Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Diabete ed anziano

2
County-level Estimates of Diagnosed Diabetes for Adults aged ≥ 20 years: United States 2007 Modificato da www. CDC.gov

5
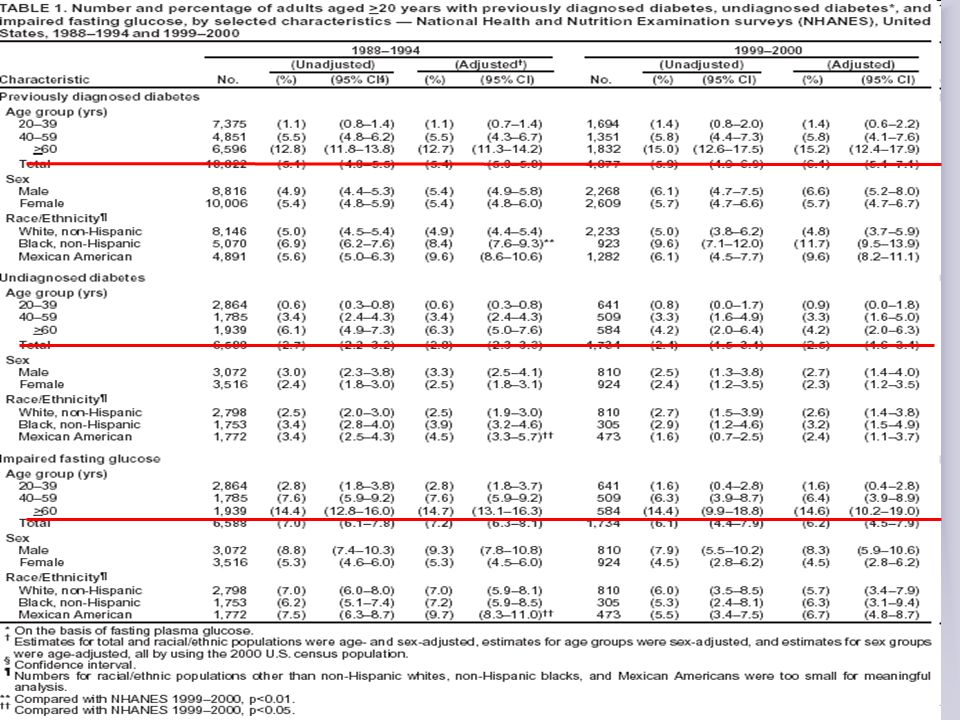
Based on data derived from the National Health Interview Survey (NHIS) and the Third National Health and Nutrition Examination Survey (NHANES III), the CDC estimated that in 2000, the percentage of adults with diabetes was 2.5% among 20 to 44 year-olds, 12.1% among 45 to 64 year-olds, 21.6% among 65 to 74 year-olds, and 18.5% among those over 75.
 and the Third National Health and Nutrition Examination Survey (NHANES III), the CDC estimated that in 2000, the percentage of adults with diabetes was 2.5% among 20 to 44 year-olds, 12.1% among 45 to 64 year-olds, 21.6% among 65 to 74 year-olds, and 18.5% among those over 75.")
6
The third National Health and Nutrition Examination Survey (NHANES III) was a national examination study conducted in the United States with the goals of: estimating the prevalence of selected diseases and risk factors; estimating population reference distributions of certain health parameters; documenting and investigating reasons for secular trends in selected diseases and risk factors; contributing to an understanding of disease etiology; and investigating the natural history of selected diseases. The NHANES III sample was selected from 81 counties between 1988 and 1994.

7
Future Prevalence Every 8 Seconds.......a Baby Boomer turns 60. By 2015, nearly 15% of our population will be over 65 years of age Last time I watched was Fonte: The American Geriatrics Society

