Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Lezione Corso di Oncologia Università Vita e Salute 30 novembre 2009
Nuovi farmaci antitumorali Giorgio Parmiani Unità di Immunobioterapia del Melanoma e Tumori Solidi, Istituto Scientifico Universitario Fondazione San Raffaele, MIlano

2
Il cancro è una malattia genetica
…..ma il lavoro lo fanno le proteine

3
cellula tumorale mRNA Proteine DNA mRNA 46 Cromosomi

4
Antireceptor Antibodies Angiogenesis Inhibitors
TERAPIE TARGET Immune System Activation (T, NK, NKT cells, Mabs) Antireceptor Antibodies Tumor Cell Kinase Inhibitors Nucleus Angiogenesis Inhibitors Hormone Agonists/ Antagonists
 Antireceptor Antibodies. Tumor Cell. Kinase Inhibitors. Nucleus. Angiogenesis Inhibitors. Hormone Agonists/ Antagonists.")
5
New targets in cancer including normal, stromal cells
Cancer Cell Endothelial Cell Growth Factors Nutrients VEGFR PDGFR-b PI3K mTOR Akt Protein Synthesis mTOR Tumor Cell Growth & Proliferation Bioenergetics Vascular Cell Growth Angiogenic Factors Vascular Pericyte

6
mTOR Coordinates Cancer Cell Growth
Blood Vessel Nutrient Availability Production of Transporters Increased Nutrient Uptake mTOR coordinates cancer cell growth mTOR activation promotes entry into the cell cycle1, thus committing the cell to divide Cells require a lot of nutrients and energy resources to maintain the metabolic requirements found in cancer2. Cancer cells have to find additional sources of nutrients and energy once the cellular supplies are low. Cancer cells gain access to additional resources through increased availability to extracellular nutrients and through angiogenesis3 mTOR activation leads to increased expression of transporters at the cell membrane and increases the secretion of proangiogenic molecules, such as VEGF4,5,6 Secretion of VEGF induces capillary outgrowth from nearby blood vessels7 Capillary outgrowth toward the tumor cells provides new sources of vital oxygen, glucose, and amino acids Additional nutrient availability enables tumor growth and survival8,9 References Nelsen et al. J Biol Chem. 2003;278: Shaw. Curr Opin Cell Biol. 2006;18(6): Hickey and Simon. Curr Top Dev Biol. 2006;76: Wieman et al. Mol Biol Cell Feb 14 (ahead of print). Fuchs and Bode. Semin Cancer Biol. 2005;15(4): Edinger and Thompson. Mol Biol Cell. 2002;13(7): Bernanke and Velkey. Anat Rec. 2002;269(4): Nishida et al. Vasc Health Risk Manag. 2006;2(3): Brahimi-Horn and Pouyssegur. Int Rev Cytol. 2005;242: Secretion of Angiogenic Growth Factors Glucose Transporter mTOR Mutations in Cancer Amino Acid Transporter M G1 G2 Cancer Cell Growth Cancer Cell S
: Hickey and Simon. Curr Top Dev Biol. 2006;76: Wieman et al. Mol Biol Cell Feb 14 (ahead of print). Fuchs and Bode. Semin Cancer Biol. 2005;15(4): Edinger and Thompson. Mol Biol Cell. 2002;13(7): Bernanke and Velkey. Anat Rec. 2002;269(4): Nishida et al. Vasc Health Risk Manag. 2006;2(3): Brahimi-Horn and Pouyssegur. Int Rev Cytol. 2005;242: Secretion of Angiogenic Growth Factors. Glucose Transporter. mTOR. Mutations in Cancer. Amino Acid Transporter. M. G1. G2. Cancer Cell Growth. Cancer Cell. S.")
7
BLOCCARE IL SINGOLO TARGET?
TERAPIE TARGET BLOCCARE IL SINGOLO TARGET? BLOCCARE IL CIRCUITO

8
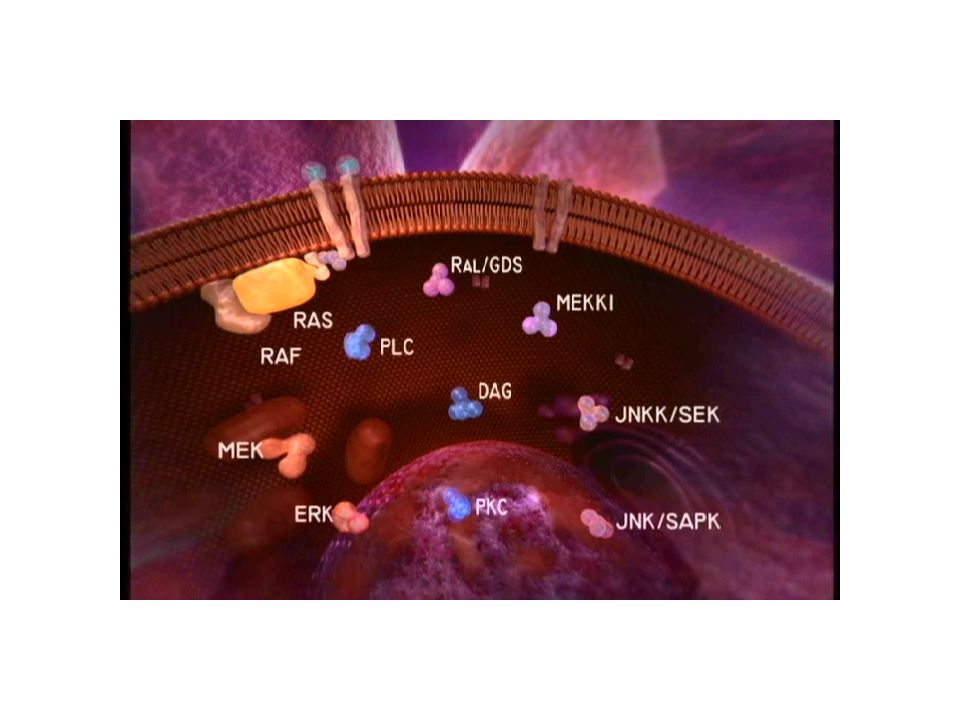
La cascata di segnali intracellulari
LPA, thrombin ET, etc. TGFa (1) EGF (1) Epiregulin (1,4) b-cellulin (1) HB-EGF (1,4) Amphi- regulin (1) NRG1 (3,4) NRG2 (4) NRG3 (4) NRG4 (4) Cytokines Ligands a b a b Input layer 2 2 4 2 1 2 2 1 1 4 3 4 4 1 3 4 1 3 3 3 Receptor dimers Src Jak Cbl Shc Adaptors and enzymes PLCg Ras-GDP Crk PI3K Vav Grb7 Shp2 GAP Grb2 Nck Sos Signal- processing layer Ras-GTP Rac In condizioni fisiologiche l’attivazione di EGFR prevede diversi step successivi: Interazione tra ligando e EGFR, Formazione di dimeri recettoriali, Attivazione del recettore, transfosforilazione dei partner del complesso dimerico, Fosforilazione delle tirosine presenti sulla coda del recettore, che diventano sito di attacco per proteine segnale intracellulari capaci di legare le tirosine fosforilate Akt RAF PAK MEK JNKK Abl Cascades PKC Bad S6K MAPK JNK Jun Transcription factors Sp1 Myc Fos Elk Egr1 Stat Output layer Apoptosis Migration Growth Adhesion Differentiation Yarden Y, Sliwkowski M. Nat Rev Mol Cell Biol 2001;2:127–37
 EGF (1) Epiregulin (1,4) b-cellulin (1) HB-EGF (1,4) Amphi- regulin (1) NRG1 (3,4) NRG2 (4) NRG3 (4) NRG4 (4) Cytokines. Ligands. a. b. a. b. Input layer Receptor dimers. Src. Jak. Cbl. Shc. Adaptors and enzymes. PLCg. Ras-GDP. Crk. PI3K. Vav. Grb7. Shp2. GAP. Grb2. Nck. Sos. Signal- processing layer. Ras-GTP. Rac. In condizioni fisiologiche l’attivazione di EGFR prevede diversi step successivi: Interazione tra ligando e EGFR, Formazione di dimeri recettoriali, Attivazione del recettore, transfosforilazione dei partner del complesso dimerico, Fosforilazione delle tirosine presenti sulla coda del recettore, che diventano sito di attacco per proteine segnale intracellulari capaci di legare le tirosine fosforilate. Akt. RAF. PAK. MEK. JNKK. Abl. Cascades. PKC. Bad. S6K. MAPK. JNK. Jun. Transcription factors. Sp1. Myc. Fos. Elk. Egr1. Stat. Output layer. Apoptosis. Migration. Growth. Adhesion. Differentiation. Yarden Y, Sliwkowski M. Nat Rev Mol Cell Biol 2001;2:127–37.")
9
Circuiti complessi hanno più interruttori che richiedono una strategia multitarget

