Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Mario Scartozzi Clinica di Oncologia Medica Ancona Targeted Therapies nella Pratica Clinica delle Neoplasie Solide: Neoplasie del Tratto Gastro-Intestinale

2
COLON-RETTO METASTATICO
BEVACIZUMAB CETUXIMAB

3
Progressi nel Carcinoma del Colon-Retto Metastatico
(prima linea) Sopravvivenza Survival ---- Best Supportive Care ---- 5FU/LV ---- Irinotecan/Oxaliplatin 5FU/LV ________________________________________ 5FU/LV OX-Irin Avastin ___________________________________________ RR 20% 40% 45% TTP 4 mesi 7 mesi 10 mesi OS 10 mesi 18 mesi 20 mesi ---- Bevacizumab/IFL p = 0.031
 Sopravvivenza. Survival Best Supportive Care FU/LV Irinotecan/Oxaliplatin 5FU/LV. ________________________________________. 5FU/LV OX-Irin Avastin. ___________________________________________. RR 20% 40% 45% TTP 4 mesi 7 mesi 10 mesi. OS 10 mesi 18 mesi 20 mesi Bevacizumab/IFL. p =")
4
Median overall survival correlates with the % of patients
who receive all 3 drugs in the course of their disease % of Patients With 3 Drugs Median OS (months) 22 21 20 19 17 16 18 15 14 13 10 30 40 50 70 60 80 90 P=.0008 Infusional 5-FU/LV + Oxaliplatin Infusional 5-FU/LV + Irinotecan Bolus 5-FU/LV + Irinotecan Irinotecan + Oxaliplatin Grothey et al. J Clin Oncol. 2004;22;
 P= Infusional 5-FU/LV + Oxaliplatin. Infusional 5-FU/LV + Irinotecan. Bolus 5-FU/LV + Irinotecan. Irinotecan + Oxaliplatin. Grothey et al. J Clin Oncol. 2004;22;")
5
Development of systemic treatments for metastatic colorectal cancer (mCRC)
1957: 5-FU introduced and subsequently dominates the systemic treatment of CRC 1970s – 1980s: various combinations based on 5-FU investigated End of 1980s: 5-FU/FA accepted as standard 1st line treatment for mCRC 1990s: the efficacy of 2nd line treatment established 1999: irinotecan + 5-FU/FA approved 1st line in Europe 1999: oxaliplatin + inf 5-FU/FA approved 1st line in Europe First decade of 21st century: the development of new biologically targeted treatments are expanding the options for mCRC

6
Progressi nel carcinoma del colon-retto metastatico (prima linea)
5FU/LV FOLFOX/FOLFIRI IFL + AVASTIN RR TTP OS 20% 4 mesi 10 mesi 40% 7 mesi 18 mesi 45% 10 mesi 20 mesi COSTI 10 Euro > 60 vv > 200 vv Courtesy Dr Berardi

