Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Scompenso cardiaco e sindromi correlate: non trascuriamo lo “sleep disorder”
Michele Emdin, Claudio Passino U.O. Medicina Cardiovascolare Fondazione Toscana Gabriele Monasterio Istituto di Fisiologia Clinica CNR, Pisa Scuola Superiore Sant’Anna Congresso tosco-umbro FIC Montecatini Terme, 14 novembre 2007

2
60 sec. 1 2 3 4 5 6 7 8 9 30 sec. Cheyne, J. “A case of Apoplexy, in Which the Fleshy Part of the Heart Was Converted into Fat.” Dublin Hospital Reports, 1818, II, 216. “…For several days his breathing was irregular; it would entirely cease for a quarter of minute, then it would become perceptible, though very low, then by degrees it became heaving and quick, and then it would gradually cease again: this revolution in the state of his breathing occupied about a minute during which there were about thirty acts of respiration...” I have little doubt that this was a case of weakened and probably fatty heart, with disease of the aorta…” …of a patient with probable cardiac asthma: Stokes, W. “Observations on some Cases of permanently slow Pulse.” Dublin Quart. Jour. Med. Sc.,1846,II, “…Then a very feeble, indeed barely perceptible inspiration would take place, followed by another somewhat stronger, until at length high heaving, and even violent breathing was established, which would then subside till the next period of suspension… This was frequently a quarter of minute in duration

3
POLYSOMNOGRAPHY

4
% 100* 34 * 20* 75 * 450# Chronic heart failure: PREVALENCE
of Cheyne-Stokes Respiration and Obstructive Apneas % 100* 34 * 20* 75 * 450# NB OA CSR Creteil 1994 Toronto 1999 Cincinnati 2005 Grenoble 1999 Melbourne 1999 * prospective # retrospective

5
Chronic heart failure: PREVALENCE
of Cheyne-Stokes Respiration and Obstructive Apneas 679 patients 5 studies 44% NB AB OA 56% CSR 16% 40%

6
Sleep characteristics - 81 HF patients
Minutes * * * Javaheri S Ital. Circulation : 2154

7
Sleep characteristics - 81 HF patients
Sleep efficiency Arousal/h Javaheri S Ital. Circulation : 2154

8
Andamento temporale su un’epoca di 12 min della potenza dell’EEG nelle bande caratteristiche in un soggetto con scompenso cardiaco senza respiro di Cheyne-Stokes. Andamento temporale su un’epoca di 12 min della potenza dell’EEG nelle bande caratteristiche in un soggetto con scompenso cardiaco con respiro di Cheyne-Stokes.

9
Analisi tramite algoritmo GSTFT
Rappresentazione tempo-frequenza del segnale EEG (C4 –A1) in un soggetto con scompenso cardiaco e respiro di Cheyne-Stokes
 in un soggetto con scompenso cardiaco e respiro di Cheyne-Stokes.")
10
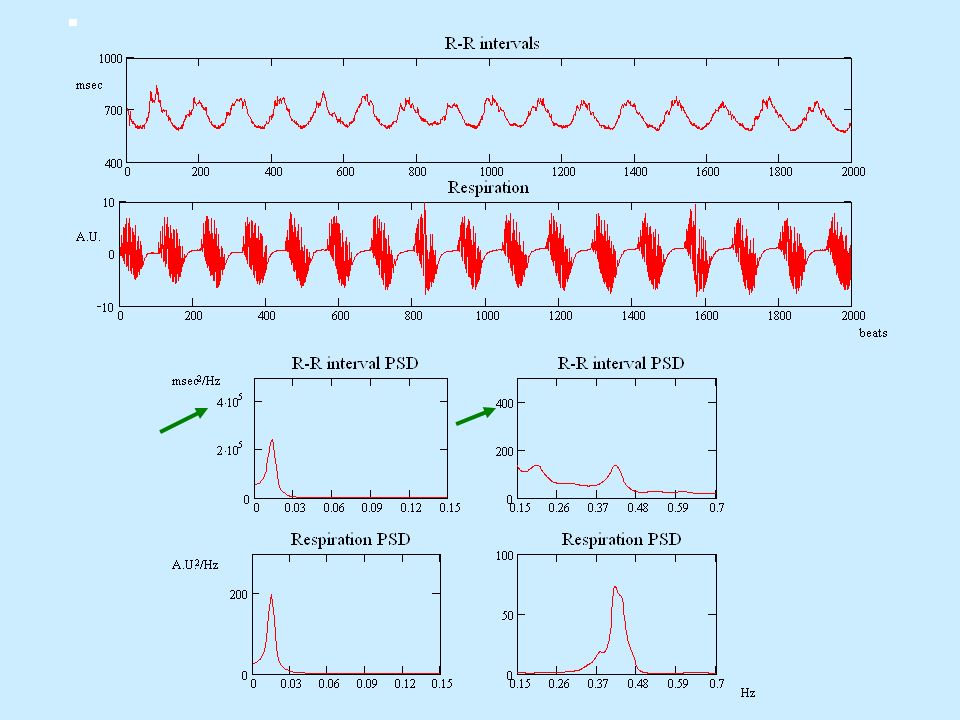
REGISTRAZIONE CARDIORESPIRATORIA BREVE
METODI REGISTRAZIONE CARDIORESPIRATORIA BREVE CHF patient

