Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Quali opzioni gestionali e farmacologiche se il paziente peggiora ?
Valentino Moretti San Daniele d.F.

2
Benchè la maggioranza dei pazienti rispondano alla terapia medica alcuni non migliorano o sperimentano una rapida ricorrenza di sintomi. Questi pazienti hanno sintomi a riposo o al minimo sforzo e richiedono ospedalizzazioni prolungate.

3
CONGESTIONE PERFUSIONE DRY WARM WET COLD
(ortopnea, congestione venosa centrale, rantoli, reflusso epato-giugulare, ascite, edemi periferici) PERFUSIONE (pressione arteriosa, polso alternante, ipotensione sintomatica, vasocostrizione periferica, deterioramento mentale) DRY WARM WET COLD Steveson, J Am Coll Cardiol 2003;41:1797
 PERFUSIONE. (pressione arteriosa, polso alternante, ipotensione sintomatica, vasocostrizione periferica, deterioramento mentale) DRY. WARM. WET. COLD. Steveson, J Am Coll Cardiol 2003;41:1797.")
4
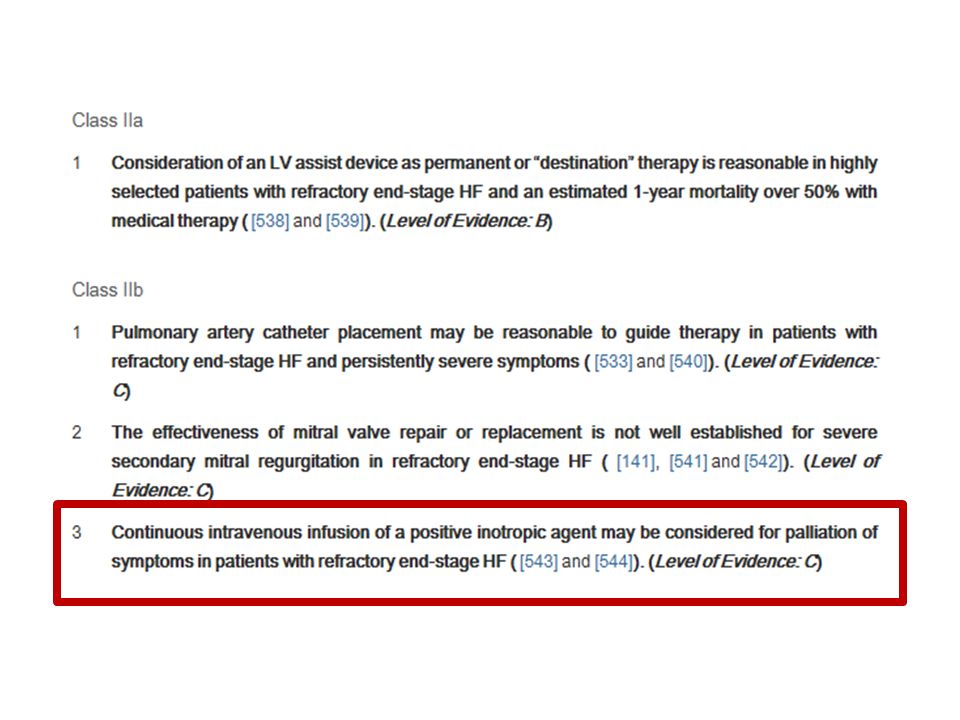
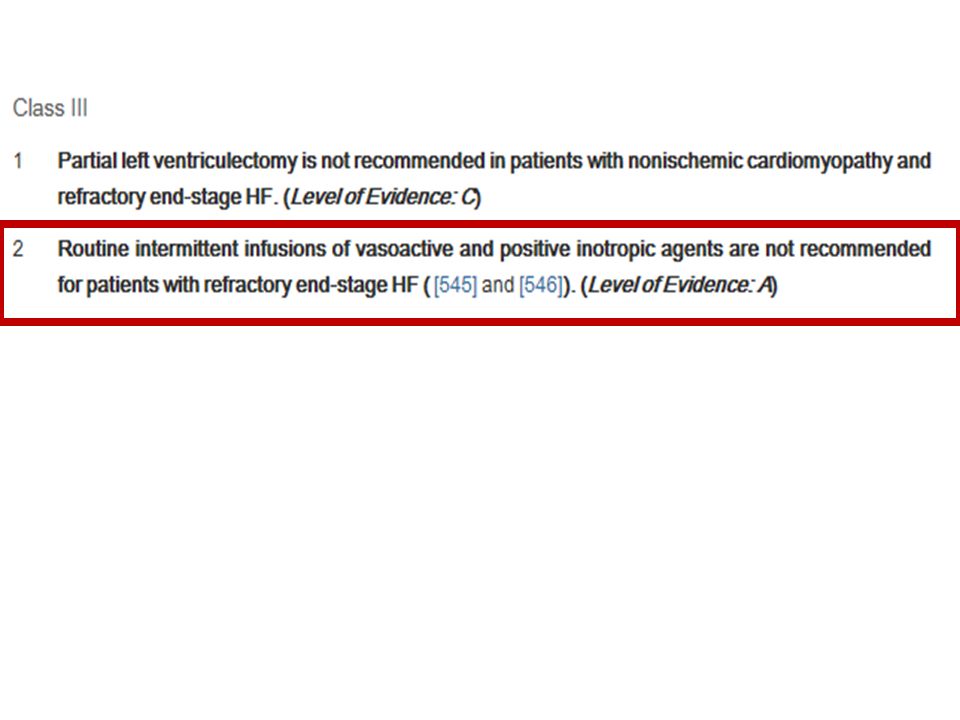
* terapia con inotropi e.v. * ultrafiltrazione
* terapia con diuretici e.v. * terapia con inotropi e.v. * ultrafiltrazione * terapia di resincronizzazione * supporto meccanico * trapianto * terapie sperimentali