8
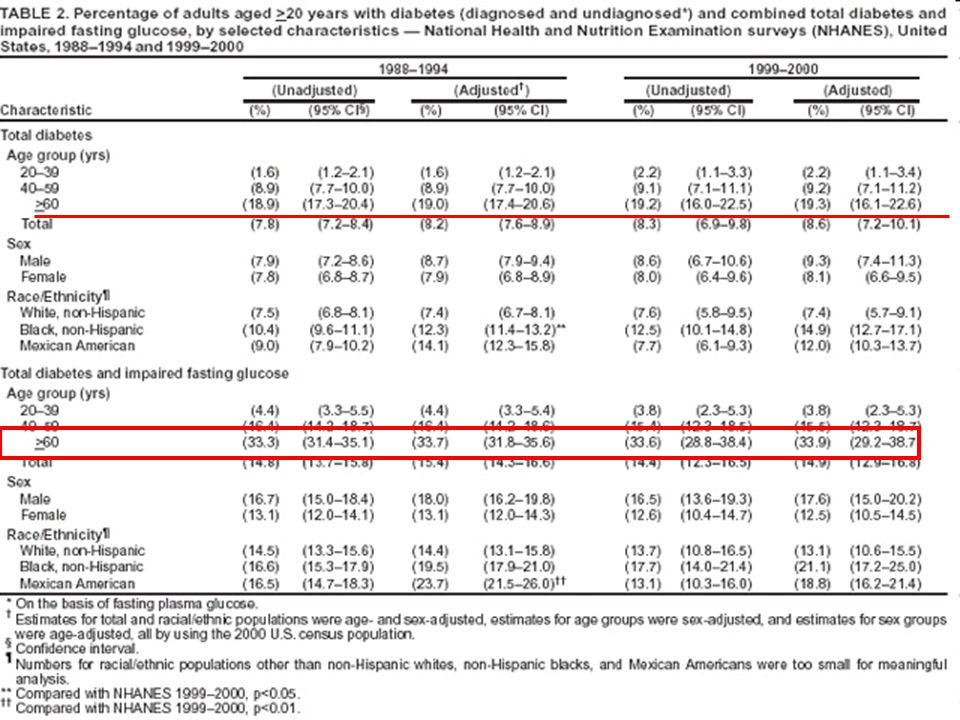
Prevalence of type 2 diabetes by age from the Third National Health and Nutrition Examination Survey (NHANES III). The prevalence of type 2 diabetes increases with advancing age. More than 20% of adults aged 60–74 yr have type 2 diabetes, including those previously diagnosed with diabetes and those newly diagnosed by fasting (FPG) or oral glucose tolerance test (OGTT) criteria.
 or oral glucose tolerance test (OGTT) criteria..")
9
In italia… Per quanto riguarda il diabete, i dati riportati nell’annuario statistico Istat 2006 indicano che è diabetico il 4,5% degli italiani (4,6% le donne e 4,3% gli uomini). Numeri che segnano un aumento rispetto all’indagine multiscopo del 1999-2000, secondo cui era diabetico il 3,7% degli italiani (4% le donne e 3,5% gli uomini). In Italia, i pazienti diabetici noti sono attualmente circa 2.200.000 e saliranno nel 2025 a 3.300.000
. In Italia, i pazienti diabetici noti sono attualmente circa e saliranno nel 2025 a")
10
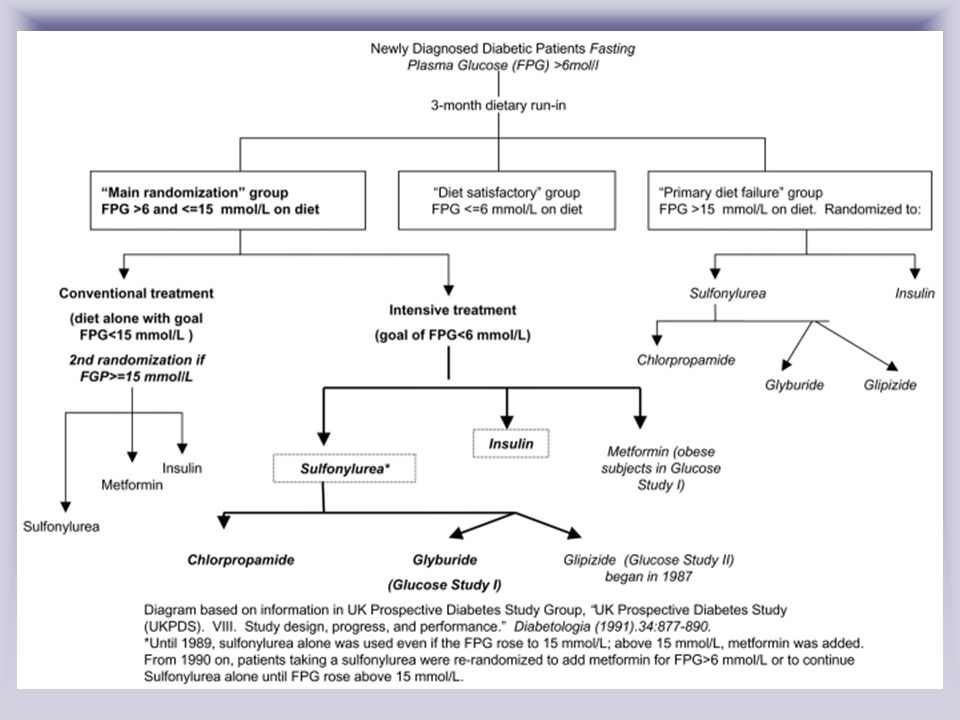
Al contrario, i grandi studi di intervento sia sul diabete tipo 1 (DCCT), sia sul diabete tipo 2 (UKPDS) hanno dimostrato che il mantenimento di un adeguato compenso metabolico, grazie a schemi intensivi di trattamento, è in grado di ridurre l’incidenza delle complicanze. Una strategia di intervento, oramai ineludibile, è quella della Gestione Integrata del paziente diabetico (individuabile nel “care management program” della letteratura internazionale).
..")
11
Goals of therapy for elderly diabetic patients should include an evaluation of their functional status, life expectancy, social and financial support, and their own desires for treatment. A full geriatric assessment performed before establishing any long-term diabetes therapy may aid in identifying potential problems that could significantly impair the success of a given therapy. Often, elderly patients have cognitive impairments, limitations in their activities of daily living, undiagnosed depression, and difficult social issues that need to be addressed. The ideal HbA1c target of 80 years of age). Major large prospective trials to date have not reported conclusive data on intensive blood glucose control and improved vascular endpoints for the geriatric population. Diabetes is associated with lower levels of cognitive functioning and greater cognitive decline in elderly.
. Major large prospective trials to date have not reported conclusive data on intensive blood glucose control and improved vascular endpoints for the geriatric population. Diabetes is associated with lower levels of cognitive functioning and greater cognitive decline in elderly..")
12
Nell’anziano si hanno alcune caratteristiche peculiari, dovute sia a cambiamenti di tipo antropometrico che fisiopatologico: Aumento della massa adiposa Riduzione della massa magra Ridotta risposta della beta cellula boh

