Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Casa di Cura San Lorenzino Cesena (FC) frankgaud@gmail.com
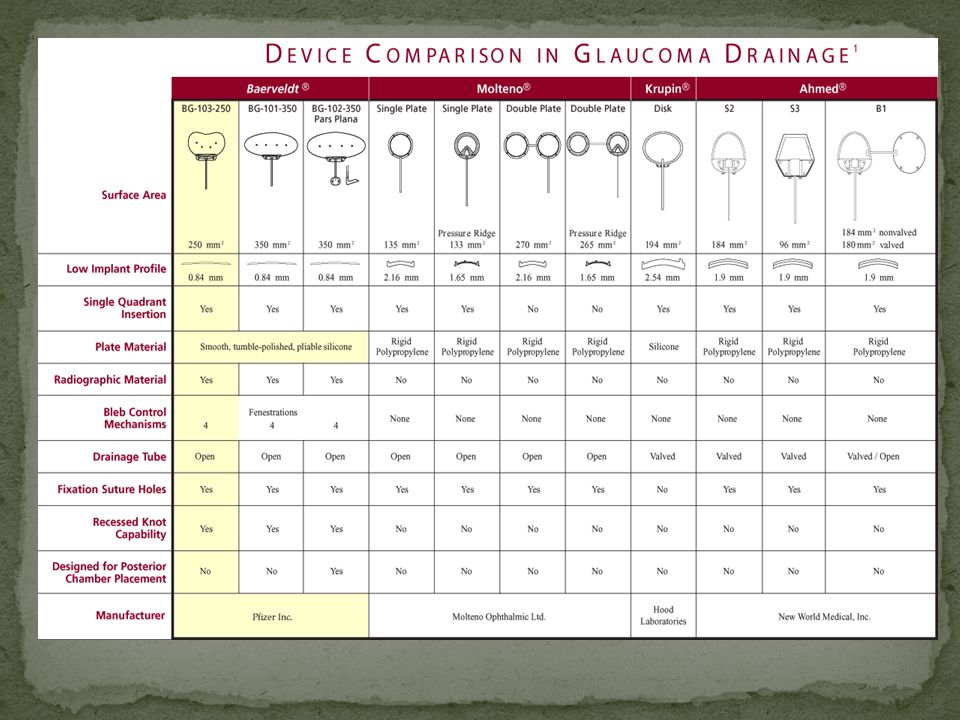
Le protesi del Glaucoma Baerveldt, Ahmed, Molteno3 Dott Francesco Gaudenzi Casa di Cura San Lorenzino Cesena (FC)
")
2
GLAUCOMA DEVICES: CENNI STORICI
Dispositivi per Paracentesi : dalla CA al sacco congiuntival Rollet e Moreau 1906: Crine di cavallo Mc Donald e Perce 1965: striscia di silicone Dispositivi Vitreali : dalla CV al sottotenone Vail 1915: Filo di seta Weekers 1922: cuffia d’oro Teuliere 1956: catgut

3
GLAUCOMA DEVICES CENNI STORICI
Impianti per Cyclodialisis Row 1934: Filo di platino e crine di cavallo Troncosco 1940: Striscia di Magnesio Troncosco 1949: Lamina di Tantalio Diversi autori: Supramid, polythene, film gelatina, polymethyl acetato, teflon Nesterov e Kolesnikova 1978: auto e alloscleral imp Strampelli : Ciclodiastasi con Supramyd Solx: Lamina d’oro