5
49% little or no Weight Loss 16% no change or gain in Body Weight
ADHERE Registry All Enrolled Discharges from October 2001 to January 2004 Change in weight was assessed in 51,013 patient episodes Discharged Home (including home with additional and/or outpatient care) 49% little or no Weight Loss 7% 6% 13% 24% 33% 11% 3% 2% 5 10 15 20 25 30 (<-20) (-20 to -15) (-15 to -10) (-10 to -5) (-5 to 0) (0 to 5) (5 to 10) (>10) Change in Weight (lbs) 16% no change or gain in Body Weight Enrolled Discharges Among patients admitted to the hospital with a primary diagnosis of acute heart failure, 16% lose no weight or gain some weight during hospitalization. The inability to adequately diurese patients reflects a failure of “standard therapy,” which consists to a large extent of diuretics as monotherapy. RAAS activation secondary to diuretics can lead to renal vasoconstriction and reduced GFR and sodium reabsorption between doses of diuretics. Both of the above confer diuretic “resistance.”
 49% little or no Weight Loss. 7% 6% 13% 24% 33% 11% 3% 2% (<-20) (-20 to -15) (-15 to -10) (-10 to -5) (-5 to 0) (0 to 5) (5 to 10) (>10) Change in Weight (lbs) 16% no change or gain in Body Weight. Enrolled Discharges. Among patients admitted to the hospital with a primary diagnosis of acute heart failure, 16% lose no weight or gain some weight during hospitalization. The inability to adequately diurese patients reflects a failure of standard therapy, which consists to a large extent of diuretics as monotherapy. RAAS activation secondary to diuretics can lead to renal vasoconstriction and reduced GFR and sodium reabsorption between doses of diuretics. Both of the above confer diuretic resistance.")
6
Perché quasi la metà dei pazienti ricoverati con ADHF non perde peso ?
.

