Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Richard Horton , Lancet 2005

2
Malattia Cronica : tempo…..
“An illness marked by long duration or frequent recurrence” “A disease lasting indefinitely. “ “A disease that persists for a long time. A chronic disease is one lasting 3 months or more, by the definition of the U.S. National Center for Health Statistics. Malattia Cronica : tempo….. “A disease that can be controlled but not cured” “A disease with one or more of the following characteristics: permanence, leaves residual disability, caused by non-reversible pathological alternation, requires special training of the patient for rehabilitation, or may require a long period of supervision, observation, or care” Malattia Cronica : prognosi…. “Chronic diseases generally cannot be prevented by vaccines or cured by medication, nor do they just disappear

3
Cause delle malattie croniche
Determinanti socioeconomici culturali ,politici, ambientali Globalizzazione Urbanizzazione Invecchiamento della popolazione Fattori di rischio intermedi Ipertensione Ipotolleranza glucidica Obesità Dislipidemia MALATTIA CRONICA Fattori di rischio comuni , modificabili Dieta incongrua Sedentarietà Uso di tabacco non modificabili Età Ereditarietà Mal CV Diabete BPCO Neoplasia

4
World Health Organization, 2005.
Preventing chronic diseases: a vital investment — WHO global report. Geneva: World Health Organization, 2005.

5
World Health Organization, 2005.
Preventing chronic diseases: a vital investment — WHO global report. Geneva: World Health Organization, 2005.

6
35 000 000 Chronic diseases Did you know??
Cardiovascular disease, mainly heart disease, stroke Cancer Chronic respiratory diseases Diabetes Did you know?? Chronic diseases Strong et al, Lancet 2005

7
Millions of Cases of Diabetes in 2000 and Projections for 2030, with Projected Percent Changes.
Data are from Wild S et al. : Diabetes Care 2004;27:1047

8
Diabetes confers an equivalent
Booth GL Lancet 2006; 368: 29–36 Relation between age and rates of AMI or death from any cause in men and women according to presence of diabetes and previous AMI Recent AMI: polynomial distribution. No recent AMI: exponential istribution.R2 >0,97 for each dotted line. Recent AMI=within 3 years of baseline. Diabetes confers an equivalent risk to ageing 15 years

9
Prevalence of Diabetes*
* Self-reported history of diagnosed diabetes S2 vs. S1 : P=0.21 S3 vs. S2 : P=0.02 S3 vs. S1 : P=0.001 Euro Heart Survey Programme ESC Quality Assurance Programme to Improve Cardiac Care in Europe

10
Risks are increasing

11
Prevalence of Obesity*
S2 vs. S1 : P=0.009 S3 vs. S2 : P=0.051 S3 vs. S1 : P=0.0002 * Body mass index ≥ 30 kg/m² Euro Heart Survey Programme ESC Quality Assurance Programme to Improve Cardiac Care in Europe

12
Prevalence of Central Obesity*
S2 vs. S1 : P=0.0001 S3 vs. S2 : P=0.47 S3 vs. S1 : P<0.0001 * Waist circumference ≥ 102 cm in men or ≥ 88 cm in women Euro Heart Survey Programme ESC Quality Assurance Programme to Improve Cardiac Care in Europe

14
Estimated prevalence of GOLD stage 2 or higher COPD
Mannino DM :Lancet 2007; 370: 765–73

15
The ARIC Study:Mannino DM:Respir Med 2006; 100: 115

16
Classificazione “spirometrica” di gravità della BPCO (GOLD 2005)
STADIO CARATTERISTICHE 0: A RISCHIO Spirometria normale, sintomi cronici I: LIEVE VEMS/CVF < 70%; VEMS ≥ 80% del teorico con o senza sintomi cronici II: MODERATA 50% ≤ VEMS < 80% del teorico con o senza sintomi cronici III: GRAVE 30%VEMS< 50% pred. con o senza sintomi IV: MOLTO GRAVE VEMS < 30% pred. o VEMS<50%pred. con insufficienza respiratoria cronica

17
Cosa e’una riacutizzazione di BPCO dal punto di vista clinico?
Funzione tempo Normali oscillazioni stato clinico Riacutizzazioni ? CHEST 2000; 117:398S Segni e sintomi Peggioramento acuto, inatteso, sostenuto… temperatura frequenza cardiaca stato mentale Sistemici dispnea (respiro corto, rapido) tosse espettorato purulento Respiratori
 tosse. espettorato purulento. Respiratori.")
18
un’ epidemia incombente
prevalenza di ipertensione arteriosa nel mondo: un’ epidemia incombente 1 miliardo di ipertesi USA & Canada Europa Cina 28%, 50 milioni 27%, 130 milioni 38-55%, milioni Wolf-Maier K et al. Hypertension JNC Dongfeng G et al Hypertension 2002