11
Prevalence of day-time CSR/PB: Pisa Prevalence in previous studies:
85 pts CSR/PB + 65 pts 57% 43% Prevalence in previous studies: - Mortara et al, Circulation 1997: CSR/PB - 64% pts - Ponikowski et al, Circulation 1999: CSR/PB - 66% pts

12
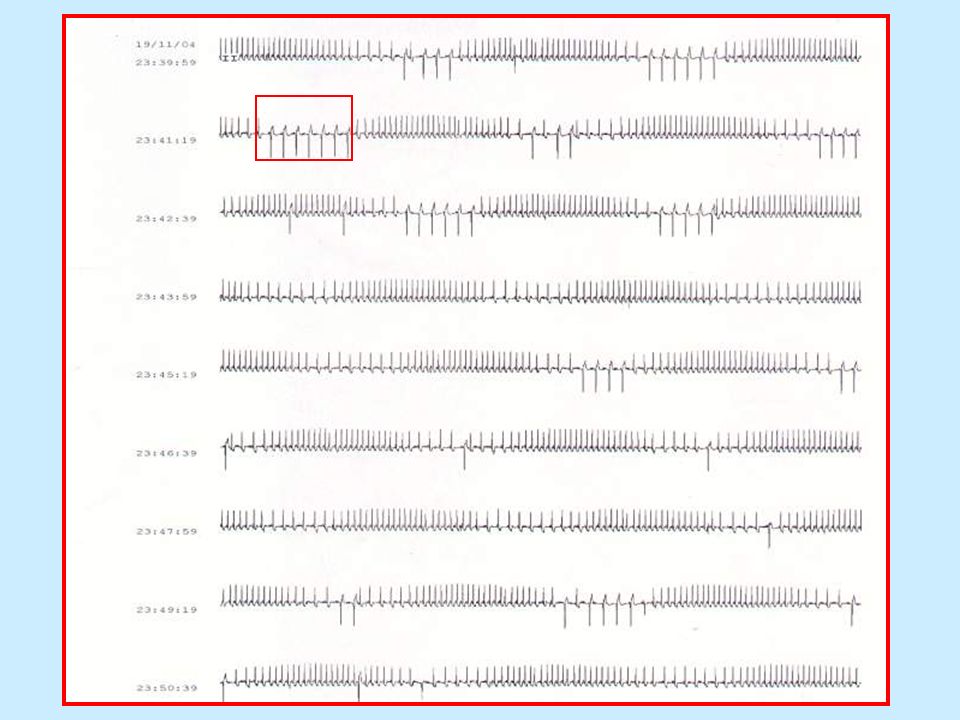
REGISTRAZIONE CARDIORESPIRATORIA AMBULATORIALE
METODI REGISTRAZIONE CARDIORESPIRATORIA AMBULATORIALE