7
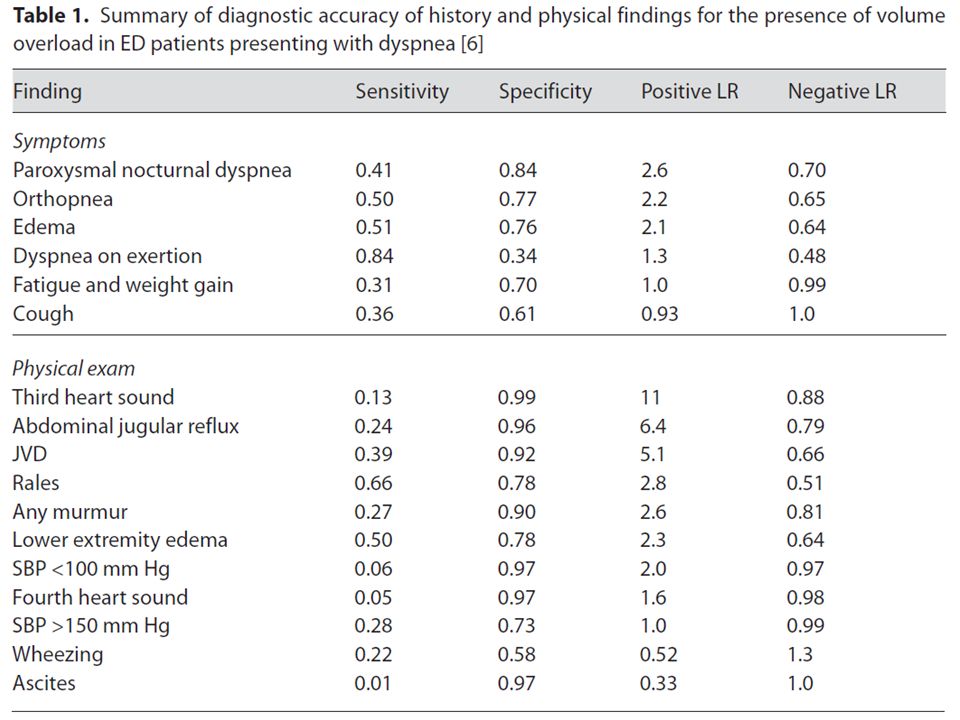
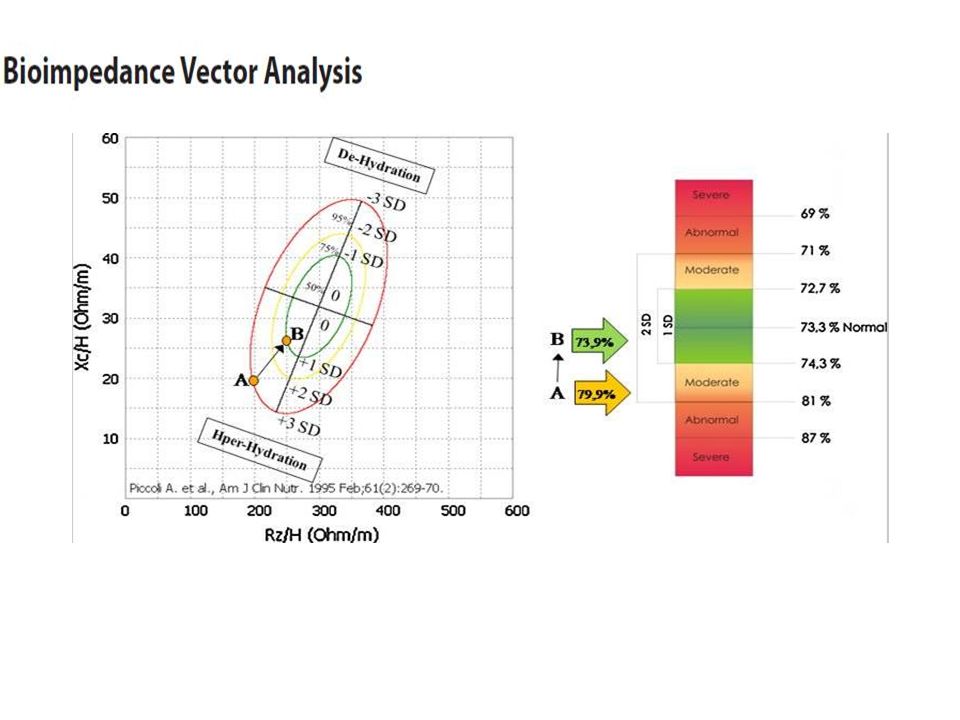
E’così facile valutare il sovraccarico di liquidi ?

9
Il gold standard : radioisotopi
BNP Impedenzometria B lines ( ultrasuoni ) Dimensioni della cava inferiore ( ultrasuoni )
 Dimensioni della cava inferiore ( ultrasuoni )")
11
Cause di resistenza ai diuretici
Ipoproteinemia Ipotensione Inibizione diretta FANS ACE/ARB Tolleranza Attivazione neuroormonale Dose inadeguata Non Compliance Farmaci non assunti Elevata introduzione di NaCl Assorbimento Secrezione IRC Età Farmaci FANS

12
La resistenza ai diuretici può essere superata da
terapia endovenosa ( in infusione continua ? ) diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso renale ultrafiltrazione
 diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso. renale. ultrafiltrazione.")
13
IV Loop Diuretics: Bolus vs. Continuous Infusion
Rudy DW et al. Ann Intern Med 1991; 115:360 Metanalysis: Continuous Infusion Superior to Bolus Injection: Total UO P = 0.003 Increase in Sr. Creatinine P < Length of Hospitaliization All Cause Mortality P = Salvador DRK et al. The Cochrane Database of Systematic Reviews 2005, Issue 3. Art. No.: CD pub3. DOI: / CD pub3.

