Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Diabete mellito Iperglicemia cronica Alterazione del metabolismo di carboidrati, grassi e proteine Deficit relativo o assoluto della secrezione insulinica e/o dell’azione insulinica

2
... ... Le azioni dell’insulina
Le azioni dell’insulina ... riduce la concentrazione di glucosio nel sangue Inibizione della gluconeogenesi Incremento della glicolisi aumento dell’uptake del glucosio ... stimola l’immagazzinamento del glucosio come Glicogeno (fegato e muscoli) come Trigliceridi (tessuto adiposo)
 come Trigliceridi (tessuto adiposo)")
3
... ... Le azioni dell’insulina stimola l’immagazzinamento degli
Le azioni dell’insulina ... stimola l’immagazzinamento degli Aminoacidi inibisce proteolisi ... favorisce l’accumulo dei trigliceridi attivazione LPL periferiche stimolo della sintesi degli acidi grassi Inibizione della lipolisi

4
— Etiologic classification of diabetes mellitus
I. Type 1 diabetes* (ß-cell destruction, usually leading to absolute insulin deficiency) A. Immune mediated B. Idiopathic II. Type 2 diabetes* (may range from predominantly insulin resistance with relative insulin deficiency to a predominantly secretory defect with insulin resistance) III. Other specific types IV. Gestational diabetes mellitus (GDM) Patients with any form of diabetes may require insulin treatment at some stage of their disease. Such use of insulin does not, of itself, classify the patient.
 A. Immune mediated. B. Idiopathic. II. Type 2 diabetes* (may range from predominantly insulin resistance with relative insulin deficiency to a predominantly secretory defect with insulin resistance) III. Other specific types. IV. Gestational diabetes mellitus (GDM) Patients with any form of diabetes may require insulin treatment at some stage of their disease. Such use of insulin does not, of itself, classify the patient.")
5
Malattia autoimmunitaria
IL DIABETE MELLITO quadro riepilogativo Tipo 1 Tipo 2 Diabete giovanile Diabete adulto Trattamento Insulina Dieta e/o antidiabetici orali e/o insulina Età di esordio < 30 anni > 30 anni (di solito) Sovrappeso No Sì Corpi chetonici Sì No Legame genetico Forte Molto forte Malattia autoimmunitaria Sì No
 Sovrappeso. No. Sì. Corpi chetonici. Sì. No. Legame genetico. Forte. Molto forte. Malattia autoimmunitaria. Sì. No.")
6
... ... Il diabete mellito di tipo 2 è una malattia frequente:
rappresenta circa l’85% di tutti i casi di diabete ... si manifesta spesso negli obesi e nei sovrappeso

7
Criteri per la diagnosi di Diabete Mellito American Diabetes Association 2007
1) Sintomi di diabete più riscontro casuale di concentrazione plasmatica di glucosio ≥ 200 mg/dL (11,1 mmol/L). Riscontro casuale significa qualsiasi momento della giornata . I classici sintomi del diabete includono: poliuria, polidipsia, perdita di peso inspiegata. oppure 2) Valori di glicemia plasmatica a digiuno ≥ 126/dL controllati almeno due volte (7,0 mmol/L). Digiuno significa non aver introdotto calorie da almeno 8 ore. 3) Glicemia plasmatica a 2 ore ≥ 200 mg/dL durante curva da carico di glucosio (questo test deve essere seguito come descritto dall’WHO: 75 g glucosio sciolto in acqua).
 Sintomi di diabete più riscontro casuale di concentrazione plasmatica di glucosio ≥ 200 mg/dL (11,1 mmol/L). Riscontro casuale significa qualsiasi momento della giornata . I classici sintomi del diabete includono: poliuria, polidipsia, perdita di peso inspiegata. oppure. 2) Valori di glicemia plasmatica a digiuno ≥ 126/dL controllati almeno due volte (7,0 mmol/L). Digiuno significa non aver introdotto calorie da almeno 8 ore. 3) Glicemia plasmatica a 2 ore ≥ 200 mg/dL durante curva da carico di glucosio (questo test deve essere seguito come descritto dall’WHO: 75 g glucosio sciolto in acqua).")
8
Fasting plasma glucose
FPG < 100 mg/dl (5.6 mmol/L) = normal fasting glucose; FPG mg/dl ( mmol/L) = IFG (impaired fasting glucose); FPG ≥ 126 mg/dl (7 mmol/L) = provisional diagnosis of diabetes. American Diabetes Association 2007 Sindrome eterogenea caratterizzata da:
 = normal fasting glucose; FPG mg/dl ( mmol/L) = IFG (impaired fasting glucose); FPG ≥ 126 mg/dl (7 mmol/L) = provisional diagnosis of diabetes. American Diabetes Association Sindrome eterogenea caratterizzata da:")
9
OGTT Glicemia dopo 2 h (durante OGTT) <140 mg/dl (7.8 mmol/L) = normal fasting glucose; Glicemia dopo 2 h (durante OGTT) mg/dl ( mmol/L) = IGT (impaired glucose tolerance); Glicemia dopo 2 h (durante OGTT) ≥ 200 mg/dl (11.1 mmol/L) = provisional diagnosis of diabetes American Diabetes Association 2007
 mg/dl ( mmol/L) = IGT (impaired glucose tolerance); Glicemia dopo 2 h (durante OGTT) ≥ 200 mg/dl (11.1 mmol/L) = provisional diagnosis of diabetes. American Diabetes Association")
10
Progressione da normale tolleranza glucidica, ad alterata tolleranza glucidica, a diabete mellito tipo 2 JAMA 2007

