregation. GP = glycoprotein; vWF = von Willebrand factor; ADP = adenosine diphosphate; TX = thromboxane. Meadows et al. Circulation Res. 2007;100:")
22
Quale trattamento I cardini del trattamento per le SCA
Terapia con anticoagulanti, trombolitici ed antiaggreganti piastrinici Terapia complessa che utilizza vari farmaci la cui azione è specifica per un particolare punto della cascata della coagulazione

41
Terapia antiaggregante combinata
Primary Efficacy Results (MI/Stroke/CV Death) at 30 months by category inclusion criteria Ed in particolare per quanto riguarda la trombosi dello stent Bhatt al. N Engl J Med 2006
 at 30 months by category inclusion criteria. Ed in particolare per quanto riguarda la trombosi dello stent. Bhatt al. N Engl J Med")
42
Major Adverse Cardiac Events
Duplice antiaggregazione dopo impianto di stent coronarici ticlopidina vs clopidogrel Major Adverse Cardiac Events Bhatt et al. J Am Coll Cardiol 2002;39:9-14

43
Studio clopidogrel ticlopidina p value
Duplice antiaggregazione dopo impianto di stent coronarici ticlopidina vs clopidogrel NECESSITA’ DI SOSPENSIONE DELLA TERAPIA (neutropenia, diarrea, rush etc.) Studio clopidogrel ticlopidina p value Moussa CIRC Mller CIRC Bertrand CIRC (CLASSICS) Taniuchi CIRC (TOPPS)