16
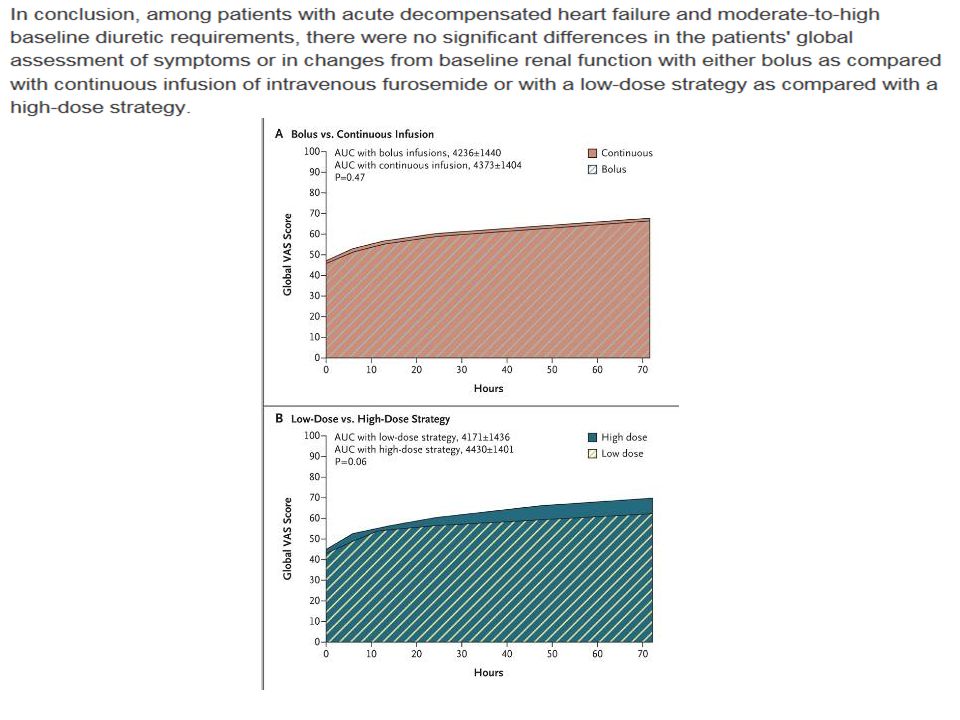
IMPLICAZIONI DEL TRIAL
The DOSE trial has importantly identified a lack of greater benefit with the diuretic regimen of continuous infusion — a regimen that is used frequently — than with a regimen of intermittent boluses. It also showed that, despite theoretical concerns and the findings of prior observational studies, a high dose of loop diuretics, as compared with a low dose, did not substantially worsen renal function. Both of these findings should change current practice. Since a high-dose regimen may relieve dyspnea more quickly without adverse effects on renal function, that regimen is preferable to a low-dose regimen. Administration of boluses may be more convenient than continuous infusion and equally effective.

17
La resistenza ai diuretici può essere superata da
terapia endovenosa ( in infusione continua ? ) diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso renale ultrafiltrazione
 diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso. renale. ultrafiltrazione.")
18
Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Ann Intern Med 1991; 114: First, nephron segments downstream from the site of diuretic action increase sodium-chloride (NaCl) reabsorption because the delivered NaCl load increases. Second, diuretic-induced contraction of the extracellular fluid volume stimulates kidney tubules to retain NaCl until the next dose of diuretic is administered. Third, kidney tubules themselves may become hypertrophic because they are chronically stimulated by diuretic-induced increases in NaCl delivery. These adaptations all increase the rate of NaCl reabsorption and blunt the effectiveness of diuretic therapy. When diuretic resistance is present, using a second diuretic drug that acts in a different nephron segment is often effective
 reabsorption because the delivered NaCl load increases. Second, diuretic-induced contraction of the extracellular fluid volume stimulates kidney tubules to retain NaCl until the next dose of diuretic is administered. Third, kidney tubules themselves may become hypertrophic because they are chronically stimulated by diuretic-induced increases in NaCl delivery. These adaptations all increase the rate of NaCl reabsorption and blunt the effectiveness of diuretic therapy. When diuretic resistance is present, using a second diuretic drug that acts in a different nephron segment is often effective.")
19
Sede di azione dei diversi tipi di diuretico
FIGURE 23-3 Sites of action of diuretics in the kidney. AVP = arginine vasopressin.

