Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
LA DIAGNOSI DI AIDS: DALL’ESPOSIZIONE, ALLA SINTOMATOLOGIA CLINICA,
Collegio Universitario Plinio Fraccaro 25 Novembre 2008 LA DIAGNOSI DI AIDS: DALL’ESPOSIZIONE, ALLA SINTOMATOLOGIA CLINICA, AI TEST DI LABORATORIO Alessia UGLIETTI Ambulatorio HIV/AIDS Clinica Malattie Infettive Fondazione IRCCS Policlinico San Matteo, Pavia

2
SITUAZIONE COMUNE Un collega chiama per riscontro di positività a un test HIV in un paziente COME PROCEDIAMO?

3
Paziente uomo, 44 anni caucasico
VISITA AMBULATORIALE Paziente uomo, 44 anni caucasico Counselling sul test HIV e sulla malattia Fattore di rischio Situazione familiare Occupazione Scrivere cosa si ricava dal paziente e fare animazione

4
MODALITA’ DI TRASMISSIONE
KISSING french or open mouth kissing non rischio evitando ovviamente che al soggetto non sanguinino le gengive Nella saliva, nelle lacroime e sudore presena di virus praticamente nulla: mai capitato. ATTENZIONE che si èparla sempre di sogg inconsapevoli del loro stato sierologico o no in terapia. MORSO UMANO non risultato contagioso: vedre l’esposizione e perdita ematica.

