Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
I Disturbi d’Ansia nel DSM IV-TR e nell’ICD 10: nuove prospettive di ricerca
E. Aguglia

2
'Uno degli uomini più in vista della città mi raccontava che aveva redatto una lista dei cinquanta avvenimenti che aveva più temuto accadessero negli ultimi 10 anni...... ......ebbene aveva concluso che sinora nessuno di questi si era verificato, ma il pensiero lo aveva fatto star male come se realmente fossero accaduti.....' Shader, 1989

3
“ Gli stessi sintomi possono essere incontrati in stati patologici diversi, ma quello che importa non sono i singoli sintomi in sé, ma lo stato mentale che li condiziona” Minkowski,1937 Il problema della diagnosi in psichiatria tra approccio dimensionale e categoriale

4
Prevalence of anxiety and other psychiatric disorders.

5
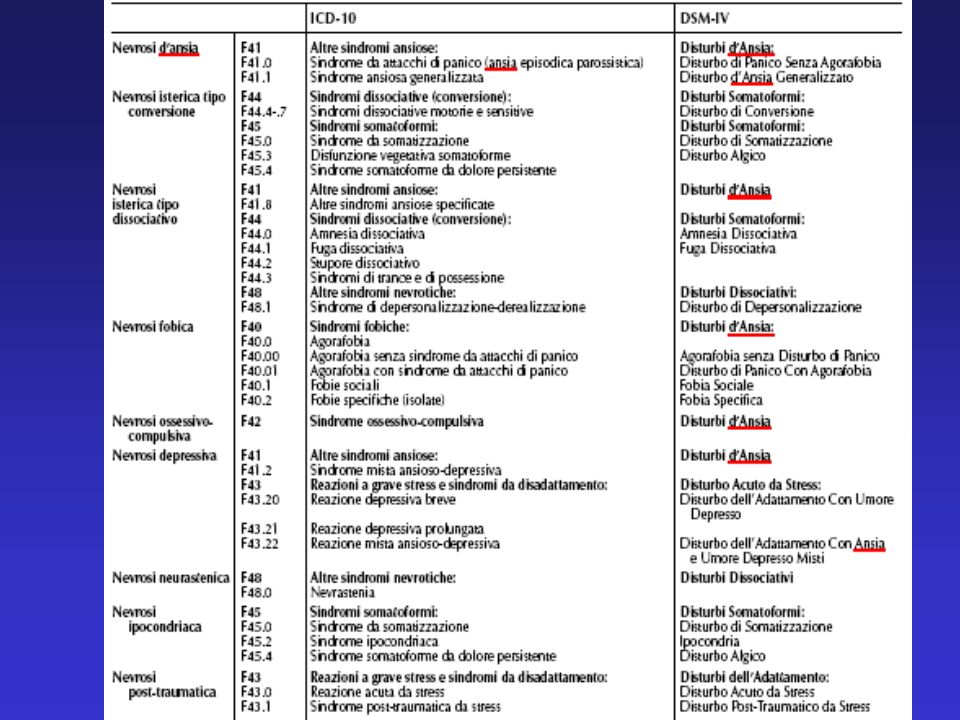
Dalle nevrosi… alla classificazione categoriale

7
The classification of anxiety disorders in ICD-10 and DSM-IV: a concordance analysis
On the surface, the classifications of anxiety disorders in DSM-IV and ICD-10 appear quite similar. However, differences exist and are evident in four aspects of the diagnostic criteria: typology, identifying criteria, inclusion and exclusion criteria. The concordance between the current classifications would be improved with the removal of the criterion for uncontrollability from DSM-IV, a closer focus on the symptoms of hypervigilance and scanning as in DSM-IV and the removal of the clinical significance criterion from DSM-IV. Equivalency of the exclusion criteria between the two classification systems reduces the concordance, demonstrating that each classification systems is a set of interdependent diagnoses and to ultimately achieve concordance, all diagnoses must be considered together. Andrews G et al. Psychopathology Mar-Jun;35(2-3):100-6
:")
8
Ansia: vantaggi della classificazione categoriale
Rassicurazione per lo psichiatra: quanto maggiore è il numero delle categorie diagnostiche e quanto più è dettagliata la descrizione dei caratteri specifici di ogni singola categoria, tanto più facile sembra essere la possibilità di inquadramento di ogni singolo caso. L’ ansia non è più un sintomo o uno “stato”, ma diventa uno spettro di disturbi, di entità nosografiche precise al limite di “malattie”.

9
Comunicazione più semplice: identificare e descrivere cluster sintomatologici precisi significa trovare concordanza di riferimento tra psichiatri di diversa formazione e cultura. In effetti i termini e le categorie utilizzati in passato (nevrosi d’ansia, stati d’ ansia) per la loro aspecificità e genericità, favorivano una diversità di linguaggi e di definizioni
 per la loro aspecificità e genericità, favorivano una diversità di linguaggi e di definizioni.")
10
Ricerca: la creazione di categorie diagnostiche basate sulla covarianza sindromica nell’ambito allargato del fenomeno ansia, ha permesso di indirizzare la ricerca psico biologica verso l’identificazione di meccanismi fisiopatologici specifici destinati a confermare o a disconfermare la validità delle singole categorie