11
Prevalence of Diabetes among U.S. Adults, BRFSS, 1990
4% 4-6% 6% n/a Mokdad et al., Diabetes Care 23: , 2000

12
Prevalence of Diabetes among U.S. Adults, BRFSS, 1997-98
4% 4-6% 6% n/a Mokdad et al., Diabetes Care 23: , 2000

14
BMI WHO, 1998 < 18.5 underweight 18.5-25 normalweight 25-30
overweight 25-30 obesity > 30 morbid obesity >40

15
Relative Risk for Type 2 Diabetes Mellitus
male health professionals, 40 to 75 years of age, without diagnosed diabetes 12 years of follow-up van Dam et al, 2002

16
Relation between BMI and the Relative Risk of disease in men
W Willett et al, 1999

17
Visceral, central, android or “apple distribution”
Intermediate type distribution Subcutaneous, peripheral, gynoid or “pear distribution” Outline of three obese women with approximately the same BMI, but differing in pattern of fat distribution

18
Overweight Waist Hip Obesity

19
Women >88 cm-increased risk
Waist circumference is a surrogate marker of visceral fat Lean et al, 1998 Women >88 cm-increased risk Men >102 cm-increased risk

20
La clinica del diabete: le complicanze croniche
1. COMPLICANZE CARDIOVASCOLARI 2. COMPLICANZE NERVOSE 3. COMPLICANZE OCULARI 4. COMPLICANZE NEFROUROGENITALI 5. COMPLICANZE A CARICO DI ALTRI APPARATI