7
BEVACIZUMAB & CETUXIMAB nel carcinoma del colon-retto: ruolo ed indicazioni
Label Restrictions; Evidence from Randomised Studies; INCREMENTALISTS!!! Major Benefits in Some Patients (Patients Selection); Sinergy (Cetuximab-Bevacizumab).
; Sinergy (Cetuximab-Bevacizumab).")
8
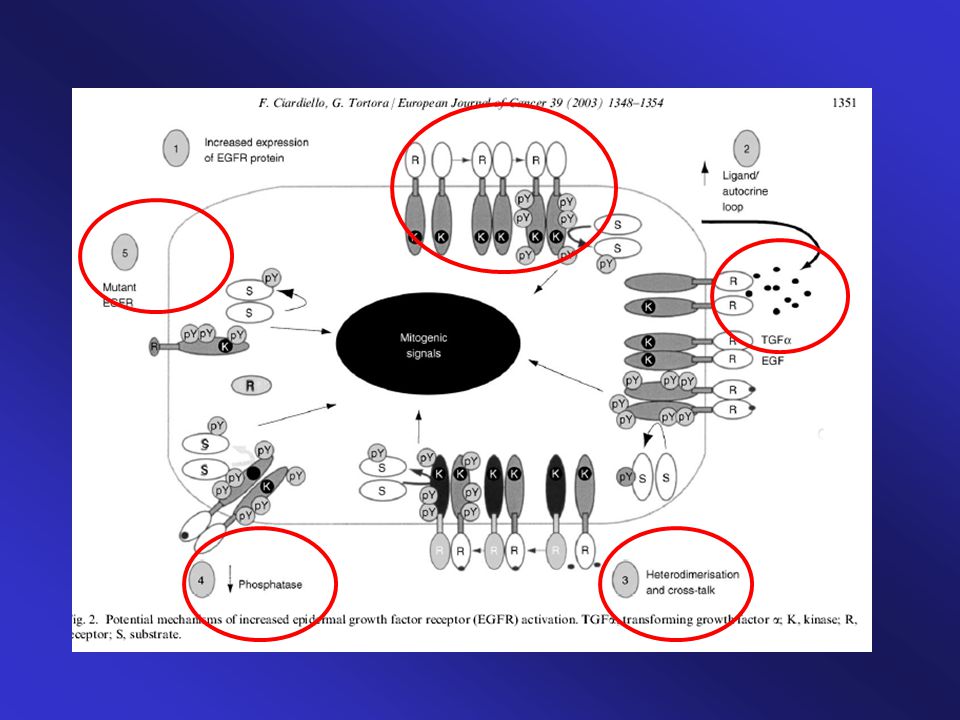
CETUXIMAB (ERBITUX) Anticorpo Monoclonale anti-EGFR
 Anticorpo Monoclonale anti-EGFR")
9
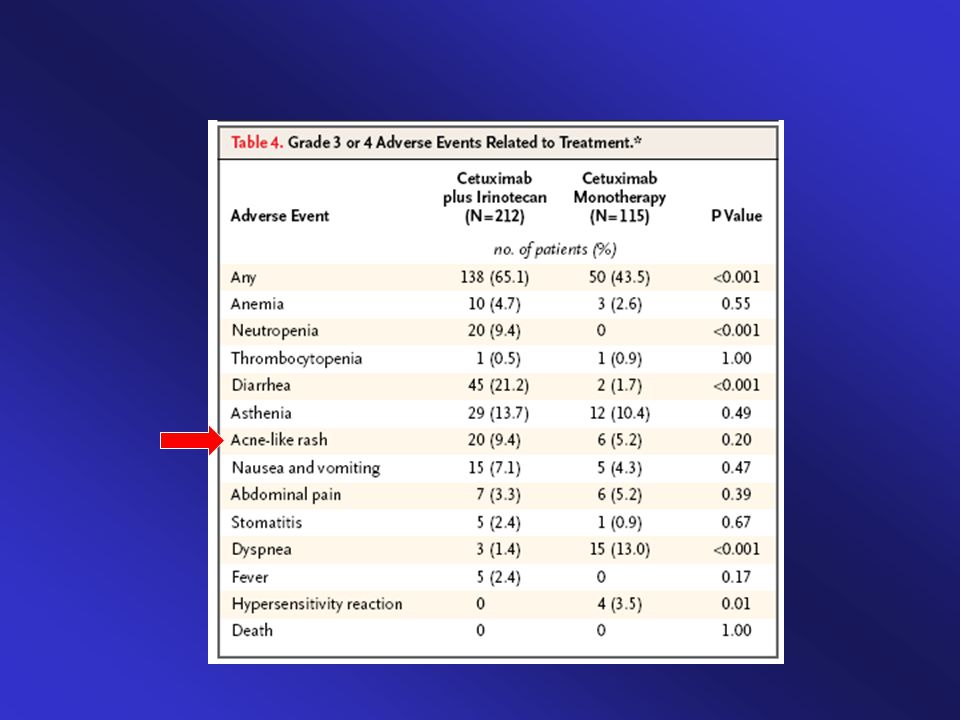
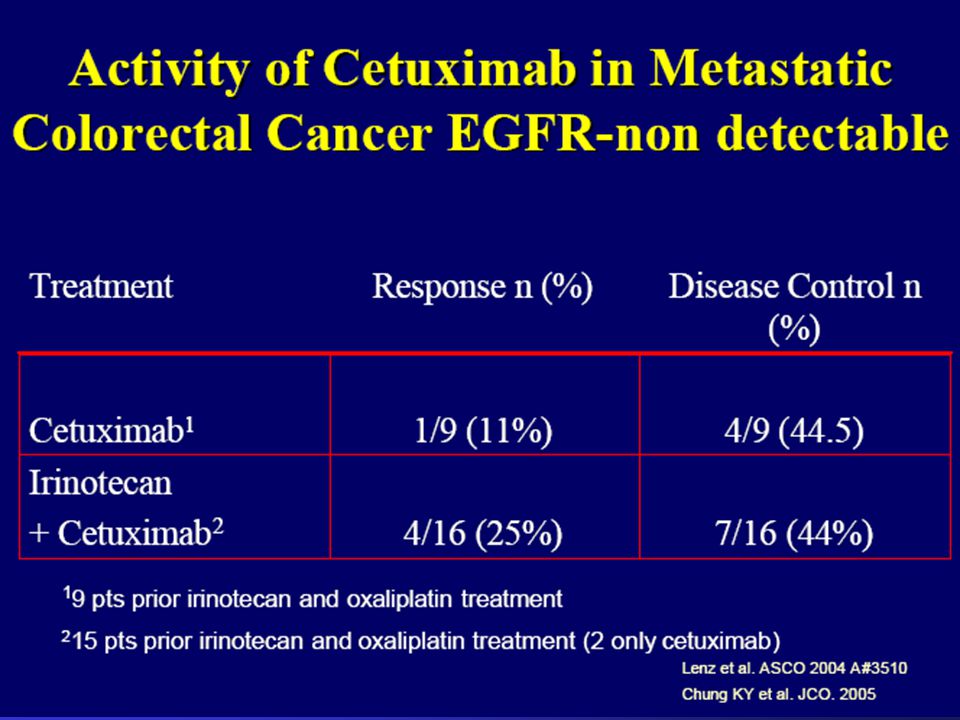
Irinotecan + cetuximab
Patients with CRC progressed on or within 3 months of irinotecan- based chemo-therapy RANDOMIZATION Cetuximab n=111 Irinotecan + cetuximab PD