11
Ansia: limiti della classificazione categoriale
Bassa stabilità diagnostica nel tempo Sovrapposizione di criteri Elevata frequenza di diagnosi in comorbidità Incertezza nella diagnosi di confine tra le categorie Scarsi risultati nella ricerca di markers biologici specifici Procedimento diagnostico inferenziale Difficoltà a tradurre in quadri categoriali alcuni vissuti psicopatologici (preoccupazione invasiva, irrequietezza psichica immotivata) Problema dell’ansia sottosoglia
 Problema dell’ansia sottosoglia.")
12
L’ordinamento nel DSM-IV TR dei disturbi d’ansia, si presta inoltre ad alcune osservazioni:
Lo stesso piano nosografico comprende condizioni di ansia primaria (ad esempio il DAG) e condizioni di ansia secondaria (ad esempio il disturbo d’ansia da assunzione di sostanze). Problema di eventuale classificazione separata dei due gruppi Principi organizzatori di tipo eterogeneo vengono utilizzati nell’identificare le categorie diagnostiche. In alcuni casi il principio è causale ( ad es. nel disturbo acuto da stress), in altri casi è basato sul contenuto (ad es. nella fobia sociale), in altri casi ancora è sindromico (ad es. nel disturbo da panico)
 e condizioni di ansia secondaria (ad esempio il disturbo d’ansia da assunzione di sostanze). Problema di eventuale classificazione separata dei due gruppi. Principi organizzatori di tipo eterogeneo vengono utilizzati nell’identificare le categorie diagnostiche. In alcuni casi il principio è causale ( ad es. nel disturbo acuto da stress), in altri casi è basato sul contenuto (ad es. nella fobia sociale), in altri casi ancora è sindromico (ad es. nel disturbo da panico)")
13
Il DSM non sembra poi risolvere adeguatamente il difficile problema dell’inquadramento dell’ansia libera o generalizzata in tutte le sue manifestazioni di fenomeno sintomatico o categoriale, sindromico o sub-sindromico, dipendente o indipendente L’ eterogeneità nosografica, dunque, fa sì che le singole categorie non abbiano, nella maggior parte dei casi, un supporto patofisiologico specifico, né un’adeguata specificità terapeutica

14
DAP DOC PTSD DAG Timore paura Specificità patogenetica
Specificità terapeutica Collocazione nosografica DAP Secondaria Probabile Autonoma? Agorafobia Primaria Incerta Possibile Disturbo d’ansia Fobia specifica Fobia sociale Primaria Incerta Possibile Disturbo d’ansia DOC Secondaria Probabile Autonoma? PTSD DAG Modif. da Pancheri 2005

15
Il problema dell’ansia libera o generalizzata
Il sintomo ansia si accompagna a molti disturbi in Asse I e costituisce manifestazione di molte patologie somatiche. In alcuni casi il sintomo può assumere la dignità categoriale del DAG, ma la sua indipendenza del disturbo in Asse I “primario” non è sempre facilmente valutabile . Inoltre, l’ansia inquadrata come DAG potrebbe rappresentare una semplice esacerbazione temporanea di una condizione di personalità e di temperamento meglio classificabile in Asse II secondo i criteri multiassiali del DSM-IV che, nella classificazione dei disturbi di personalità non prevede, contrariamente ad ogni evidenza clinica, l’esistenza di un “disturbo ansioso di personalità”

16
Il concetto di spettro Un approccio in grado di ovviare ad alcuni dei limiti osservati è rappresentato dal modello di spettro. Lo spettro panico-agorafobico ad esempio (secondo il modello proposto da Cassano e coll.) è un continuum dimensionale che comprende, oltre ai sintomi e ai segni della diagnosi categoriale DSM, anche elementi trascurati nella diagnosi tradizionale: -segni e sintomi sottosoglia -tratti temperamentali e di personalità -sintomi prodromici e residui
 è un continuum dimensionale che comprende, oltre ai sintomi e ai segni della diagnosi categoriale DSM, anche elementi trascurati nella diagnosi tradizionale: -segni e sintomi sottosoglia. -tratti temperamentali e di personalità. -sintomi prodromici e residui.")
17
Il panico complesso Sempre all’interno del concetto di spettro,ad esempio, sono state proposte entità sindromiche complesse ( complex panic) come DAP-GAD o DAP-RBA (ansia breve ricorrente) accomunate da alcune caratteristiche: maggiore gravità sul piano clinico esordio più precoce frequente comorbidità con agorafobia, fobia sociale, depressione, abuso di BDZ e alcol maggior rischio suicidario elevata cronicità Angst, 2002
 come DAP-GAD o DAP-RBA (ansia breve ricorrente) accomunate da alcune caratteristiche: maggiore gravità sul piano clinico. esordio più precoce. frequente comorbidità con agorafobia, fobia sociale, depressione, abuso di BDZ e alcol. maggior rischio suicidario. elevata cronicità. Angst,")
18
Il continuum sintomatologico
“ La variazione tra una condizione con sintomi estesi e disabilitanti e la mancanza quasi totale di sintomi appare essere continua, senza una dimostrabile zona di rarità. Di conseguenza, il confine tra normalità e disturbo mentale deve essere deciso arbitrariamente su basi pragmatiche.” Kendell e Jablensky, 2003

19
Diagnosi di confine E’ stata proposta nell’appendice B del DSM-IV TR la categoria del Disturbo Ansioso-Depressivo misto per indicare tutti quei casi caratterizzati dalla presenza di sintomi depressivi e ansiosi che: Non soddisfano i criteri per ognuno di queste due categorie ma causano una compromissione del funzionamento sociale e lavorativo Richiedono un trattamento farmacologico