20
La resistenza ai diuretici può essere superata da
terapia endovenosa ( in infusione continua ? ) diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso renale ultrafiltrazione
 diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso. renale. ultrafiltrazione.")
23
La resistenza ai diuretici può essere superata da
terapia endovenosa ( in infusione continua ? ) diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso renale ultrafiltrazione
 diuretici in combinazione ( es furosemide/metolazone ) uso di diuretici e farmaci che incrementano il flusso. renale. ultrafiltrazione.")
24
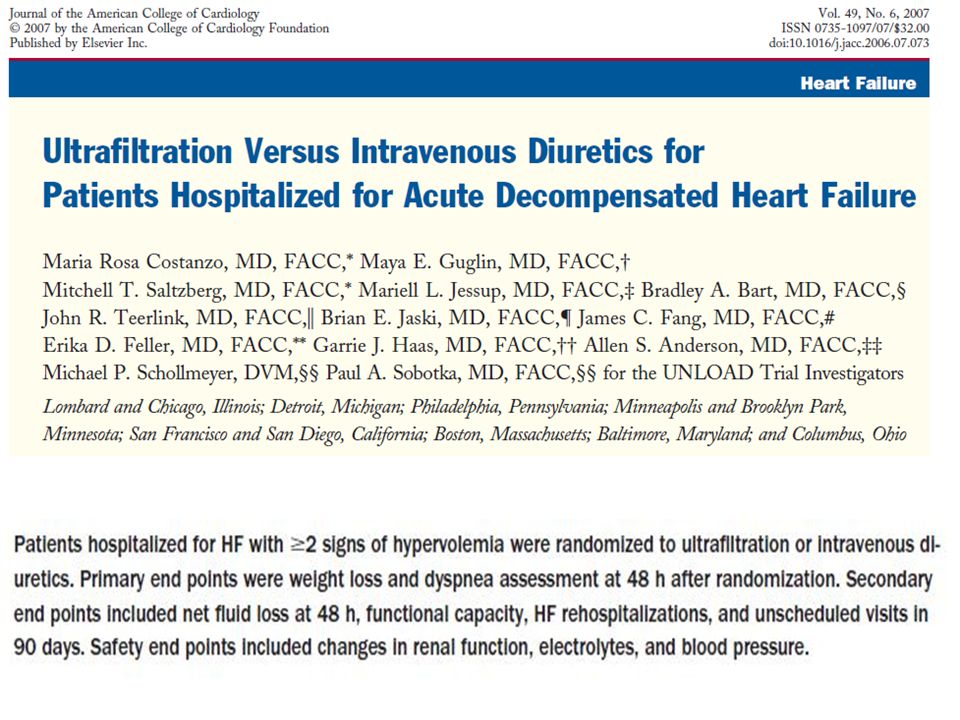
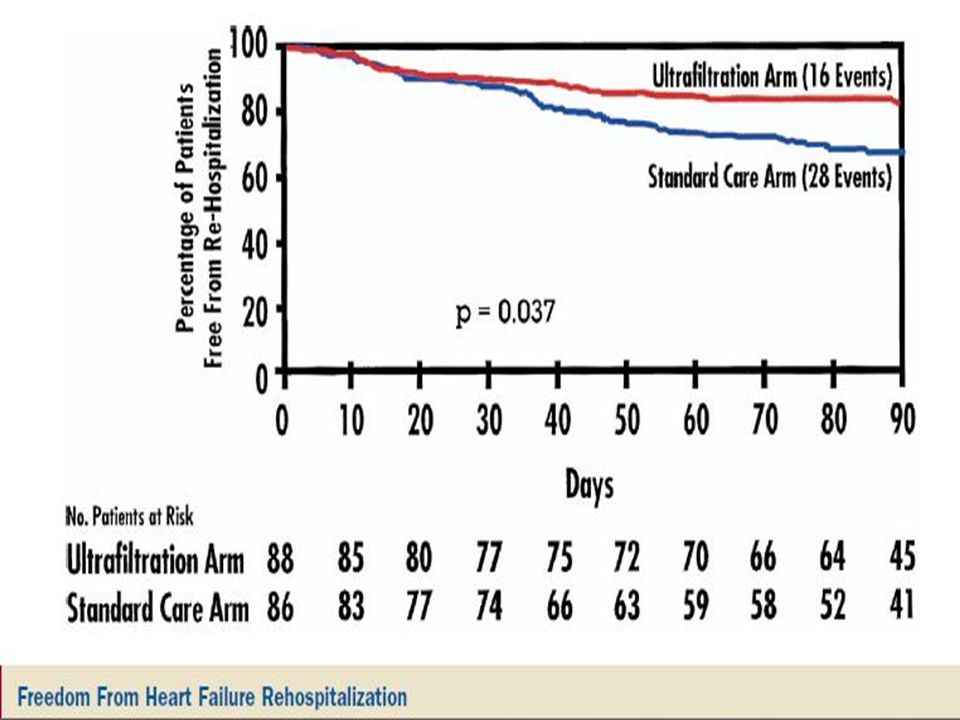
Fluid Removal by Ultrafiltration
Section 4: Ultrafiltration History and Physiology Fluid Removal by Ultrafiltration Interstitial Space (Edema) Ultrafiltration can remove fluid from the blood at the same rate that fluid can be naturally recruited from the tissue The transient removal of blood elicits a compensatory mechanism, called plasma or intravascular refill (PR), aimed at minimizing this reduction1,2 Na P H2O Na K UF K PR The plasma refill (PR) response is a compensatory response by the circulation in response to volume loss.1 The rate of plasma refill is important, for if the ultrafiltration rate is too aggressive intravascular volume may decrease because the rate of refill from the interstitial to the intravascular space is exceeded. This in turn may lead to hemodynamic instability and renal dysfunction. There have been studies that document an increase in creatinine and hemodynamic instability when ultrafiltration rates are too aggressive in a high-risk, advanced HF subset of patients,2 and thus the clinician should be aware of this risk. References: 1. Marenzi et al. J Am Coll Cardiol. 2001;38:4. 2. Liang KV et al. J Card Fail. 2006;12: P Na Vascular Space Vascular Space Na 1. Lauer et al. Arch Intern Med. 1983;99: 2. Marenzi et al. J Am Coll Cardiol. 2001;38:4.