19
Pressione e mortalità ictus Ischemia cardiaca sistolica diastolica

21
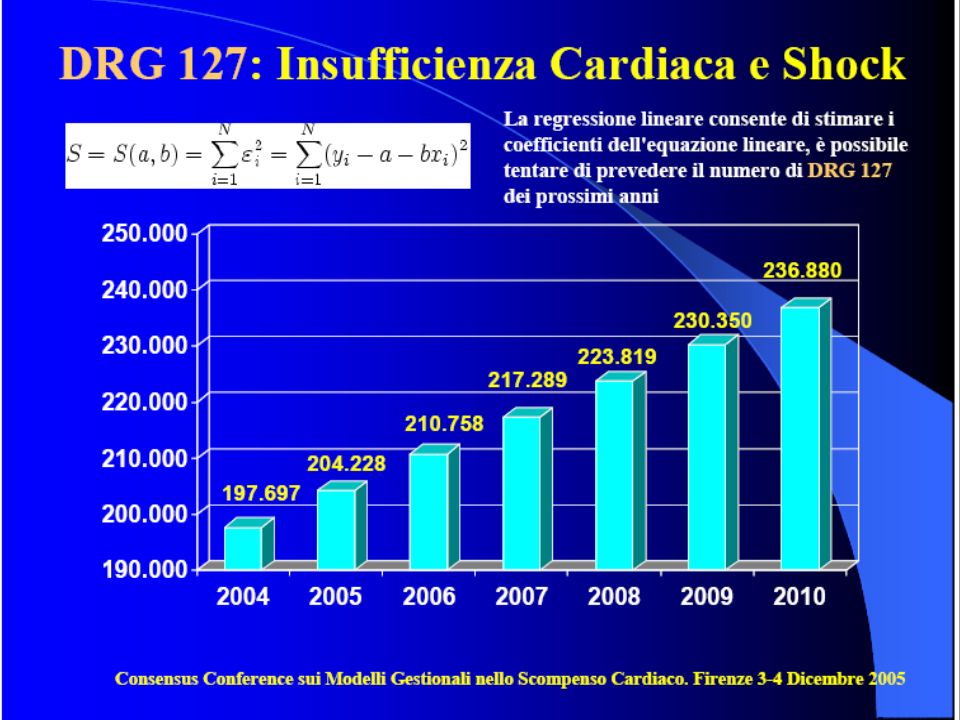
Scompenso Cardiaco N. Ricoveri 2001 2002 2003
Attraverso questi criteri è stata definita per lo SC nell’area di analisi la prevalenza (numero di pazienti M/F con SC/totale popolazione) e il tasso di letalità (numero di deceduti M/F nel 2004/totale pazienti con SC). Sono stati individuati con questi criteri nelle Regioni e ASL partecipanti pazienti affetti da SC, per una prevalenza pari a 1.19% Il tasso di letalità globale è del 15.4%. L’analisi è stata quindi segmentata per classi di età (Fig.4): la prevalenza, analogamente a quanto dimostrato negli studi epidemiologici di popolazione, è maggiore nel sesso maschile e cresce, come la letalità in maniera esponenziale con l’età. 7
 e il tasso di letalità (numero di. deceduti M/F nel 2004/totale pazienti con SC). Sono stati individuati con questi. criteri nelle Regioni e ASL partecipanti pazienti affetti da SC, per una. prevalenza pari a 1.19% Il tasso di letalità globale è del 15.4%. L’analisi è stata quindi segmentata per classi di età (Fig.4): la prevalenza, analogamente a quanto dimostrato negli studi epidemiologici di popolazione, è. maggiore nel sesso maschile e cresce, come la letalità in maniera esponenziale con. l’età. 7.")
22
Epidemiologia in EUROPA: prevalenza
Prevalenza ICC sintomatica: 0,4-2% Aumenta con l’età (età media 74 aa) È IN AUMENTO Anche la mortalità (età agg.) è in aumento 900 Milioni di europei 10 Milioni ICC Altrettanti con ICC asintomatica
 È IN AUMENTO. Anche la mortalità (età agg.) è in aumento. 900 Milioni di europei 10 Milioni ICC. Altrettanti con ICC asintomatica.")
23
The REACH Study (30.000 pts, 52% donne)
Mc Cullough PA JACC 2002;39:60

24
IV=(P≥65/P≤14)*100 242.0
*")
25
(da Pulignano G, 2005)
")
26
Sempre più su……….

27
MDGs: chronic diseases are not on the agenda Fuster V : Lancet 2005;366:1513
Projected deaths by major cause and World Bank income group, all ages, 2005

28
Number of Cardiovascular Deaths Projected to 2020
Millions

29
Si può fare qualcosa?

30
Terapia intensiva su tutti i
160 DIABETICI TIPO 2 FOLLOW UP 7.8 ANNI ETA’ MEDIA 55 A. TUTTI MICROALBUMINURICI Terapia intensiva su tutti i fattori di rischio - 20% Morte + eventi cardiovascolari Gaede P. NEJM 2003;348:383

31
Riduzione % del rischio relativo
Benefici della terapia antipertensiva dimostrati nei trials con PA clinica (riduzione di circa 10 sist./5 dia. mmHg) –35-40% -20-25% -50% Riduzione % del rischio relativo rallentamento progressione IR
 –35-40% % -50% Riduzione % del rischio relativo. rallentamento progressione IR.")
32
RR= 0.64 RR=0.64