 Studio clopidogrel ticlopidina p value. Moussa CIRC Mller CIRC Bertrand CIRC (CLASSICS) Taniuchi CIRC (TOPPS)")
44
Duplice antiaggregazione dopo impianto di stent coronarici
Stent metallici (BMS) Classe I For post-PCI patients receiving a BMS, dual antiplatelet therapy should be given for a minimum of 1 month (level of Evidence: A) ACC/AHA 2007 PCI Guidelines update
 Classe I. For post-PCI patients receiving a BMS, dual antiplatelet therapy should be. given for a minimum of 1 month (level of Evidence: A) ACC/AHA 2007 PCI Guidelines update.")
45
Duplice antiaggregazione dopo impianto di stent coronarici
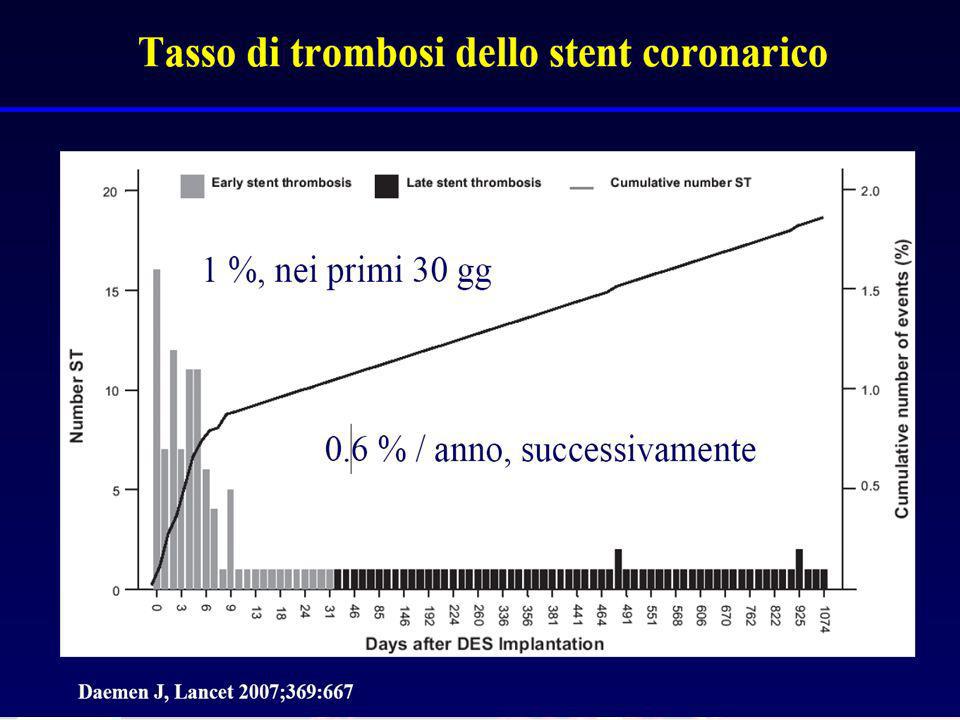
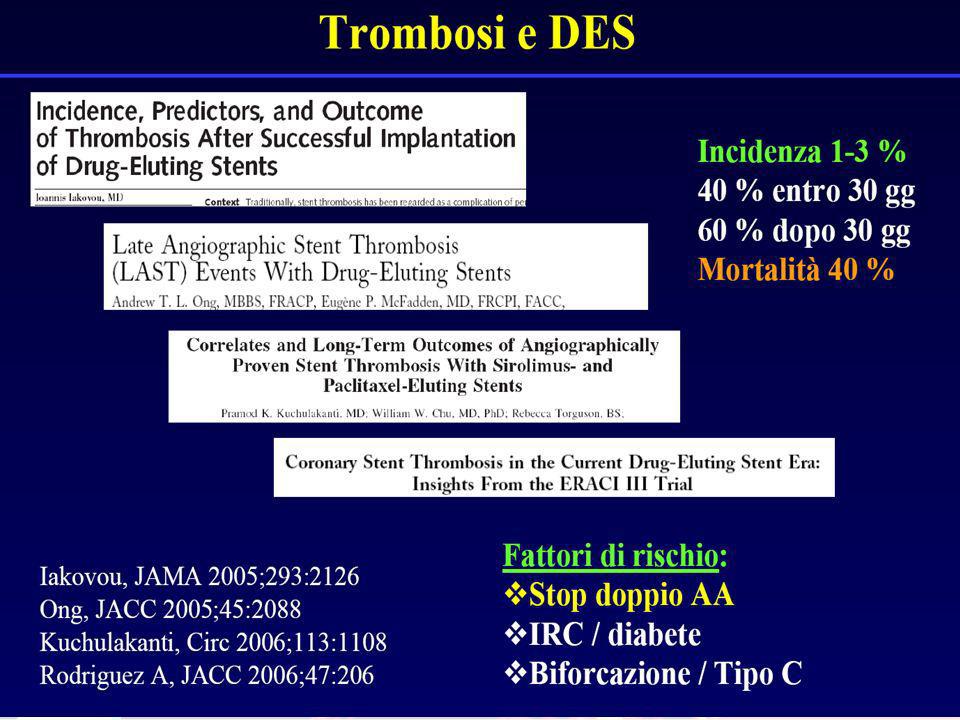
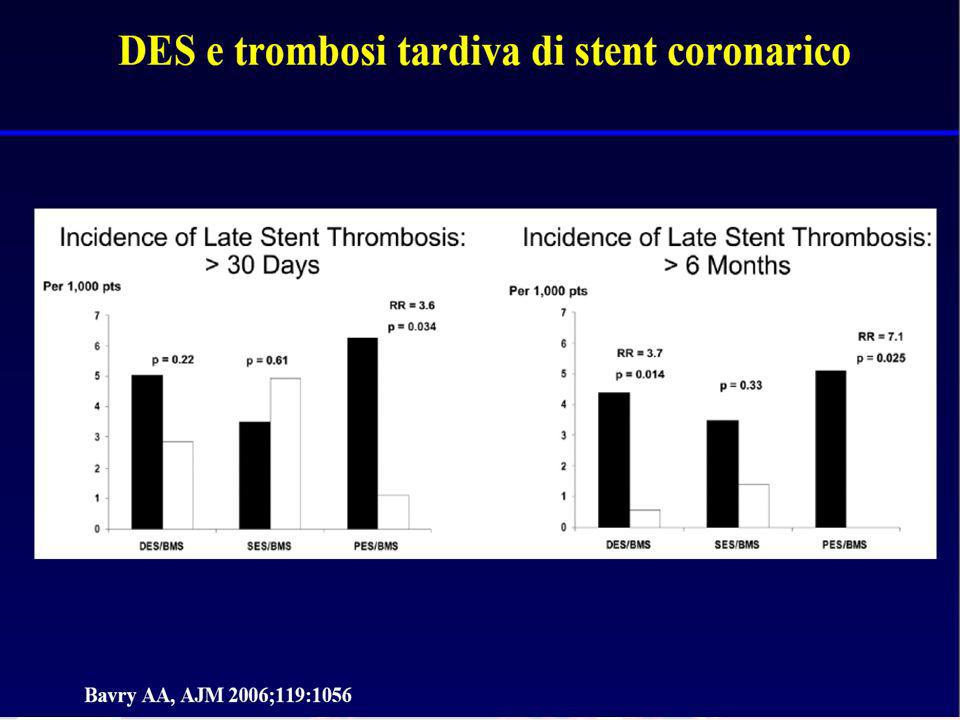
Stent medicati (DES) Il problema della trombosi tardiva NEI TRIALS RANDOMIZZATI L’INCIDENZA CUMULATIVA AD UN FOLLOW-UP DI 9-12 MESI = 0.7 – 1.2% NEI REGISTRI “REAL WORLD”, PIÙ RAPPRESENTATIVI DELLA PRATICA CLINICA QUOTIDIANA, L’INCIDENZA E’ 2-3 VOLTE SUPERIORE Kaul S et al. JACC 2007