5
Distribuzione percentuale dei casi di AIDS per modalità di trasmissione

6
Età mediana alla diagnosi di infezione da HIV
6

7
Non adottano misure per non trasmettere l’infezione
Impatto sulla Sanità Pubblica dei soggetti inconsapevoli del proprio sierostato HIV Non assumono la terapia (viremia persistente e maggior contagiosità) Non adottano misure per non trasmettere l’infezione L’efficienza di trasmissione è 3.5 volte maggiore tra i non consapevoli (tasso annuo stimato di trasmissione 6.9% versus 2.0%) La trasmissione sessuale potrebbe essere ridotta del 31% se tutti i soggetti fossero consapevoli del loro sierostato G. Marks et al., AIDS, 2006
 Non adottano misure per non trasmettere l’infezione. L’efficienza di trasmissione è 3.5 volte maggiore tra i non consapevoli (tasso annuo stimato di trasmissione 6.9% versus 2.0%) La trasmissione sessuale potrebbe essere ridotta del 31% se tutti i soggetti fossero consapevoli del loro sierostato. G. Marks et al., AIDS,")
8
RISCHIO DI TRASMISSIONE DI HIV PER RAPPORTI SESSUALI NON PROTETTI
TIPI DI RAPPORTO anale recettivo con persone HIV-positive anale recettivo con persone con stato HIV sconosciuto anale insertivo con persona con stato HIV sconosciuto vaginale recettivo vaginale insertivo Sesso orale RISCHIO PER CONTATTO 0.82% ( ) 0.27% ( ) 0.06% ( ) % The risk of HIV transmission is present if an HIV-negative person comes into contact with the blood, semen or vaginal fluids of an HIV-positive source person. But exposure of intact skin to HIV-contaminated body fluids (e.g. blood) is not sufficient to transfer the virus. Rapporti orali sessuali: solo singoli casi sono stati riportati in particolare con liquido spermatico in bocca Transmission is possible if HIV-containing material enters the body by: . accidental needlestick injury or incision by surgical instruments . exposure of damaged skin or mucosal membranes . unprotected sexual intercourse with an infected person . IDU sharing needle or equipment . transfusion of HIV-contaminated blood or blood products HIV is not a very contagious pathogen. The transmission rate after contact is about 1:1000 to 1:100. Compared with HIV, the transmission rate for hepatitis C is 10 times higher, and 100 times higher for hepatitis B. Factors for the probability of transmission are the amount of incorporated virus and the exposure time. Contact with body fluids of a patient with a high viral load supposably holds a higher risk of contagion than a similar contact with body fluids of a patient under HAART with a suppressed viral load. Additionally, quick removal of infectious material e.g. from damaged skin or mucosal membrane by washing or disinfection presumably decreases the risk of an HIV infection. For percutaneous contact with HIV-containing blood, an infectiousness of 0.3 % in total is assumed. % ?
 0.27% ( ) 0.06% ( ) % The risk of HIV transmission is present if an HIV-negative person comes into contact. with the blood, semen or vaginal fluids of an HIV-positive source person. But. exposure of intact skin to HIV-contaminated body fluids (e.g. blood) is not sufficient. to transfer the virus. Rapporti orali sessuali: solo singoli casi sono stati riportati in particolare con liquido spermatico in bocca. Transmission is possible if HIV-containing material enters the body by: . accidental needlestick injury or incision by surgical instruments. . exposure of damaged skin or mucosal membranes. . unprotected sexual intercourse with an infected person. . IDU sharing needle or equipment. . transfusion of HIV-contaminated blood or blood products. HIV is not a very contagious pathogen. The transmission rate after contact is about. 1:1000 to 1:100. Compared with HIV, the transmission rate for hepatitis C is 10. times higher, and 100 times higher for hepatitis B. Factors for the probability of. transmission are the amount of incorporated virus and the exposure time. Contact. with body fluids of a patient with a high viral load supposably holds a higher risk of. contagion than a similar contact with body fluids of a patient under HAART with a. suppressed viral load. Additionally, quick removal of infectious material e.g. from. damaged skin or mucosal membrane by washing or disinfection presumably decreases. the risk of an HIV infection. For percutaneous contact with HIV-containing. blood, an infectiousness of 0.3 % in total is assumed %")
9
MALATTIE SESSUALMENTE TRASMESSE (MST)
HIV epatiti HAV-HBV-HCV sifilide gonorrea Chlamydia trachomatis linfogranuloma venereo Trichomonas cancroide (ulcera molle) condilomi acuminati Hiv è solo una punta delle MST ma ricordiamoci anche di tuttel altre: epatiti, ….lue… Inoltre in caso di infezione MST non trattatta incontrollata c’ è un aumento della possibilità di trasmissione della malattia da HIV Attenzione alla trasmissone verticale da clamidia che può dare al neonato polmoniti e congiuntiviti Haemophlus ducrey per cancroide
 condilomi acuminati. Hiv è solo una punta delle MST ma ricordiamoci anche di tuttel altre: epatiti, ….lue… Inoltre in caso di infezione MST non trattatta incontrollata c’ è un aumento della possibilità di trasmissione della malattia da HIV. Attenzione alla trasmissone verticale da clamidia che può dare al neonato polmoniti e congiuntiviti. Haemophlus ducrey per cancroide.")
10
Human Immunodeficiency Virus (HIV)
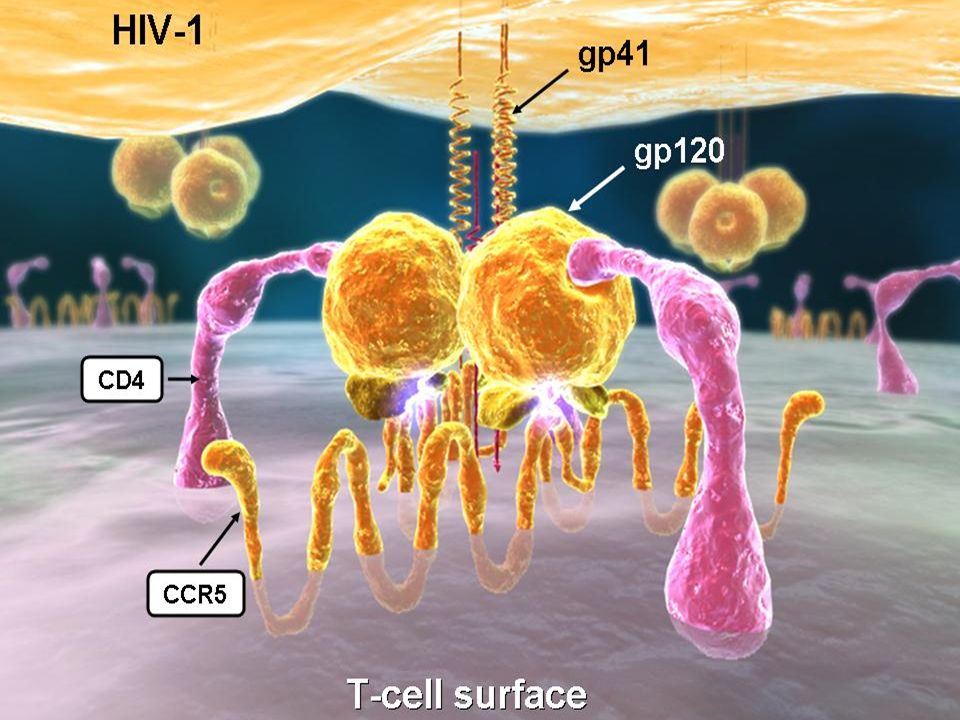
HIV Structure HIV is composed of the following major structural elements: Envelope gp120 gp41 HIV Core Structural proteins p24 2 strands of single stranded RNA Enzymes Reverse transcriptase Integrase Protease HIV-1 is a retrovirus and belongs to the family of lentiviruses. Each viral particle contains 72 glycoprotein complexes, which are integrated into this lipid membrane, and are each composed of trimers of an external glycoprotein gp120 and a transmembrane spanning protein gp41. The p24 core antigen contains two copies of HIV-1 RNA. The HIV-1 RNA is part of a protein-nucleic acid complex, which is composed of the nucleoprotein p7 and the reverse transcriptase p66 (RT). The viral particle contains all the enzymatic equipment that is necessary for replication: a reverse transcriptase (RT), an integrase p32 and a protease p11
. The viral particle contains all the. enzymatic equipment that is necessary for replication: a reverse transcriptase (RT), an integrase p32 and a protease p11.")
11
HIV Lifecycle Il ciclo vitale di HIV lè completato in circa 2 giorni e comprende 6 step chiave 1. Attacco 2. Ingresso 3. Trascrizione Inversa 4. Integrazione 5. Trascrizione e traslazione 6. Assemblamento e gemmazione Ognuno di questi step è essesnziale nel produrre virioni potenzialmente infettanti Gp41, as the transmembrane part of the envelope glycoprotein gp160, is crucial for the fusion of the viral and the host cell membrane. T20 is the first of several peptides that bind to gp41 and has been tested in clinical trials for suppressing viral replication