10
INCREMENTALIST (!)
")
12
Clinical Trials investigating the role of Cetuximab in advanced Colorectal Cancer

13
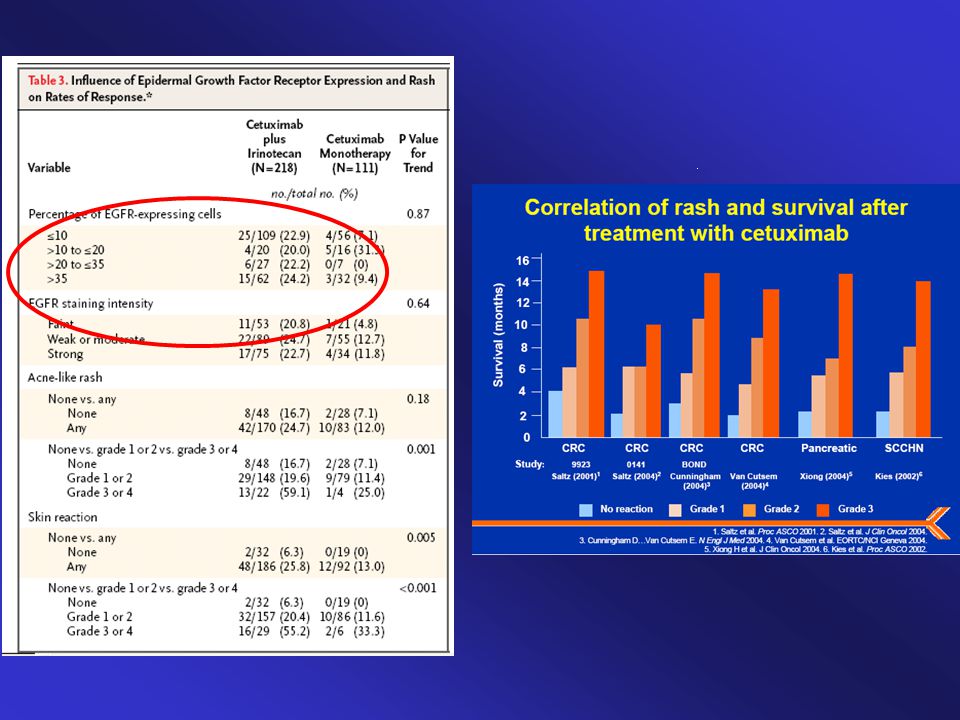
Selezione dei Pazienti (?)
")
19
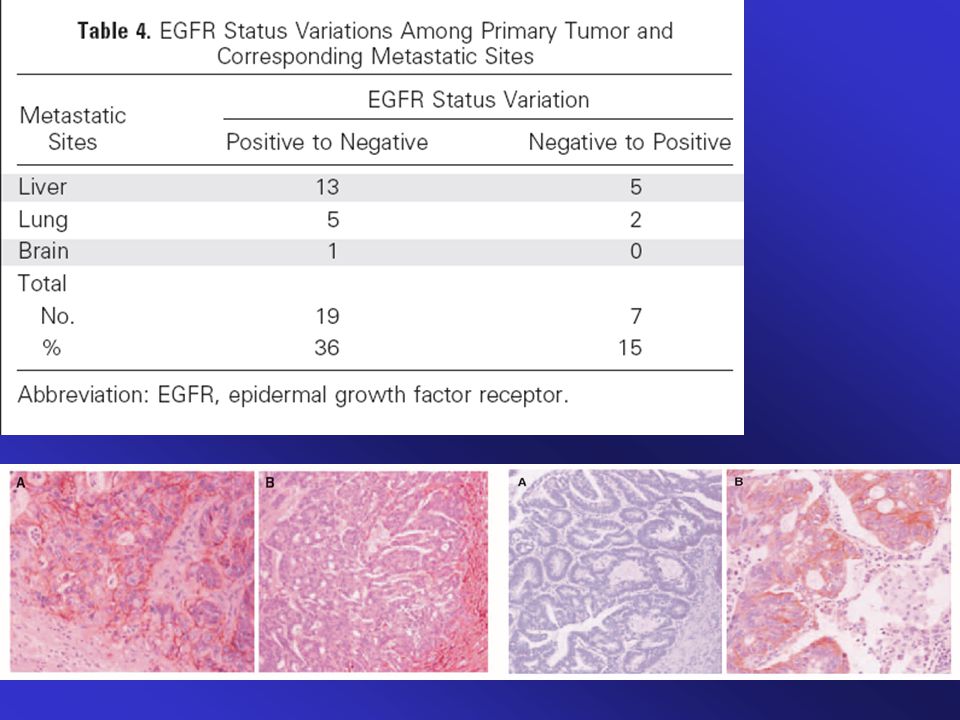
Akt and MAPK status variations among primary tumor and corresponding metastatic sites.
Submitted JCO