20
Il concetto di disturbo ansioso-depressivo: conservazione o innovazione clinico terapeutica ?
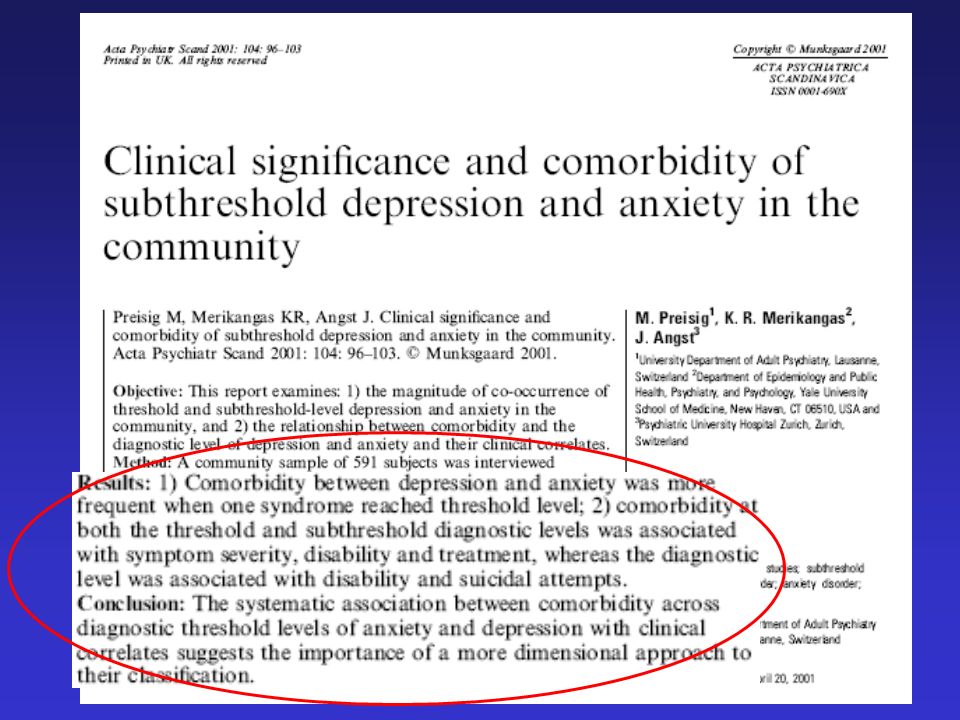
Il razionale che è alla base del nuovo concetto di sindrome ansioso-depressiva è che Il DSM-IV ha proposto nei criteri di ricerca il Disturbo Ansioso-Depressivo Misto (MAD) come un’entità nosologica a sé stante caratterizzata dalla presenza di sintomi ansiosi o depressivi che per durata o numero non soddisfano i criteri di un Disturbo dell’Umore o di un Disturbo d’Ansia. Le manifestazioni dell’ansia o della depressione si esprimono più frequentemente a livello «sottosoglia» (la prevalenza del Disturbo Ansioso Depressivo Misto è dello 0,8%, quella della depressione subsindromica è del 2,4%, mentre quella dell’ansia subsindromica è del 21,9%, Wittchen e Essau, 1993) che non come sindrome conclamata. Tali sintomi «sottosoglia» costituiscono un’area di vasto interesse per la loro fluttuazione nel tempo e per il fatto che in particolari condizioni (es. eventi di vita stressanti) possono aggravarsi e, più elevati costi sociali e minore risposta al trattamento (Zajecka e Ross, 1998)… A.C. Altamura et al. 2001
 come un’entità nosologica a sé stante caratterizzata dalla presenza di sintomi ansiosi o depressivi che per durata o numero non soddisfano i criteri di un Disturbo dell’Umore o di un Disturbo d’Ansia. Le manifestazioni dell’ansia o della depressione si esprimono più frequentemente a livello «sottosoglia» (la prevalenza del Disturbo Ansioso Depressivo Misto è dello 0,8%, quella della depressione subsindromica è del 2,4%, mentre quella dell’ansia subsindromica è del 21,9%, Wittchen e Essau, 1993) che non come sindrome conclamata. Tali sintomi «sottosoglia» costituiscono un’area di vasto interesse per la loro fluttuazione nel tempo e per il fatto che in particolari condizioni (es. eventi di vita stressanti) possono aggravarsi e, più elevati costi sociali e minore risposta al trattamento (Zajecka e Ross, 1998)… A.C. Altamura et al")
21
The ICD-10 criteria have to be specified more exactly.
Mixed anxiety-depression in a 1 year follow-up study: shift to other diagnoses or remission? In 1992, the ICD-10 introduced the concept of mixed anxiety-depression disorder (MAD)… … MAD cannot be seen as a stable diagnosis: most of MAD patients remit; many of them shift to other diagnoses than depression or anxiety. The ICD-10 criteria have to be specified more exactly. Barkow K et al. J Affect Disord Apr;79(1-3):235-9
… … MAD cannot be seen as a stable diagnosis: most of MAD patients remit; many of them shift to other diagnoses than depression or anxiety. The ICD-10 criteria have to be specified more exactly. Barkow K et al. J Affect Disord Apr;79(1-3):")
22
Il problema della comorbidità
Nell’Australian National Survey of Mental Health and WellBeing, il 21% delle persone con una diagnosi DSMIV di un qualunque disturbo mentale soddisfaceva anche i criteri per almeno tre altri disturbi mentali. Andrews et al., 2002

23
Depressione e ansia: tra geni e ambiente
Sviluppo Fattori genetici Fattori ambientali Geni di vulnerabilità e resistenza Supporto sociale Vulnerabilità / Plasticità fenotipica Interventi psichiatrici Traumi Disfunzioni endocrine Malattie somatiche Sintomi ansiosi Depressione Adattato da: Plotsky PM, et al. Psychiatr Clin North Am. 1998;21:

24
Comorbidità tra ansia e depressione prevalenza puntuale
Disturbo depressivo in atto 11.7% Disturbo d’ansia in atto 10.2% 5.6% 4.6% 7.1% A study by the World Health Organization (WHO) – the Collaborative Study on Psychological Problems in General Health Care – has investigated the form and frequency of psychiatric disorders in primary care patients in 14 different countries. Comorbidity was common, with the overlap between anxiety and depressive episodes being particularly great. Indeed, the proportion of those with a current anxiety disorder who also had a current depressive disorder was reported to be approximately 45%. Likewise, the proportion of those with a current depressive disorder who also had a current anxiety disorder was reported to be approximately 40%. The study also showed that the association between depression and anxiety disorders was stronger than between the anxiety disorders themselves. Lecrubier Y. The impact of comorbidity on the treatment of panic disorder. J Clin Psychiatry 1998; 59 (Suppl 8): Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 8):
 – the Collaborative Study on Psychological Problems in General Health Care – has investigated the form and frequency of psychiatric disorders in primary care patients in 14 different countries. Comorbidity was common, with the overlap between anxiety and depressive episodes being particularly great. Indeed, the proportion of those with a current anxiety disorder who also had a current depressive disorder was reported to be approximately 45%. Likewise, the proportion of those with a current depressive disorder who also had a current anxiety disorder was reported to be approximately 40%. The study also showed that the association between depression and anxiety disorders was stronger than between the anxiety disorders themselves. Lecrubier Y. The impact of comorbidity on the treatment of panic disorder. J Clin Psychiatry 1998; 59 (Suppl 8): Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 8):")
25
Comorbidità tra ansia e depressione lifetime
DISTURBI D’ANSIA Prevalenza lifetime: 25% COMORBIDITÀ >50% con DM va incontro ad un disturbo d’ansia DEPRESSIONE MAGGIORE Prevalenza lifetime: 17% Kessler RC, et al. Arch Gen Psychiatry. 1994;51:8-19.