13
HIV Reservoirs

14
STORIA DEL PAZIENTE Rappresentante di materiale tessile
Coniugato Rappresentante di materiale tessile Fumatore 1 pack/die Fattore di rischio: rapporti eterosessuali non protetti con partner sconosciuta

15
SINTOMATOLOGIA In anamnesi: appendicetomia
negli ultimi 6 mesi calo ponderale di 6 Kg astenia riscontro di ernia inguinale da ridurre chirurgicamente All’esame obiettivo: Lingua impaniata Cuore-polmoni: NDS Addome: fegato a 1cm dall’arco costale Microlinfoadenopatia generalizzata Paziente dopo il ricover e i diversi accertamenti: su che base faccio HIV….sintomatologia HIV…..condiversi quadri…poi ritorno al paziente che no aveva nessun sintomo ma rientrbva infez cronica….test e poi PPE… si scopre HIV pos….nessuna sintomatologia inerente HIV: infezione cronica ma ci possono essere diversi casi: scoperta da altri reparti ina quanto test HIV pre operatorio sembra essere entrato nela routine clinica.

16
INFEZIONE CRONICA AVANZATA
INFEZIONE DA HIV INFEZIONE ACUTA INFEZIONE PRECOCE INFEZIONE CRONICA INFEZIONE CRONICA AVANZATA E non sempre sono così evidenti o ci possono essere Da definire meglio

17
STORIA NATURALE DELL’INFEZIONE DA HIV
Viral load and CD4 T-Cells over time Fase di aids che si verifica in una buona parte di pazienti diagnisticati negli ultimi anni. Ciò che ci permette di inquadrare la malattia sono i due parametri di CD4+ e livello di viremia di virus, oltre il possibile corredo sintomatologico che si accompagna. CD4 e condizioni cliniche determinano la classif cdc

18
Primary HIV Infection: Signs e Symptoms
40-90% of patients will be symptomatic A mononucleosis-like illness of non-specific signs and symptoms Signs and symptoms typically begin 1-4 weeks post-exposure High index of suspicion is critical Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39. Schacker T, et al. Ann Intern Med. 1996;125:

19
SINTOMI DA INFEZIONE ACUTA DA HIV
Rash e/o febbre, solitamente in combinazione con: malessere generale inappetenza perdita di peso faringodinia ulcere orali dolori articolari e/o muscolari linfoadenopatia diarrea nausea/vomito sudorazioni notturne cefalea Alcuni sintomo possono essere simili a una sindrome influenzale, mononucleosi..importante la diagnosi differenziale

20
CLASSIFICAZIONE CDC’ 93 STADIO A e B
Infezione HIV asintomatica Infezione HIV acuta (primaria) Linfoadenopatia persistente generalizzata Stadio B Condizioni sintomatiche che non sono incluse nell’elenco di condizioni dello stadio C: Angiomatosi bacillare Candidiasi, orofaringea (mughetto) Candidiasi, vulvovaginale; persistente, frequente, o scarsamente responsiva alla terapia Displasia cervicale (moderata o grave) / carcinoma cervicale in situ Sintomi costituzionali, come febbre (38.5° C) o diarreamaggiore di un mese Hairy leukoplakia, orale Herpes zoster (shingles), coinvolgendo almeno 2 o più dermatomeri Porpora trombocitopenica idiopatica Listeriosi Malattia infiammatoria pelvica, se complicata da ascesso tuboovarico Neuropatia periferica
 Linfoadenopatia persistente generalizzata. Stadio B. Condizioni sintomatiche che non sono incluse nell’elenco di condizioni dello stadio C: Angiomatosi bacillare. Candidiasi, orofaringea (mughetto) Candidiasi, vulvovaginale; persistente, frequente, o scarsamente responsiva alla terapia. Displasia cervicale (moderata o grave) / carcinoma cervicale in situ. Sintomi costituzionali, come febbre (38.5° C) o diarreamaggiore di un mese. Hairy leukoplakia, orale. Herpes zoster (shingles), coinvolgendo almeno 2 o più dermatomeri. Porpora trombocitopenica idiopatica. Listeriosi. Malattia infiammatoria pelvica, se complicata da ascesso tuboovarico. Neuropatia periferica.")
21
CONDIZIONI CLINICHE AIDS-DEFINENTI CDC’ 93 STADIO C
Candidosi bronchi, trachea o polmoni Candidosi esofagea Carcinoma della cervice invasivo Coccidiomicosi, disseminata o extrapolmonare Criptococcosi extrapolmonare Criptosporidiosi, cronica intestinale (>1mese) Malattia da citomegalovirus (oltre a fegato, milza o linfonodi) Retinite da citomegalovirus (con perdita del visus) Istoplasmosi disseminata o extrapolmonare Isosporiasi cronica intestinale (>1mese) Sarcoma di Kaposi Linfoma di Burkitt Linfoma primario encefalico Mycobacterium avium complex o Mycobacterium Kansasii a localizzazione disseminata o extrapolmonare Mycobacterium tubercolosis qualsiasi localizzazione Polmonite da Pneumocystis carinii Polmonite ricorrente Leucoencefalopatia multifocale progressiva Setticemia da salmonella, ricorrente Toxoplasmosi encefalica Wasting syndrome HIV correlata A common problem among HIV-infected people is the HIV wasting syndrome, defined as unintended and progressive weight loss (10%) all’anno often accompanied by weakness, fever, nutritional deficiencies and diarrhea.
 Malattia da citomegalovirus (oltre a fegato, milza o linfonodi) Retinite da citomegalovirus (con perdita del visus) Istoplasmosi disseminata o extrapolmonare. Isosporiasi cronica intestinale (>1mese) Sarcoma di Kaposi. Linfoma di Burkitt. Linfoma primario encefalico. Mycobacterium avium complex o Mycobacterium Kansasii a localizzazione disseminata o extrapolmonare. Mycobacterium tubercolosis qualsiasi localizzazione. Polmonite da Pneumocystis carinii. Polmonite ricorrente. Leucoencefalopatia multifocale progressiva. Setticemia da salmonella, ricorrente. Toxoplasmosi encefalica. Wasting syndrome HIV correlata. A common problem among HIV-infected people is the HIV wasting syndrome, defined as unintended and progressive weight loss (10%) all’anno often accompanied by weakness, fever, nutritional deficiencies and diarrhea.")
22
CD4+ > 500 cell/ul 1 CD4+ 200-500 cell/ul 2
LINFOCITI T CD4+ CD4+ > 500 cell/ul 1 CD cell/ul 2 CD4+ <200 cell/ul 3