21
COMPLICANZE CARDIOVASCOLARI
CARDIOPATIA ISCHEMICA: rischio di coronaropatia > 2 v nei maschi 3 v femmine. Manifestazioni: angina pectoris, IMA, aritmia, morte improvvisa; insuff.cardiaca congestizia. Non rari episodi ischemici senza dolore per la coesistente neuropatia che può causare anche turbe del ritmo e conduzione. CARDIOMIOPATIA DIABETICA: insuff. cardiaca congestizia in assenza di alterazioni significative dei vasi coronarici (lesioni microvascolari). DENERVAZIONE CARDIACA: neuropatia autonomica che si manifesta con tachicardia (interessamento vagale). Denervazione totale (rara) porta a gravi aritmie e arresto cardiaco. ARTERIOPATIA PERIFERICA: 10 v >della popolazione non diabetica. Processi ateromatosi prediligono le arterie di medio calibro: claudicatio intermittens che si complica con disturbi trofici (ulcera, gangrena). Coesistenza di microangiopatia e suscettibilità alle infezioni (piede diabetico) con possibile focolai di osteomielite. Con neuropatia (ipoanestesia termodolorifica) il pz non avverte i traumatismi anche minimi. IPERTENSIONE ARTERIOSA: più frequente nel pz diabetico, correla con l’insulinoresistenza e la conseguente iperinsulinemia.
. DENERVAZIONE CARDIACA: neuropatia autonomica che si manifesta con tachicardia (interessamento vagale). Denervazione totale (rara) porta a gravi aritmie e arresto cardiaco. ARTERIOPATIA PERIFERICA: 10 v >della popolazione non diabetica. Processi ateromatosi prediligono le arterie di medio calibro: claudicatio intermittens che si complica con disturbi trofici (ulcera, gangrena). Coesistenza di microangiopatia e suscettibilità alle infezioni (piede diabetico) con possibile focolai di osteomielite. Con neuropatia (ipoanestesia termodolorifica) il pz non avverte i traumatismi anche minimi. IPERTENSIONE ARTERIOSA: più frequente nel pz diabetico, correla con l’insulinoresistenza e la conseguente iperinsulinemia.")
22
MORTALITA’ CARDIOVASCOLARE NEL DIABETICO E NEL NON DIABETICO
(Haffner et al, 1998) _ 50 _ 40 _ 30 Incidenza cumulativa in 7 anni (%) _ 20 _ 10 _ Non diabetici Diabetici Senza precedente infarto Con precedente infarto Dati aggiustati per sesso ed età
 _. 50. _. 40. _. 30. Incidenza cumulativa in 7 anni (%) _. 20. _. 10. _. Non diabetici. Diabetici. Senza precedente infarto. Con precedente infarto. Dati aggiustati per sesso ed età.")
23
1-year Survival Post- Hospital 1-year Survival Post- Hospital
High Impact of Diabetes on Mortality at First Myocardial Infarction: FINMONICA n=3,442 n=620 87% 1-year Survival Post- Hospital 74% 1-year Survival Post- Hospital 8% 28-day-1-year mortality 28-day mortality Out-of-hospital sudden cardiac death 18% 4% 9% 23% n=145 20% n=685 Miettinen H, et al. Diabetes Care. 1998;21:69-75.

24
COMPLICANZE NERVOSE Sistema nervoso periferico La neuropatia si manifesta nel 10% dei diabetici (sia 1 che 2) dopo anni di malattia ed è dovuta a degenerazione assonica. Mononeuropatia:più rara, dovuta a lesioni microangiopatiche. Interessamento asimmetrico e prossimale, prevalentemente motorio. Spesso sono coinvolti i nervi cranici (oculomotori). Polineuropatia: più frequente. Interessamento simmetrico, distale, con coinvolgimento dei nervi somatici e viscerali. Insorge più tardivamente con andamento lento e progressivo. Si sviluppano prevalentemente alterazioni sensitive quali dolori, parestesie, iperestesie.
 dopo anni di malattia ed è dovuta a degenerazione assonica. Mononeuropatia:più rara, dovuta a lesioni microangiopatiche. Interessamento asimmetrico e prossimale, prevalentemente motorio. Spesso sono coinvolti i nervi cranici (oculomotori). Polineuropatia: più frequente. Interessamento simmetrico, distale, con coinvolgimento dei nervi somatici e viscerali. Insorge più tardivamente con andamento lento e progressivo. Si sviluppano prevalentemente alterazioni sensitive quali dolori, parestesie, iperestesie.")
25
Questa sintomatologia è in genere preceduta da ipoareflessia osteotendinea, ipoanestesia vibratoria e termodolorifica (pianta del piede). La neuropatia autonomica può interessare sia il parasimpatico che l’ortosimpatico. La neuropatia simpatica comporta assenza di tachicardia e sudorazione riflesse così che episodi di ipoglicemia non sono avvertiti dal paziente. Sistema nervoso centrale Tia, ictus cerebri, trombosi od emorragia o mielopatia vascolare.

26
COMPLICANZE OCULARI RETINOPATIA: la più frequente complicanza oculare del diabete si divide in due fasi: Background:100% dei casi dopo anni di malattia Forma proliferativa: 30-40% dei casi. Bilaterale, microaneurismi, dilatazione ed aumento della permeabilità vasale, emorragie, successivamente lesioni essudative con aspetto “cotonoso” fino alla riduzione dell’acuità visiva per maculopatia. Nella forma proliferante compaiono vasi neoformati che possono causare vaste emorragie preretiniche, successivamente si può avere fibrosi con distacchi di retina. La neovascolarizzazione dell’angolo irido-corneale può determinare glaucoma. CATARATTA: più frequente nel diabetico, è bilaterale. Insorge in caso di cattivo controllo metabolico ed è dovuta ad abnorme accumulo di sorbitolo. ALTRE: cheratopatia, paresi dei muscoli oculomotori, atrofia ottica, patologia infettiva degli annessi oculari. Cecità nel 2% diabetici