4
GLAUCOMA DEVICES CENNI STORICI
Dispositivi per il mantenimento della beanza translimbare : dalla CA allo spazio sottocongiuntivale 1912 Zorab 1912: Acqueoplasty (seta) Mayou 1912, Wood 1915, Stefansson 1925, Wolf e Blaess 1936, Blaess 1938, Wolf e Wolf 1940, Gibson 1944, Bick 1949, Troncosco 1949, Bock 1950, Parry 1952, Muldoon 1951, Qadeer 1954, Stone 1958, Lehman e Mc Caslin 1959, Epstein 1959, Ellis 1960, La Rocca 1962, Richards e Van Bijsterved 1965, Sampimon 1966): Tubi, Perni, Piastre nei più diversi materiali Oro, Seta, Tantalio, Vetro, Platino, Protoplast, Canali lacrimali autologhi, Polythene, Polyvinyl Ex-press 2001
 Mayou 1912, Wood 1915, Stefansson 1925, Wolf e Blaess 1936, Blaess 1938, Wolf e Wolf 1940, Gibson 1944, Bick 1949, Troncosco 1949, Bock 1950, Parry 1952, Muldoon 1951, Qadeer 1954, Stone 1958, Lehman e Mc Caslin 1959, Epstein 1959, Ellis 1960, La Rocca 1962, Richards e Van Bijsterved 1965, Sampimon 1966): Tubi, Perni, Piastre nei più diversi materiali Oro, Seta, Tantalio, Vetro, Platino, Protoplast, Canali lacrimali autologhi, Polythene, Polyvinyl. Ex-press")
5
GLAUCOMA DEVICES CENNI STORICI
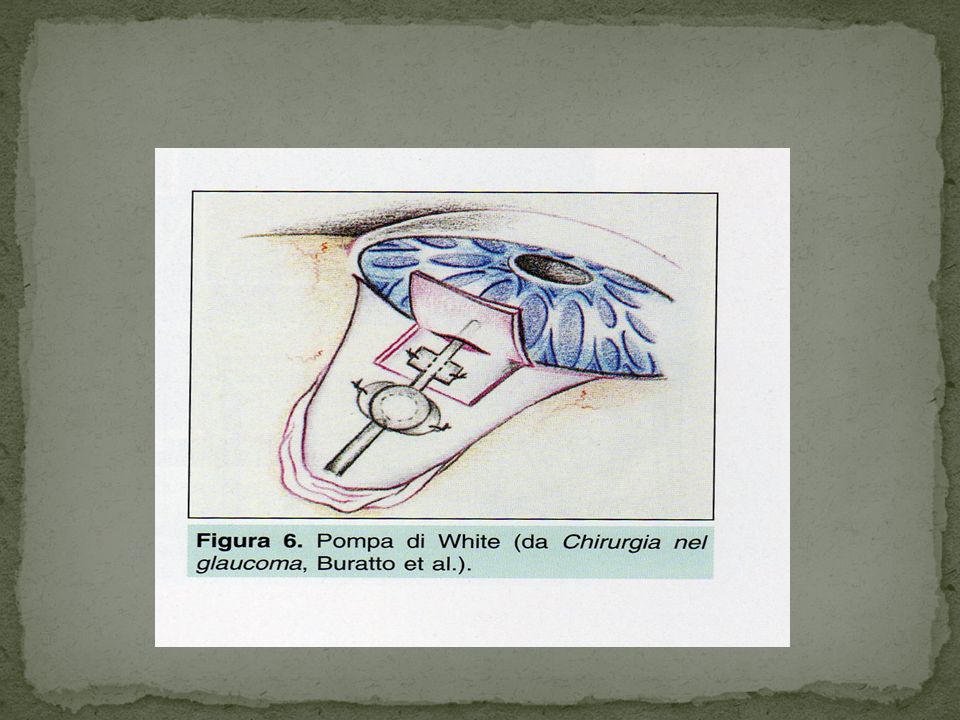
Dispositivi per favorire la formazione della bozza Roig 1954, Tripode d’argento sulla trapanazione sclerale Laval 1955, Gel sull’iridencleisis Tubi translimbari associati a dispositivi per favorire la formazione di una bozza Molteno Ahmed 1993? Krupin-Denver Baerveldt 1992? White 1986 Schocket 1992