10
Vie multiple di trasmissione del segnale rendono difficile il blocco della crescita cellulare o l’eliminazione delle cellule neoplastiche.

11
I Recettori per EGF Iperattivi nei tumori per eccesso di stimoli recettoriali o per mutazione Una volta fosforilati innescano: La cascata metabolica Ras-Raf-MAPK (Mitogen Activated Protein Kinase pathway), La cascata metabolica, PI3K (Phosphatidyl Inositol 3 Kinase)-Akt (Protein Kinase B), La via metabolica PLC- e PKC porta all’attivazione di Proteina kinasi-C (PKC),
, La cascata metabolica, PI3K (Phosphatidyl Inositol 3 Kinase)-Akt (Protein Kinase B), La via metabolica PLC- e PKC porta all’attivazione di Proteina kinasi-C (PKC),")
12
STRATEGIE ANTI-RECETTORE EGF
The concept targeted therapy for a broad range of common solid tumors Clinical trials proof of concept well tolerated therapy tumor responses in several tumor types The promise improved outcomes in the treatment of common solid tumors EGFR R R MAb Tumor cell membrane K Small mol K K Tumor response Razionale per l’utilizzo di Iressa nei tumori solidi che overesprimono EGFR. Allo stato attuale vi sono studi di combinazione con chemioterapia nel polmone e carcinoma del colon e studi in monoterapia in diverse neoplasie solide. Infine sono in corso di valutazioni combinazioni con ormonoterapia e radioterapia nel carcinoma dell amammella e della prostata. Metastasis Invasion Inibition of apoptosis Angiogenesis Proliferation

13
1. ANTICORPI MONOCLONALI
Anti-antigeni di superficie Rituximab; Linfociti T, NK Anti recettore EGF Cetuximab (anti-HER1) Trastuzumab (anti-HER2) Pertuzumab (anti-dimerizzazione) Anti fattori angiogenici Bevacizumab (anti-VEGF)
 Trastuzumab (anti-HER2) Pertuzumab (anti-dimerizzazione) Anti fattori angiogenici. Bevacizumab (anti-VEGF)")
14
RITUXIMAB Immunoglobulina, con alta affinità per CD20
CD20 è un antigene di superficie, coinvolto nella regolazione della crescita delle cellule B L’Ag CD20 è ristretto ai precursori delle cellule B e alle B cellule mature, ma viene perso quando le cellule B si differenziano in plasmacellule Ab secernenti. CD20 è espresso in oltre il 95% delle cellule maligne dei LNH di tipo B.

15
RITUXIMAB Rituximab (R) è attivo nei LNH a basso grado, follicolari, e in quelli ad alto grado, sia come agente singolo, sia in associazione alla chemioterapia. In monoterapia induce risposte fino al 50% nei LNH indolenti recidivati e fino al 30% nei LNH aggressivi recidivati. Le percentuali di risposta sono più alte (> 70%) se il farmaco viene usato in pazienti non pretrattati.
 è attivo nei LNH a basso grado, follicolari, e in quelli ad alto grado, sia come agente singolo, sia in associazione alla chemioterapia. In monoterapia induce risposte fino al 50% nei LNH indolenti recidivati e fino al 30% nei LNH aggressivi recidivati. Le percentuali di risposta sono più alte (> 70%) se il farmaco viene usato in pazienti non pretrattati.")
16
CETUXIMAB Blocca i siti di legame extra-cellulare di EGFR (HER1)
Primi studi: Primi dati clinici: Attività additiva/sinergica con la Radioterapia Attività additiva/sinergica con la Chemioterapia (Platino, Doxorubicina, Gemcitabina, CPT-11) Registrato per i tumori del colon retto e del capo-collo
 Registrato per i tumori del colon retto e del capo-collo.")
17
Cetuximab + RT nei tumori testa/collo: aumenta controllo locale, PFS e OS
Bonner JA et al NEJM 2006;354:

18
Cetuximab + cisplatino nei tumori testa/collo recidivati o metastatici
Per la prima volta in 25 anni, dalla comparsa dell’uso del cisplatino, si ottiene un aumento della sopravvivenza, Vermorken JB, ASCO 2007:abs.6013

19
Cetuximab nel carcinoma del colon
1147 Pazienti Resistenti a Irinotecan Cetuximab nel carcinoma del colon

20
Cetuximab nel ca. colon retto

21
CETUXIMAB nei carcinomi del colon retto e testa/collo
Molto attivo anche in paziente chemio-resistenti Sinergico con la chemioterapia e la radioterapia Non aumenta le complicanze chirurgiche Ben tollerato: diarrea e rash cutaneo acneiforme come tossicità principali