33
12 studi , 8307 pazienti BMJ published online 11 Oct 2007; ABSTRACT
Objective To review the evidence base from randomised controlled trials of combined cardiac resynchronisation therapy and implantable cardioverter defibrillator therapy in left ventricular impairment and symptomatic heart failure. Design Bayesian network meta-analysis. Data sources Medline, Embase, and Cochrane databases up to June 2006. Review methods Two reviewers independently assessed trial eligibility and quality. Included trials compared cardiac resynchronisation therapy, implantable cardioverter defibrillator therapy, combined resynchronisation and implantable defibrillator therapy, and medical therapy alone, in patients with impaired left ventricular systolic function. Bayesian random effects network models were used to examine overall number of deaths. Results 12 studies including 1636 events in 8307 patients were identified. Combined cardiac resynchronisation and implantable cardioverter defibrillator therapy reduced the number of deaths by one third compared with medical therapy alone (odds ratio 0.57, 95% credible interval 0.40 to 0.80) but did not further improve survival when compared with implantable defibrillator therapy (0.82, 0.57 to 1.18) or resynchronisation (0.85, 0.60 to 1.22) therapy alone. Conclusion Evidence from randomised controlled trials is insufficient to show the superiority of combined cardiac defibrillator therapy over cardiac resynchronisation therapy alone in patients with left ventricular impairment. 12 studi , 8307 pazienti
 but did not. further improve survival when compared with implantable. defibrillator therapy (0.82, 0.57 to 1.18) or. resynchronisation (0.85, 0.60 to 1.22) therapy alone. Conclusion Evidence from randomised controlled trials is. insufficient to show the superiority of combined cardiac. defibrillator therapy over cardiac resynchronisation. therapy alone in patients with left ventricular impairment. 12 studi , 8307 pazienti.")
34
Home Based Intervention
297 pts per 4.2 anni età media 75 anni 50% ischemici 30% diabetici Home Based Intervention + 28% Home-Based Intervention in Congestive Heart Failure Long-Term Implications on Readmission and Survival Simon Stewart, PhD, FESC; John D. Horowitz, PhD, FRACP Background—It is not known to what extent initially observed benefits of postdischarge programs of care for patients with chronic congestive heart failure (CHF) in respect to event-free survival, readmissions, and healthcare costs persist in the long term. Methods and Results—We prospectively studied the long-term effects of a multidisciplinary home-based intervention (HBI) in a cohort of CHF patients randomly allocated to either to HBI (n149) or usual care (n148). During a median of 4.2 years of follow-up, there were significantly fewer primary end points (unplanned readmission or death) in the HBI versus usual care group: a mean of 0.21 versus 0.37 primary events per patient per month (P0.01). Median event-free survival was more prolonged in the HBI than usual care group (7 versus 3 months; P0.01). Fewer HBI patients died (56% versus 65%; P0.06) and had more prolonged survival (a median of 40 versus 22 months; P0.05) compared with usual care. Assignment to HBI was both an independent predictor of event-free survival (RR 0.70; P0.01) and survival alone (RR 0.72; P0.05). Overall, HBI patients had 78 fewer unplanned readmissions compared with usual care (0.17 versus 0.29 readmissions per patient per month; P0.05). The median cost of these readmissions was $A325 versus $A660/month per HBI and usual care patient (P0.01). Conclusions—The beneficial effects of HBI in reducing frequency of unplanned readmissions in CHF patients persist in the long term and are associated with prolongation of survival. (Circulation. 2002;105: ) Stewart S Circulation 2002;105:2861
 in respect to event-free survival, readmissions, and healthcare costs persist in the. long term. Methods and Results—We prospectively studied the long-term effects of a multidisciplinary home-based intervention. (HBI) in a cohort of CHF patients randomly allocated to either to HBI (n149) or usual care (n148). During a median. of 4.2 years of follow-up, there were significantly fewer primary end points (unplanned readmission or death) in the HBI. versus usual care group: a mean of 0.21 versus 0.37 primary events per patient per month (P0.01). Median event-free. survival was more prolonged in the HBI than usual care group (7 versus 3 months; P0.01). Fewer HBI patients died. (56% versus 65%; P0.06) and had more prolonged survival (a median of 40 versus 22 months; P0.05) compared. with usual care. Assignment to HBI was both an independent predictor of event-free survival (RR 0.70; P0.01) and. survival alone (RR 0.72; P0.05). Overall, HBI patients had 78 fewer unplanned readmissions compared with usual. care (0.17 versus 0.29 readmissions per patient per month; P0.05). The median cost of these readmissions was $A325. versus $A660/month per HBI and usual care patient (P0.01). Conclusions—The beneficial effects of HBI in reducing frequency of unplanned readmissions in CHF patients persist in. the long term and are associated with prolongation of survival. (Circulation. 2002;105: ) Stewart S Circulation 2002;105:2861.")
35
Stewart S et al.: Lancet 354,1077,1999 200 pts con CHF ,classi NYHA II-IV ,età media 75 a., comorbidità (BPCO 33%, diabete 34%) INTERVENTO : unica visita di infermiera 7-14 g da dimissio- ne(comprehensive home assessment) contatti telefonici , rapporti col curante DURATA : mesi intervento + 6 mesi follow up RISULTATI: Intervento Controllo End points primari (-40%) (ricoveri +decessi) Ricoveri urgenti 68 (118) (156) Giorni di ricovero Costi totali $ $ Costo/paziente $ $ 2.200 Costo dell’intervento : $ 350/paziente Il beneficio si prolungò altri 6 mesi oltre l’intervento.
 contatti telefonici , rapporti col curante. DURATA : 6 mesi intervento + 6 mesi follow up. RISULTATI: Intervento Controllo. End points primari 77 (-40%) 129. (ricoveri +decessi) Ricoveri urgenti 68 (118) 118 (156) Giorni di ricovero Costi totali $ $ Costo/paziente $ 900 $ Costo dell’intervento : $ 350/paziente. Il beneficio si prolungò altri 6 mesi oltre l’intervento.")
36
Authors’ conclusions Exercise training improves exercise capacity and quality of life in patients mild to moderate heart failure in the short term. One study found beneficial effects of exercise on cardiac mortality and hospital readmissions over 3 years of follow-up, the remaining included studies did not aim to measure clinical outcomes and were of short duration. The findings of the review are based on small-scale trials in patients who are unrepresentative of the total population of patients with heart failure. Other groups (more severe patients, the elderly,women) may also benefit. Large-scale pragmatic trials of exercise training of longer duration, recruiting a wider spectrum of patients are needed to address these issues. The Cochrane Library 2007, Isssue 4
 may also benefit. Large-scale pragmatic trials of exercise training of longer duration, recruiting a wider spectrum of patients are needed to address these issues. The Cochrane Library 2007, Isssue 4.")
37
The Cochrane Library 2007, Isssue 4

38
BMJ 2006;332:1379

39
A U T H O R S ’ C O N C L U S I O N S “The results of this meta-analysis strongly support respiratory rehabilitation including at least four weeks of exercise training as part of the spectrum of management for patients with COPD. We found clinically and statistically significant improvements in important domains of quality of life, including dyspnea, fatigue emotional function. When compared with the treatment effect of other important modalities of care…rehabilitation resulted in greater improvements in important domains of health-related quality of life and functional exercise capacity.”

40
Conclusion Early pulmonary rehabilitation after admission to hospital for acute exacerbations of COPD is safe and leads to statistically and clinically significant improvements in exercise capacity and health status at three months. BMJ 2004;329:1209–11

41
BMJ 2004;329:1209–11 Pulmonary rehabilitation
A multidisciplinary team ran the pulmonary rehabilitation programme, which consisted of two classes per week for eight weeks. Each class lasted two hours, consisting of one hour of exercise (aerobic walking and cycling, strength training for the upper and lower limb) and one hour of educational activities (with an emphasis on self management of the disease, nutrition, and lifestyle issues). Respiratory physiotherapists and nurses supervised the exercise component, as did health centre based fitness instructors. Physiotherapists, respiratory nurses, an occupational therapist, a dietician, a respiratory doctor, a smoking cessation adviser, a social worker, a pharmacist, and a lay member of a patients’ group supervised education activities on a rolling rota. Patients also received individualised home exercise programmes, which encouraged at least 20 minutes of exercise per day. BMJ 2004;329:1209–11
 and one hour of educational activities (with an emphasis on self management of the disease, nutrition, and lifestyle issues). Respiratory physiotherapists and nurses supervised the exercise component, as did health centre based fitness instructors. Physiotherapists, respiratory nurses, an occupational therapist, a dietician, a respiratory doctor, a smoking cessation adviser, a social worker, a pharmacist, and a lay member of a patients’ group supervised education activities on a rolling rota. Patients also received individualised home exercise programmes, which encouraged at least 20 minutes of exercise per day. BMJ 2004;329:1209–11.")
42
BMJ 2004;329:1209–11

43
BMJ 2004;329:1209–11

44
“ Ma è davvero così semplice?”

45
Compliance significa: Accettazione, osservanza delle prescrizioni mediche da parte del paziente il quale ha solo il dovere di seguire quanto prescritto

46
Adherence L’OMS ha promosso il termine Adherence per utilizzarlo nelle patologie croniche come “il grado di comportamento di una persona che assume farmaci, che segue una dieta e/o stile di vita e risponde alle esigenze delle raccomandazioni condivise da parte delle agenzie di salute” (Report on Medication Adherence Geneva –World Health Org. 2003)
")
47
Compliance Adherence

48
La terapia nella malattia cronica
Nella cronicità il paziente deve assumere e condividere la responsabilità della terapia e della sua salute La formazione del paziente ad un’autogestione consapevole della malattia diventa parte integrante della terapia

49
Adesione e malattie croniche
Nonostante la ricerca clinica abbia raggiunto risultati rilevanti per il trattamento e per il controllo delle patologie croniche, più del 50% dei pazienti cronici non riesce ad eseguire correttamente la terapia consigliata

53
the best available evidence,
Che fa il buon dottore? Good doctors use both individual clinical expertise and the best available evidence, neither is enough Sackett DL et al, BMJ 1996; 312: 71-2

54
E’ necessario l’intervento del paziente

56
Dying slowly, painfully and prematurely

57
Causes of chronic diseases

58
The economic impact: billions

59
Si può fare qualcosa su base mondiale?

60
Horton, The Lancet 2005

61
The global goal A 2% annual reduction in chronic disease death rates worldwide, per year, over the next 10 years. The scientific knowledge to achieve this goal already exists.