 Il problema della trombosi tardiva. NEI TRIALS RANDOMIZZATI L’INCIDENZA CUMULATIVA AD UN. FOLLOW-UP DI 9-12 MESI = 0.7 – 1.2% NEI REGISTRI REAL WORLD , PIÙ RAPPRESENTATIVI DELLA PRATICA. CLINICA QUOTIDIANA, L’INCIDENZA E’ 2-3 VOLTE. SUPERIORE. Kaul S et al. JACC")
46
Durata della duplice antiaggregazione dopo impianto di stent medicati
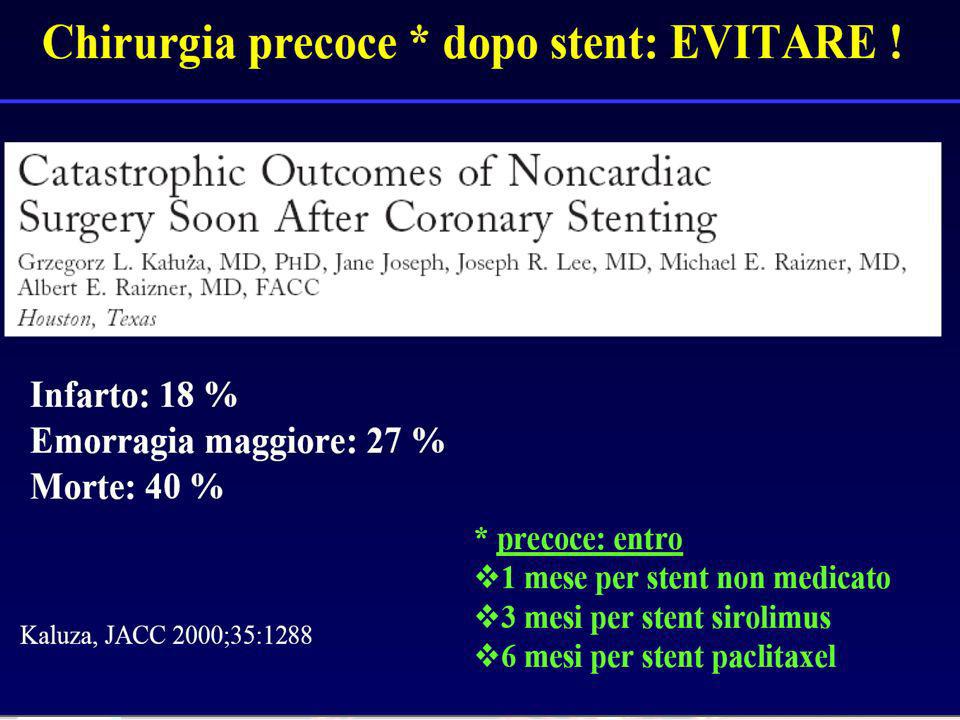
PCI Guidelines 2005 Classe I In patients who have undergone PCI, clopidogrel 75 mg daily should be given for at least 3 months after sirolimus stent implantation, and 6 months after paclitaxel stent implantation, and ideally up to 12 months in patients who are not at high risk of bleeding. (Level of Evidence: B) PCI Guidelines UPDATE 2007 Classe I For all post-PCI stented patients receiving a DES, clopidogrel 75 mg daily should be given for at least 12 months if patients are not at high risk of bleeding. (Level of Evidence: B) ACC/AHA PCI Guidelines
 PCI Guidelines UPDATE Classe I. For all post-PCI stented patients receiving a DES, clopidogrel 75 mg daily should be given for at least 12 months if patients are not at high risk of bleeding. (Level of Evidence: B) ACC/AHA PCI Guidelines.")