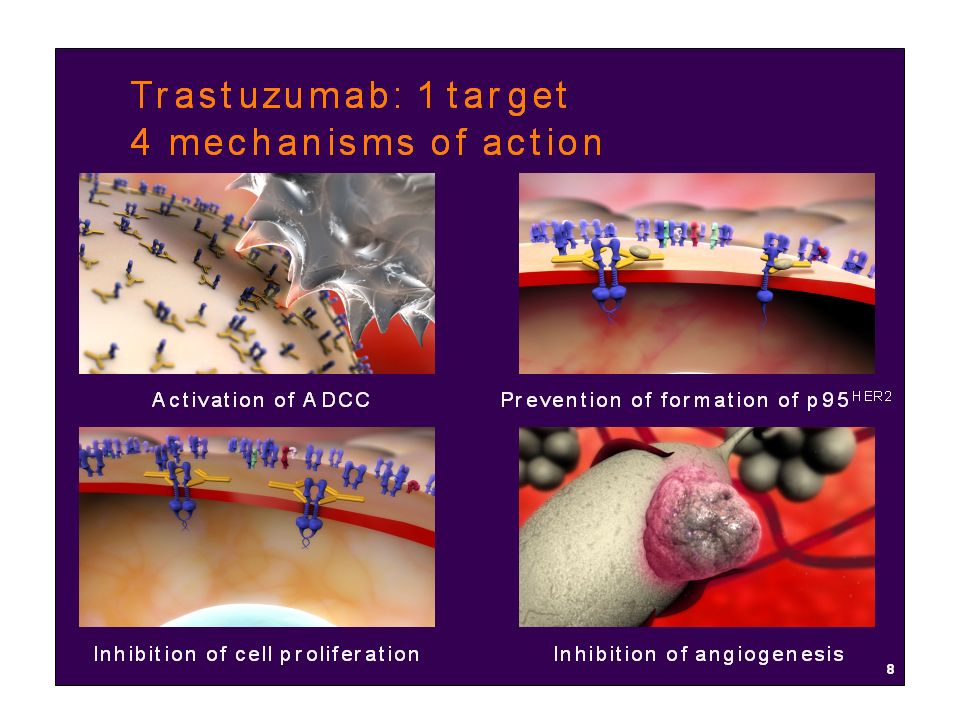
22
TRASTUZUMAB nel carcinoma mammario (Herceptin)
Anticorpo monoclonale “umanizzato” Diretto contro HER2/neu Approvato dalla FDA nel 1998 Herceptin è un anticorpo monoclonale umanizzato, ricombinante diretto contro Her2 Umanizzare si intende: identificare la sequenza minima di aminoacidi residui nella regione che determina la complementarietà dell’anticorpo murino richiesta per la specificità antigenica e per l’affinità antigene-legante e sostituire queste regioni con un frame work consenso di IgG umana in modo da mantenere sia la specificità dell’antigene che l’affinità di legame.

24
Carcinoma della mammella: Trastuzumab +Paclitaxel vs Paclitaxel
(HER+++) Trastuzumab + Paclitaxel Paclitaxel P-value Median TTP (mos.) 6.9 3.0 <0.001 OR (%) 38.0 16.0 Median duration 10.5 4.5 Median TTF (mos) 5.8 2.9 Median OS (mos) 22.1 18.4 <0.05 Slamon NEJM 2001
 Trastuzumab + Paclitaxel. Paclitaxel. P-value. Median TTP (mos.) < OR (%) Median duration Median TTF (mos) Median OS (mos) <0.05. Slamon NEJM")
25
Carcinoma della mammella: Trastuzumab + Docetaxel vs Docetaxel
TRASTUZ.+DOCETAX. DOCETAXEL ALONE P ORR 61 34 0.0002 CR 7 2 PR 54 32 SD 27 44 DR* med. mos. 11.7 5.7 0.009 TTPmed. mos. 6.1 0.0001 OS med. mos. 31.2 22.7 0.0325 *Duration of response Marty M et al, JCO 2005

26
Tassi di risposte obbiettive nel carcinoma della mammella
Herceptin Taxanes Antracyclines Pre-Antracyclines 1970 1980 1990 2000 Mean values fron pooled studies

27
HERA: Trastuzumab in HER2+ Early Breast Cancer (cont’d)
1703 1127 140 1698 930 114 HR: 0.63 (95% CI: ; P<0.0001) 3-year DFS: 80.6% vs 74.0% Disease-Free Survival (Censored) Patients (%) 100 80 60 40 20 12 36 18 6 24 30 Observation 1 year trastuzumab Months From Randomization Patients Alive (%) 1703 1190 146 1698 1042 126 100 80 60 40 20 12 36 18 6 24 30 Overall Survival (Censored) Observation 1 year trastuzumab Months From Randomization HR: 0.63 (95% CI: ; P<0.0051) 3-year OS: 92.4% vs 89.2% I. Smith. ASCO, 2006.
 3-year DFS: 80.6% vs 74.0% Disease-Free Survival (Censored) Patients (%) Observation. 1 year trastuzumab. Months From Randomization. Patients Alive (%) Overall Survival (Censored) Observation. 1 year trastuzumab. Months From Randomization. HR: 0.63 (95% CI: ; P<0.0051) 3-year OS: 92.4% vs 89.2% I. Smith. ASCO,")
28
Trastuzumab nella terapia adiuvante del carcinoma mammario HER2+ (HERA trial)
DFS a 3 anni (1a T vs O) ITT: Hazard Ratio 0.64, P<0.0001 OS a 3 anni (1a T vs O) ITT: HR 0.66, P=0.015 Principale tossicità: cardiotossicità Risultati simili in altri 4 studi, particolarmente NSABP B31 (AC Tax ±Trastuzumab) Smith I. ASCO, 2006.
 ITT: Hazard Ratio 0.64, P< OS a 3 anni (1a T vs O) ITT: HR 0.66, P= Principale tossicità: cardiotossicità. Risultati simili in altri 4 studi, particolarmente NSABP B31 (AC Tax ±Trastuzumab) Smith I. ASCO,")
29
Trastuzumab: conclusioni
Trastuzumab rappresenta attualmente la terapia standard, sia in fase avanzata che adiuvante,per il trattamento della pazienti con carcinoma della mammella con iperespressione di HER2+ determinata con Immunoistochimica (3+) o con positività di fluorescence in situ hybridization (FISH). Sulla base di questi risultati, herceptin è il trattamento standard per pazianti con carcinoma mammario con overspressione di cerbB-2 e che I migliori risultati si ottengono se utilizzato in prima linea.
 o con positività di fluorescence in situ hybridization (FISH). Sulla base di questi risultati, herceptin è il trattamento standard per pazianti con carcinoma mammario con overspressione di cerbB-2 e che I migliori risultati si ottengono se utilizzato in prima linea.")
30
Terapia anti-vascolare

31
Vascular Endotelial Growth Factor: elemento chiave dell’angiogenesi
Hypoxia PDGF IGF-1 EGF IL-8 Binding and activation of VEGF receptor VEGF release bFGF COX-2 Nitric oxide Oncogenes P– – P P– – P Survival Proliferation Migration Permeability ANGIOGENESIS VEGF = vascular endothelial growth factor; IGF = insulin-like growth factor PDGF = platelet-derived growth factor; EGF = epidermal growth factor 31

32
BEVACIZUMAB Anticorpo monoclonale con elevata affinità per VEGF-A.
Inibizione diretta di VEGF-A Previene l’interazione di VEGF-A con i recettori VEGFR1 e VEGFR2 sulla superficie delle cellule endoteliali, inibendo così la neo-angiogenesi.