6
Impianto di Schocket

7
Long tube Krupin-Denver Valve

12
Principio di Bernoulli:

15
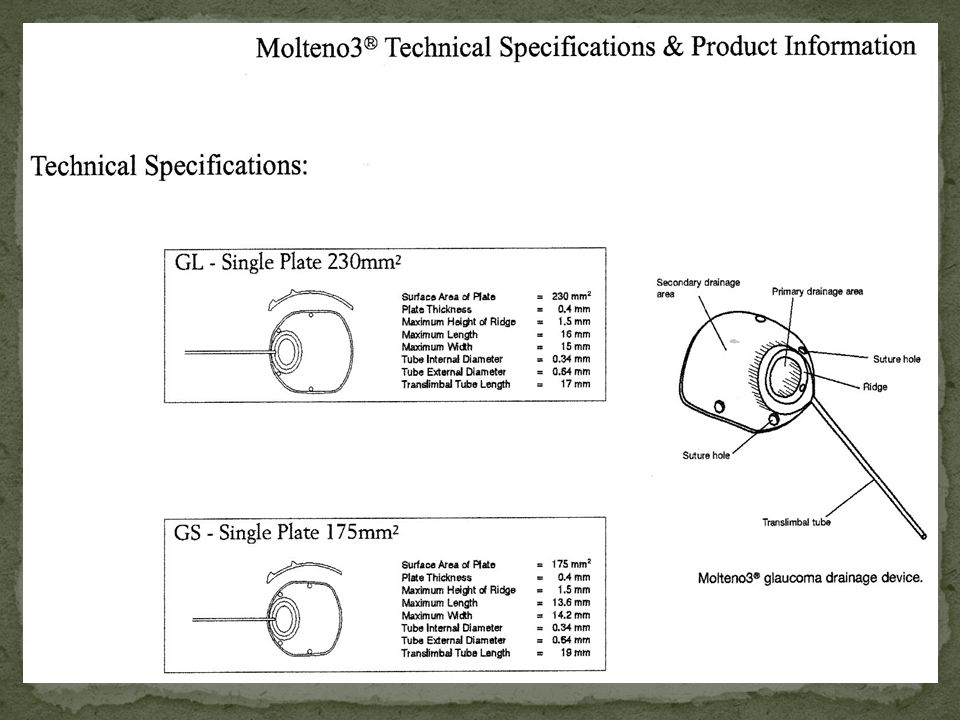
The Molteno3® Implant Plate surface divided into primary and secondary drainage areas primary drainage area secondary drainage area