23
QUADRI PATOLOGICI Sarcoma di Kaposi Tubercolosi polmonare
Polmonite da Pneumocystis carinii Toxoplasmosi cerebrale Candidosi esofagea Retinite da citomegalovirus

24
COSA FACCIAMO?

25
TEST HIV Test immunoenzimatico ricombinante (recombinant enzyme linked immunoassay - ELISA) Test di laboratorio standard per screening di HIV, entro 2 ore il risultato. Non distingue fra HIV-1 e HIV-2. Valuta la presrenza degli anticorpi anti-HIV nel siero del paziente Falsi positivi, -negativi e risultati indeterminati sono possibili (ma rari). Alta sensibilità (quasi 100%) e alta specificità 99,5 Deve essere estremamente sensibile per minimizzare i falsi neg.. Se test pos deve essere ripetutio altro test. In most ELISA tests, viral antigen is bound to the so-called solid phase (e.g. on the bottom of the wells in a microtitre plate). Upon addition of patient serum containing antibodies directed specifically against these antigens, antigen-antibody binding will occur. A washing step then removes all unbound constituents of the serum, including all antibodies not recognizing the viral antigen. Un coniugat enzimatico per coniugare gl iAb del paziente.. E se presente ab si forma coniugato e l’enzima determina viraggio del core del pozzetti
. Alta sensibilità (quasi 100%) e alta specificità 99,5. Deve essere estremamente sensibile per minimizzare i falsi neg.. Se test pos deve essere ripetutio altro test. In most ELISA tests, viral antigen is bound to the so-called solid phase (e.g. on the. bottom of the wells in a microtitre plate). Upon addition of patient serum containing. antibodies directed specifically against these antigens, antigen-antibody binding. will occur. A washing step then removes all unbound constituents of the serum, including all antibodies not recognizing the viral antigen. Un coniugat enzimatico per coniugare gl iAb del paziente.. E se presente ab si forma coniugato e l’enzima determina viraggio del core del pozzetti.")
26
TEST HIV Antigene p24 Antigene p24 compare giorni dopo l’esposizione: prima dello sviluppo degli anticorpi anti-HIV Licenziato per la diagnosi di soindrome acuta da HIV – durante il periodo finestra UTILE NELLO SCREENING TRASFUSIONI Oggi combinato in test di IV generazione con Elisa Ab-Ag