26
Sovrapposizione tra sintomi ansiosi e sintomi depressivi
Ansia* Depressione Umore depresso Perdita di interessi Anedonia Disturbi dell’appetito Ideazioni suicidarie Bassa autostima Ansia Preoccupazione Xerostomia Palpitazioni Sudorazione Tremori Rossore Agitazione Irritabilità Astenia Difficoltà di concentrazione Dist. del sonno Tensione muscolare Dolore There are many overlapping symptoms in depression, GAD, and SAD. While some forms of anxiety (eg, SAD) may appear more distinct than others when compared with depression, they still share some common symptoms. In contrast, the symptomatology of chronic anxiety (eg, GAD) and depression share many common features. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition-Text Revision. 2000; Washington, DC: APA. *Sintomi del DAG e della FS DSM-IV-TR. Washigton, DC: American Psychiatric Association; 2000.
 may appear more distinct than others when compared with depression, they still share some common symptoms. In contrast, the symptomatology of chronic anxiety (eg, GAD) and depression share many common features. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition-Text Revision. 2000; Washington, DC: APA. *Sintomi del DAG e della FS. DSM-IV-TR. Washigton, DC: American Psychiatric Association;")
27
Sovrapposizione tra sintomi ansiosi e sintomi depressivi
FOBIA SOCIALE paura/evitamento di situazioni sociali rossore, tremori DISTURBO D’ANSIA GENERALIZZATA DISTURBO DEPRESSIVO MAGGIORE palpitazioni sudorazione bassa autostima difficoltà di concentrazione difficoltà interpersonali anedonia umore depresso ideazioni suicidarie disturbi dell’appetito preoccupazione ansia tensione muscolare xerostomia agitazione, irritabilità disturbi del sonno affaticamento dolore DSM-IV-TR. Washigton, DC: American Psychiatric Association; 2000.

28
Depressione associata ad ansia in medicina generale
13% Depressione associata ad ansia Tutte le altre diagnosi In almeno il 65% dei pazienti depressi è presente anche ansia moderata

29
Implicazioni della comorbidità tra depressione e ansia
Diminuita risposta ai trattamenti Aumento della gravità dei sintomi Maggiore utilizzo delle risorse sanitarie Maggiore incidenza di suicidio Maggiore compromissione occupazionale This slide outlines some of the consequences of comorbid depression and anxiety disorders. Patients with comorbid psychiatric disorders have a greater symptom severity and a more chronic course of illness compared with those patients with a single psychiatric disorder. The HARP study has shown that, as a consequence, patients with comorbid disorders have a greater impairment of social functioning and quality of life, and a lower socioeconomic and educational status. Furthermore, such patients have a greater likelihood of committing suicide. Patients with comorbid disorders are also less likely to respond to treatment and are more likely to have a history of psychiatric hospitalization, resulting in a greater burden on health care resources and to society as a whole. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Arch Gen Psychiatry 1994; 51: 8-19. Lecrubier Y. The impact of comorbidity on the treatment of panic disorder. J Clin Psychiatry 1998; 59 (Suppl 8): Lecrubier Y. Comorbidity in social anxiety disorder. J Clin Psychiatry 1998; 59 (Suppl 17): Kaufman J, Charney D. Comorbidity of mood and anxiety disorders. Depress Anxiety 2000; 12 (Suppl 1): 69-76, Maggiore compromissione sociale Maggiore impatto sociale Aumento della cronicità Kessler et al. Arch Gen Psychiatry 1994; 51: 8-19. Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 8): Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 17): Kaufman & Charney. Depress Anxiety 2000; 12 (Suppl 1):
: Lecrubier Y. Comorbidity in social anxiety disorder. J Clin Psychiatry 1998; 59 (Suppl 17): Kaufman J, Charney D. Comorbidity of mood and anxiety disorders. Depress Anxiety 2000; 12 (Suppl 1): 69-76, Maggiore compromissione sociale. Maggiore impatto sociale. Aumento della cronicità. Kessler et al. Arch Gen Psychiatry 1994; 51: Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 8): Lecrubier. J Clin Psychiatry 1998; 59 (Suppl 17): Kaufman & Charney. Depress Anxiety 2000; 12 (Suppl 1):")
30
Depressione e ansia 45-95% dei pazienti di medicina generale con DEPRESSIONE lamenta soltanto sintomi somatici I sintomi fisici non spiegati dovrebbero far pensare a questi disturbi 32-62% di questi pazienti hanno un disturbo depressivo 24-50% un disturbo d’ansia Le sindromi somatiche funzionali sono spesso associate a depressione e ansia Simon et al. N Engl J Med 1999; 341: Kroenke et al. Arch Fam Med 1994; 3: Katon et al. Ann Intern Med 2001; 134:

31
Somatic symptoms as potential markers for anxiety disorders
Somatic symptoms as potential markers for anxiety disorders. Data were collected from patients presenting at 4 primary care clinics.