27
COMPLICANZE NEFROUROGENITALI
NEFROPATIA DIABETICA: caratterizzata dalla glomerulosclerosi di Kimmmelstiel-Wilson: ispessimento della membrana basale glomerulare ed espansione mesangiale. Si classifica in 5 stadi: I: aumento del GFR, con microalbuminuria e nefromegalia (regressione col compenso metabolico). II: progressione del danno renale III:microalbuminuria persistente IV: ↓ GFR , con ipertensione arteriosa V: insuff renale terminale. ALTRE: pielonefriti e necrosi papillare , infezioni delle basse vie urinarie e genitali, batteriurie asintomatiche: sono favorite oltre che da maggior suscettibilità alle infezioni anche da turbe dell’innervazone vegetativa vescicale (atonia vescicale della vescica neurogena). L’impotenza è dovuta alla compromissione dell’innervazione vegetativa dell’apparato genitale.
. II: progressione del danno renale. III:microalbuminuria persistente. IV: ↓ GFR , con ipertensione arteriosa. V: insuff renale terminale. ALTRE: pielonefriti e necrosi papillare , infezioni delle basse vie urinarie e genitali, batteriurie asintomatiche: sono favorite oltre che da maggior suscettibilità alle infezioni anche da turbe dell’innervazone vegetativa vescicale (atonia vescicale della vescica neurogena). L’impotenza è dovuta alla compromissione dell’innervazione vegetativa dell’apparato genitale.")
28
COMPLICANZE A CARICO DI ALTRI APPARATI
COMPLICANZE DIGESTIVE: causate sempre da neuropatia autonomica. A livello gastrico si ha atonia che causa senso di ripienezza e vomito; a livello intestinale: stipsi, incontinenza fecale. COMPLICANZE OSTEOARTICOLARI: osteoporosi, osteolisi, fratture ossee. COMPLICANZE CUTANEE: di origine infettiva da Gram-negativi (foruncolosi, favi, erisipela, idrosadeniti, piodermiti, ascessi, flemmoni); infezioni micotiche specie da Candida Albicans. Manifestazioni cutanee poi sono dovute a neuropatia autonomica che causa turbe della sudorazione.
; infezioni micotiche specie da Candida Albicans. Manifestazioni cutanee poi sono dovute a neuropatia autonomica che causa turbe della sudorazione.")
29
-SINDROME IPEROSMOLARE NON CHETOSICA
COMPLICANZE ACUTE DEL DIABETE MELLITO -CHETOACIDOSI -SINDROME IPEROSMOLARE NON CHETOSICA -IPOGLICEMIA

30
CHETOACIDOSI DIABETICA
Mortalità del 16% Il 10% degli episodi di chetoacidosi diabetica avvengono in soggetti fra 45 e 65 anni. Il 75 % dei soggetti sono anziani. I soggetti con età >65 anni hanno mortalità compresa tra 15 e 28%.

31
CAUSE DI CHETOACIDOSI DIABETICA
Concomitanti patologie 50% 25% Mancata somministrazione di insulina 25% Causa scatenante sconosciuta

32
Stress traumatici o chirurgici
PATOLOGIE CONCOMITANTI Gravi infezioni Stati setticemici Stress traumatici o chirurgici Infarto del miocardio

33
Patogenesi DKA Carenza insulinica
Aumento ormoni contro-regolatori (GH, Catecolamine, Cortisolo, glucagone) Catabolismo proteico Attivazione neoglucogenesi epatica
 Catabolismo proteico. Attivazione neoglucogenesi epatica.")
34
MECCANISMI FISIOPATOLOGICI DI DKA-1
Deficit insulinico proteolisi Glucagone Cortisolo neoglucogenesi Utilizzo glucosio glicosuria Diuresi osmotica disidratazione