47
Durata della duplice antiaggregazione dopo impianto di stent medicati
For patients with clinical features associated with stent thrombosis, such as renal insufficiency, diabetes, or procedural characteristics such as left main, bifurcating left main, single patent coronary vessel, multiple stents or treatment of a bifurcation lesion, extended DAT beyond 1 year may be reasonable. ACC/AHA 2007 PCI Guidelines update

48
Durata della duplice antiaggregazione dopo impianto di stent medicati
In patients with coronary anatomy who are at very high risk of fatal stent thrombosis (left main, last remaining vessel), the antiplatelet thetapy with ASA and a tienopyridine following DES implantation should be permanent, until different scientific evidence become available J Cardiovasc Med 2007;8:
, the antiplatelet thetapy with ASA and a tienopyridine following DES implantation should be permanent, until different scientific evidence become available. J Cardiovasc Med 2007;8:")
49
Clopidogrel and Prasugrel Formazione dei metaboliti attivi
CH3 O C O Pro-drug N N O O C S S Cl F C H Prasugrel Clopidogrel Pre-hepatic metabolism Esterases in blood (? Small intestine) 3 85% Inactive Metabolites Esterases in blood O N O S F The pathways leading to conversion of prasugrel and clopidogrel to their respective active metabolites differ In a competing metabolic reaction, esterases convert clopidogrel to inactive metabolites; this inactivation pathway accounts for an estimated 85% of a dose of clopidogrel28 Prasugrel is rapidly hydrolyzed in vivo by esterases to a thiolactone, which is subsequently metabolized to the active metabolite in a single step by several CYP enzymes: Mainly CYP3A4/5 and CYP2B6, and to a lesser extent by CYP2C19 and CYP2C927 Two sequential CYP-dependent oxidative steps are required to convert clopidogrel to its active metabolite The first step leads to formation of 2-oxo-clopidogrel, which is then metabolized to the active metabolite Enzymes involved in the metabolism of clopidogrel include CYP1A2, CYP2B6, CYP2C9, CYP2C19 and CYP3A4/529–31 Quindi è un processo più complesso e quindi almeno teoricamente polimorfismi di taliu citocromi (con ridotta attività) o farmaci che inibiscono in parte tali citocromi (es PPi) possono ridurre la quota attiva del clop e quindi il suo effetto. O CH3 O C N O S HOOC * HS N O Cl OCH3 Cl Hepatic Metabolism Cytochrome P450 HOOC N * HS F Active Metabolite Active Metabolite
 3. 85% Inactive. Metabolites. Esterases in blood. O. N. O. S. F. The pathways leading to conversion of prasugrel and clopidogrel to their respective active metabolites differ. In a competing metabolic reaction, esterases convert clopidogrel to inactive metabolites; this inactivation pathway accounts for an estimated 85% of a dose of clopidogrel28. Prasugrel is rapidly hydrolyzed in vivo by esterases to a thiolactone, which is subsequently metabolized to the active metabolite in a single step by several CYP enzymes: Mainly CYP3A4/5 and CYP2B6, and to a lesser extent by CYP2C19 and CYP2C927. Two sequential CYP-dependent oxidative steps are required to convert clopidogrel to its active metabolite. The first step leads to formation of 2-oxo-clopidogrel, which is then metabolized to the active metabolite. Enzymes involved in the metabolism of clopidogrel include CYP1A2, CYP2B6, CYP2C9, CYP2C19 and CYP3A4/529–31. Quindi è un processo più complesso e quindi almeno teoricamente polimorfismi di taliu citocromi (con ridotta attività) o farmaci che inibiscono in parte tali citocromi (es PPi) possono ridurre la quota attiva del clop e quindi il suo effetto. O. CH3. O. C. N. O. S. HOOC. * HS. N. O. Cl. OCH3. Cl. Hepatic Metabolism. Cytochrome P450. HOOC. N. * HS. F. Active Metabolite. Active Metabolite.")