13
REGISTRAZIONE CARDIORESPIRATORIA AMBULATORIALE

14
Effetti clinici del respiro di CS
Cicli di desaturazione arteriosa Ipossia disfunzione d’organo/danno endoteliale, vasocostrizione polmonare Iperattivazione simpatica Diretta Indiretta in risposta all’ipossia Effetti emodinamici (prevalentemente indiretti) FC, vasocostrizione Aumento del post-carico e del lavoro cardiaco Effetti sulla variabilità della FC e PA
 FC, vasocostrizione. Aumento del post-carico e. del lavoro cardiaco. Effetti sulla variabilità della FC e PA.")
15
Effetti clinici del respiro di CS

19
NEURO-HORMONAL IMBALANCE IN HEART FAILURE
LV BNP ANP system activation >>> - baroreflex ergo-chemoreflex Sympathetic RAA DYSFUNCTION - Na H20 retention – vasoconstriction arrhythmogenesis tissue ischaemia dyspnoea oedema arrhythmias sudden death fatigue

20
Cheyne-Stokes e Mortalità nello SCC
16 pazienti con SCC severo in fase di stabilità clinica età media 64 aa, FE < 35% CSR 9/16 (AHI 41± 17 vs 6 ± 5) Hanly PJ, Am J Resp Crit C M 1996;153:272
 Hanly PJ, Am J Resp Crit C M 1996;153:272.")
21
Valore prognostico del CS notturno nello SCC
62 pz con FE < 35%, NYHA II-III P Lanfranchi et al, Circulation 1999; 99:1435

22
Valore prognostico RP/CS durante la veglia
MT LA Rovere et al., Eur Heart J 2003;

23
Cheyne-Stokes Respiration during exercise in CHF:
impact on PROGNOSIS 60 sec. Exercise Recovery 6 7 8 9 1 10 20 30 0.8 0.6 0.4 0.2 p=0.0001 AHI > 30 / hour AHI < 30 / hour months proportion surviving AHI = apnea-hypopnea index EOV AHI > 30 / hour + EOV Corrà, Circulation 2006 .

24
Pathogenesis of CSR in CHF: hypotheses
Central (?) Hypocapnic (?!) “Instability loop” (!) - increased chemosensitivity - prolonged circulation time
 Hypocapnic ( !) Instability loop (!) - increased chemosensitivity. - prolonged circulation time.")
25
Ipotesi periferica- ipersensibilità chemocettoriale
Variazioni di PaCO2 Risposta ventilatoria eccessiva PaCO2 sotto la soglia apneica Apnea PaCO2 Ripresa ventilazione

26
Hypoxic Ventilatory Response
SaO2 (%) VE/MIN (L/min) R= -0.87, p<0.001 Slope = 5 6 7 8 9 10 11 12 13 14 15 16 80 82 84 86 88 90 92 94 96 98 100 HVR slope Hypoxic Ventilatory Response 1050 RR interval ms 700 30 Minute Ventilation L/min 90 PET CO2 mmHg 100 Sa O2 % 65 6 TIME (min)
 VE/MIN (L/min) R= -0.87, p< Slope = HVR slope. Hypoxic Ventilatory Response RR interval. ms Minute Ventilation. L/min. 90. PET CO2. mmHg Sa O2. % TIME (min)")
27
HypercapnicVentilatory Response
R = 0.93, p<0.001 Slope = 1.001 6 8 10 12 14 16 18 20 36 38 40 42 44 46 48 50 52 VE/MIN (L/min) HCVR slope Pet CO2 HypercapnicVentilatory Response 1050 RR interval ms 700 30 Minute Ventilation L/min 90 PET CO2 mmHg 100 Sa O2 % 65 6 TIME (min)
 HCVR slope. Pet CO2. HypercapnicVentilatory Response RR interval. ms Minute Ventilation. L/min. 90. PET CO2. mmHg Sa O2. % TIME (min)")
28
* † Normal chemoreflex Increased HVR Prevalence of diurnal CSR (%)
HCVR HVR+HCVR 5 10 15 20 Nocturnal apnea-hypopnea index * † Giannoni A, Emdin M, Poletti R, Bramanti F, Prontera C, Piepoli M, Passino C. Clinical significance of chemosensitivity in chronic heart failure: influence on neurohormonal derangement, Cheyne-Stokes respiration and arrhythmias. Clin Sci (Lond) Oct 26; [Epub ahead of print]
 Oct 26; [Epub ahead of print]")
29
peakVO2 VE/VCO2 slope NB CS NB CS ** * ml/min/kg
* p<0.05, ** p<0.01 Giannoni A, Emdin M, et al.. Clin Sci (Lond) Oct 26; [Epub ahead of print]
 Oct 26; [Epub ahead of print]")
30
NB CS NB CS NB CS NorEPI BNP NT-proBNP pg/ml ** *** ***
Giannoni A, Emdin M, et al.. Clin Sci (Lond) Oct 26; [Epub ahead of print]
 Oct 26; [Epub ahead of print]")
31
Multivariate Analysis
CO2-sensitivity and BNP level are independent predictors of CSR (also considering O2-sensitivity, peak VO2, VE-VCO2 slope, norepinephrine, NT-proBNP from univariate analysis)
")
32
CO2-sensitivity and BNP as predictors of CSR
HCVR slope Sensitivity AUC 0.93 P<0.001 BNP AUC 0.89 P<0.001 Specificity