35
MECCANISMI FISIOPATOLOGICI DI DKA-2
Sangue Fegato acqua polipnea acidosi Aceto-acetato e B idrossi-butirrato vomito Muscolo Formazione di corpi chetonici Corpi chetonici Deficit insulinico Elevato acetil-Coa Ossidazione acidi grassi (2) Acidi grassi liberi T. adiposo Lipolisi (1) * Sintesi di trigliceridi Trigliceridi in VLDL * In mancanza di Malonil-Coa non completa ossidazione dei grassi con accumulo di corpi chetonici
 Acidi grassi. liberi. T. adiposo. Lipolisi. (1) * Sintesi di. trigliceridi. Trigliceridi. in VLDL. * In mancanza di Malonil-Coa non completa ossidazione dei grassi con accumulo di corpi chetonici.")
36
SINTOMI E SEGNI DI CHETOACIDOSI DIABETICA
- nausea - cute secca e calda - vomito - mucose aride - dolore addominale - ipotermia - sete alito acetonemico - poliuria ipotonia muscolare - tachicardia iporeflessia - ipotensione coscienza alterata sino al coma - disidratazione - respiro di Kussmaul

37
DATI DI LABORATORIO - elevata iperglicemia (500-700 mg/dl)
- presenza di corpi chetonici - lieve iposodiemia - normo/iperpotassiemia - aumento osmolarità (>300 mOsm) - ipertrigliceridemia - emogasanalisi: pH 7.20, pCO2 <40 mmHg, bicarbonati <24 mmol/l - gap anionico Na-(Cl+HCO3)= - emoglobina ed ematocrito - leucocitosi Gap anionico normale tra mmol/L
 - ipertrigliceridemia. - emogasanalisi: pH 7.20, pCO2 <40 mmHg, bicarbonati <24 mmol/l. - gap anionico Na-(Cl+HCO3)= - emoglobina ed ematocrito. - leucocitosi. Gap anionico normale tra mmol/L.")
38
CHETOACIDOSI DIABETICA
Controllare: - glicemia - acetonuria - emogasanalisi - creatininemia, urea - emocromo - osmolalità plasmatica - ECG: ricercare segni di ipokaliemia o di infarto miocardico N.B. osmolalità: mOsm/l= 2(Na+K) + glucosio + urea se glicemia ed urea sono espresse in mg/dl, la prima va divisa per 18, la seconda per 2.8. (vn )
 + glucosio + urea. se glicemia ed urea sono espresse in mg/dl, la. prima va divisa per 18, la seconda per 2.8. (vn )")
39
CHETOACIDOSI DIABETICA
Posizionare: catetere vescicale accesso venoso periferico (se possibile catetere venoso centrale) Monitorare ogni ora: -frequenza cardiaca -pressione arteriosa -temperatura -diuresi -glicemia
 Monitorare ogni ora: -frequenza cardiaca. -pressione arteriosa. -temperatura. -diuresi. -glicemia.")
40
TRATTAMENTO DELLA CHETOACIDOSI
DIABETICA insulina elettroliti fluidi

41
TRATTAMENTO DELLA CHETOACIDOSI DIABETICA
Somministrazione di liquidi La soluzione isotonica (NaCl 0.9%) oltre a correggere la disidratazione, riduce l’iperglicemia aumentando sia la risposta dei tessuti periferici all’insulina sia l’escrezione urinaria di glucosio. Soluzione fisiologica: L in minuti circa - 1L/h per le seguenti 2-4 ore (Basandosi sul bilancio entrate/uscite e sulla valutazione clinica dello stato di idratazione). La velocità di infusione può essere variata a secondo dei valori di PVC (vn= 2-8 cm2 acqua). In mancanza di catetere venoso centrale, eseguire ripetutamente auscultazione polmonare.
 oltre a correggere la. disidratazione, riduce l’iperglicemia aumentando sia la risposta. dei tessuti periferici all’insulina sia l’escrezione urinaria di glucosio. Soluzione fisiologica: - 1L in minuti circa. - 1L/h per le seguenti 2-4 ore. (Basandosi sul bilancio entrate/uscite e sulla valutazione clinica. dello stato di idratazione). La velocità di infusione può essere variata a secondo dei valori di PVC. (vn= 2-8 cm2 acqua). In mancanza di catetere venoso centrale, eseguire ripetutamente. auscultazione polmonare.")
42
TRATTAMENTO DELLA CHETOACIDOSI DIABETICA
Somministrazione di liquidi Quando la glicemia raggiunge mg/dl, somministrare glucosio ad una velocità di 5-10 g/h (Glucosata 5%: cc/h), come soluzione separata o in combinazione con fisiologica. La velocità di somministrazione di soluzioni contenenti glucosio deve essere regolata in base a frequenti misure della glicemia.
, come soluzione separata o in combinazione con fisiologica. La velocità di somministrazione di soluzioni contenenti glucosio. deve essere regolata in base a frequenti misure della glicemia.")
43
TRATTAMENTO DELLA CHETOACIDOSI
DIABETICA INSULINA per via venosa Può essere somministrata per via intramuscolare