50
Inibizione dell’aggregazione piastrinica Prasugrel vs Clopidogrel
Loading Dose Maintenance Doses 100 * * * * * 10 mg * * * * * p < vs. Clop 300 mg, 600 mg and 75 mg * * 80 60 mg † * 60 600 mg p < vs. Clop 300 mg/75 mg Inhibition of Platelet Aggregation (%) 75 mg 40 † 300 mg 20 Source: Page 369, Figure 7, IPA comparison during clopidogrel 300 mg or 600 mg versus prasugrel 60 mg (loading dose phase) and clopidogrel 75 mg versus prasugrel 10 mg (maintenance dose phase) from the published review article. Arrows indicate time of dose administration. Figure is adapted from Payne et al., Am J Cardiol 2006; 98 (Suppl 7):14. Si mantiene anche allo steady stete. La stessa cosa, anche se con differenza inferiore si verifica per carico di clop di 600 mg. Quindi gli studi di fase 2 dimostrano una maggiore potenza e più rapida insorgenza dell’attività antipiastinica per il prasugrel risptto al clopidogrel DA QUESTI STUDI di fase 2 IL RAZIONALE PER LO STUDIO DI FASE 3 Clop Pras 0.25 0.5 1 2 4 6 2 3 4 5 6 7 8 9 Time Day 1, Hours Days Payne et al., Am J Cardiol 2006; 98 (Suppl 7):14
 75 mg. 40. † 300 mg. 20. Source: Page 369, Figure 7, IPA comparison during clopidogrel 300 mg or 600 mg versus prasugrel 60 mg (loading dose phase) and clopidogrel 75 mg versus prasugrel 10 mg (maintenance dose phase) from the published review article. Arrows indicate time of dose administration. Figure is adapted from Payne et al., Am J Cardiol 2006; 98 (Suppl 7):14. Si mantiene anche allo steady stete. La stessa cosa, anche se con differenza inferiore si verifica per carico di clop di 600 mg. Quindi gli studi di fase 2 dimostrano una maggiore potenza e più rapida insorgenza dell’attività antipiastinica per il prasugrel risptto al clopidogrel. DA QUESTI STUDI di fase 2 IL RAZIONALE PER LO STUDIO DI FASE 3. Clop. Pras Time. Day 1, Hours. Days. Payne et al., Am J Cardiol 2006; 98 (Suppl 7):14.")
51
Prasugrel vs Clopidogrel TRITON-TIMI 38
Main Trial - Cumulative Incidence of Primary Endpoint and TIMI Major Bleeds Clopidogrel Prasugrel - 12.1 Primary Efficacy: CV Death, Nonfatal MI, Nonfatal Stroke P < 0.001 9.9 E questi sono i risultati principali del trial Riduzione degli eventi ischemici con un aumento degli eventi emorragici Key Safety: Non-CABG TIMI Major Bleed P = 0.03 2.4 1.8 Days after Randomization Wiviott S et al. NEJM 2007;357:

52
Timing of Benefit (landmark analysis)
Prasugrel vs Clopidogrel TRITON-TIMI 38 Timing of Benefit (landmark analysis) LOADING DOSE MAINTEINANCE DOSE Clopidogrel 6.9 5.6 Clopidogrel 5.6 4.7 Prasugrel Prasugrel Se ci concentriamo sugli end point di efficacia come si può vedere da un analisi landmark il beneficio del prasugrel inizia precocemente, già nelle prime ore dopo la dose di carico e si amplifica ulteriormente nel tempo P=0.01 P=0.003 Primary Endpoint: CV Death/ Nonfatal MI/ Nonfatal Stroke Wiviott S et al. NEJM 2007;357:
 LOADING DOSE. MAINTEINANCE DOSE. Clopidogrel Clopidogrel Prasugrel. Prasugrel. Se ci concentriamo sugli end point di efficacia come si può vedere da un analisi landmark il beneficio del prasugrel inizia precocemente, già nelle prime ore dopo la dose di carico e si amplifica ulteriormente nel tempo. P=0.01. P= Primary Endpoint: CV Death/ Nonfatal MI/ Nonfatal Stroke. Wiviott S et al. NEJM 2007;357:")
53
TIMI 38 stent analysis Stent Thrombosys: (N=12844)
2.35% 2.5 CLOPIDOGREL 2 52% % of Subjects 1.5 1.13% Subanalisi nei pazienti sottoposti ad impianto di stent che rappresentano il 94% della popolazione totale Riduzione di oltre il 50% della stent thrombosys PRASUGREL 1 1 year: 1.06 vs 2.15% HR 0.48 [ ], P<0.0001 DAYS 450 Wiviott ACC 2008 53

54
Ticagrelor (AZD 6140): an oral reversible P2Y12 antagonist
H O N N N H O H N F O Ticagrelor is a cyclo-pentyl-triazolo-pyrimidine (CPTP) N N F S O H Direct acting Not a prodrug; does not require metabolic activation Rapid onset of inhibitory effect on the P2Y12 receptor Greater inhibition of platelet aggregation than clopidogrel Reversibly bound Degree of inhibition reflects plasma concentration Faster offset of effect than clopidogrel Functional recovery of all circulating platelets
 N. N. F. S. O. H. Direct acting. Not a prodrug; does not require metabolic activation. Rapid onset of inhibitory effect on the P2Y12 receptor. Greater inhibition of platelet aggregation than clopidogrel. Reversibly bound. Degree of inhibition reflects plasma concentration. Faster offset of effect than clopidogrel. Functional recovery of all circulating platelets.")