16
Epstien’s Experiment 1957

17
Interpretation of Bleb Formation 1964
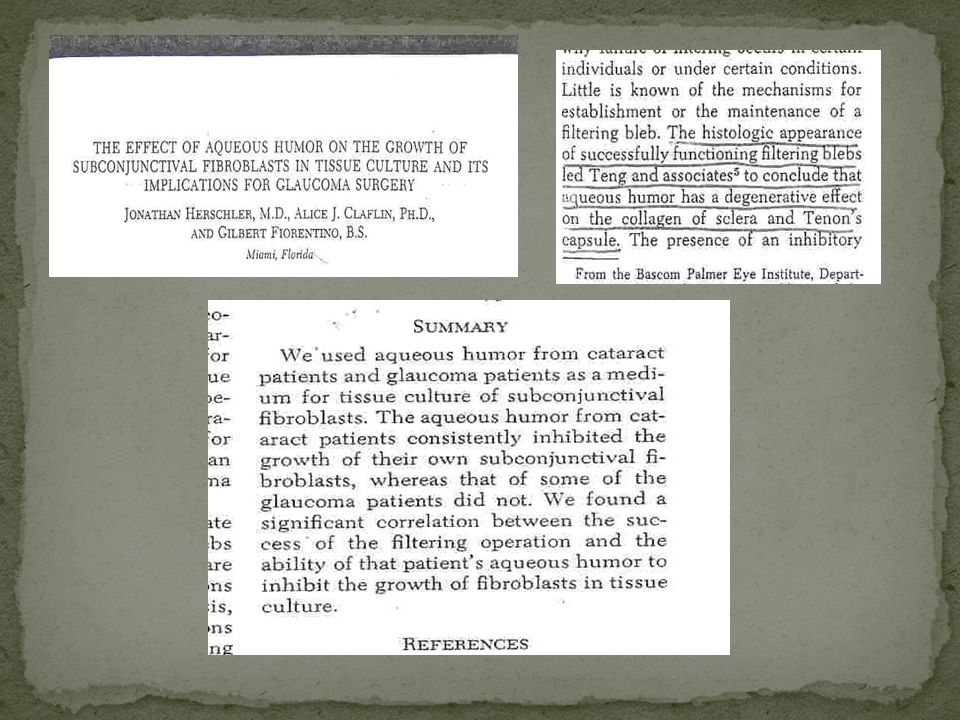
Epstein Aqueous stimulates fibroblasts to lay down collagen (absolute Glaucoma) Teng et al Aqueous causes degeneration of fibroblasts and collagen (successful drainage operations) Molteno Aqueous from hypertensive eyes stimulates fibroblasts to lay down collagen Aqueous from normotensive eyes causes degeneration of fibroblasts and collagen
 Teng et al. Aqueous causes degeneration of fibroblasts and collagen (successful drainage operations) Molteno. Aqueous from hypertensive eyes stimulates fibroblasts to lay down collagen. Aqueous from normotensive eyes causes degeneration of fibroblasts and collagen.")
19
Evolution of tissue defence mechanisms
Amoebae - phagocytosis, lysis Social amoebae - phagocytosis, autolysis Flatworms - apoptosis Chordates - apoptosis, feeble inflammation Man - inflammation, apoptosis

20
NZ flatworm Arthurdendyii australis
No circulatory system Apoptotic features Blebbing Swelling Lysis Tissue shrinks Animal shrinks (hypoxia, starvation) 5 mm
 5 mm.")
21
Cytology of Apoptosis Apoptosis 1600 X H&E Stressed Flatworm
Human bleb capsule

22
GLAUCOMA:FIBROSI DELLA BOZZA
Per capire quello che succede in una bozza è necessario riconsiderare il meccanismo alla base di qualunque processo di riparazione nel ns organismo: L’INFIAMMAZIONE Essa è il risultato di 2 fenomeni: 1) La formazione dell’essudato 2) La cellularità
 La formazione dell’essudato. 2) La cellularità.")
23
DAL FAVILLI PATOLOGIA GENERALE
“Il processo infiammatorio ha inizio con alterazioni vascolari a livello della microcircolazione alle quali conseguono fuoriuscita di componenti del plasma (formazione dell’essudato) e migrazione di cellule ematiche negli interstizi dei tessuti. (formazione della cellularità)” “Successivamente prevalgono i fenomeni regressivi degli elementi parenchimali fino alla necrosi delle cellule nei casi più gravi per anossia.” (rimodellamento tissutale)
 e migrazione di cellule ematiche negli interstizi dei tessuti. (formazione della cellularità) Successivamente prevalgono i fenomeni regressivi degli elementi parenchimali fino alla necrosi delle cellule nei casi più gravi per anossia. (rimodellamento tissutale)")
24
MECCANISMO DELL’INFIAMMAZIONE
ANGIOFLOGOSI (acuta) ISTOFLOGOSI (cronica)
 ISTOFLOGOSI (cronica)")
25
IPEREMIA ATTIVA: RUBOR
AUMENTO DELLA VELOCITA’: CALOR ESSUDAZIONE DAL VASO CAPILLARE AL TESSUTO INTERSTIZIALE: TUMOR