35
Exploration of DSM-IV criteria in primary care patients with medically unexplained symptoms.
OBJECTIVES: Investigators and clinicians almost always rely DSM-IV somatoform disorders (and its derivative diagnoses) to characterize and identify patients with medically unexplained symptoms (MUS). Our objective was to evaluate this use by determining the prevalence of DSM-IV somatoform and non somatoform disorders in patients with MUS proven by a gold standard chart review. Smith RC et al. Psychosom Med Jan-Feb;67(1):123-9
 to characterize and identify patients with medically unexplained symptoms (MUS). Our objective was to evaluate this use by determining the prevalence of DSM-IV somatoform and non somatoform disorders in patients with MUS proven by a gold standard chart review. Smith RC et al. Psychosom Med Jan-Feb;67(1):")
36
Two hundred six MUS patients averaged 13
Two hundred six MUS patients averaged 13.6 visits in the year preceding study, 79.1% were females, and the average age was 47.7 years. 124 patients (60.2%) had a non somatoform ("psychiatric") DSM-IV diagnosis of any type 36 (17.5%) had 2 full non somatoform diagnoses 41 (19.9%) had >2 92 (44.7%) had some full anxiety diagnosis 94 (45.6%) had either full depression or minor depression diagnoses 9 of 206 (4.4%) had any full DSM-IV somatoform diagnosis 39 (18.9%) had abridged somatization disorder 48 (23.3%) were "DSM somatoform-positive“ 158 (76.7%) were "DSM somatoform-negative The latter exhibited less anxiety, depression, mental dysfunction, and psychosomatic symptoms (all p <.001) and less physical dysfunction (p = .011). Correlates of this DSM somatoform-negative status were female gender (p = .007), less severe mental (p = .007), and physical dysfunction (p = .004), a decreased proportion of MUS (p <.10), and less psychiatric comorbidity (p <.10); c-statistic = 0.77.
 had a non somatoform ( psychiatric ) DSM-IV diagnosis of any type. 36 (17.5%) had 2 full non somatoform diagnoses. 41 (19.9%) had >2. 92 (44.7%) had some full anxiety diagnosis. 94 (45.6%) had either full depression or minor depression diagnoses. 9 of 206 (4.4%) had any full DSM-IV somatoform diagnosis. 39 (18.9%) had abridged somatization disorder. 48 (23.3%) were DSM somatoform-positive 158 (76.7%) were DSM somatoform-negative. The latter exhibited less anxiety, depression, mental dysfunction, and psychosomatic symptoms (all p <.001) and less physical dysfunction (p = .011). Correlates of this DSM somatoform-negative status were female gender (p = .007), less severe mental (p = .007), and physical dysfunction (p = .004), a decreased proportion of MUS (p <.10), and less psychiatric comorbidity (p <.10); c-statistic =")
37
Smith concluded that depression and anxiety characterized MUS patients better than the somatoform disorders. Our data suggested radically revising the somatoform disorders for DSM-V by incorporating a new, very large group of now-overlooked DSM somatoform-negative patients who were typically women with less severe dysfunction. Smith RC et al. Psychosom Med Jan-Feb;67(1):123-9
:")
38
A Potential Etiological Model for Functional Somatic Symptoms
Mayou et al., 2005

39
Somatoform Disorders: Time for a New Approach in DSM-V
Diagnoses currently within somatoform disorders could be redistributed into other groupings. The disorders currently defined solely by somatic symptoms could be placed on axis III as “functional somatic symptoms and syndromes.” The Authors also argue that more use could also be made of the category “psychological factors affecting medical condition” that appears in DSM-IV only as part of the chapter titled “other conditions that may be a focus of clinical attention.” This could be an axis I accompaniment to any axis III diagnosis. Mayou et al., 2005

40
A Multidimensional Descriptive System for Somatic Symptoms
Type of somatic symptom Number of symptoms Course (e.g., acute, chronic, recurrent) Disease pathology/pathophysiology Health beliefs Illness behavior Associated psychiatric disorder Social factors (e.g., employment, social benefits) Mayou et al., 2005
 Disease pathology/pathophysiology. Health beliefs. Illness behavior. Associated psychiatric disorder. Social factors (e.g., employment, social benefits) Mayou et al.,")
41
Review and critique of the new DSM-IV diagnosis of acute stress disorder.
…The diagnosis of acute stress disorder does not appear to achieve the important objective of providing adequate clinical coverage for individuals with acute posttraumatic symptoms. The validity and utility of requiring peritraumatic dissociative symptoms as a core feature are questionable, as is the separation of essentially continuous clinical phenomena into two disorders with different criteria sets (acute stress disorder and PTSD) based on persistence of symptoms for 30 or more days. Longitudinal studies using acute stress disorder criteria, as well as broader considerations of the clinical and scientific functions that posttraumatic diagnoses should serve, suggest a need to reevaluate the current DSM-IV approach to post traumatic syndromes. Marshall RD et al. Am J Psychiatry Nov;156(11):
 based on persistence of symptoms for 30 or more days. Longitudinal studies using acute stress disorder criteria, as well as broader considerations of the clinical and scientific functions that posttraumatic diagnoses should serve, suggest a need to reevaluate the current DSM-IV approach to post traumatic syndromes. Marshall RD et al. Am J Psychiatry Nov;156(11):")
43
Nuove prospettive di ricerca