27
TEST DI CONFERMA Western Blot
Usato per confermare un test ELISA positivo, eseguito in circa 3 ore. Reazione Ag-Ab Bassa sensibilità, soprattutto in fasi iniziali di infezione maggior tempo Costi maggiori Maggiori falsi-positivi, negativi, e indeterminati rispetto a ELISA Escludere gli errori di laboratorio completamente (campioni mixed up, contaminazione attraverso pipette con materiale positivo) WB valuta reaz ag-Ab la presenza del virus facendo reagire prot migrate su coltura con siero paz x valutare la presenza di ab vrerso quelle prot virali. Recuperare un WB reale e inserirlo con prot analizzate(prot env gp 41, gp 120, gp 160), gag or nuclear prot (p18, p24/p25, p55), pol (p34, p40, p52,p68). Usato sia per HIV 1 e 2. Quando WB è positivo???FDA (p24, p34 e gp41 o gp 120) diverso da WHO recomandation (solo 2 bande di env) The Western blot is a methodology for which HIV is propagated in cell cultures, harvested, purified and denatured (i.e. split into its constituents). The resulting viral proteins are separated according to their molecular weight by electrophoresis and blotted onto a nitrocellulose membrane which is then cut into strips. To perform the test, the membrane is incubated with patient serum. If this contains antibodies against the various viral proteins, they will bind to the areas on the strip onto which the respective antigens have been blotted. This antigen-antibody reaction is revealed using an enzyme-labeled secondary antibody and matching substrate, whereupon the so-called "bands" appear on the test strip.
 WB valuta reaz ag-Ab la presenza del virus facendo reagire prot migrate su coltura con siero paz x valutare la presenza di ab vrerso quelle prot virali. Recuperare un WB reale e inserirlo con prot analizzate(prot env gp 41, gp 120, gp 160), gag or nuclear prot (p18, p24/p25, p55), pol (p34, p40, p52,p68). Usato sia per HIV 1 e 2. Quando WB è positivo FDA (p24, p34 e gp41 o gp 120) diverso da WHO recomandation (solo 2 bande di env) The Western blot is a methodology for which HIV is propagated in cell cultures, harvested, purified and denatured (i.e. split into its constituents). The resulting viral. proteins are separated according to their molecular weight by electrophoresis and. blotted onto a nitrocellulose membrane which is then cut into strips. To perform the. test, the membrane is incubated with patient serum. If this contains antibodies. against the various viral proteins, they will bind to the areas on the strip onto which. the respective antigens have been blotted. This antigen-antibody reaction is revealed. using an enzyme-labeled secondary antibody and matching substrate, whereupon the so-called bands appear on the test strip.")
28
Western Blot indeterminato
4-20% of reactive ELISAs; usually due to single p24 band Subsequent pregnancy, blood transfusion, HIV vaccine, organ transplantation, autoantibodies from collagen vascular ds., influenzae vaccine, HIV-2 HIV viral load negative confirms false positive

29
OraQuick Advance HIV-1/2
TEST RAPIDI OraQuick Advance HIV-1/2 Conservato a temperatura ambiente Screening per HIV-1 e 2 Resultati in 20 minuti Divesri tipi di test rapidi che potrebbero essere usati in pronto socc, prima di operazioni, in caso di puntura accindentale con ago. Però rischio di alcni test è di avere bassa sensibilità perciò rischio di risultati falsi neg maggiori C’è u test con saliva con possibilità di rilevare HIV1 e 2 con sensibilità del 99,3% e specificità del 99,9% Immunoglobulins may also be eluted from blood spots blotted onto filter paper and dried (Lillo 1992). Such dried blood spots from routinely obtained Guthrie cards are used for the unlinked anonymous screening of newborn babies (whose antibody prevalence mirrors that of their mothers) (Peckham 1990) and in developing countries with insufficient cold storage and transport facilities. Once completely dry, blood from HIV-infected patients does not constitute an infection risk and is stable over long time periods. Urine or oral fluid (oral transudate, often incorrectly referred to as "saliva") may also be employed for some assays (Tamashiro 1994, King 2000). The FDA licensed a rapid HIV test marketed by OraSure Technologies for use with oral fluid in 2004. According to available information this assay allows the detection of antibodies against HIV-1 or HIV-2 with a sensitivity of 99.3 % and a specificity of 99.9 %. Under certain conditions, only such non-blood specimen types make testing possible (non-invasive sampling). However, their sensitivities and specificities are mostly considerably lower. Therefore, blood remains the preferred type of specimen. Whatever type of sample is used, a reactive test result of course requires confirmatory testing.
. Such dried blood spots from routinely obtained Guthrie cards are. used for the unlinked anonymous screening of newborn babies (whose antibody. prevalence mirrors that of their mothers) (Peckham 1990) and in developing countries. with insufficient cold storage and transport facilities. Once completely dry, blood from HIV-infected patients does not constitute an infection risk and is stable. over long time periods. Urine or oral fluid (oral transudate, often incorrectly referred to as saliva ) may. also be employed for some assays (Tamashiro 1994, King 2000). The FDA licensed. a rapid HIV test marketed by OraSure Technologies for use with oral fluid in According to available information this assay allows the detection of antibodies. against HIV-1 or HIV-2 with a sensitivity of 99.3 % and a specificity of 99.9 %. Under certain conditions, only such non-blood specimen types make testing possible. (non-invasive sampling). However, their sensitivities and specificities are. mostly considerably lower. Therefore, blood remains the preferred type of specimen. Whatever type of sample is used, a reactive test result of course requires confirmatory. testing.")
30
Obtain finger stick specimen…