26
GLAUCOMA : LA FIBROSI DELLA BOZZA
Dobbiamo a questo punto ricordare 1) 50 mmHg della pressione idrostatica nell’arteriola precapillare normale 2) 32 mmHg della pressione idrostatica nel capillare arterioso normale 3) 12 mmHg della pressione idrostatica nel capillare venoso normale 4) 22 mmHg della pressione colloidosmotica sanguigna(costante) Ciò permette che la filtrazione avvenga verso i tessuti dove la pressione idrostatica supera la colloidosmotica (distretto arterioso) e verso il torrente capillare dove avviene l’inverso (distretto venoso) con un gradiente che cambia in continuo da positivo a neutro e quindi negativo man mano che si procede dall’uno all’altro.
 50 mmHg della pressione idrostatica nell’arteriola precapillare normale. 2) 32 mmHg della pressione idrostatica nel capillare arterioso normale. 3) 12 mmHg della pressione idrostatica nel capillare venoso normale. 4) 22 mmHg della pressione colloidosmotica sanguigna(costante) Ciò permette che la filtrazione avvenga verso i tessuti dove la pressione idrostatica supera la colloidosmotica (distretto arterioso) e verso il torrente capillare dove avviene l’inverso (distretto venoso) con un gradiente che cambia in continuo da positivo a neutro e quindi negativo man mano che si procede dall’uno all’altro.")
27
GLAUCOMA: LA FIBROSI DELLA BOZZA
Nella Flogosi, al momento che si rilascia lo sfintere precapillare, la pressione idrostatica si distribuisce senza più alcun effetto diga a tutto il distretto capillare. Ecco che i valori diventano i seguenti: 1) mmHg nel distretto capillare arterioso 2) 23 mmHg nel distretto capillare venoso (Landis 1930) 3) La pressione colloidosmotica non è sufficiente a creare nessun flusso negativo (verso il capillare venoso) 4) Il capillare è un vaso che possiede solo rivestimento endoteliale senza tunica muscolare o elastica di alcun tipo, si danneggia e si fenestra per cui la pressione totale nel tessuto interstiziale sale tanto più quanto più è violenta la risposta infiammatoria e il risultato è l’edema (tumor)
 mmHg nel distretto capillare arterioso. 2) 23 mmHg nel distretto capillare venoso (Landis 1930) 3) La pressione colloidosmotica non è sufficiente a creare nessun flusso negativo (verso il capillare venoso) 4) Il capillare è un vaso che possiede solo rivestimento endoteliale senza tunica muscolare o elastica di alcun tipo, si danneggia e si fenestra per cui la pressione totale nel tessuto interstiziale sale tanto più quanto più è violenta la risposta infiammatoria e il risultato è l’edema (tumor)")
28
Human tissue responses to environmental stressors e
Human tissue responses to environmental stressors e.g hypoxia, low protein Evolved Fibrosis Rapid onset Activation and migration of cells Inflammation Synthesis of collagen barrier Damaged part isolated Primitive Apoptosis Slower onset Autodigestion of cells Mucous barrier Tissue shrinks

29
Molteno3® action Aqueous restricted to primary area for 2+ weeks
Minimises early hypotony Forms local fibrous layer, IOP rises Starts apoptosis, releases Fas-ligand Aqueous escape to main bleb from +2 weeks Carries Fas-ligand, “kick-starts” apoptosis in main bleb Decreases fibrotic and increases apoptic tissue responses Thinner, more permeable main bleb, lower IOP

30
4 weeks after surgery primary drainage area Vicryl® tie

31
Bleb at 1 year secondary bleb primary bleb bleb extending beyond plate
Cyst of Moll

32
Bleb capsule at 8 weeks completed op secondary bleb primary bleb
thicker layer, more fibrosis, less apoptosis thinner layer, less fibrosis more apoptosis primary drainage secondary drainage completed op secondary bleb 2° primary bleb 1°