44
Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications.
“We review psychometric and other evidence relevant to mixed anxiety-depression… … With these data, we argue for a tripartite structure consisting of GENERAL DISTRESS PHYSIOLOGICAL HYPERAROUSAL (specific anxiety) ANHEDONIA (specific depression) …we propose a diagnosis of mixed anxiety-depression.” Clark LA, Watson D, J Abnorm Psychol Aug;100(3):316-36
 ANHEDONIA (specific depression) …we propose a diagnosis of mixed anxiety-depression. Clark LA, Watson D, J Abnorm Psychol Aug;100(3):")
45
Rethinking the mood and anxiety disorders: a quantitative hierarchical model for DSM-V.
…The existing structural evidence eliminate this rational system and replace it with an empirically based structure that reflects establishes that the mood and anxiety disorders should be collapsed together into an overarching class of emotional disorders, which can be decomposed into 3 subclasses: bipolar disorders (bipolar I, bipolar II, cyclothymia) distress disorders (major depression, dysthymic disorder, generalized anxiety disorder, posttraumatic stress disorder) fear disorders (panic disorder, agoraphobia, social phobia, specific phobia). The optimal placement of other syndromes (e.g., obsessive-compulsive disorder) needs to be clarified in future research Watson D., J Abnorm Psychol Nov;114(4):522-36
 distress disorders (major depression, dysthymic disorder, generalized anxiety disorder, posttraumatic stress disorder) fear disorders (panic disorder, agoraphobia, social phobia, specific phobia). The optimal placement of other syndromes (e.g., obsessive-compulsive disorder) needs to be clarified in future research. Watson D., J Abnorm Psychol Nov;114(4):")
47
The structure of common DSM-IV and ICD-10 mental disorders in the Australian general population.
…. Participants consisted of a random population-based sample of community volunteers, representing a response rate of 78%. DSM-IV and ICD-10 mental disorder diagnoses were obtained using the Composite International Diagnostic Interview (CIDI), version 2.0. Confirmatory factor analysis (CFA) was used to assess the relative fit of competing models… Slade T., Watson D., Psychol Med Nov;36(11):
, version 2.0. Confirmatory factor analysis (CFA) was used to assess the relative fit of competing models… Slade T., Watson D., Psychol Med Nov;36(11):")
48
Distress factor Fear factor Externalizing factor INTERNALIZING FACTORS
…A hierarchical three-factor variation of a two-factor model demonstrated the best fit to the correlations among the mental disorders. This model included: INTERNALIZING FACTORS Distress factor Fear factor Externalizing factor social phobia Neurasthenia (ICD-10 only) alcohol agoraphobia PTSD GAD OCD dystimia drug dependence panic disorder major depression Modif. da Slade T 2006
 alcohol. agoraphobia. PTSD. GAD. OCD. dystimia. drug dependence. panic disorder. major depression. Modif. da Slade T")
49
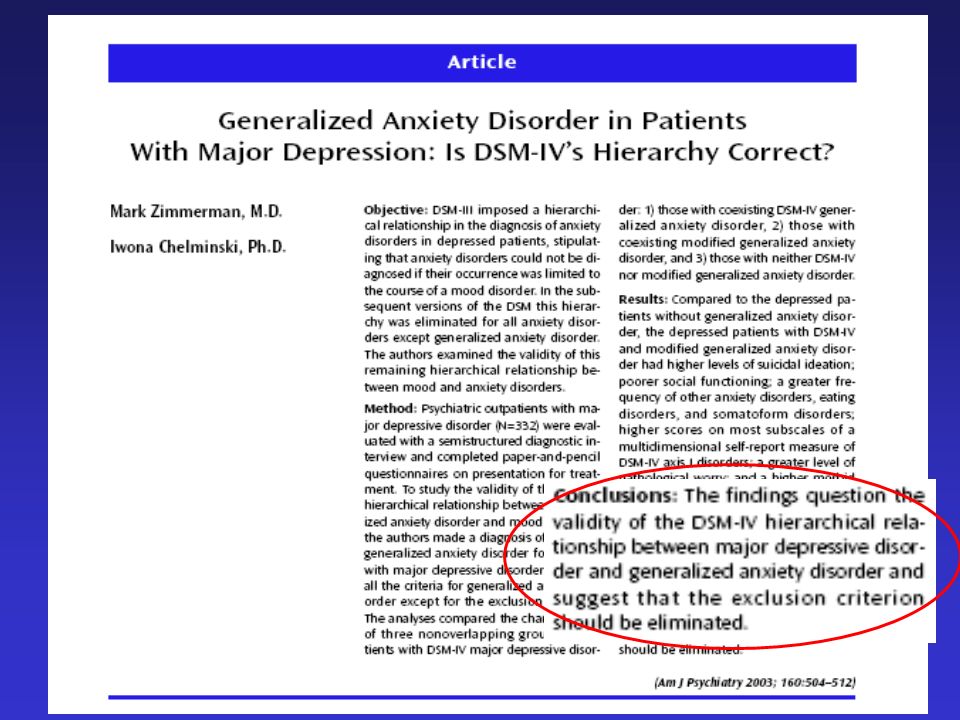
Major depression and generalised anxiety disorder
Major depression and generalised anxiety disorder. Same genes, (partly)different environments--revisited. In both clinical and epidemiological samples, major depression (MD) and generalised anxiety disorder (GAD) display substantial comorbidity… … The best-fitting twin models, when GAD was diagnosed with or without a diagnostic hierarchy, found a genetic correlation of unity between the two disorders. The correlation in environmental risk factors was when GAD was diagnosed non-hierarchically, but zero when hierarchical diagnoses were used. Our findings provide further support for the hypothesis that in women, MD and GAD are the result of the same genetic factors. Environmental risk factors that predispose to 'pure' GAD episodes may be relatively distinct from those that increase risk for MD. Kendler KS Br J Psychiatry Suppl Jun;(30):68-75