20
These are both mammals, but quite different, aren’t they?

22
LABEL RESTRICTIONS (!) IRINOTECAN FAILURE
 IRINOTECAN FAILURE")
23
BEVACIZUMAB (AVASTIN)
Anticorpo Monoclonale anti-VEGF

24
Avastin in combinazione con 5-FU/LV o 5-FU/LV/irinotecan: studi di fase II-III
AVF 2107 (n=923) IFL/placebo (n=411) IFL/Avastin 5 mg (n=402) 5-FU/LV/Avastin 5 mg (n=110) AVF 2192 (n=209) (non candidabili per 1a linea con irinotecan) 5-FU/LV/Avastin 5 mg (n = 104) 5-FU/LV/Placebo (n=105) 5-FU/LV/Avastin 10 mg (n=33) AVF 0780 (n=104) 5-FU/LV (n=36) 5-FU/LV/Avastin 5 mg (n=35)
 IFL/placebo (n=411) IFL/Avastin 5 mg (n=402) 5-FU/LV/Avastin 5 mg (n=110) AVF 2192 (n=209) (non candidabili per 1a linea con irinotecan) 5-FU/LV/Avastin 5 mg (n = 104) 5-FU/LV/Placebo (n=105) 5-FU/LV/Avastin 10 mg (n=33) AVF 0780 (n=104) 5-FU/LV (n=36) 5-FU/LV/Avastin 5 mg (n=35)")
26
Ca colon-retto metastatico 1a linea 5-FU/LV + bevacizumab (n=110)
Studio di fase III nel ca colorettale metastatico: IFL ± bevacizumab (AVF 2107) IFL: 5-FU 500mg/m2 bolo leucovorin 20mg/m2 irinotecan 125mg/m2 4/6 settimane 5-FU/LV: 5-FU 500mg/m2 bolo leucovorin 500mg/m2 6/8 settimane Avastin: 5 mg/kg ogni 2 sett IFL + bevacizumab (n=403) Ca colon-retto metastatico a linea 5-FU/LV + bevacizumab (n=110) IFL + placebo (n=412) Hurwitz H, et al. N Engl J Med 2004;350:2335–42