33
Aumento significativo del tempo a progressione e della sopravvivenza
Bevacizumab + Irinotecan* come terapia di prima linea nel carcinoma del colon retto Median PFS 6.2 vs 10.6 months HR=0.54 p<0.0001 Median OS 15.6 vs 20.3 months HR=0.66 p<0.001 1.0 0.8 0.6 0.4 0.2 1.0 0.8 0.6 0.4 0.2 IFL + Avastin (n=402) IFL + placebo (n=411) IFL + Avastin (n=402) IFL + placebo (n=411) PFS estimate Survival estimate Progression-free survival was also significantly increased by 71% in the IFL plus Avastin arm (10.6 [95% CI 9.0–11.0] vs 6.2 [95% CI 5.6–7.7] months, p<0.001).1 The stratified HR for disease progression or death during first‑line therapy in the IFL plus Avastin arm relative to the IFL plus placebo arm was 0.54 (95% CI 0.45–0.66). It is interesting to note that the difference in overall and progression-free survival between the two treatment arms is relatively constant at 4.7 and 4.4 months. Together with the study design, in which the treatment arms differed only with the addition of Avastin to IFL, this suggests that the increase in survival is due to the addition of Avastin. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. 6.2 10.6 15.6 20.3 Months Months Aumento significativo del tempo a progressione e della sopravvivenza *Inibitore di topoisomeasi Hurwitz, et al. NEJM 2004
 IFL + placebo (n=411) IFL + Avastin (n=402) IFL + placebo (n=411) PFS estimate. Survival estimate. Progression-free survival was also significantly increased by 71% in the IFL plus Avastin arm (10.6 [95% CI 9.0–11.0] vs 6.2 [95% CI 5.6–7.7] months, p<0.001).1. The stratified HR for disease progression or death during first‑line therapy in the IFL plus Avastin arm relative to the IFL plus placebo arm was 0.54 (95% CI 0.45–0.66). It is interesting to note that the difference in overall and progression-free survival between the two treatment arms is relatively constant at 4.7 and 4.4 months. Together with the study design, in which the treatment arms differed only with the addition of Avastin to IFL, this suggests that the increase in survival is due to the addition of Avastin. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335– Months. Months. Aumento significativo. del tempo a progressione e della sopravvivenza. *Inibitore di topoisomeasi. Hurwitz, et al. NEJM")
34
Bevacizumab nei pazienti in progressione dopo chemioterapia di prima linea con Bevacizumab
Patients with previously untreated, unresectable metastatic CRC (n=1,953) 1st-line Avastin + CTx 1st progression (n=1,445) No treatment (n=253) No Avastin post PD (n=531) Avastin post PD (n=642) 932 deaths (reported as of the January 21, 2007 data cutoff) Median follow-up time 19.6 months Grothey, et al. ASCO 2007
 1st-line Avastin + CTx. 1st progression (n=1,445) No treatment (n=253) No Avastin post PD (n=531) Avastin post PD. (n=642) 932 deaths (reported as of the January 21, 2007 data cutoff) Median follow-up time 19.6 months. Grothey, et al. ASCO")
35
NB: studio retrospettivo osservazionale
Bevacizumab nei pazienti in progressione dopo chemioterapia di prima linea con Bevacizumab Post-progression therapy 1.0 0.8 0.6 0.4 0.2 Avastin post PD (n=642) No Avastin post PD (n=531) No treatment (n=253) Survival estimate Post-progression Avastin HR=0.48 (0.41–0.57) p<0.001 Last updated: June 11, 2007 This slide shows the Kaplan-Meier estimate for median overall survival for the different subgroups of patients with metastatic CRC in the BRiTE study. Data show that median overall survival is superior in patients who received Avastin post progression compared with patients who did not receive Avastin or any other therapy post progression. Similarly, survival beyond first progression was better in patients who received Avastin post progression. These are the first data to show an improvement in overall survival in patients who received first-line Avastin and continued with Avastin-based therapy post progression. BRiTE = Bevacizumab (Avastin) Regimens: Investigation of Treatment Effects and Safety; PD = progressive disease Grothey A, Sugrue M, Hedrick E, et al. Association between exposure to bevacizumab (BV) beyond first progression (BBP) and overall survival (OS) in patients with metastatic colorectal cancer (mCRC): Results from a large observational study (BRiTE). J Clin Oncol 2007;25(June 20 Suppl.):172s (Abstract 4036). 12.6 19.9 31.8 Months NB: studio retrospettivo osservazionale Grothey, et al. ASCO 2007
 No Avastin post PD (n=531) No treatment (n=253) Survival estimate. Post-progression Avastin HR=0.48 (0.41–0.57) p< Last updated: June 11, This slide shows the Kaplan-Meier estimate for median overall survival for the different subgroups of patients with metastatic CRC in the BRiTE study. Data show that median overall survival is superior in patients who received Avastin post progression compared with patients who did not receive Avastin or any other therapy post progression. Similarly, survival beyond first progression was better in patients who received Avastin post progression. These are the first data to show an improvement in overall survival in patients who received first-line Avastin and continued with Avastin-based therapy post progression. BRiTE = Bevacizumab (Avastin) Regimens: Investigation of Treatment Effects and Safety; PD = progressive disease. Grothey A, Sugrue M, Hedrick E, et al. Association between exposure to bevacizumab (BV) beyond first progression (BBP) and overall survival (OS) in patients with metastatic colorectal cancer (mCRC): Results from a large observational study (BRiTE). J Clin Oncol 2007;25(June 20 Suppl.):172s (Abstract 4036) Months. NB: studio retrospettivo osservazionale. Grothey, et al. ASCO")
36
99% increase in median PFS
Bevacizumab + chemio nella terapia di prima linea del carcinoma mammario (Fase III) Avastin + paclitaxel (n=368) 99% increase in median PFS Median PFS (months) 15 10 5 Avastin + paclitaxel Paclitaxel Paclitaxel (n=354) 100 HR=0.48; p<0.0001 80 60 Progression-free survival estimate 40 20 This slide shows median progression-free survival for Avastin plus paclitaxel in trial E2100. The primary analysis of duration of progression-free survival was performed on December 2005, using a cut-off date of 14 April 2005 for progression events.1 This cut-off was used because the results of an earlier analysis (data cut-off 9 February 2005, after approximately 50% of prespecified events) had been reported at the 2005 annual ASCO meeting, revealing that the primary trial endpoint, duration of progression-free survival, had crossed the O’Brien-Fleming boundary in favour of the Avastin plus paclitaxel arm. This had the potential to bias subsequent analyses, due to the open-label nature of this trial.1 At the data cut-off point, 395 progression events or deaths had occurred in the 722 randomised patients (207 in the paclitaxel-alone arm and 188 in the Avastin plus paclitaxel arm).1 A significant increase in median progression-free survival was observed in patients receiving Avastin plus paclitaxel compared with paclitaxel alone (13.3 vs 6.7 months, respectively). The HR for progression was 0.48 (p<0.0001), which corresponds to a two-fold higher chance of patients being progression free.1 These data are not only highly statistically significant, but also clinically meaningful for mBC patients. HR = hazard ratio; mBC = metastatic breast cancer References EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August 2007. 6.7 13.3 Time (months) Raddoppio del tempo di progressione EMEA Avastin Report, 2007