different environments--revisited. In both clinical and epidemiological samples, major depression (MD) and generalised anxiety disorder (GAD) display substantial comorbidity… … The best-fitting twin models, when GAD was diagnosed with or without a diagnostic hierarchy, found a genetic correlation of unity between the two disorders. The correlation in environmental risk factors was when GAD was diagnosed non-hierarchically, but zero when hierarchical diagnoses were used. Our findings provide further support for the hypothesis that in women, MD and GAD are the result of the same genetic factors. Environmental risk factors that predispose to pure GAD episodes may be relatively distinct from those that increase risk for MD. Kendler KS Br J Psychiatry Suppl Jun;(30):")
50
Co-morbid major depression and generalized anxiety disorders in the National Comorbidity Survey follow-up. … Although generalized anxiety disorder (GAD) and major depressive episode (MDE) are known to be highly co-morbid, little prospective research has examined whether these two disorders predict the subsequent first onset or persistence of the other or the extent to which other predictors explain the time-lagged associations between GAD and MDE. … The existence of differences in risk factors for GAD and MDE argues against the view that the two disorders are merely different manifestations of a single underlying internalizing syndrome or that GAD is merely a prodrome, residual, or severity marker of MDE Kessler RC Psychol Med Nov 30;:1-10
 and major depressive episode (MDE) are known to be highly co-morbid, little prospective research has examined whether these two disorders predict the subsequent first onset or persistence of the other or the extent to which other predictors explain the time-lagged associations between GAD and MDE. … The existence of differences in risk factors for GAD and MDE argues against the view that the two disorders are merely different manifestations of a single underlying internalizing syndrome or that GAD is merely a prodrome, residual, or severity marker of MDE. Kessler RC Psychol Med Nov 30;:1-10.")
51
Supplementary dimensional assessment in anxiety disorders.
Anxiety disorders, as defined in the DSM-IV, comprise a relatively heterogeneous group of clinical conditions that range from specific phobias to obsessive compulsive disorder (OCD) and post-traumatic stress disorder (PTSD)… … We suggest the use of cross-cutting dimensional ratings that might ultimately lead to an improved classification model. We also suggest that a staging approach to illness, based upon supplementary dimensional rating could provide useful information for clinical and research purposes. Shear MK et al. Int J Methods Psychiatr Res. 2007;16 Suppl :S52-64
 and post-traumatic stress disorder (PTSD)… … We suggest the use of cross-cutting dimensional ratings that might ultimately lead to an improved classification model. We also suggest that a staging approach to illness, based upon supplementary dimensional rating could provide useful information for clinical and research purposes. Shear MK et al. Int J Methods Psychiatr Res. 2007;16 Suppl :S")
52
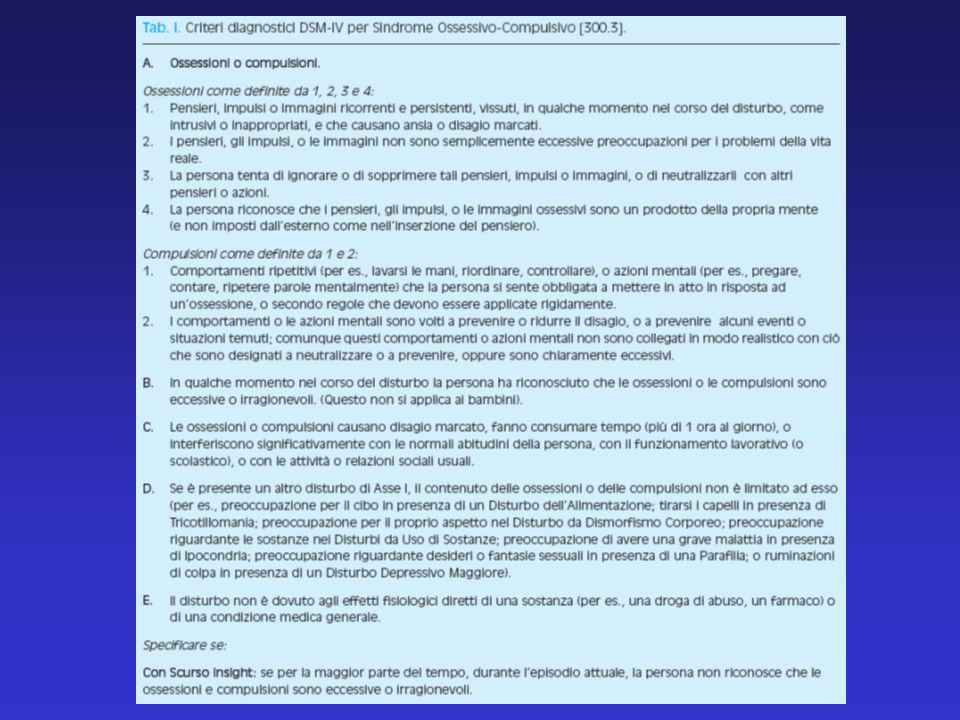
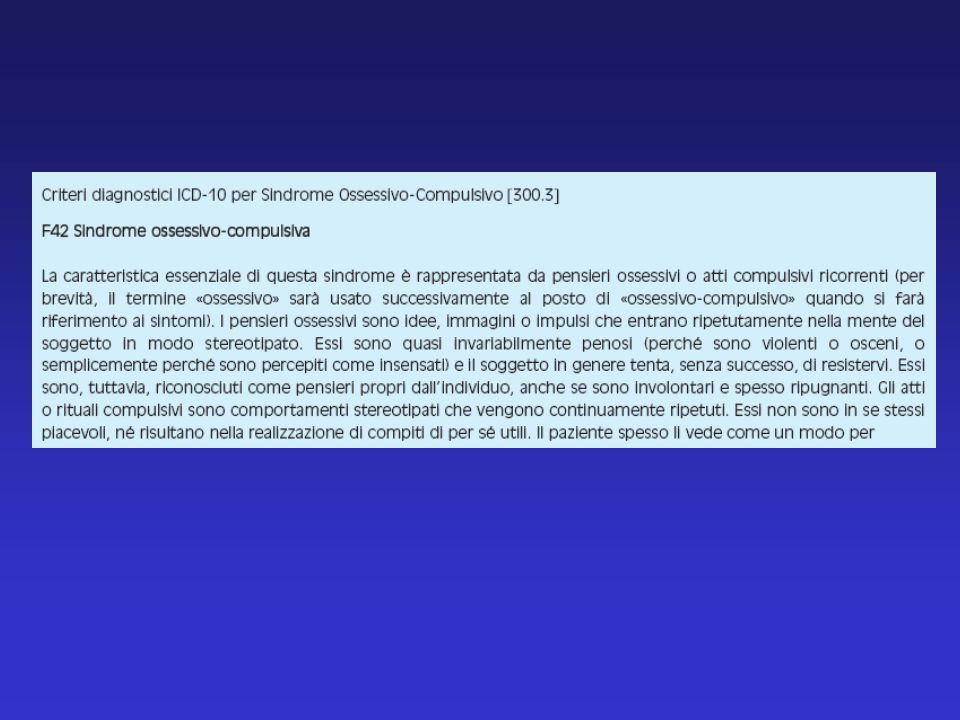
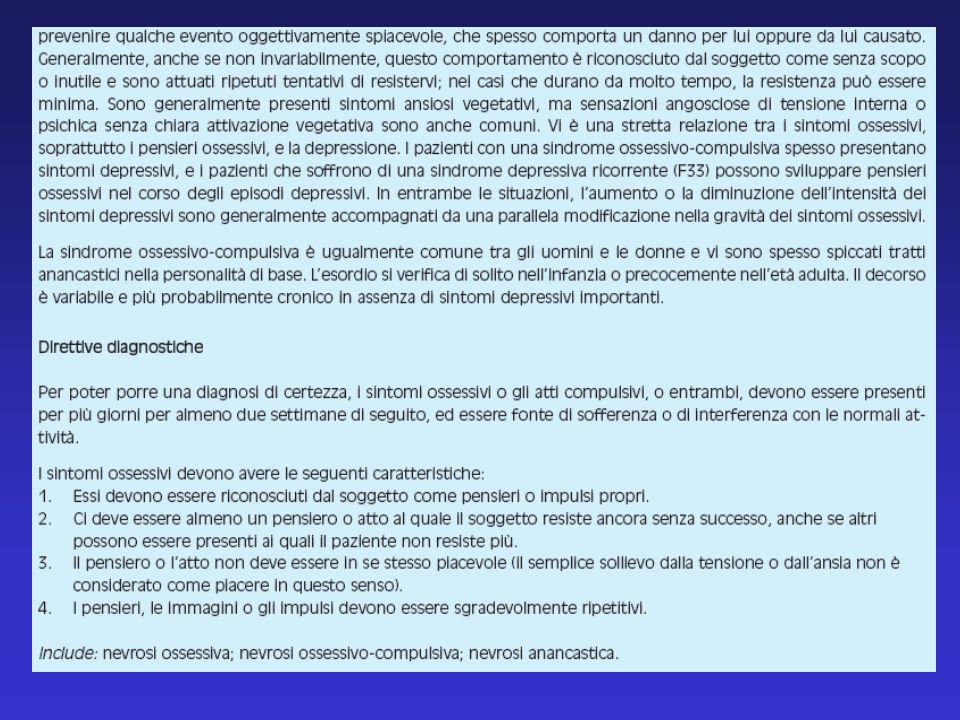
… e il D.O.C.?