63
Epping-Jordan et al, Lancet 2005

64
Number of interventions
Combined effects of 3 interventions that each reduce relative risk by 25% (20%) Three successive 25% RR reductions Three successive 20% RR reductions Number of interventions
 Three successive 25% RR reductions. Three successive 20% RR reductions. Number of interventions.")
65
9 out of 10 lives saved: low and middle income countries

66
Economic gain: billions

67
Potential for Europe If there are 40 million individuals with a 10 year CV risk of 25% In the absence of treatment every year there will be 1 million strokes and HA About half these could be averted (10 year CV risk 11.25%)
")
68
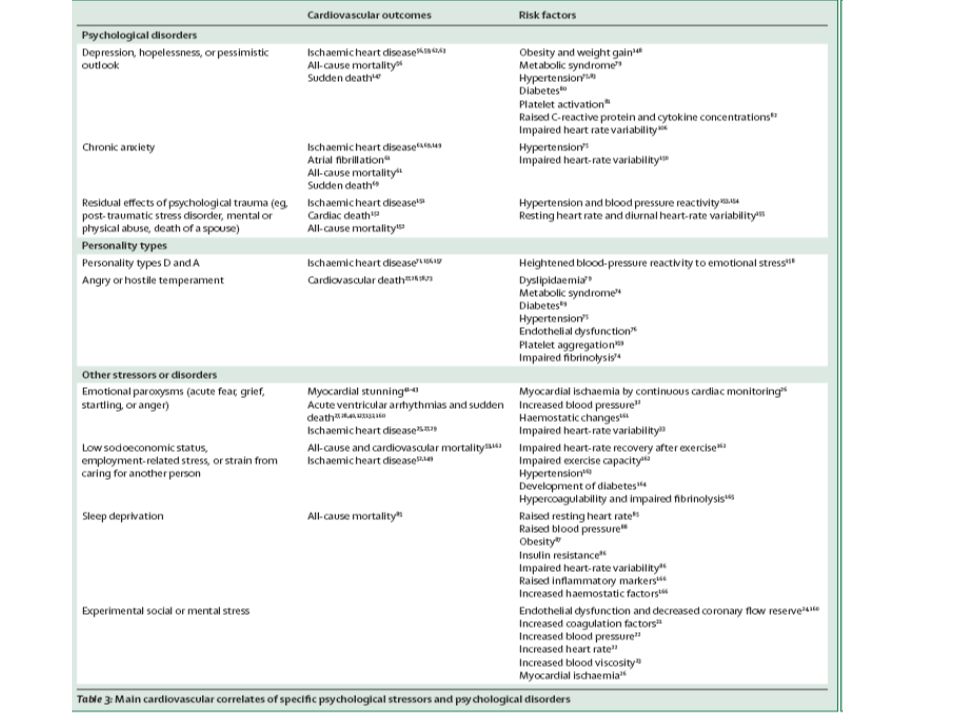
The cardiovascular toll of stress
Daniel J Brotman, Sherita H Golden, Ilan S Wittstein Lancet 2007; 370: 1089–100 Psychological stress elicits measurable changes in sympathetic-parasympathetic balance and the tone of the hypothalamic-pituitary-adrenal axis, which might negatively aff ect the cardiovascular system both acutely—by precipitating myocardial infarction, left-ventricular dysfunction, or dysrhythmia; and chronically—by accelerating the atherosclerotic process. We provide an overview of the association between stress and cardiovascular morbidity, discuss the mechanisms for this association, and address possible therapeutic implications.

70
The cardiovascular toll of stress
Brotman DJ Lancet 2007;370:1089

71
Estimated decrease in blood pressure mediated by non-pharmacological intervention in hypertension
Messerli, Williams, Ritz. Lancet 2007; 370: 591

72
Blood pressure control
Potential therapeutic strategies to prevent the develoment and/or progression of cardiovascular disease Blood pressure control Glycemic control Weight loss Lipid lowering Combination treatment in a unique “polypill”?

73
Specifically, we recommend further evaluation
Combination Pharmacotherapy and Public Health Research Working Group Report (CDC & US Experts) Developing countries may manufacture and distribute variations of Combination Pharmacotherapy without waiting for the developed world. We think Combination Pharmacotherapy offers the potential to decrease the incidence of CVD worldwide. This expert panel believes that the concept of CP shows sufficient promise to justify the additional scientific testing of its potential public health applications. Specifically, we recommend further evaluation (Ann Intern Med. 2005;143:593)
 Developing countries may manufacture and distribute variations of Combination Pharmacotherapy without waiting for the developed world. We think Combination Pharmacotherapy offers the potential to decrease the incidence of CVD worldwide. This expert panel believes that the concept of CP shows sufficient promise to justify the additional scientific testing of its potential public health applications. Specifically, we recommend further evaluation. (Ann Intern Med. 2005;143:593)")
74
Fixed Drug Combination for Patients with CHD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)")
75
Fixed Drug Combination for Patients with CVD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)")
76
“ Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.”