 Avastin + paclitaxel (n=368) 99% increase in median PFS. Median PFS (months) Avastin + paclitaxel. Paclitaxel. Paclitaxel (n=354) 100. HR=0.48; p< Progression-free survival estimate This slide shows median progression-free survival for Avastin plus paclitaxel in trial E2100. The primary analysis of duration of progression-free survival was performed on December 2005, using a cut-off date of 14 April 2005 for progression events.1. This cut-off was used because the results of an earlier analysis (data cut-off 9 February 2005, after approximately 50% of prespecified events) had been reported at the 2005 annual ASCO meeting, revealing that the primary trial endpoint, duration of progression-free survival, had crossed the O’Brien-Fleming boundary in favour of the Avastin plus paclitaxel arm. This had the potential to bias subsequent analyses, due to the open-label nature of this trial.1. At the data cut-off point, 395 progression events or deaths had occurred in the 722 randomised patients (207 in the paclitaxel-alone arm and 188 in the Avastin plus paclitaxel arm).1. A significant increase in median progression-free survival was observed in patients receiving Avastin plus paclitaxel compared with paclitaxel alone (13.3 vs 6.7 months, respectively). The HR for progression was 0.48 (p<0.0001), which corresponds to a two-fold higher chance of patients being progression free.1. These data are not only highly statistically significant, but also clinically meaningful for mBC patients. HR = hazard ratio; mBC = metastatic breast cancer. References. EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August Time (months) Raddoppio del tempo di progressione. EMEA Avastin Report,")
37
Avastin + paclitaxel (n=246)
Bevacizumab + chemio nella terapia di prima linea del carcinoma mammario (Phase III trial) Complete response Partial response 36.2 19.8% p<0.0001 16.4 Overall response rate (%) This slide shows the objective response rate in patients with measurable disease for Avastin plus paclitaxel in trial E2100. The primary analysis population for objective response consisted of all randomised patients with measurable disease at baseline. A cut-off date of 14 April 2005 was used for tumour evaluation.1 Objective response was defined by ECOG as the occurrence of a complete or partial best overall response (according to RECIST), which was confirmed by the investigator on repeat assessment at least 4 weeks after the criteria for response were first met. A significant, more than two-fold, increase in objective response rate (complete response plus partial response) was observed in patients receiving Avastin plus paclitaxel compared with paclitaxel alone (36.2% vs 16.4%, p<0.0001). The rate of complete response more than doubled with the addition of Avastin.1 ECOG = Eastern Cooperative Oncology Group; RECIST = response evaluation criteria in solid tumours Reference EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August 2007. Paclitaxel (n=268) Avastin + paclitaxel (n=246) Raddoppio del tasso di risposta EMEA Avastin Report, 2007
 Complete response. Partial response % p< Overall response rate (%) This slide shows the objective response rate in patients with measurable disease for Avastin plus paclitaxel in trial E2100. The primary analysis population for objective response consisted of all randomised patients with measurable disease at baseline. A cut-off date of 14 April 2005 was used for tumour evaluation.1. Objective response was defined by ECOG as the occurrence of a complete or partial best overall response (according to RECIST), which was confirmed by the investigator on repeat assessment at least 4 weeks after the criteria for response were first met. A significant, more than two-fold, increase in objective response rate (complete response plus partial response) was observed in patients receiving Avastin plus paclitaxel compared with paclitaxel alone (36.2% vs 16.4%, p<0.0001). The rate of complete response more than doubled with the addition of Avastin.1. ECOG = Eastern Cooperative Oncology Group; RECIST = response evaluation criteria in solid tumours. Reference. EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August Paclitaxel (n=268) Avastin + paclitaxel (n=246) Raddoppio del tasso di risposta. EMEA Avastin Report,")
38
Bevacizumab nel carcinoma del polmone (PFS)
1.0 0.8 0.6 0.4 0.2 CP + Bevacizumab CP HR=0.66 (0.57–0.77) p<0.001 Probability Last updated: March 23, 2007 The Kaplan-Meier curve shown here demonstrates the effect of adding Avastin to carboplatin/paclitaxel on progression-free survival.1 Median progression-free survival was significantly increased in patients receiving Avastin plus CP compared with CP alone (6.2 months vs 4.5 months). The HR for progression was 0.66 (p<0.001). NSCLC = non-small cell lung cancer; HR = hazard ratio; CP = carboplatin/paclitaxel Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med 2006;355:2542–50. 4.5 6.2 Time (months) Sandler, et al. NEJM 2006 “En España pendiente de autorización de precio y condiciones de reembolso”
 p< Probability. Last updated: March 23, The Kaplan-Meier curve shown here demonstrates the effect of adding Avastin to carboplatin/paclitaxel on progression-free survival.1. Median progression-free survival was significantly increased in patients receiving Avastin plus CP compared with CP alone (6.2 months vs 4.5 months). The HR for progression was 0.66 (p<0.001). NSCLC = non-small cell lung cancer; HR = hazard ratio; CP = carboplatin/paclitaxel. Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med 2006;355:2542– Time (months) Sandler, et al. NEJM En España pendiente de autorización de precio y condiciones de reembolso")
39
Tossicità di Bevacizumab in associazione alla chemioterapia
Less frequently reported events: congestive heart failure (CHF)/cardiomyopathy arterial thromboembolism (ATE) venous thromboembolism (VTE) wound-healing complications gastrointestinal perforations Commonly reported events: hypertension proteinuria bleeding/haemorrhage Typical chemotherapy-associated side effects: Neuropathy,neutropenia,fatigue This slide lists the adverse events that have been consistently reported in clinical trials when Avastin is added to chemotherapy. The most commonly reported events (of any grade) that are reported in Avastin clinical trials are hypertension, proteinuria and bleeding/haemorrhage. Other events that are reported less frequently are CHF/cardiomyopathy, ATE, VTE, wound-healing complications and gastrointestinal perforations. The incidence of certain adverse events that are associated with cytotoxic chemotherapy agents has been increased by the addition of Avastin to these agents. These include neuropathy, neutropenia and fatigue. In phase III mBC trial E2100, it is suggested that this increase is due to longer exposure of patients in the combination arm to paclitaxel, as time to progression was significantly increased in this arm.1 CHF = congestive heart failure; ATE = arterial thromboembolic event; VTE = venous thromboembolic event Reference EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August 2007.
/cardiomyopathy. arterial thromboembolism (ATE) venous thromboembolism (VTE) wound-healing complications. gastrointestinal perforations. Commonly reported events: hypertension. proteinuria. bleeding/haemorrhage. Typical chemotherapy-associated side effects: Neuropathy,neutropenia,fatigue. This slide lists the adverse events that have been consistently reported in clinical trials when Avastin is added to chemotherapy. The most commonly reported events (of any grade) that are reported in Avastin clinical trials are hypertension, proteinuria and bleeding/haemorrhage. Other events that are reported less frequently are CHF/cardiomyopathy, ATE, VTE, wound-healing complications and gastrointestinal perforations. The incidence of certain adverse events that are associated with cytotoxic chemotherapy agents has been increased by the addition of Avastin to these agents. These include neuropathy, neutropenia and fatigue. In phase III mBC trial E2100, it is suggested that this increase is due to longer exposure of patients in the combination arm to paclitaxel, as time to progression was significantly increased in this arm.1. CHF = congestive heart failure; ATE = arterial thromboembolic event; VTE = venous thromboembolic event. Reference. EMEA Avastin European Public Assessment Report, Available at: Accessed 16 August")
40
Bevacizumab + IFN nel carcinoma del rene metastatico
IFNα + BEVACIZUMAB N=289 N= 306 Overall Response Rate 13% 31% Median Duration of Response 11 mos 13 mos Median Duration of Stable Disease 7 mos 10 mos Escudier B. ASCO 2007 abs.3