55
Ticaglelor vs clopidogrel PLATO Primary efficacy endpoint over time (composite of CV death, MI or stroke) 8 8 6.60 Clopidogrel Clopidogrel 5.43 5.28 4 4 Cumulative incidence (%) 4.77 Ticagrelor Ticagrelor 2 2 HR 0.88 (95% CI 0.77–1.00), p=0.045 HR 0.80 (95% CI 0.70–0.91), p<0.001 10 20 30 31 90 150 210 270 330 No. at risk Days after randomisation Days after randomisation Ticagrelor 9,333 8,942 8,827 8,763 8,673 8,543 8,397 7,028 6,480 4,822 Clopidogrel 9,291 8,875 8,763 8,688 8,688 8,437 8,286 6,945 6,379 4,751 Wallentin et al. N Engl J Med 2009;361:
 Ticagrelor. Ticagrelor HR 0.88 (95% CI 0.77–1.00), p= HR 0.80 (95% CI 0.70–0.91), p< No. at risk. Days after randomisation. Days after randomisation. Ticagrelor. 9,333. 8,942. 8,827. 8,763. 8,673. 8,543. 8,397. 7,028. 6,480. 4,822. Clopidogrel. 9,291. 8,875. 8,763. 8,688. 8,688. 8,437. 8,286. 6,945. 6,379. 4,751. Wallentin et al. N Engl J Med 2009;361:")
56
Antiaggreganti piastrinici nel paziente cardiovascolare ad alto rischio “NET CLINICAL BENEFIT”
ASA ASA+ Clopidogrel -22% Reduction In Ischemic Events ASA+ Prasugrel -20% -19% Increase in Major Bleeds +32% +38% +60% Placebo APTC CURE TRITON-TIMI 38 Single Antiplatelet Rx DAT DAT Higher IPA

57
Linee guida ESC trattamento della FA
Aspirina 325 mg/die Età < 60 anni senza malattia cardiaca Età < 60 anni con malattia cardiaca ma senza fattori di rischio per ictus: scompenso cardiaco, EF < 35%, ipertensione arteriosa Età > 60 anni senza fattori di rischio* Anticoagulanti orali Età ≥ 60 anni con diabete o pregresso by-pass aorto-coronarico (INR 2.0) Età ≥ 75 anni (INR 2.0) Scompenso cardiaco ACC/AHA/ESC Guidelines for management of patients with atrial fibrillation 2006
 Età ≥ 75 anni (INR 2.0) Scompenso cardiaco. ACC/AHA/ESC Guidelines for management of patients with atrial fibrillation")
60
Conclusioni Nonostante una terapia medica aggressiva abbia sostanzialmente modificato la storia naturale della CAD, la possibilità di una simile terapia medica esiste anche per la prevenzione primaria. È importante che il rapporto costo/beneficio per popolazioni potenzialmente eleggibili venga valutato per ogni specifico trattamento. Se ciò non avvenisse potrebbe accadere che 200 soggetti senza storia di CAD debbano ingerire compresse (effetti tossici?) per un periodo di 5 anni, allo scopo di evitare la morte coronarica di uno di loro.
 per un periodo di 5 anni, allo scopo di evitare la morte coronarica di uno di loro.")
Presentazioni simili





















>")




 17 Ottobre 2009 DOPPIA ANTIAGGREGAZIONE PIASTRINICA.>")