78
Fixed Drug Combination for Patients with CHD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)")
79
Fixed Drug Combination for Patients with CVD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)")
80
A pill to prevent 80% of heart attacks
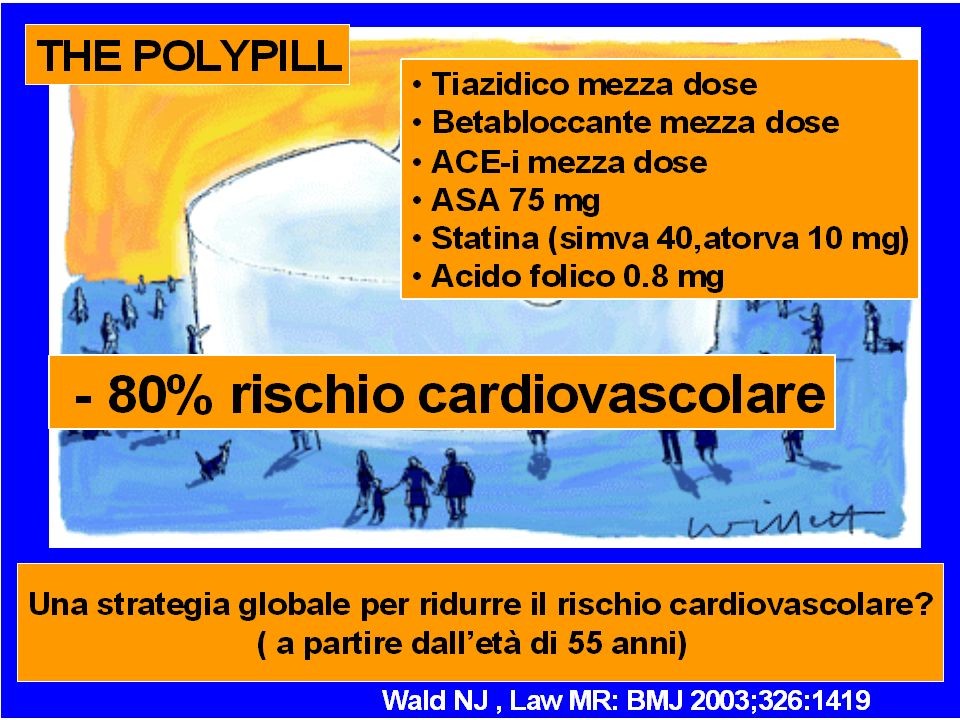
Paper A pill to prevent 80% of heart attacks N J Wald and M R Law BMJ 2003;326:1419 (28 June) POLYPILL: a formulation with a statin, 3 blood pressure lowering drugs each at half standard dose, folic acid (0.8 mg), and aspirin (75 mg) It reduces IHD events by 88% and stroke by 80% One third of people taking this pill from age 55 would benefit, gaining on average about 11 years of life free from an IHD event or stroke
 POLYPILL: a formulation with a statin, 3 blood pressure lowering drugs each at half standard dose, folic acid (0.8 mg), and aspirin (75 mg) It reduces IHD events by 88% and stroke by 80% One third of people taking this pill from age 55 would benefit, gaining on average about 11 years of life free from an IHD event or stroke.")
81
ISO Format MENDIS, Shanthi et al
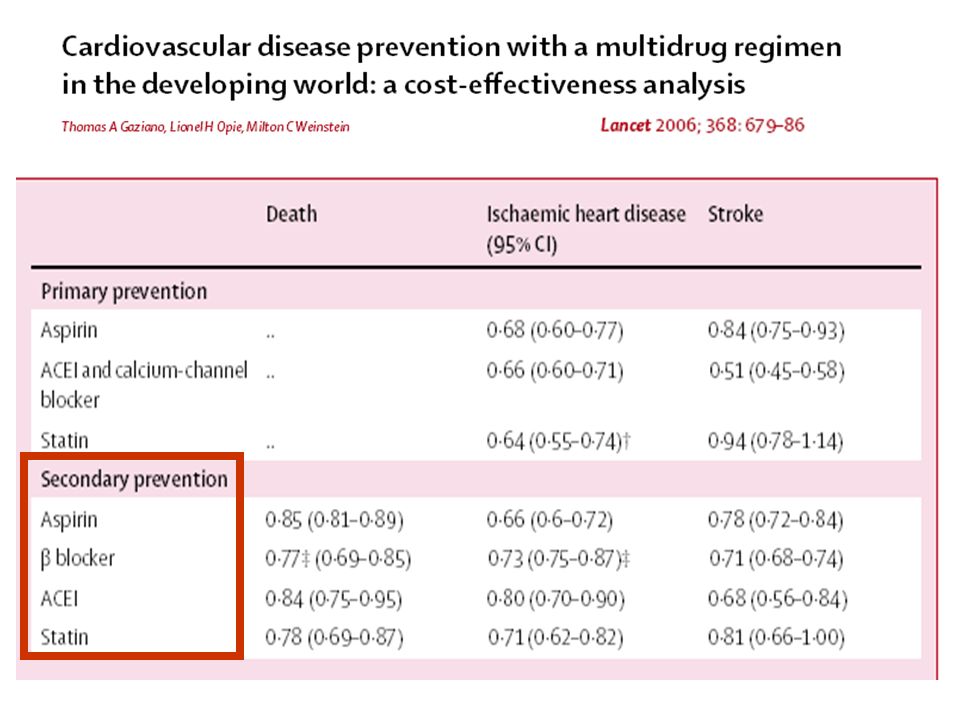
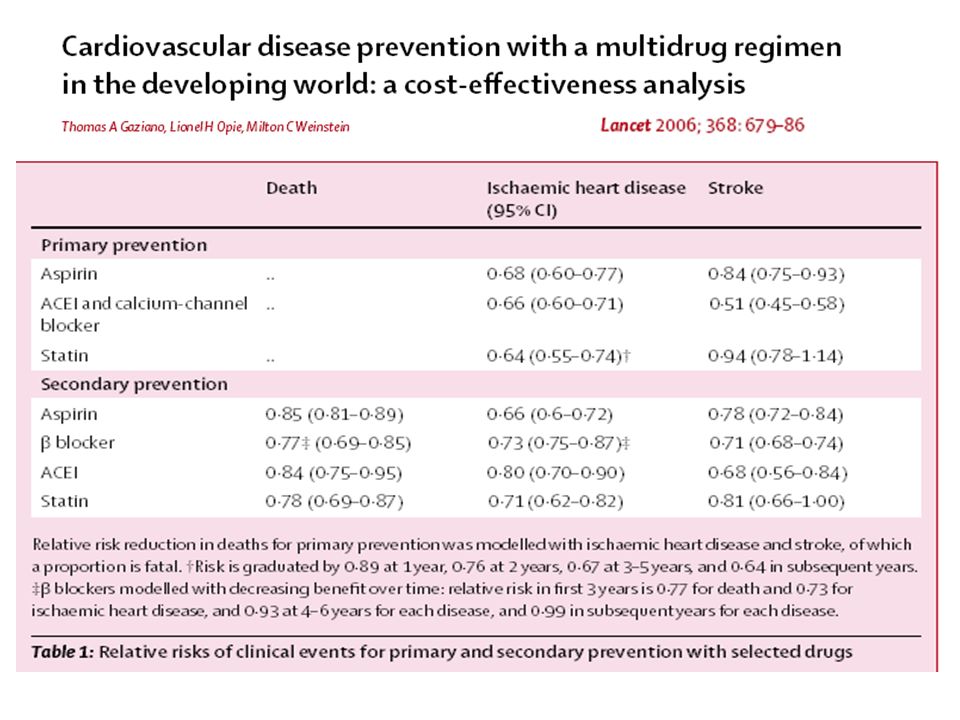
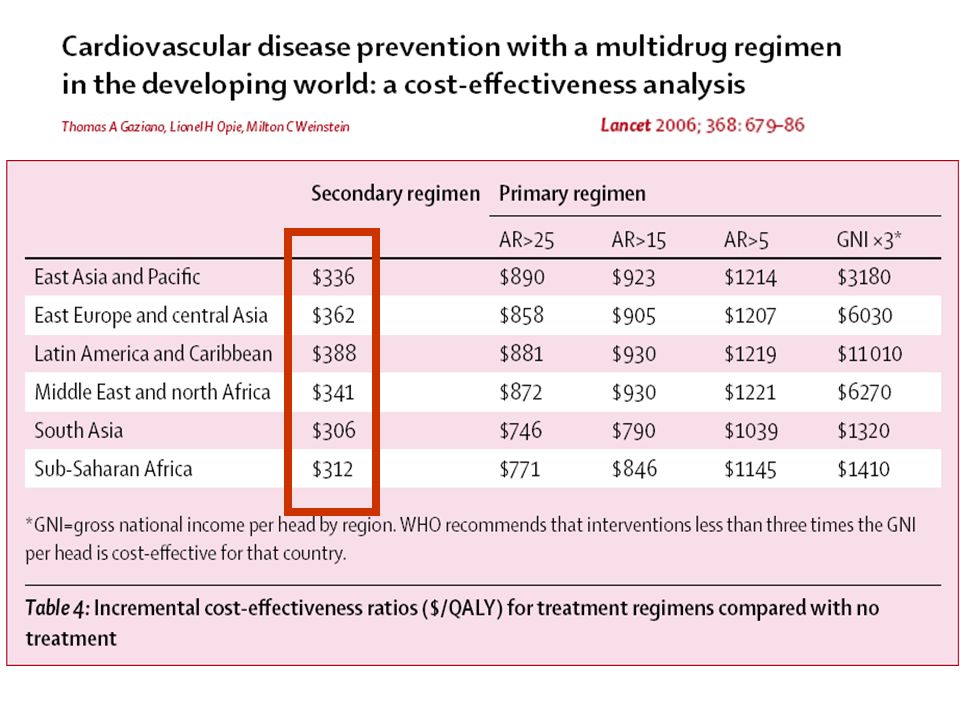
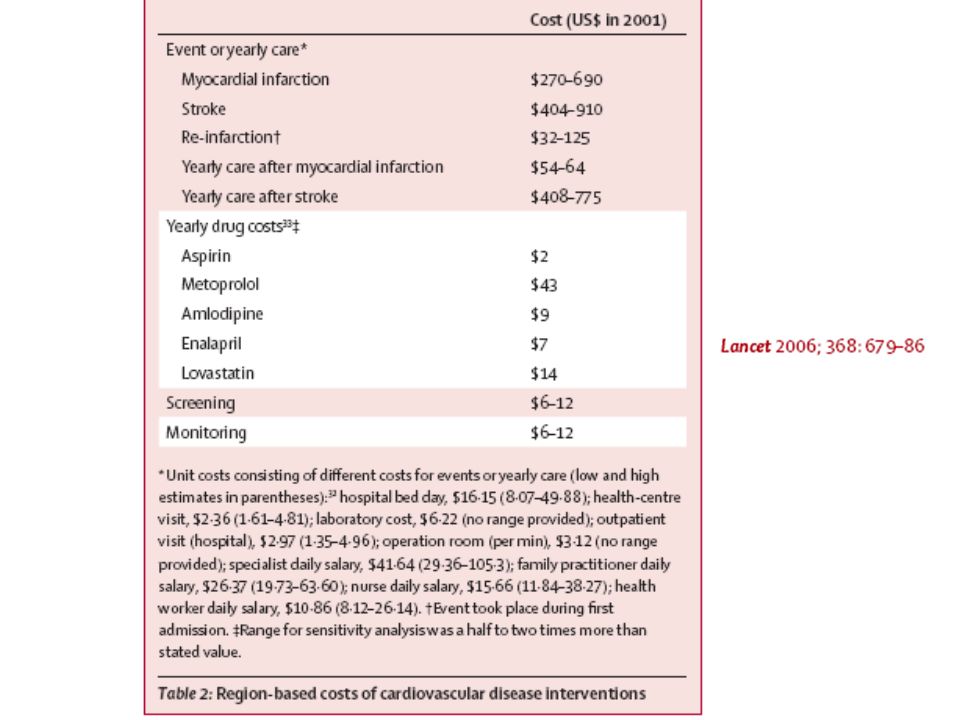
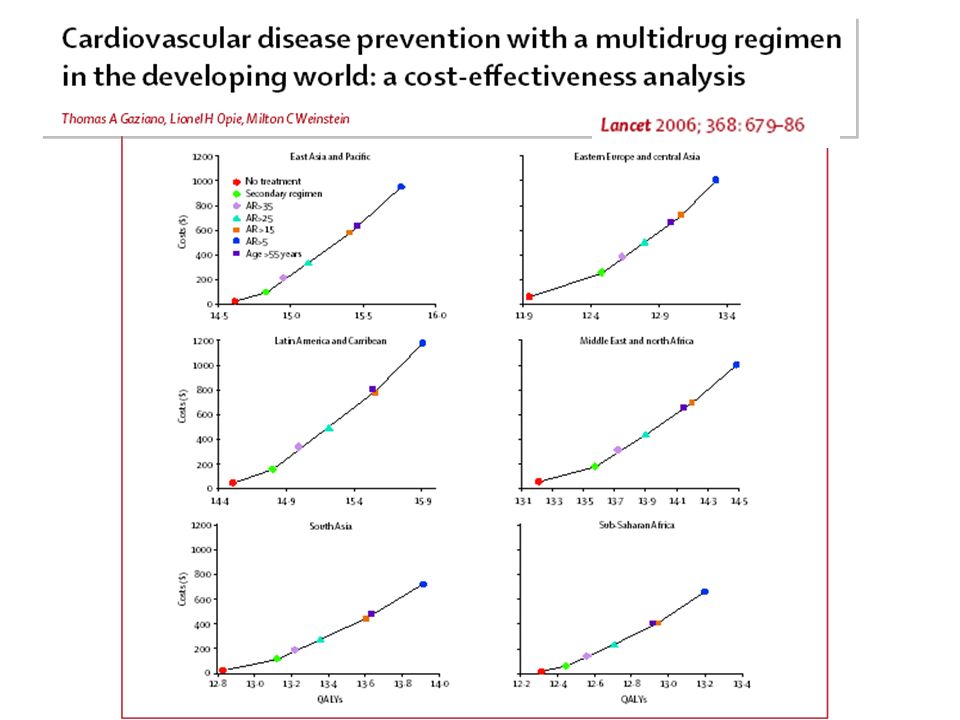
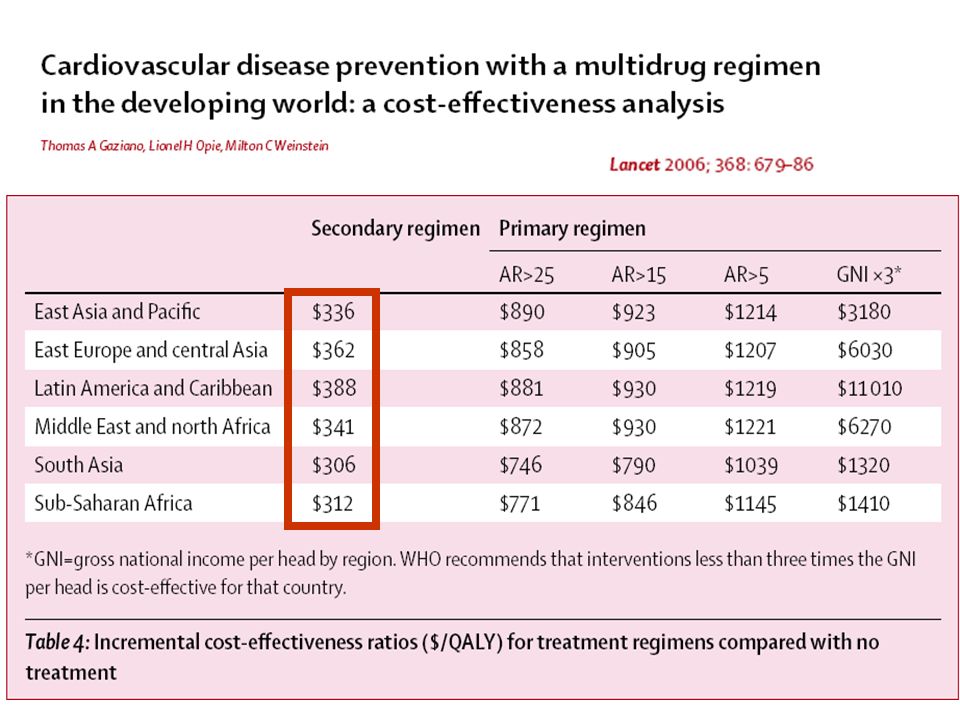
ISO Format MENDIS, Shanthi et al. WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE). Bull World Health Organ, Nov. 2005, vol.83, no.11, p ISSN WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE) Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis Thomas A Gaziano, Lionel H Opie, Milton C Weinstein Lancet 2006;368:679 Summary Background Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries.We therefore aimed to establish whether use of evidence-based multidrug regimens for patients at high risk for cardiovascular disease would be cost-e. ective in low-income and middle-income countries. Methods We used a Markov model to do a cost-e. ectiveness analysis with two combination regimens. For primary prevention, we used aspirin, a calcium-channel blocker, an angiotensin-converting-enzyme inhibitor, and a statin, and assessed them in four groups with different thresholds of absolute risks for cardiovascular disease. For secondary prevention, we assessed the same combination of drugs in one group, but substituted a â blocker for the calcium-channel blocker. To compare strategies, we report incremental cost-effectiveness ratios (ICER), in US$ per quality-adjusted life-year (QALY). Findings We recorded that preventive strategies could result in a 2-year gain in life expectancy. Across six developing World Bank regions, primary prevention yielded ICERs of US$746–890/QALY gained for patients with a 10-year absolute risk of cardiovascular disease greater than 25%, and $1039–1221/QALY gained for those with an absolute risk greater than 5%. ICERs for secondary prevention ranged from $306/QALY to $388/QALY gained. Interpretation Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.