33
CSR chemoceptors Norepi BNP, ANP hypoxia LV dysfunction altered
haemodynamics

34
NEURO-HORMONAL IMBALANCE IN HEART FAILURE
LV BNP ANP system activation >>> - baroreflex ergo-chemoreflex Sympathetic RAA DYSFUNCTION - Na H20 retention – vasoconstriction arrhythmogenesis tissue ischaemia dyspnoea oedema arrhythmias sudden death fatigue

35
CSR in CHF: therapeutical target?
60 sec. CSR in CHF: therapeutical target? Why? To improve respiratory pattern To improve sleep quality/QOL To improve cardiac performance To improve prognosis (?) When? Which patient? Which marker (daytime abnormalities, PSG-AHI, BNP, …)? How?
 When Which patient Which marker (daytime abnormalities, PSG-AHI, BNP, …) How")
36
Ottimizzare la terapia per CHF. un trattamento specifico
60 sec. Diagramma del trattamento del respiro di Cheyne Stokes nello scompenso cardiaco Scompenso cardiaco con respiro di Cheyne-Stokes Ottimizzare la terapia per CHF. (farmaci, CRT) Assenza di Cheyne-Stokes Cheyne-Stokes persiste Considerare un trattamento specifico O2 terapia Metilxantine CPAP o altri device (Trapianto Cardiaco)
 Assenza di. Cheyne-Stokes. Cheyne-Stokes. persiste. Considerare. un trattamento specifico. O2 terapia. Metilxantine. CPAP o altri device. (Trapianto Cardiaco)")
37
N Engl J Med 2005;353:

38
Grazie per l’attenzione!

39
NYHA CLASS LVEF NB CS NB CS * * % * p<0.05
Giannoni A, Emdin M, et al.. Clin Sci (Lond) Oct 26; [Epub ahead of print]
 Oct 26; [Epub ahead of print]")
40
Effect of Theophylline on Sleep-Disordered Breathing in Heart Failure
S. Javaheri et al. NEJM August 22,1996 n8 335: Protocollo dello studio: 15 pz con scompenso cardiaco e disturbi della respirazione notturni (AHI > 10/ora). Somministrazione orale di Teofillina o placebo 2 volte die per 5 gg con una settimana di washout fra i due periodi. Risultati: Significativa riduzione degli episodi di apnea/ipopnea rispetto al placebo: Placebo 37 Teofillina 47 18 Possibili meccanismi della Teofillina: Competizione a livello centrale con il sito recettoriale dell’Adenosina (depressore respiratorio) Incremento del deficit ventilatorio polmonare restrittivo associato allo scompenso cardiaco Effetto inotropo
. Somministrazione orale di Teofillina o placebo 2 volte die per 5 gg con una settimana di washout fra i due periodi. Risultati: Significativa riduzione degli episodi di apnea/ipopnea rispetto al placebo: Placebo 47 37. Teofillina 47 18. Possibili meccanismi della Teofillina: Competizione a livello centrale con il sito recettoriale dell’Adenosina (depressore respiratorio) Incremento del deficit ventilatorio polmonare restrittivo associato allo scompenso cardiaco. Effetto inotropo.")
41
Analisi tramite algoritmo GSTFT
Rappresentazione tempo-frequenza del segnale EEG (C4 –A1) in un soggetto con scompenso cardiaco senza respiro di Cheyne-Stokes
 in un soggetto con scompenso cardiaco senza respiro di Cheyne-Stokes.")
42
Bi-level PAP may fit the abnormal breathing
pattern of CSR-CSA better than CPAP. Therefore, bi-level PAP improves an abnormal breathing pattern more immediately and effectively than CPAP. In a recent study, it has been reported that 57% of patients showed no response to CPAP