41
Bevacizumab + IFN nel carcinoma del rene metastatico
significativo aumento, delle Risposte obbiettive e della PFS Solo in pazienti a rischio basso o intermedio, non in quelli ad alto rischio Con un trend all’aumento della sopravvivenza ben tollerato: non tossicità diverse da quelle attese con IFN e bevacizumab da soli manca il braccio con bevacizumab da solo Escudier B ASCO 2007 abs.3 Bukowski RJ, ASCO 2007 Plenary S.

42
EGFR signaling in tumor development
The concept targeted therapy for a broad range of common solid tumors Clinical trials proof of concept well tolerated therapy tumor responses in several tumor types The promise improved outcomes in the treatment of common solid tumors EGFR R R T cell Mb. K Small mol. K K Tumor response Razionale per l’utilizzo di Iressa nei tumori solidi che overesprimono EGFR. Allo stato attuale vi sono studi di combinazione con chemioterapia nel polmone e carcinoma del colon e studi in monoterapia in diverse neoplasie solide. Infine sono in corso di valutazioni combinazioni con ormonoterapia e radioterapia nel carcinoma dell amammella e della prostata. metastasis invasion Inibition of apoptosis angiogenesis proliferation

43
2. INIBITORI DELLA TRASMISSIONE DEL SEGNALE (SMALL MOLECULES)
Gefitinib (IRESSA) Erlotinib (TARCEVA) Imatinib (GLIVEC) Sunitinib (SUTENT) Sorafenib (NEXAVAR)
 Erlotinib (TARCEVA) Imatinib (GLIVEC) Sunitinib (SUTENT) Sorafenib (NEXAVAR)")
44
(Iressa Dose Evaluation in Advanced Lung cancer)
STUDI IDEAL 1 e IDEAL 2 (Iressa Dose Evaluation in Advanced Lung cancer) FASE II RANDOMIZZATI Ideal 1* Ideal 2** (Oct/ Jan/2001) (Nov/ Apr/2001) 250 mg/die mg/die 250 mg/die mg/die N° Pazienti % di paz. > 1 linea CT Tasso di Risposta (%) Controllo di malattia (risposte + stabilità) (%) Sopravv. mediana (mesi) Progr. Free Surv. (mesi) Miglioramento sintomi (%) * JCO 2003: 21: ** JAMA 2003; 290:
 FASE II RANDOMIZZATI. Ideal 1* Ideal 2** (Oct/ Jan/2001) (Nov/ Apr/2001) 250 mg/die 500 mg/die 250 mg/die 500 mg/die. N° Pazienti % di paz. > 1 linea CT Tasso di Risposta (%) Controllo di malattia. (risposte + stabilità) (%) Sopravv. mediana (mesi) Progr. Free Surv. (mesi) Miglioramento sintomi (%) * JCO 2003: 21: ** JAMA 2003; 290:")
45
ERLOTINIB * 150 mg daily Placebo “150 mg” daily
A randomized placebo-controlled trial of erlotinib in patients with advanced NSCLC 731 stage IIIB-IV NSCLC Nov/01 – Feb/03 Stratified by: Centre PS, 0/1 vs 2/3 Response to prior Rx (CR/PR:SD:PD) Prior regimens, (1 vs 2) Prior platinum, /Yes vs no) ERLOTINIB * 150 mg daily R A N D O M Placebo “150 mg” daily * 2:1Randomization 1° endpoint: Survival 2° endpoints: PFS, RR, Tox., Q.o.L.
 Prior regimens, (1 vs 2) Prior platinum, /Yes vs no) ERLOTINIB * 150 mg daily. R. A. N. D. O. M. Placebo. 150 mg daily. * 2:1Randomization. 1° endpoint: Survival. 2° endpoints: PFS, RR, Tox., Q.o.L.")
46
A randomized placebo-controlled trial of Erlotinib
in patients with advanced NSCLC

47
A randomized placebo-controlled trial of erlotinib
in patients with advanced NSCLC

48
IMATINIB (Glivec) nella leucemia mieloide cronica (LMC)
Prima identificazione nel1990 Sintesi nel 1992: Inibizione selettiva di alcune Tirosina-Kinasi (BCR-ABL, KIT, PDGFR) Dimostrazione di attività in vivo nel 1996 (topi BCR-ABL transgenici) Primo paziente con LMC trattato: 1998 Approvazione FDA nella LMC nel 2001
 Dimostrazione di attività in vivo nel (topi BCR-ABL transgenici) Primo paziente con LMC trattato: Approvazione FDA nella LMC nel")
49
IMATINIB NELLA LMC 532 PAZ RESISTENTI AD INTERFERONE
RISPOSTE OBIETTIVE: >90% REMISSIONI COMPLETE: 28% (citogenetica) PROGRESSIONI: 3% VIVI AD 1 ANNO: 73% Risultati notevoli B. Druker, ASCO 2001 Ed. Book: 419
 PROGRESSIONI: 3% VIVI AD 1 ANNO: 73% Risultati notevoli. B. Druker, ASCO 2001 Ed. Book: 419.")
50
IMATINIB nei Tumori Stromali GastroIntestinali (GIST)
2001: apoptosi in linee cellulari di GIST 2001: pubblicazione su NEJM del primo pz. con GIST, trattato con Glivec 2001: NIH GIST Workshop Febbraio 2002: approvazione FDA di Glivec per trattamento dei GIST