. Bull World Health Organ, Nov. 2005, vol.83, no.11, p ISSN WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE) Cardiovascular disease prevention with a multidrug regimen. in the developing world: a cost-effectiveness analysis. Thomas A Gaziano, Lionel H Opie, Milton C Weinstein. Lancet 2006;368:679. Summary. Background Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries.We therefore aimed to establish whether use of evidence-based multidrug regimens for patients at high risk for cardiovascular disease would be cost-e. ective in low-income and middle-income countries. Methods. We used a Markov model to do a cost-e. ectiveness analysis with two combination regimens. For primary prevention, we used aspirin, a calcium-channel blocker, an angiotensin-converting-enzyme inhibitor, and a statin, and assessed them in four groups with different thresholds of absolute risks for cardiovascular disease. For secondary prevention, we assessed the same combination of drugs in one group, but substituted a â blocker for the calcium-channel blocker. To compare strategies, we report incremental cost-effectiveness ratios (ICER), in US$ per quality-adjusted life-year (QALY). Findings. We recorded that preventive strategies could result in a 2-year gain in life expectancy. Across six developing World Bank regions, primary prevention yielded ICERs of US$746–890/QALY gained for patients with a 10-year absolute risk of cardiovascular disease greater than 25%, and $1039–1221/QALY gained for those with an absolute risk greater than 5%. ICERs for secondary prevention ranged from $306/QALY to $388/QALY gained. Interpretation. Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from. cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.")
82
ISO Format MENDIS, Shanthi et al
ISO Format MENDIS, Shanthi et al. WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE). Bull World Health Organ, Nov. 2005, vol.83, no.11, p ISSN WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE) Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis Thomas A Gaziano, Lionel H Opie, Milton C Weinstein Lancet 2006;368:679 Summary Background Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries.We therefore aimed to establish whether use of evidence-based multidrug regimens for patients at high risk for cardiovascular disease would be cost-e. ective in low-income and middle-income countries. Methods We used a Markov model to do a cost-e. ectiveness analysis with two combination regimens. For primary prevention, we used aspirin, a calcium-channel blocker, an angiotensin-converting-enzyme inhibitor, and a statin, and assessed them in four groups with different thresholds of absolute risks for cardiovascular disease. For secondary