13
Model for age-related hyperglycemia. AJP-Endocrinol Metab VOL 284 JANUARY 2003 www.ajpendo.org

14
Multiple risk factors for type 2 diabetes associated with aging predispose older adults to develop glucose intolerance and increased insulin resistance. However, in elderly humans, β -cell function is impaired, and compensatory hyperinsulinemia does not occur. With further loss of β -cell function, impaired glucose tolerance (IGT) and type 2 diabetes develop.
 and type 2 diabetes develop..")
15
Valutazione multidimensionale del soggetto diabetico anziano BADL (Katz, Barthel) IADL (Lawton-Brody) Funzioni cognitive (MMSE, SPMSQ) Stato affettivo (GDS) Comorbidità (indice di Charlson) Stato nutrizionale (MNA) Supporto sociale EUGMS Linee Guida Cliniche per il Diabete Mellito Tipo 2 Gruppo di Lavoro Europeo sul Diabete nell’Anziano 2001-2004
 IADL (Lawton-Brody) Funzioni cognitive (MMSE, SPMSQ) Stato affettivo (GDS) Comorbidità (indice di Charlson) Stato nutrizionale (MNA) Supporto sociale EUGMS Linee Guida Cliniche per il Diabete Mellito Tipo 2 Gruppo di Lavoro Europeo sul Diabete nell’Anziano")
16
50% degli anziani diabetici sono ignari di esserne affetti Sintomi dell’iperglicemia raramente presenti