 IFL: 5-FU 500mg/m2 bolo. leucovorin 20mg/m2 irinotecan 125mg/m2 4/6 settimane. 5-FU/LV: 5-FU 500mg/m2 bolo leucovorin 500mg/m2 6/8 settimane. Avastin: 5 mg/kg ogni 2 sett. IFL + bevacizumab (n=403) Ca colon-retto metastatico 1a linea. 5-FU/LV + bevacizumab (n=110) IFL + placebo (n=412) Hurwitz H, et al. N Engl J Med 2004;350:2335–42.")
27
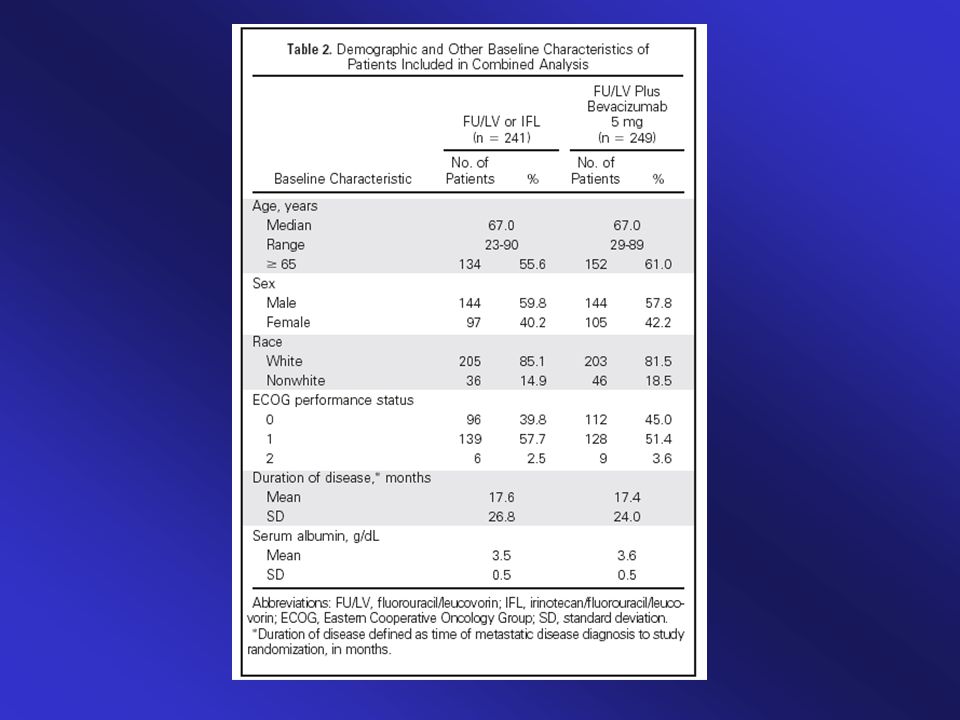
IFL ± Avastin: caratteristiche demografiche
Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without Avastin 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. For the groups in the primary comparison (IFL plus placebo vs IFL plus Avastin), baseline characteristics were similar.1 A total of 813 patients were randomised to these groups. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Hurwitz H, et al. N Engl J Med 2004;350:2335–42
, baseline characteristics were similar.1 A total of 813 patients were randomised to these groups. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Hurwitz H, et al. N Engl J Med 2004;350:2335–42.")
28
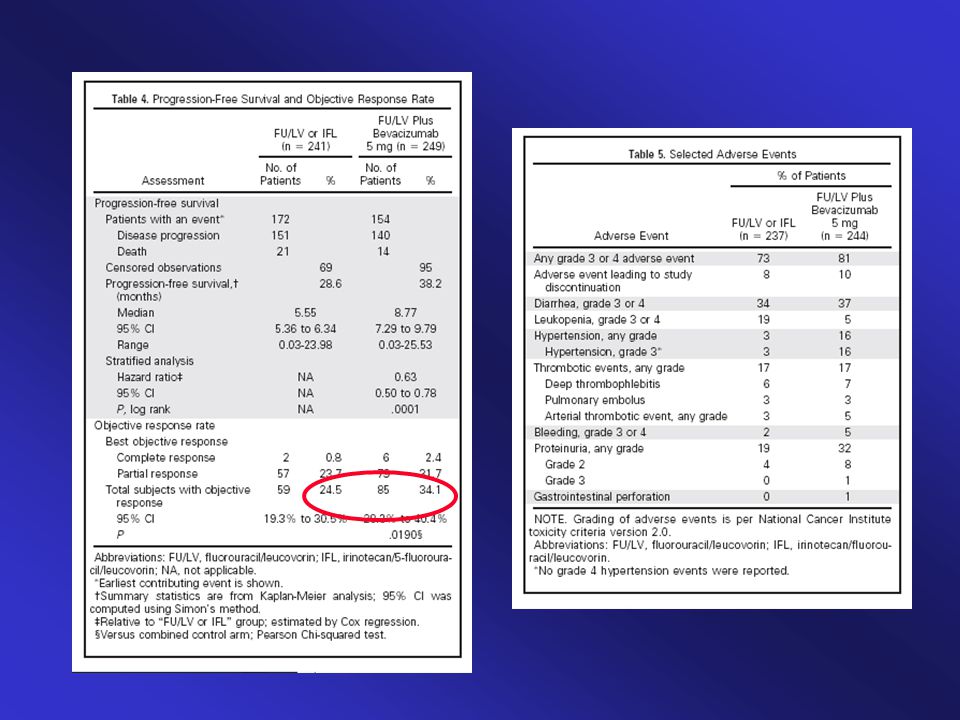
IFL ± Avastin (AVF 2107): risultati clinici
This gives an overview of the excellent efficacy results for Avastin + IFL - all efficacy endpoints were significantly improved in the Avastin arm Hurwitz H, et al. N Engl J Med 2004;350:2335–42