 Ultrafiltration can remove fluid from the blood at the same rate that fluid can be naturally recruited from the tissue. The transient removal of blood elicits a compensatory mechanism, called plasma or intravascular refill (PR), aimed at minimizing this reduction1,2. Na. P. H2O. Na. K. UF. K. PR. The plasma refill (PR) response is a compensatory response by the circulation in response to volume loss.1 The rate of plasma refill is important, for if the ultrafiltration rate is too aggressive intravascular volume may decrease because the rate of refill from the interstitial to the intravascular space is exceeded. This in turn may lead to hemodynamic instability and renal dysfunction. There have been studies that document an increase in creatinine and hemodynamic instability when ultrafiltration rates are too aggressive in a high-risk, advanced HF subset of patients,2 and thus the clinician should be aware of this risk. References: 1. Marenzi et al. J Am Coll Cardiol. 2001;38:4. 2. Liang KV et al. J Card Fail. 2006;12: P. Na. Vascular. Space. Vascular. Space. Na. 1. Lauer et al. Arch Intern Med. 1983;99: Marenzi et al. J Am Coll Cardiol. 2001;38:4.")
28
Il mondo reale

29
Primo DRG Età media 80 anni Assenza tecnologia Comorbidità IRC > 50%

30
Il mondo reale Oltre 80 anni ? Diuretici e.v.
Dobutamina/dopamina – furosemide Ultrafiltrazione : occasionale Oltre 80 anni ? Resincronizzazione ICD

31
Il mondo reale Percorsi con MMG Aspetti gestionali follow up
ambulatorio dedicato Post acuzie RSA Hospice Percorsi con MMG

Presentazioni simili






 devices receive FDA approval annually 3500 medium-risk (class II) products are approved for marketing.>")


>")