17
Deterioramento cognitivo Il diabete è associato a declino cognitivo / demenza Il medico dovrebbe sempre valutare lo stato cognitivo del paziente diabetico anziano usando un test standardizzato nel corso della valutazione iniziale e in caso di peggioramento delle condizioni cliniche Un peggioramento dello stato cognitivo o funzionale dovrebbe essere considerato di per sé come un peggioramento delle condizioni cliniche (evidenza IIIA) California Healthcare Foundation/American Geriatrics Society Panel on improving care for elders with diabetes JAGS 2003
 California Healthcare Foundation/American Geriatrics Society Panel on improving care for elders with diabetes JAGS 2003")
18
Obiettivi del trattamento del diabete IPOGLICEMIA REAZIONI AVVERSE DA FARMACI GARANTIRE LA QUALITA’ DELLA VITA pREVENZIONE COMPLICANZE A BREVE TERMINE PREVENZIONE COMPLICANZE A LUNGO TERMINE (?)
")
19
For elderly patients who require medical therapy, the following options are available. 1. Alpha-glucosidase inhibitors (e.g., acarbose [Precose] and miglitol [Glyset]). These agents delay digestion of complex carbohydrates and disaccharides. Although less effective than other agents, they should be considered in all elderly patients with mild diabetes. Gastrointestinal side effects may limit therapy or may benefit those who suffer from constipation. Liver functioning may be impaired at high doses, but this has not been a clinical problem. 2. Biguanides (e.g., metformin [Glucophage]). The benefit of metformin in the elderly is that it does not cause hypoglycemia when used independently. However, it is used with caution in the elderly because it can cause anorexia and weight loss.Before starting therapy, all elderly patients should have their creatinine clearance calculated. Serum creatinine is a poor correlate because of low muscle mass in the elderly. Metformin should not be administered if the creatinine clearance is <60 mg/dl. 3. Thiazolidinediones (e.g., rosiglitazone [Avandia] and pioglitazone [Actos]). These are true insulin sentisitizers and enhance insulin effects by activating the PPAR alpha receptor.18 Rosiglitazone has been shown to be safe and effective in elderly patients. It does not cause hypoglycemia. However, it should be avoided in patients with heart failure. Thiazolidinediones are comparatively expensive drugs, but for elderly patients who can afford them, they are potentially very useful. 4. Sulfonylureas (e.g, glipizide [Glucotrol], glyburide [Micronase, Diabeta, Glynase]) and other types of secretagogues (e.g., repaglinide [Prandin] and nateglinide [Starlix]). Traditional sulfonylureas are still widely used as first-line therapy. First-generation agents such as chlorpropamide should be avoided in the elderly because of their long half-life and increased propensity for hypoglycemia in the elderly. Although sulfonylureas can cause hypoglycemia in the elderly, the incidence is relatively low if shorter- acting agents are used.20,21 Repaglinide is unrelated to the sulfonylureas but also promotes insulin secretion from pancreatic -cells. Unlike with sulfonylureas, in the absence of exogenous glucose, insulin release is lessened with repaglinide. Nateglinide is unrelated to the sulfonylureas and repaglinide, but it also acts on pancreatic –cells as an insulin secretagogue. Both repaglinide and nateglinide are used around meal times and are short-acting, which may lessen the risk of hypoglycemia. With the exception of nateglinide, insulin secretagogues should be used with caution in patients with renal dysfunction. All insulin secretagogues should be avoided in those with liver disease.
. These agents delay digestion of complex carbohydrates and disaccharides. Although less effective than other agents, they should be considered in all elderly patients with mild diabetes. Gastrointestinal side effects may limit therapy or may benefit those who suffer from constipation. Liver functioning may be impaired at high doses, but this has not been a clinical problem. 2. Biguanides (e.g., metformin [Glucophage]). The benefit of metformin in the elderly is that it does not cause hypoglycemia when used independently. However, it is used with caution in the elderly because it can cause anorexia and weight loss.Before starting therapy, all elderly patients should have their creatinine clearance calculated. Serum creatinine is a poor correlate because of low muscle mass in the elderly. Metformin should not be administered if the creatinine clearance is <60 mg/dl. 3. Thiazolidinediones (e.g., rosiglitazone [Avandia] and pioglitazone [Actos]). These are true insulin sentisitizers and enhance insulin effects by activating the PPAR alpha receptor.18 Rosiglitazone has been shown to be safe and effective in elderly patients. It does not cause hypoglycemia. However, it should be avoided in patients with heart failure. Thiazolidinediones are comparatively expensive drugs, but for elderly patients who can afford them, they are potentially very useful. 4. Sulfonylureas (e.g, glipizide [Glucotrol], glyburide [Micronase, Diabeta, Glynase]) and other types of secretagogues (e.g., repaglinide [Prandin] and nateglinide [Starlix]). Traditional sulfonylureas are still widely used as first-line therapy. First-generation agents such as chlorpropamide should be avoided in the elderly because of their long half-life and increased propensity for hypoglycemia in the elderly. Although sulfonylureas can cause hypoglycemia in the elderly, the incidence is relatively low if shorter- acting agents are used.20,21 Repaglinide is unrelated to the sulfonylureas but also promotes insulin secretion from pancreatic -cells. Unlike with sulfonylureas, in the absence of exogenous glucose, insulin release is lessened with repaglinide. Nateglinide is unrelated to the sulfonylureas and repaglinide, but it also acts on pancreatic –cells as an insulin secretagogue. Both repaglinide and nateglinide are used around meal times and are short-acting, which may lessen the risk of hypoglycemia. With the exception of nateglinide, insulin secretagogues should be used with caution in patients with renal dysfunction. All insulin secretagogues should be avoided in those with liver disease..")
20
Sicuramente però tra le principali cause di diabete nel paziente anziano dobbiamo annoverare: 1) cause antropometriche età dipendententi; 2) variazioni età-dipendenti dello stile di vita; 3) cause iatrogene; 4) cause neuro-ormonali. Per quanto riguarda le cause antropometriche con l’avanzare dell’età si assiste ad un progressivo rimodellamento della composizione corporea con una riduzione della massa magra (metabolicamente attiva) ed un aumento assoluto e relativo del tessuto adiposo. Tale ridistribuzione età correlato dei rapporti tra massa magra e tessuto adiposo crea una situazione sfavorevole dal punto di vista metabolico che sicuramente è foriera di alterata omeostasi glicemica.
 ed un aumento assoluto e relativo del tessuto adiposo. Tale ridistribuzione età correlato dei rapporti tra massa magra e tessuto adiposo crea una situazione sfavorevole dal punto di vista metabolico che sicuramente è foriera di alterata omeostasi glicemica..")
23
Insulin. The risk of severe hypoglycemia associated with insulin increases with age.5,22 Initiation of insulin in elderly type 2 diabetic patients should be done with the involvement of a multidisciplinary team. A complete geriatric assessment should be performed first to assure that patients can comply with their regimens and to identify potential complicating factors. If there are identified caregivers, provisions for adequate respite programs should be offered to avoid caregiver burnout.