29
Hurwitz H, et al. N Engl J Med 2004;350:2335–42
Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without Avastin 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Progression-free survival was also significantly increased by 71% in the IFL plus Avastin arm (10.6 [95% CI 9.0–11.0] vs 6.2 [95% CI 5.6–7.7] months, p<0.001).1 The stratified HR for disease progression or death during first‑line therapy in the IFL plus Avastin arm relative to the IFL plus placebo arm was 0.54 (95% CI 0.45–0.66). It is interesting to note that the difference in overall and progression-free survival between the two treatment arms is relatively constant at 4.7 and 4.4 months. Together with the study design, in which the treatment arms differed only with the addition of Avastin to IFL, this suggests that the increase in survival is due to the addition of Avastin. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Hurwitz H, et al. N Engl J Med 2004;350:2335–42
.1. The stratified HR for disease progression or death during first‑line therapy in the IFL plus Avastin arm relative to the IFL plus placebo arm was 0.54 (95% CI 0.45–0.66). It is interesting to note that the difference in overall and progression-free survival between the two treatment arms is relatively constant at 4.7 and 4.4 months. Together with the study design, in which the treatment arms differed only with the addition of Avastin to IFL, this suggests that the increase in survival is due to the addition of Avastin. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Hurwitz H, et al. N Engl J Med 2004;350:2335–42.")
30
Hurwitz H, et al. N Engl J Med 2004;350:2335–42
OS a 2-anni: 45% vs 30% Hurwitz H, et al. N Engl J Med 2004;350:2335–42

31
IFL ± Avastin: PFS in responder vs non-responder
Mass R, et al. ASCO 2005: Abstract 3514

32
IFL ± Avastin: OS in responder vs non-responder
Mass R, et al. ASCO 2005: Abstract 3514

33
IFL ± Avastin: profilo tossicità
10 20 30 40 50 60 70 80 90 G 3/4* Tutti G 3/4 leucopenia G 3/4 diarrea Tutte ipertensione* G 3 ipertensione* Trombo embol. G 3/4 sanguin. Perforazione GI IFL Avastin + IFL % pazzienti (%) *Differenza significativa Hurwitz H, et al. N Engl J Med 2004;350:2335–42
 *Differenza significativa. Hurwitz H, et al. N Engl J Med 2004;350:2335–42.")
34
IFL ± Avastin: eventi avversi
Hurwitz H, et al. N Engl J Med 2004;350:2335–42

35
Registro Safety USA post-commercializzazione BRiTE: eventi avversi correlati ad Avastin
Perforazione GI 1.6 % Post-operatorie 0.5 % Tromboembolismi Venosi 2 % Tromboembolismi Arteriosi 0.4 % Kozloff M, et al. ASCO 2005: Abstract 3566 Update WCGC 17 June 2005