31
Collect oral fluid specimens by swabbing gums with test device.
Gloves optional; waste not biohazardous

32
Uni-Gold Recombigen TEST RAPIDI Conservato a temperatura ambiente
Screening per HIV-1 e 2 Resultati in 10 minuti

33
PERIODO FINESTRA HIV antibody WINDOW PERIOD 10,000,000 1,000,000
HIV RNA (cp/ml) HIV antibody 1,000,000 100,000 10,000 { Days } 1,000 WINDOW PERIOD This time interval, the serologic "window period," is characterized by seronegativity, occasionally detectable antigenemia, viremia (as measured by RNA), and variable CD4 lymphocyte levels. Detection of specific antibody to HIV signals the end of the window period and labels the individual as seropositive. The switch from antibody-negative to antibody-positive is called "seroconversion". The screening tests currently used are able to recognize an HIV infection six weeks after primary infection in about 80 % and after the 12th week in almost 100 % of cases; only in very rare cases is an infection recognized only after six months. 4th generation screening assays attempt to shorten the duration of the "diagnostic window" by detecting HIV antibodies and HIV p24 antigen simultaneously Early during seroconversion the antibody screening test will be only borderline or weakly reactive. A Western blot carried out for confirmation may at this stage not show any bands at all or an incomplete band pattern, with the p24 band often the first to become visible. IMPORTANTE ANHE LE INFORMAZIONI CLINICHE 100 10
 HIV antibody. 1,000, , ,000. { Days ---} 1,000. WINDOW PERIOD. This time interval, the serologic window period, is characterized by seronegativity, occasionally detectable antigenemia, viremia (as measured by RNA), and variable CD4 lymphocyte levels. Detection of specific antibody to HIV signals the end of the window period and labels the individual as seropositive. The switch from antibody-negative to antibody-positive is called. seroconversion . The screening tests currently used are able to recognize an HIV. infection six weeks after primary infection in about 80 % and after the 12th week in. almost 100 % of cases; only in very rare cases is an infection recognized only after. six months. 4th generation screening assays attempt to shorten the duration of the diagnostic. window by detecting HIV antibodies and HIV p24 antigen simultaneously. Early during seroconversion the antibody screening test will be only borderline or. weakly reactive. A Western blot carried out for confirmation may at this stage not. show any bands at all or an incomplete band pattern, with the p24 band often the. first to become visible. IMPORTANTE ANHE LE INFORMAZIONI CLINICHE")
34
NAT (HIV nucleic acid testing)
HIV RNA rilevato anche nelle prime 2 settimane PCR (Polymerase Chain Reaction ) qualitativa o quantitativa branched-DNA (b-DNA) nucleic acid sequence-based amplification (NASBA) Esistono due tipi di test PCR per l'HIV: la PCR quantitativa, per misurare la viremia o carica virale, cioè per misurare quante copie virali ci sono nell'unità di volume di sangue, e la PCR qualitativa che, invece, si limita soltanto a rilevare la presenza del materiale genetico del virus. Anche se quest'ultimo test, rispetto al primo, non opera una quantificazione, in caso di possibile esposizione all'HIV, per stabilire se sia avvenuto il contagio, si preferisce utilizzare la PCR qualitativa, poiché quella quantitativa, a volte, dà luogo a false positività, per cui è meglio utilizzarla solo in caso di contagio già precedentemente accertato. Occorre inoltre notare che, mentre con la PCR qualitativa si può identificare o l'HIV-DNA provirale o HIV-RNA virale, la PCR quantitativa determina il numero di copie per unità di volume di HIV-RNA. NASBA PER AMPLIFICARE TRASCRITTASI, BRANCHED PER IL PROVIRALE Viral RNA can be detected within the first 2 weeks using the highly sensitive RT-PCR method. An HIV infection may also be diagnosed through the detection of virus, rather than indirectly through the detection of antibodies. However, virus detection is only necessary in certain situations such as suspected primary infection and to test babies born to HIV-infected mothers. The detection of viral nucleic acid (i.e. of virus genome) may be achieved by different laboratory techniques, to detect either proviral cDNA in leucocytes (EDTA whole blood) or viral RNA in the cell-free compartment (EDTA plasma or EDTA whole blood). Various commercial and "in house" methods are available for NAT. These are based on polymerase chain reaction (PCR), branched DNA (b-DNA), nucleic acid sequence-based amplification (NASBA), ligase chain reaction (LCR), or real-time PCR. These assays are generally demanding in terms of laboratory equipment, staff skills etc., require stringent quality control, and are cumbersome, relatively errorprone and expensive. Qualitative testing for viral genome serves as a marker of infection. It supplements antibody testing for the diagnosis of HIV infection in special situations (suspected primary infection: absence of antibodies during the diagnostic window; newborn of infected mother: presence of maternal antibodies . also see below). The risk of HIV transmission through blood transfusion has decreased enormously through careful selection of donors . to exclude people with potential risk factors for blood-borne viral infections (besides HIV mainly hepatitis B and C) . and through donor screening. Several countries now stipulate HIV NAT in addition to using antibody testing.
 qualitativa o quantitativa. branched-DNA (b-DNA) nucleic acid sequence-based amplification (NASBA) Esistono due tipi di test PCR per l HIV: la PCR quantitativa, per misurare la viremia o carica virale, cioè per misurare quante copie virali ci sono nell unità di volume di sangue, e la PCR qualitativa che, invece, si limita soltanto a rilevare la presenza del materiale genetico del virus. Anche se quest ultimo test, rispetto al primo, non opera una quantificazione, in caso di possibile esposizione all HIV, per stabilire se sia avvenuto il contagio, si preferisce utilizzare la PCR qualitativa, poiché quella quantitativa, a volte, dà luogo a false positività, per cui è meglio utilizzarla solo in caso di contagio già precedentemente accertato. Occorre inoltre notare che, mentre con la PCR qualitativa si può identificare o l HIV-DNA provirale o HIV-RNA virale, la PCR quantitativa determina il numero di copie per unità di volume di HIV-RNA. NASBA PER AMPLIFICARE TRASCRITTASI, BRANCHED PER IL PROVIRALE. Viral RNA can be detected within the first 2 weeks using the highly sensitive RT-PCR method. An HIV infection may also be diagnosed through the detection of virus, rather than. indirectly through the detection of antibodies. However, virus detection is only necessary. in certain situations such as suspected primary infection and to test babies. born to HIV-infected mothers. The detection of viral nucleic acid (i.e. of virus genome) may be achieved by different. laboratory techniques, to detect either proviral cDNA in leucocytes (EDTA. whole blood) or viral RNA in the cell-free compartment (EDTA plasma or EDTA. whole blood). Various commercial and in house methods are available for NAT. These are. based on polymerase chain reaction (PCR), branched DNA (b-DNA), nucleic acid. sequence-based amplification (NASBA), ligase chain reaction (LCR), or real-time. PCR. These assays are generally demanding in terms of laboratory equipment, staff. skills etc., require stringent quality control, and are cumbersome, relatively errorprone. and expensive. Qualitative testing for viral genome serves as a marker of infection. It supplements. antibody testing for the diagnosis of HIV infection in special situations (suspected. primary infection: absence of antibodies during the diagnostic window; newborn of. infected mother: presence of maternal antibodies . also see below). The risk of HIV transmission through blood transfusion has decreased enormously. through careful selection of donors . to exclude people with potential risk factors. for blood-borne viral infections (besides HIV mainly hepatitis B and C) . and. through donor screening. Several countries now stipulate HIV NAT in addition to. using antibody testing.")
35
INQUADRAMENTO DEL PAZIENTE HIV-POSITIVO
Test HIV ELISA e Western Blot POSITIVI ESENZIONE PER PATOLOGIA emocromo e biochimica completa (fegato, rene, lipidi, elettroliti profilo linfocitario + HIV RNA branched test di resistenza e clade esame urine sierologie epatiti A, B e C sierologia sifilide sierologia toxoplasmosi, citomegalovirus, EBV Rx torace + ECG Mantoux