53
DSM IV ICD 10 Disturbi d’ansia Sindromi fobiche, legate a stress
e somatoformi DOC

57
Obsessive-compulsive disorder and obsessive-compulsive spectrum disorders: diagnostic and dimensional issues Although obsessive-compulsive disorder (OCD) is classified as an anxiety disorder in the DSM-IV, recent considerations for a reclassification into an obsessive-compulsive spectrum disorders (OCSDs) cluster are gaining prominence. … With further studies, it is ultimately the goal to define OCD and related disorders based on endophenotypes. Despite efforts in this field, there are several fundamental unresolved issues, including the question of which disorders should be grouped together in this category and which characteristics to include as their shared common features. A reclassification of OCD among the OCSDs would allow for better scrutiny of distinct obsessive-compulsive symptoms, as currently this disorder often goes undetected in patients who complain of a broad symptom of anxiety. Hollander E. et al. CNS Spectr Feb;12(2 Suppl 3):5-13
 is classified as an anxiety disorder in the DSM-IV, recent considerations for a reclassification into an obsessive-compulsive spectrum disorders (OCSDs) cluster are gaining prominence. … With further studies, it is ultimately the goal to define OCD and related disorders based on endophenotypes. Despite efforts in this field, there are several fundamental unresolved issues, including the question of which disorders should be grouped together in this category and which characteristics to include as their shared common features. A reclassification of OCD among the OCSDs would allow for better scrutiny of distinct obsessive-compulsive symptoms, as currently this disorder often goes undetected in patients who complain of a broad symptom of anxiety. Hollander E. et al. CNS Spectr Feb;12(2 Suppl 3):5-13.")
58
Spettro Ossessivo-compulsivo
I Disturbi dello Spettro sono tutti accumunati dall’incapacità di ritardare o inibire comportamenti ripetitivi ed egodistonici, con relativo sollievo solo al termine del compimento dell’atto (Hantouche & Merckaert,1991; Hollander, 1996; Cartwright, 1998). Hollander, 1998
. Hollander,")
59
Classification of obsessive-compulsive disorder in childhood and adolescence
… The agreement between the two diagnostic systems was low. The diagnostic stability of ICD-10-DCR was highly dependent on age, whereas that of the criteria DSM-IV did not depend on age and almost all subjects could be diagnosed definitely. CONCLUSION: This study suggests that the DSM-IV criteria are superior to that of ICD-10-DCR for diagnosing OCD in children and younger adolescents. Steinberger K et al. Acta Psychiatr Scand Aug;106(2):97-102
:")
60
Symptom dimensions in obsessive-compulsive disorder: implications for the DSM-V.
In the absence of definitive etiological markers of vulnerability or a unitary profile of pathophysiology for obsessive-compulsive disorder (OCD), obsessive-compulsive (OC) symptom dimensions seem to offer a fruitful point of orientation. The complex clinical presentation of OCD can be summarized using a few consistent and temporally stable symptom dimensions, understood as a spectrum of potentially overlapping features that are likely to be continuous with "normal" worries and extend beyond the traditional nosological boundaries of OCD. Leckman JF et al. CNS Spectr May;12(5):376-87, 400
, obsessive-compulsive (OC) symptom dimensions seem to offer a fruitful point of orientation. The complex clinical presentation of OCD can be summarized using a few consistent and temporally stable symptom dimensions, understood as a spectrum of potentially overlapping features that are likely to be continuous with normal worries and extend beyond the traditional nosological boundaries of OCD. Leckman JF et al. CNS Spectr May;12(5):376-87, 400.")
61
Although the understanding of the dimensional structure of obsessive-compulsive symptoms (OCS) is still imperfect, this quantitative approach to phenotypic traits has the potential to advance our understanding of OCD and may aid in the identification of more robust endophenotypes. Preliminary data suggest that these dimensional phenotypes may be useful in studies of the natural history, genetics, neurobiology, and treatment outcome of OCD. A dimensional approach is not mutually exclusive of other methods to parse the larger spectrum of disorders related to OCD. Thus far, age-of-onset of OCS and the individual's "tic-related" status seem to be particularly useful categorical distinctions. Finally, existing assessment methods are inadequate and new dimensional scales are needed to take full advantage of a dimensional approach in clinical and population-based studies.

Presentazioni simili