25
Third National Health & Nutrition Examination Survey Public health A population-based survey conducted by the National Center for Health Statistics, designed to assess the health and nutritional status of the noninstitutionalized Americans

26
The third National Health and Nutrition Examination Survey (NHANES III) was a national examination study conducted in the United States with the goals of: estimating the prevalence of selected diseases and risk factors; estimating population reference distributions of certain health parameters; documenting and investigating reasons for secular trends in selected diseases and risk factors; contributing to an understanding of disease etiology; and investigating the natural history of selected diseases. The NHANES III sample was selected from 81 counties between 1988 and 1994. Approximately 40,000 people >2 months old were selected to be interviewed and have a physical examination in a mobile examination center. Accordi

28
The Centers for Disease Control and Prevention (CDC) has compiled data on diabetes in the United States obtained from several surveys, including the National Health Interview Survey (NHIS), the third National Health and Nutrition Examination Survey (NHANES III), the National Hospital Discharge Survey, and surveys conducted through the Behavioral Risk Factor Surveillance System (BRFSS). Based on data from these sources, the CDC estimates that 17 million people, or 6.2% of the population, had diabetes in 2000. A third of these cases were undiagnosed. Almost 9% of people >20 years old and 20.1% of people >65 years old had diabetes. The estimated worldwide prevalence of diabetes in 1997, derived from World Health Organization (WHO) data, was 124 million people, with the majority (97%) having type 2 diabetes. According to the same projections, the number of people with diabetes is expected to increase to 221 million in 2010. Other less conservative projections by King et al used WHO data combined with demographic estimates and projections issued by the United Nations to place the number of people worldwide with diabetes at 135.3 million in 1995 and 300 million in 2025.
 data, was 124 million people, with the majority (97%) having type 2 diabetes. According to the same projections, the number of people with diabetes is expected to increase to 221 million in Other less conservative projections by King et al used WHO data combined with demographic estimates and projections issued by the United Nations to place the number of people worldwide with diabetes at million in 1995 and 300 million in")
29
Based on data derived from the National Health Interview Survey (NHIS) and the Third National Health and Nutrition Examination Survey (NHANES III), the CDC estimated that in 2000, the percentage of adults with diabetes was 2.5% among 20 to 44 year-olds, 12.1% among 45 to 64 year-olds, 21.6% among 65 to 74 year-olds, and 18.5% among those over 75.
 and the Third National Health and Nutrition Examination Survey (NHANES III), the CDC estimated that in 2000, the percentage of adults with diabetes was 2.5% among 20 to 44 year-olds, 12.1% among 45 to 64 year-olds, 21.6% among 65 to 74 year-olds, and 18.5% among those over 75.")
Presentazioni simili


>")

