36
IFL ± Avastin: sopravvivenza nei sottogruppi (1)
IFL + bevacizumab IFL + placebo Caratteristiche basali Totale Mediana Mediana (n) n (mesi) n (mesi) HR 95% CI HR Tutti i pazienti 813 411 15.61 402 20.34 0.67 0.55 – 0.82 Performance Status ECOG 461 227 17.87 234 24.18 0.66 0.49 – 0.88 ³1 352 184 12.12 168 14.92 0.69 0.53 – 0.90 Numero di siti metastatici 1 306 159 17.94 147 20.50 0.75 0.53 – 1.04 >1 507 252 14.59 255 19.91 0.62 0.48 – 0.80 Sede tumore primario Colon 644 334 15.70 310 19.52 0.74 0.59 – 0.92 Recto 169 77 14.92 92 24.15 0.47 0.30 – 0.73 Età (anni) Subgroup analysis indicates that all subgroups of patients based on clinical characteristics obtain similar benefit from adding bevacizumab to IFL.1,2 Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Novotny WF, Hurwitz H, Fehrenbacher L, et al. Bevacizumab demonstrates a survival benefit in all pre-specified patient subgroups. Proc Am Soc Clin Oncol GI Cancers Symposium 2004 (Abstract 223). <40 35 17 15.61 18 22.83 0.50 0.19 – 1.30 40–64 507 253 15.80 254 19.61 0.71 0.55 – 0.92 ³65 271 141 14.92 130 24.15 0.61 0.43 – 0.87 Novotny W, et al. ASCO GI 2004 (Abstract 223)
 n. (mesi) n. (mesi) HR. 95% CI. HR. Tutti i pazienti – Performance Status ECOG – ³ – Numero di siti metastatici – > – Sede tumore primario. Colon – Recto – Età (anni) Subgroup analysis indicates that all subgroups of patients based on clinical characteristics obtain similar benefit from adding bevacizumab to IFL.1,2 Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Novotny WF, Hurwitz H, Fehrenbacher L, et al. Bevacizumab demonstrates a survival benefit in all pre-specified patient subgroups. Proc Am Soc Clin Oncol GI Cancers Symposium 2004 (Abstract 223). < – – – ³ – Novotny W, et al. ASCO GI 2004 (Abstract 223)")
37
IFL ± Avastin: sopravvivenza nei sottogruppi (2)
IFL + bevacizumab IFL + placebo Caratteristiche basali Totale Mediana Mediana (n) n (mesi) n (mesi) HR 95% CI HR Tutti i pazienti 813 411 15.61 402 20.34 0.67 0.55 – 0.82 Sesso Donne 328 163 15.70 165 18.66 0.73 0.54 – 0.99 Mashi 485 248 15.44 237 21.22 0.64 0.4 9 – 0.83 Razza Bianca 645 328 15.28 317 19.61 0.68 0.55 – 0.85 Altra 168 83 17.43 85 0.61 0.38 – 0.98 Precedente chemioterapia adiuvante Si 209 113 17.64 96 21.62 0.64 0.42 – 0.97 No 604 298 14.62 306 19.42 0.67 0.53 – 0.84 Durata della malattia metastatica (mesi) These data suggest that patients obtained benefit from bevacizumab whether or not they had poor prognostic factors at baseline.1,2 Laboratory measurements were unavailable from some patients for certain parameters, so the subgroups do not all add up to the total of 813. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Novotny WF, Hurwitz H, Fehrenbacher L, et al. Bevacizumab demonstrates a survival benefit in all pre-specified patient subgroups. Proc Am Soc Clin Oncol GI Cancers Symposium 2004 (Abstract 223). <12 760 386 15.70 374 19.91 0.71 0.58 – 0.87 ≥12 53 25 14.65 28 24.54 0.29 0.13 – 0.66 Durata della malattia (mesi) <12 527 260 14.59 267 18.66 0.72 0.38 – 0.91 ≥12 285 151 17.02 134 24.15 0.57 0.40 – 0.82 Novotny W, et al. ASCO GI 2004 (Abstract 223)
 n. (mesi) n. (mesi) HR. 95% CI. HR. Tutti i pazienti – Sesso. Donne – Mashi – Razza. Bianca – Altra – Precedente chemioterapia adiuvante. Si – No – Durata della malattia metastatica (mesi) These data suggest that patients obtained benefit from bevacizumab whether or not they had poor prognostic factors at baseline.1,2. Laboratory measurements were unavailable from some patients for certain parameters, so the subgroups do not all add up to the total of 813. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. Novotny WF, Hurwitz H, Fehrenbacher L, et al. Bevacizumab demonstrates a survival benefit in all pre-specified patient subgroups. Proc Am Soc Clin Oncol GI Cancers Symposium 2004 (Abstract 223). < – ≥ – Durata della malattia (mesi) < – ≥ – Novotny W, et al. ASCO GI 2004 (Abstract 223)")
38
IFL ± Avastin: analisi sui determinanti molecolari