prevention, we assessed the same combination of drugs in one group, but substituted a â blocker for the calcium-channel blocker. To compare strategies, we report incremental cost-effectiveness ratios (ICER), in US$ per quality-adjusted life-year (QALY). Findings We recorded that preventive strategies could result in a 2-year gain in life expectancy. Across six developing World Bank regions, primary prevention yielded ICERs of US$746–890/QALY gained for patients with a 10-year absolute risk of cardiovascular disease greater than 25%, and $1039–1221/QALY gained for those with an absolute risk greater than 5%. ICERs for secondary prevention ranged from $306/QALY to $388/QALY gained. Interpretation Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.
. Bull World Health Organ, Nov. 2005, vol.83, no.11, p ISSN WHO study on Prevention of REcurrences of Myocardial Infarction and StrokE (WHO-PREMISE) Cardiovascular disease prevention with a multidrug regimen. in the developing world: a cost-effectiveness analysis. Thomas A Gaziano, Lionel H Opie, Milton C Weinstein. Lancet 2006;368:679. Summary. Background Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries.We therefore aimed to establish whether use of evidence-based multidrug regimens for patients at high risk for cardiovascular disease would be cost-e. ective in low-income and middle-income countries. Methods. We used a Markov model to do a cost-e. ectiveness analysis with two combination regimens. For primary prevention, we used aspirin, a calcium-channel blocker, an angiotensin-converting-enzyme inhibitor, and a statin, and assessed them in four groups with different thresholds of absolute risks for cardiovascular disease. For secondary prevention, we assessed the same combination of drugs in one group, but substituted a â blocker for the calcium-channel blocker. To compare strategies, we report incremental cost-effectiveness ratios (ICER), in US$ per quality-adjusted life-year (QALY). Findings. We recorded that preventive strategies could result in a 2-year gain in life expectancy. Across six developing World Bank regions, primary prevention yielded ICERs of US$746–890/QALY gained for patients with a 10-year absolute risk of cardiovascular disease greater than 25%, and $1039–1221/QALY gained for those with an absolute risk greater than 5%. ICERs for secondary prevention ranged from $306/QALY to $388/QALY gained. Interpretation. Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from. cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.")
83
And so on… Letter Polypill debate continues Letter
People will always be sceptical Letter "Polypill" to fight cardiovascular disease Interpretation of trial data is optimistic Letter "Polypill" to fight cardiovascular disease Birthday present was much appreciated Letter "Polypill" to fight cardiovascular disease Now who's playing God? And so on…