33
Bleb capsule development
Vascular fibroproliferative response IOP low after surgery vasodilation Fibrous layer is formed IOP rises above episcleral venous pressure Venules collapse, O2 and protein levels fall Apoptotic fibrodegenerative response Apoptotic death messengers in aqueous Blocks fibroproliferative response Breakdown of fibrous layer IOP falls Long-term equilibrium 0-3 wks 2-6 wks

34
Fibroproliferative response Cells <50 µ from capillary, O2 & protein high while IOP < episcleral venous pressure, capillaries patent capillary cell migration Activation Multiplication Cell migration upstream Collagen synthesis Collagen barrier formed IOP rises Aqueous flows bottom to top collagen barrier capsule, 11 days

35
Fibrodegenerative response Cells >50 µ from capillary,O2 & protein low initiated when IOP > episcleral venous pressure, capillaries collapsed Activation Cell migration upstream Apoptosis Death messenger drift downstream Collagen breakdown IOP falls Aqueous flows bottom to top death messenger drift collagen breakdown capsule, 56 days

36
Equilibrium from 6 weeks
TENON’S TISSUE Aqueous flows at ≈ 6-12 µ/minute Cells migrate at ≈ 6 µ/hour Vasodilation Diapedesis Activation Collagen synthesis Apoptosis Vasoconstriction Inhibits diapedesis Inactivation Collagen digestion Fas ligand, enzymes BLEB CAVITY

37
Apoptosis and lysis - 56 days
400 X Gomori trichrome 13 X Gomori trichrome Renga bleb 56 day old bleb, tangential section

38
Apoptosis and lysis - 10 years
100 X H&E polarised light 1000 X H&E Cato bleb 10 year old bleb, tangential section

39
Equilibrium maintained - 21 years
1000 X apoptosis and collagenolysis 100 X H&E phase contrast 21 year old bleb, less cellular

40
40

41
FIGURE 2. Graph showing the mean preoperative and postoperative intraocular pressures in the Ahmed valve and Molteno implant groups. *P < 0.001, **P _ 0.001, ***P < 0.01, Mann–Whitney U test comparisons of the figures at the different time points between 2 groups. Nassiri N et al ,Am J Ophthalmol 2010:149,

42
Efficacy of the Ahmed S2 Glaucoma Valve Compared with the Baerveldt 250-mm2 Glaucoma Implant
Robert J. Goulet III, MD, Anh-Danh T. Phan, MD, Louis B. Cantor, MD, Darrell WuDunn, MD, PhD Conclusions: Our study suggests that the Ahmed S2 Glaucoma Valve may be less effective at lowering IOP than the Baerveldt 250-mm2 Glaucoma Implant. Ophthalmology 2008; 115:1141–1147 © 2008 by the American Academy of Ophthalmology.