36
Counselling e HIV/AIDS

37
….E ORA? TEST HIV ALLA MOGLIE POSITIVO NEGATIVO COUNSELLING
VITA DI COPPIA INQUADRAMENTO DEL PAZIENTE RIPETERE TEST HIV DOPO 1, 3, 6 MESI E SUCCESSIVAMENTE 1 VOLTA ALL’ANNO

38
PROCEDIAMO… Moglie NEGATIVA
Paziente inizia una HAART e dopo 1 mese viene valutato con visita ambulatoriale ed esami ematici MA…. Dottoressa……AIUTO!! mi sono bucata con l’ago del paziente XY!!!!!

39
Profilassi Postesposizione dopo esposizione al virus HIV
DHHS raccomandano di iniziare prontamente una PEP con HAART quando la persona sia venuta a contatto con il virus entro le 72 ore, che la fonte di contatto sia certamente HIV-positiva, e che l’esposizione presenti un rischio effettivo di trasmissione MMWR January 21, 2005 / 54(RR02);1-20
;1-20.")
40
Profilassi Postesposizione
Esposizione di vagina, retto, occhio, bocca, cute non intatta, o contatto percutaneo con sangue, liquido spermatico, secrezioni vaginali latte materno, o qualunque altro fluido corporeo con presenza di sangue MMWR January 21, 2005 / 54(RR02);1-20
;1-20.")
41
Nel caso della nostra infermiera