43
PRO CONTRO 15 pz con OSA e PM bicamerale AHI in ritmo spontaneo: 28
Benefit of Atrial Pacing in Sleep Apnea Syndrome NEJM February 7, 2002 n 6, 346: Stephane Garrigue, M.D., Philippe Bordier, M.D., Pierre Jaïs, M.D., Dipen C. Shah, M.D., Meleze Hocini, M.D., Chantal Raherison, M.D., Manuel Tunon De Lara, M.D., Michel Haïssaguerre, M.D., and Jacques Clementy, M.D. 15 pz con OSA e PM bicamerale AHI in ritmo spontaneo: 28 AHI in ritmo elettroindotto 11 (P<0.001) PRO CONTRO
 PRO. CONTRO.")
45
Increased long-term mortality in heart failure due to sleep apnoea is not yet proven
T. Roebuck1, P. Solin1, D.M. Kaye2,4, P. Bergin2, M. Bailey3 and M.T. Naughton1 Eur Respir J May; 23: CHF-N CHF-OSA CHF-CSA 78 pazienti LVEF 19.9 ± 7.2% PCP 16.5 ± 8.3 mmHg

46
Effetti clinici del respiro di CS
Cicli di desaturazione arteriosa Ipossia disfunzione d’organo/danno endoteliale, vasocostrizione polmonare Iperattivazione simpatica Diretta Indiretta in risposta all’ipossia Effetti emodinamici (prevalentemente indiretti) FC, vasocostrizione
 FC, vasocostrizione.")
47
Overall CO2 sensitivity vs
adrenergic activation and ventilatory efficiency 70 10000 R=0.322 P<0.05 R=0.549 P<0.001 60 1000 50 NEPI (pg/ml) VE-VCO2 SLOPE 40 100 30 10 20 0.0 0.5 1.0 1.5 2.0 2.5 0.0 0.5 1.0 1.5 2.0 2.5 CO2 SENSITIVITY CO2 SENSITIVITY
 VE-VCO2 SLOPE CO2 SENSITIVITY. CO2 SENSITIVITY.")
48
Overall CO2 sensitivity B-type Natriuretic Peptides
vs B-type Natriuretic Peptides 70 10000 R=0.411 P<0.01 R=0.549 P<0.001 R=0.400 P<0.01 R=0.322 P<0.05 60 1000 50 BNP (pg/ml) NT-proBNP (pg/ml) 40 100 30 20 10 0.0 0.5 1.0 1.5 2.0 2.5 0.0 0.5 1.0 1.5 2.0 2.5 CO2 SENSITIVITY CO2 SENSITIVITY
 NT-proBNP (pg/ml) CO2 SENSITIVITY. CO2 SENSITIVITY.")
49
CONCLUSIONS CSR is predicted by: CSR is associated with:
Enhanced chemoceptive sensitivity to O2 and CO2 Symptom severity and systolic dysfunction Functional capacity and ventilatory efficiency Adrenergic activation BNP/NT-proBNP levels CSR is predicted by: Enhanced chemoceptive sensitivity to CO2 BNP plasma level

Presentazioni simili





 is a disease state characterized by airflow limitation that is not fully reversible. The.>")




>")





>")