84
“ Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.”

89
RIGHT or WRONG? “The dogs howl, but the moon still keeps on shining” BMJ letter from a medical student “Now who's playing God ?” BMJ letter from S. Taylor and A. Konings A Polypill for Everything ? Is polypill approach feasible and effective in preventing cardiovascular damage?

90
Ingredients of Polymeal:
Wine (150 ml/day) Fish (114 g 4 times/week) Dark chocolate (100 g/day) Fruit & vegetables (400 g/day) Garlic (2.7 g/day) Almonds (68 g/day) BMJ 2004; 329: 1447
 Fish (114 g 4 times/week) Dark chocolate (100 g/day) Fruit & vegetables (400 g/day) Garlic (2.7 g/day) Almonds (68 g/day) BMJ 2004; 329:")
91
Lifetime effect of Polymeal at age 50 Life expectancy free from CVD
Total life expectancy Life expectancy free from CVD None Polymeal +8.1 yrs +4.8 yrs +6.6 yrs +9.0 yrs Years Years Franco OH et al. BMJ 2004; 329: 1447

92
“It may be argued that the Polypill is even more effective, but the Polymeal promises to be an effective, non-pharmacological, safe, and tasty alternative for reducing cardiovascular morbidity and increasing life expectancy in the general population.” Franco OH et al. BMJ 2004; 329: 1447

93
The REACH Study (30.000 pts, 52% donne)
Mc Cullough PA JACC 2002;39:60

94
Naylor MD et al.: JAMA, 281,613,1999 363 pts anziani ( M=75 a.) can varie patologie (60 CHF) ad alto rischio di ricovero INTERVENTO : piano di dimissione articolato visite a casa di infermiere a 2 e 10 gg. contatti telefonici DURATA : 24 settimane RISULTATI : Intervento Controllo Reospedalizzazioni % (-45%) % Reosp. multiple % % Giorni di ricovero Spesa sanitaria $ 0.6 milioni $ 1.2 milioni Costo/paziente $ $ 6661
 37.1% Reosp. multiple 6.2% 14.5% Giorni di ricovero Spesa sanitaria $ 0.6 milioni $ 1.2 milioni. Costo/paziente $ 3630 $")
95
“Gli interventi più efficaci sono quelli capaci di ridurre il
numero delle ospedalizzazioni, la lunghezza della degenza ospedaliera (soprattutto in terapia intensiva), di allungare la vita e di migliorarne la qualità. I dati della Letteratura dimostrano che il “management” ottimale dello scompenso cardiaco congestizio sotto il profi- lo del rapporto costo-efficacia può essere raggiunto attra - verso un approccio multidisciplinare combinato di misure non farmacologiche e di terapia medica massimale. Questo risultato può essere conseguito con un rapporto incrementale costo-efficacia ampiamente nei limiti di accet- tabilità.” ( Rich Mw et al.: Arch. Intern. Med. 159,1690,1999)
, di allungare. la vita e di migliorarne la qualità. I dati della Letteratura dimostrano che il management ottimale dello scompenso cardiaco congestizio sotto il profi- lo del rapporto costo-efficacia può essere raggiunto attra - verso un approccio multidisciplinare combinato di misure. non farmacologiche e di terapia medica massimale. Questo risultato può essere conseguito con un rapporto. incrementale costo-efficacia ampiamente nei limiti di accet- tabilità. ( Rich Mw et al.: Arch. Intern. Med. 159,1690,1999)")
96
CLINIC OR HOME BASED INTERVENTIONS?

97
Veramente, io ero sicuro che…….

98
some widespread misunderstandings about chronic disease - and the reality
Chronic disease epidemic is rapidly evolving Global recognition and response has not kept pace Misunderstandings can be dispelled by the strongest evidence

99
Reality: 80% of chronic disease deaths occur in low & middle income countries

100
Facing illness and deepening poverty

101
Reality: chronic diseases affect men and women almost equally

102
Reality: poor and children have limited choice
The next generation

103
Strong et al, Lancet 2005

104
Strong et al, Lancet 2005

105
Strong et al, Lancet 2005

107
Cost utility Burden of disease Cost effectiveness Cost benefit DALY
IMPATTO SULLE CAUSE DI MORTE/ SPERANZA DI VITA Cost effectiveness COSTO/ANNI DI VITA GUADAGNATI Cost utility DALY QALY OGGETTIVO SOGGETTIVO (anni senza disabilità) (anni in buona qualità di vita percepita) Cost benefit DENARO/DENARO
 (anni in buona qualità di vita. percepita) Cost benefit. DENARO/DENARO.")
112
Blood pressure control
Potential therapeutic strategies to prevent the develoment and/or progression of cardiovascular disease Blood pressure control Glycemic control Weight loss Lipid lowering Combination treatment in a unique “polypill”?

114
Fixed Drug Combination for Patients with CHD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a BB (atenolol 25 mg)")
115
Fixed Drug Combination for Patients with CVD
The Polypill? Low dose antiplatelet (aspirin 75 mg) Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)
 Full dose of a statin (simvastatin 40 mg) Full dose of an ACEI (lisinopril 10 mg) Half dose of a diuretic (HCT 12.5 mg)")
117
“ Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.”

Presentazioni simili






 Brussels, 26 settembre 2013.>")
 Università degli Studi, Pavia (founder) IRCCS Fondazione.>")



 is a disease state characterized by airflow limitation that is not fully reversible. The.>")











>")