42
Algoritmo per eventuale PPE occupazionale e non in esposizione ad HIV
Esposizione al rischio effettivo Esposizione al rischio irrilevante <72 ore dall’esposizione >72 ore dall’esposizione Soggetto fonte HIV-positivo Soggetto fonte con HIV sconosciuto PEP raccomandata Determinare caso per caso PEP non raccomandata MMWR January 21, 2005 / 54(RR02);1-20
;1-20.")
43
Regime standard per PPE HIV
2 NRTI tenofovir + lamivudina o emtricitabina zidovudina + lamivuina PI lopinavir/ritonavir Early reports on the use of AZT after occupational needlestick injuries date from 1989. An analysis of retrospective case-control studies shows that even prophylaxis with a single substance after exposure reduces the probability of an infection by approximately 80 % (Tokars 1993). The combination of multiple drugs is supposedly even more potent. Unfortunately there have been transmissions despite the use of PEP. Transmission of HIV infection cannot always be prevented. Many of the described cases of PEP failure were treated with AZT mono-prophylaxis. But there are also reports about failures of antiretroviral combination therapies. PEP should be initiated as soon as possible, preferably within hours rather than days of exposure. If a question exists concerning which antiretroviral drugs to use, or whether to use a basic or expanded regimen, the basic regimen should be started immediately rather than delay PEP administration. The optimal duration of PEP is unknown. Because 4 weeks of ZDV appeared protective in occupational and animal studies, PEP should be administered for 4 weeks, if tolerated. The risks of PEP mainly concern the adverse effects of the antiretroviral substances, most frequently gastrointestinal symptoms such as nausea, vomiting or diarrhea. Changes of hematology, transaminases or creatinine are also possible. Additionally, there have been reports of elevated triglycerides and cholesterol levels, and insulin resistance even in short term use of protease inhibitors (Parkin 2000). 4 settimane MMWR September 30, 2005 / 54(RR09);1-17
. The combination of multiple drugs is supposedly. even more potent. Unfortunately there have been transmissions despite the use. of PEP. Transmission of HIV infection cannot always be prevented. Many of the. described cases of PEP failure were treated with AZT mono-prophylaxis. But there. are also reports about failures of antiretroviral combination therapies. PEP should be initiated as soon as possible, preferably within hours rather than days of exposure. If a question exists concerning which. antiretroviral drugs to use, or whether. to use a basic or expanded regimen, the basic regimen should be started. immediately rather than delay PEP. administration. The optimal duration of PEP is unknown. Because 4 weeks of ZDV appeared protective in occupational and animal studies, PEP should be administered for 4 weeks, if tolerated. The risks of PEP mainly concern the adverse effects of the antiretroviral substances, most frequently gastrointestinal symptoms such as nausea, vomiting or diarrhea. Changes of hematology, transaminases or creatinine are also possible. Additionally, there have been reports of elevated triglycerides and cholesterol levels, and insulin. resistance even in short term use of protease inhibitors (Parkin 2000). 4 settimane. MMWR September 30, 2005 / 54(RR09);1-17.")
44
CONTROLLO PPE FOLLOW UP
ematochimici a 2 settimane e alla fine della PPE test HIV ELISA a 1, 3, 6 mesi dalla fine della profilassi se sospetto di infezione acuta eseguire NAT Controllare gli esami ematochimici dell’infermieraa 2 settimane e alla fine della PEP, valutare se sopporta la trapia e raccomandarsi di eseguire test HIV un mese dopo la fine della PEP, a 3 mesi e a 6 mesi…eseguire un test di HIV rNA soo in caso di sopsetto di infezione acuta Ovviamente oltre all’HIV, considerare anche epatiti…B e C. NON DIMENTICARE LE EPATITI

45
Dottoressa, vorremmo avere un figlio sano…come facciamo??
DOPO 1 ANNO E MEZZO XY, in terapia antiretrovirale con HIV RNA soppresso malattia controllata Siamo davanti a una comune situazione di coppia discordante….. Dottoressa, vorremmo avere un figlio sano…come facciamo??

46
DESIDERIO DI GRAVIDANZA
Tecniche di riproduzione assistita se maschio infetto lavaggio della sperma con FIVET o inseminazione intra-uterina se femmina infetta auto-inseminazione/ riproduzione assistita se entrambi infetti riproduzione assistita Inseminazione da donatore sano Adozione After sperm washing and testing for HIV, spermatozoa can be utilized in three different reproductive techniques depending on whether the couples have any additional fertility issues: intra-uterine insemination (IUI), extracorporal fertilization by conventional in-vitro fertilization (IVF). The success rate using IUI has been shown to be reduced if the sperm is washed and then cryopreserved before use. Rapporti sessuali non protetti uomo HIV-positivo soppresso virologicamente
, extracorporal fertilization by. conventional in-vitro fertilization (IVF). The success rate using IUI has been shown to. be reduced if the sperm is washed and then cryopreserved before use. Rapporti sessuali non protetti uomo HIV-positivo soppresso virologicamente.")
47
No transmission if VL « undetectable »
All Men-Women Women-Men No transmission if VL « undetectable » Studio ugandese « Rakai » Study: Transmission risk as a function of viral load Quinn et al. N Engl J Med 2000;342:921-9 47

48
Concepimento naturale in coppie discordanti
62 couples Infected partners with undetectable viremia Non-protected sex, in principal only during fertile days 78 pregnancies at term No HIV transmission Barreiro P et al. Natural Pregnancies in HIV-Serodiscordant Couples Receiving Successful Antiretroviral Therapy. J Acquir Immune Defic Syndr 2006;43:324–326. 48

49
QUANDO FINALMENTE VERRA’ SCOPERTO IL VACCINO PER L’HIV?

50
IL VERO VACCINO ESISTE GIA’ !

Presentazioni simili





.>")

>")