51
Imatinib triplica la sopravvivenza dei pazienti con GIST

52
Indicazioni Attuali e Potenziali per Glivec
BCR-ABL positive leukemias KIT expressing tumors: Gastro-intestinal stromal tumors (GIST) Small cell lung cancer Systemic mastocytosis, neuroblastoma PDGF-R expressing tumors: Soft Tissue Sarcomas, Gliomas Ovarian, breast, GI tract, Prostate cancer Chronic Myelomoncytic Leukemia
 Small cell lung cancer. Systemic mastocytosis, neuroblastoma. PDGF-R expressing tumors: Soft Tissue Sarcomas, Gliomas. Ovarian, breast, GI tract, Prostate cancer. Chronic Myelomoncytic Leukemia.")
53
Resistenza a Glivec Si sviluppa nella maggior parte dei pazienti entro 18 to 26 mesi Deriva da mutazioni aggiuntive nelle diverse KIT or PDGFR A kinasi Richiede nuovi farmaci con target specifico, per riportare la malattia sotto controllo

54
Sunitinib (Sutent): approccio multitarget
Inibisce l’attività di molte vie metaboliche regolate dalle Tirosina Kinasi di diversi fattori di crescita presenti su cellule tumorali: FLT-3, KIT, and CSF-1R su cellule endoteliali and periciti: VEGF and PDGF Con il risultato di bloccare i recettori Tirosina Kinasi su entrambe, ottenendo la regressione del tumore

55
Sunitinib nei GIST resistenti a Imatinib

56
Sunitinib: approccio multitarget
Attività dimostrata in: GIST Carcinoma del rene Carcinoma della mammella Tumori Neuroendocrini Rappresenta un vero approccio multitarget nella terapia dei tumori

57
Sunitinib nel carcinoma del rene
Investigator Assessment Independent Central Review Sunitinib (n=374) IFN-a (n=373) Sunitinib (n=365) IFN-a (n=346) Response (RECIST) % Objective response* 46 12 39% 8% Complete response 1 Partial response 45 11 39 8 Stable disease 41 55 40% 48% PD or Not evaluable 13 33 21 44 *Sunitinib vs IFN-a: P< Motzer R. ASCO 2007
 IFN-a (n=373) Sunitinib (n=365) IFN-a (n=346) Response (RECIST) % Objective response* % 8% Complete response. 1. Partial response Stable disease % 48% PD or Not evaluable *Sunitinib vs IFN-a: P< Motzer R. ASCO")
58
Sunitinib. Progression-free survival
(Independent Central Review) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Time (Months) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Progression Free Survival Probability Sunitinib Median: 11 months (95% CI: 10–12) IFN- Median: 5 months (95% CI: 4–6) Hazard Ratio = 0.415 (95% CI: 0.320–0.539) P < No. at Risk Sunitinib: No. at Risk IFN-:
 Time (Months) Progression Free Survival Probability. Sunitinib. Median: 11 months. (95% CI: 10–12) IFN- Median: 5 months. (95% CI: 4–6) Hazard Ratio = (95% CI: 0.320–0.539) P < No. at Risk Sunitinib: No. at Risk IFN-:")
59
Sunitinib. Overall Survival (Trend to …)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Time (Months) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Overall Survival Probability Sunitinib (n=375) Median not reached IFN- (N=375) Hazard Ratio = 0.65 (95% CI: 0.449–0.942) P = * Sunitinib IFN- No. at Risk Sunitinib: No. at Risk IFN-: *The observed p-value did not meet the pre-specified level of significance for this interim analysis
 Overall Survival Probability. Sunitinib (n=375) Median not reached. IFN- (N=375) Hazard Ratio = (95% CI: 0.449–0.942) P = * Sunitinib. IFN- No. at Risk Sunitinib: No. at Risk IFN-: *The observed p-value did not meet the pre-specified level of significance for this interim analysis.")
60
Sorafenib (BAY ) inhibits Raf-1, una serina/treonina kinasi, membro – della via metabolica RAF/MEK/ERK Attivo anche contro β-Raf e altri recettori tirosina kinasi (VEGFR-2, PDGFR, FLT3, c-KIT) Randomized Phase III Trial of Sorafenib in patients with IFN/IL-2 refractory, advanced RCC [slide 80] Study Design Disease status was assessed at 12 weeks using modified WHO criteria based on change in bidimensional tumor measurements Patients with a change in tumor size of <25 percent were entered into the randomized phase of the trial Patients with progressive disease (>=25 percent tumor growth or clinically assessed progression) were discontinued Patients with >=25 percent tumor shrinkage continued to receive sorafenib open label until disease progression or toxicity Placebo patients who progressed could cross over to sorafenib Escudier B, et al. NEJM 2007
 Randomized Phase III Trial of Sorafenib in patients with IFN/IL-2 refractory, advanced RCC. [slide 80] Study Design. Disease status was assessed at 12 weeks using modified WHO criteria based on change in bidimensional tumor measurements. Patients with a change in tumor size of <25 percent were entered into the randomized phase of the trial. Patients with progressive disease (>=25 percent tumor growth or clinically assessed progression) were discontinued. Patients with >=25 percent tumor shrinkage continued to receive sorafenib open label until disease progression or toxicity. Placebo patients who progressed could cross over to sorafenib. Escudier B, et al. NEJM")
61
80% Objective Response by independent review
Best RR (RECIST) Sorafenib (n=335)* Placebo (n=337)* PR ( 2%) ( 0%) SD (78%) (55%) PD ( 9%) (30%) Missing (11%) (15%) 80% Maximum percent reduction in Tumor Measurement* Placebo Sorafenib Maximum Percent Reduction in Tumor Measurement *Independently assessed measurements available for 574 patients
 Sorafenib (n=335)* Placebo (n=337)* PR 7 ( 2%) 0 ( 0%) SD 261 (78%) 186 (55%) PD 29 ( 9%) 102 (30%) Missing 38 (11%) 49 (15%) 80% Maximum percent reduction in Tumor Measurement* Placebo. Sorafenib. Maximum Percent Reduction in Tumor Measurement. *Independently assessed measurements available for 574 patients.")
62
ASCO 2007

63
Inibitori Tirosina Chinasi: tossicità
Di solito modesta e ben gestibile Prevalentemente a carico delle strutture epiteliali di rivestimento (rash cutaneo) o intestinali (diarrea) Possibili ma poco frequenti, astenia, problemi cardiocircolatori (ipertensione/ipotensione) o metabolici
 o intestinali (diarrea) Possibili ma poco frequenti, astenia, problemi cardiocircolatori (ipertensione/ipotensione) o metabolici.")
64
Benefici delle terapie target
Elevati tassi di risposta in combinazione con chemio Aumento significativo della sopravvivenza libera da progressione Aumento della sopravvivenza (alcuni). Atkins MB et al, Clin Cancer Res Jan 15;13, 667s-670s, Sosman JA et al,Clin Cancer Res Jan 15;13:764s-769s
. Atkins MB et al, Clin Cancer Res Jan 15;13, 667s-670s, Sosman JA et al,Clin Cancer Res Jan 15;13:764s-769s.")
65
Limiti delle terapie target
Risposte complete rare o assenti Necessaria una somministrazione a lungo termine: rapida progressione con l’interruzione del trattamento Tutti i pazienti alla fine sviluppano resistenza (entro 6-12 mesi) Atkins MB et al, Clin Cancer Res Jan 15;13, 667s-670s, Sosman JA et al,Clin Cancer Res Jan 15;13:764s-769s
 Atkins MB et al, Clin Cancer Res Jan 15;13, 667s-670s, Sosman JA et al,Clin Cancer Res Jan 15;13:764s-769s.")
66
Limiti delle terapie target
Costi estremamente elevati: Necessità di più precisa identificazione dei pazienti responsivi “Target the target Target the network in the right host”