44
Three-Year Follow-up of the Tube vsTrabeculectomy Study STEVEN J
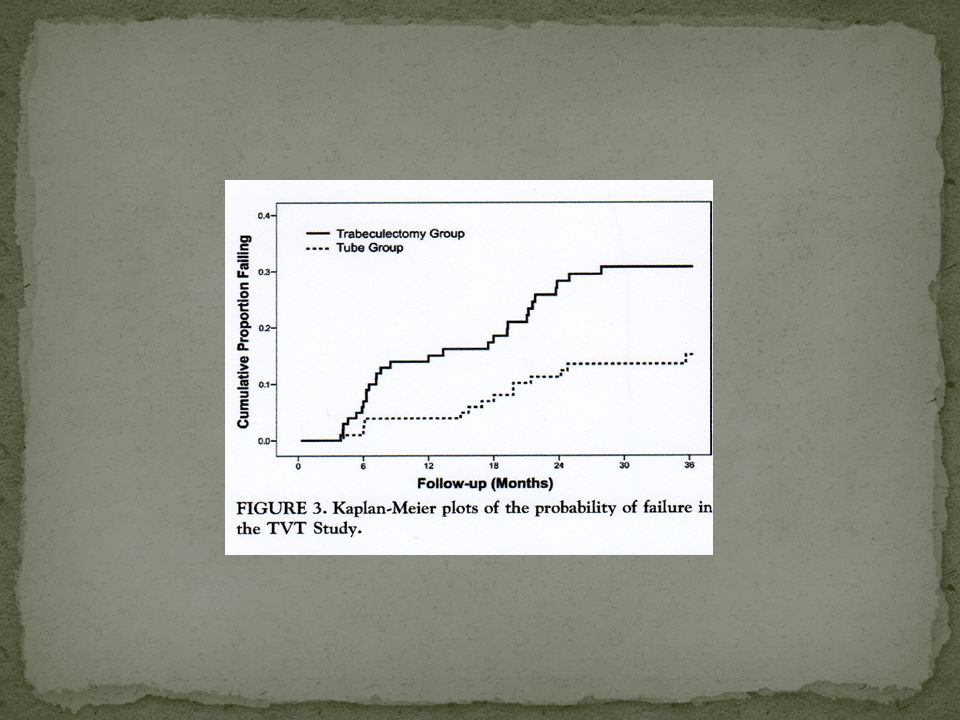
Three-Year Follow-up of the Tube vsTrabeculectomy Study STEVEN J. GEDDE, JOYCE C. SCHIFFMAN, WILLIAM J. FEUER, LEON W. HERNDON, JAMES D. BRANDT, AND DONALD L. BUDENZ, ON BEHALF OF THE TUBE VERSUS TRABECULECTOMY STUDY GROUP RESULTS: A total of 212 eyes of 212 patients were enrolled, including 107 in the tube group and 105 in the trabeculectomy group. At 3 years, IOP (mean standard deviation [SD]) was /- 4.9 mm Hg in the tube group and /- 6.8 mm Hg in the trabeculectomy group (P.78).
 was /- 4.9 mm Hg in the tube group and /- 6.8 mm Hg in the trabeculectomy group (P.78).")
45
The cumulative probability of failure during the first 3 years of follow-up was 15.1% in the tube group and 30.7% in the trabeculectomy group (P ; Tube shunt surgery had a higher success rate compared to trabeculectomy withMMCduring the first 3 years of follow-up in the TVT Study. Both procedures were associated with similar IOP reduction and use of supplemental medical therapy at 3 years. While the incidence of postoperative complications was higher following trabeculectomy with MMC relative to tube shunt surgery, most complications were transient and self-limited. (Am JOphthalmol 2009;148:670–684. © 2009

49
Table of Conversion Suture Diameter in mm U.S.P designation
Metric diameter in mm 11-0 0,01 10-0 0,02 9-0 0,03 8-0 0,05 7-0 0,07 6-0 0,1 5-0 0,15 4-0 0,2 3-0 0,3 2-0 0,35 0,4 1 0,5 2 0,6 3 0,7 4 0,8 Table of Conversion Suture Diameter in mm

50
AWG N° Diam mm Area mm2 Area mm2 1 7,350 42,400 16 1,290 1,3100 2 6,540 33,600 17 1,150 1,0400 3 5,190 21,200 18 1,024 0,8230 4 19 0,912 0,6530 5 4,620 16,800 20 0,812 0,5190 6 4,110 13,300 21 0,723 0,4120 7 3,670 10,600 22 0,644 0,3250 8 3,26 8,350 23 0,573 0,2590 9 2,910 6,620 24 0,511 0,2050 10 2,590 5,270 25 0,455 0,1630 11 2,300 4,150 26 0,405 0,1280 12 2,050 3,310 27 0,361 0,1020 13 1,830 2,630 28 0,321 0,0804 14 1,630 2,080 29 0,286 0,0646 15 1,450 1,650 30 0,255 0,0503

Presentazioni simili













 Brussels, 26 settembre 2013.>")





>")

 A.Cristofoli (laureando.>")

>")


 17 Ottobre 2009 DOPPIA ANTIAGGREGAZIONE PIASTRINICA.>")