+ placebo + Avastin Biomarcatore Totale n n Mediana (mesi) HR (95% CI) Tutti i pazienti 267 120 17.45 147 26.35 0.57 (0.39–0.85) k-ras (sequenziamento) Mutante Wild type 34 67 44 85 (0.37–1.31) (0.34–0.99) b-raf (sequenziamento) Mutante Wild type 3 97 7 120 (0.01–1.06) (0.34–0.82) K-ras e b-raf (sequenziamento) Mutante Wild type 37 57 51 68 (0.37–1.20) (0.31–1.06) p53 (sequenziamento) 63 31 76 35 27.7 NR (0.30–0.95) (0.32–1.42) p53 (immunoistochimica) Positiva Negativa 92 28 99 47 (0.45–1.10) (0.15–0.70) VEGF-A (ibridazione in situ) Score = 3 Score <3 28 55 29 75 NR (0.18–1.19) (0.20–0.69) HR 0.2 0.5 1 2 5 Koeppen H, et al. EORTC–NCI-AACR 2004; (Abstract 150)
 HR. (95% CI) Tutti i pazienti (0.39–0.85) k-ras (sequenziamento) Mutante Wild type (0.37–1.31) (0.34–0.99) b-raf (sequenziamento) Mutante Wild type (0.01–1.06) (0.34–0.82) K-ras e b-raf (sequenziamento) Mutante Wild type (0.37–1.20) (0.31–1.06) p53 (sequenziamento) NR (0.30–0.95) (0.32–1.42) p53 (immunoistochimica) Positiva Negativa (0.45–1.10) (0.15–0.70) VEGF-A (ibridazione in situ) Score = 3 Score < NR (0.18–1.19) (0.20–0.69) HR Koeppen H, et al. EORTC–NCI-AACR 2004; (Abstract 150)")
39
IFL ± Avastin: analisi sui determinanti molecolari
Frequenza di mutazioni di k-ras, b-raf e p53 simile a quella riportata in letteratura Pazienti con mutazioni in k-ras e/o b-raf hanno una prognosi peggiore, indipendentente dal trattamento La terapia con Avastin ha un impatto sulla sopravvivenza indipendente dallo stato delle mutazioni di k-ras, b-raf o p53, e dall’espressione di p53 o VEGF Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without Avastin 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. The frequency of k-ras, b-raf and p53 mutations in this retrospective subset analysis was similar to published data. Patients with mutations in k-ras and/or b-raf appear to have a poorer prognosis, irrespective of treatment.1 A retrospective analysis of biomarkers (e.g. k-ras, b-raf and p53) in tissue from patients treated with IFL plus Avastin and IFL plus placebo was performed. These data indicate that Avastin therapy has survival benefit in metastatic CRC, regardless of k-ras, b-raf and p53 mutation status, P53 or VEGF expression. Koeppen HKW, Ince WL, Holmgren E, et al. Molecular tumor characteristics and response to bevacizumab plus irinotecan/ 5-fluorouracil/leucovorin in metastatic colorectal cancer. 16th EORTC–NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, Geneva, Switzerland, September 28–October 1, 2004: Abstract 150. Koeppen H, et al. EORTC–NCI-AACR 2004; (Abstract 150)
 in tissue from patients treated with IFL plus Avastin and IFL plus placebo was performed. These data indicate that Avastin therapy has survival benefit in metastatic CRC, regardless of k-ras, b-raf and p53 mutation status, P53 or VEGF expression. Koeppen HKW, Ince WL, Holmgren E, et al. Molecular tumor characteristics and response to bevacizumab plus irinotecan/ 5-fluorouracil/leucovorin in metastatic colorectal cancer. 16th EORTC–NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics, Geneva, Switzerland, September 28–October 1, 2004: Abstract 150. Koeppen H, et al. EORTC–NCI-AACR 2004; (Abstract 150)")
40
BEVACIZUMAB IN COMBINAZIONE CON 5-FU/LV

45
RR 35 vs 45 RR 15 vs 26

46
Label Restrictions

47
Cetuximab/ irinotecan Avastin/ cetuximab/ irinotecan
BOND-2 (vs BOND-1) Cetuximab/ irinotecan (storico) Avastin/ cetuximab/ irinotecan p Tasso risposte (%) 23 37 0.03 TTP (mesi) 4 7.9 <0.01 Cetuximab Avastin/ cetuximab 11 20 0.05 1.5 5.6 BOND 3= cetux-bevaciz-irino vs cetux-bevaciz (in pazienti pretrattati con bevacizumab) Saltz L, et al. ASCO 2005 (Abstract 358)
 Cetuximab/ irinotecan. (storico) Avastin/ cetuximab/ irinotecan. p. Tasso risposte (%) TTP (mesi) <0.01. Cetuximab. Avastin/ cetuximab BOND 3= cetux-bevaciz-irino vs cetux-bevaciz (in pazienti pretrattati con bevacizumab) Saltz L, et al. ASCO 2005 (Abstract 358)")
49
Terapia su “Misura”? ….Variabilita` Biologica!!
______________________________________________

Presentazioni simili

















>")





 N. Pazienti in Dialisi (2002: 308.910)>")