67
Terapie immunologiche a bersaglio noto (Antigeni specifici)
Attive (vaccinazioni) Passive o adottive (Anticorpi, linfociti, cellule dendritiche)
 Passive o adottive (Anticorpi, linfociti, cellule dendritiche)")
68
Vaccination of breast cancer patients with Her2/neu E75 peptide (Peoples et al. Clin Cancer Res 2008) LN+ vs. LN- pre-treated, high-risk HLA-A2,-A3 patients received E75+GM-CSF. Recurrence rate: 5.6% in vaccinated group (N=101) vs. 14% in controls (N=85) (P=0.04) at 24 mos follow-up. Association with the T cell response (mean frequency of specific T cells increased from 0.39 % at baseline to 1.8 % post-vax).
 vs. 14% in controls (N=85) (P=0.04) at 24 mos follow-up. Association with the T cell response (mean frequency of specific T cells increased from 0.39 % at baseline to 1.8 % post-vax).")
69
Phase III study of gp100 peptide vaccine in melanoma
A phase III multi-institutional randomized study of immunization with the gp100 (210M) peptide followed by high-dose of IL-2 compared with high dose IL-2 alone in patients with metastatic melanoma. Schwartzentruber DJ, Lawson D, Richards J, Conry RM, Miller D, Triesman J, Gailani F, Riley LB, Vena D, Hwu P ASCO 2009
 peptide followed by high-dose of IL-2 compared with high dose IL-2 alone in patients with metastatic melanoma. Schwartzentruber DJ, Lawson D, Richards J, Conry RM, Miller D, Triesman J, Gailani F, Riley LB, Vena D, Hwu P. ASCO")
70
Phase III study of gp100 peptide vaccine
21 centers; total of 185 patients Stage IV or locally advanced stage III, HLA-A*0201 Therapy. IL-2: 720’000IU/kg/dose+/- Gp100 (210M) peptide+Montanide Results. High toxicity (IL-2); RR 22.1% vs. 9.7% (P=0.0223); PFS: 2.9 vs. 1.6 mos (P=0.010); Median OS: 17.6 vs mos (P=0.096)
 peptide+Montanide. Results. High toxicity (IL-2); RR 22.1% vs. 9.7% (P=0.0223); PFS: 2.9 vs. 1.6 mos (P=0.010); Median OS: 17.6 vs mos (P=0.096)")
71
IMMUNOTERAPIA ADOTTIVA

72
Terapia linfoablativa e TIL (Rosenberg SA, 2005)
")
73
50 patients with IL-2-unresponsive melanoma
Adoptive immunotherapy of advanced melanoma: Toxicity and clinical response 50 patients with IL-2-unresponsive melanoma Generation of TILs 81% Response rate (CR+PR) 51–72% (chemo-TBI myelodepletion) Mean response duration 11.5 months Sites of response Lung, liver, LN, skin, subcute, brain Response to a second treatment 47% (8/17) Problems: Toxicity Overall survival Dudley et al. J Clin Oncol 2005/2008.
 51–72% (chemo-TBI myelodepletion) Mean response duration months. Sites of response. Lung, liver, LN, skin, subcute, brain. Response to a second treatment. 47% (8/17) Problems: Toxicity. Overall survival. Dudley et al. J Clin Oncol 2005/2008.")
74
REQUISITI PER IL SUCCESSO DELL’INFUSIONE DEI CTLs
Alte dosi di linfociti T espansi ex-vivo: 6.3x1010 CD3+ ( ) Chemio- o radio-terapia (TBI) immunosoppressiva Persistenza e proliferazione dei linfociti in-vivo essenziali per l’attività antitumorale IL-2 in-vivo dopo re-infusione dei linfociti T
 Chemio- o radio-terapia (TBI) immunosoppressiva. Persistenza e proliferazione dei linfociti in-vivo essenziali per l’attività antitumorale. IL-2 in-vivo dopo re-infusione dei linfociti T.")
76
I nuovi approcci di immunoterapia adottiva sono promettenti ma ancora troppo associati a importanti effetti collaterali

77
FINE

78
Uguale aumento della sopravvivenza nei pazienti con risposta e con malattia stabile

79
Capecitabina Lapatinib nel carcinoma della mammella metastatico: attività
HER2+ MBC refractory to anthracycline, taxane, and/or trastuzumab Lapatinib + Addition of lapatinib to capecitabine in women with treatment-refractory MBC associated with Longer time to progression 36.9 vs 19.7 wks (P= ) Longer progression-free survival 36.9 vs 17.9 wks (P= ) Fewer progressions or deaths 38% vs 48% Response (independent review) Overall: 22.5% vs 14.3% (P=0.113) Capecitabine Progression-Free Survival (%) 100 80 60 40 ITT, intent to treat 20 10 20 30 40 50 Time (Wks) ITT population C. Geyer. Oral presentation at 42nd Annual Meeting of ASCO, Atlanta, GA, June 2-6, 2006.
 Longer progression-free survival vs 17.9 wks (P= ) Fewer progressions or deaths. 38% vs 48% Response (independent review) Overall: 22.5% vs 14.3% (P=0.113) Capecitabine. Progression-Free Survival (%) ITT, intent to treat Time (Wks) ITT population. C. Geyer. Oral presentation at 42nd Annual Meeting of ASCO, Atlanta, GA, June 2-6,")
80
Volume 343:750-758 September 14, 2000 Number 11
September 14, 2000 Number 11 REGRESSION OF METASTATIC RENAL-CELL CARCINOMA AFTER NONMYELOABLATIVE ALLOGENEIC PERIPHERAL-BLOOD STEM-CELL TRANSPLANTATION Richard Childs, M.D., Allen Chernoff, M.D., Nathalie Contentin, M.D., Erkut Bahceci, M.D., David Schrump, M.D., Susan Leitman, M.D., Elizabeth J. Read, M.D., John Tisdale, M.D., Cynthia Dunbar, M.D., W. Marston Linehan, M.D., Neal S. Young, M.D., and A. John Barrett, M.D.

86
Recettori diversi

87
I Recettori per EGF EGFR Tumor cell membrane Tumor response invasion
K K K Tumor response Razionale per l’utilizzo di Iressa nei tumori solidi che overesprimono EGFR. Allo stato attuale vi sono studi di combinazione con chemioterapia nel polmone e carcinoma del colon e studi in monoterapia in diverse neoplasie solide. Infine sono in corso di valutazioni combinazioni con ormonoterapia e radioterapia nel carcinoma dell amammella e della prostata. metastasis invasion Inibition of apoptosis angiogenesis proliferation

Presentazioni simili




















>")

>")