44
INSULINA per via venosa
10 U di insulina pronta ev come dose di carico, seguite da 5-10 U/ora (Velocità oraria 0.1 U/kg del peso corporeo): (50 U di insulina pronta in 500 cc di fisiologica = 0.1 U/ml, per somministrare 10 U/ora: 100cc/ora). L’infusione di insulina deve essere innestata su una linea di infusione indipendente in maniera tale da regolarla in modo autonomo.
: (50 U di insulina pronta in 500 cc di fisiologica = 0.1 U/ml, per somministrare 10 U/ora: 100cc/ora). L’infusione di insulina deve essere innestata su una linea di. infusione indipendente in maniera tale da regolarla in modo. autonomo.")
45
INSULINA per via muscolare
10 U di insulina pronta im come dose di carico, seguite da Somministrazioni di 5-10 U/ora La velocità media di abbassamento della glicemia è di circa mg/dl/h. La mancata riduzione della glicemia del 10% (o di più di 100 mg/dl) nelle prime due ore, deve costituire la base per un ulteriore valutazione e per l’uso di dosi di insulina più elevate.
 nelle prime due ore, deve costituire la. base per un ulteriore valutazione e per l’uso di dosi di insulina. più elevate.")
46
ELETTROLITI POTASSIO -misurare la potassiemia ed eseguire ECG
-se il potassio è 4-5 mEq/L, aggiungere 20 mEq K in ogni litro di fisiologica ed infondere a 1 L/h -mantenere il K fra 4 e 5 mEq/L: a-se è 4-5 mEq/L, proseguire con infusione di K a 20 mEq/h b-se è 5-6 mEq/L, ridurre a 10 mEq/h c-se è >6 mEq/L, stop K d-se è 3-4 mEq/L, aumentare K a 30 mEq/h e-se è <3 mEq/L, aumentare K a mEq/h. BICARBONATO non è raccomandato per il trattamento di routine.

47
DELLA CHETOACIDOSI DIABETICA
COMPLICANZE DELLA CHETOACIDOSI DIABETICA -edema cerebrale -edema polmonare acuto non cardiogeno

48
IPEROSMOLARE NON CHETOSICA
SINDROME IPEROSMOLARE NON CHETOSICA -Pazienti anziani che non hanno dati anamnestici di diabete mellito o nei quali il diabete è stato lieve fino a quel momento -mortalità del 40-70% Cause scatenanti: malattie intercorrenti: infezioni pancreatiti ustioni farmaci glucocorticoidi diuretici b-bloccanti fenitoina Comparsa graduale: dai 7 ai 10 giorni

49
SINDROME IPEROSMOLARE NON CHETOSICA
Età avanzata (-alterazione meccanismo della sete -compromissione conservazione renale di acqua) Prodromi protratti Importante deficit di acqua corporea Grave iperglicemia
 Prodromi protratti. Importante deficit di acqua corporea. Grave iperglicemia.")
50
FISIOPATOLOGIA DELLA SINDROME IPEROSMOLARE NON CHETOSICA
Produzione epatica di glucosio Iperglicemia severa Insulino resistenza Ormoni dello stress Malattie intercorrenti disidratazione Ridotta ingestione liquidi e/o febbre Glicosuria poliuria oliguria Ridotta escrezione renale di glucosio e sodio iperglicemia ipernatriemia

51
SEGNI E SINTOMI -stato confusionale fino al coma
-sintomi neurologici focali (emiplegia) -convulsioni -oliguria -disidratazione -ipotensione -ipotermia
 -convulsioni. -oliguria. -disidratazione. -ipotensione. -ipotermia.")
52
DATI DI LABORATORIO -iperglicemia (range 600-2700 mg/dl)
-iperosmolarità (> 350 mOsm/kg) -ipopotassiemia - creatinina - corpi chetonici assenti
 -ipopotassiemia. - creatinina. - corpi chetonici assenti.")
53
TRATTAMENTO DELLA SINDROME IPEROSMOLARE IPERGLICEMICA
- correggere la grave disidratazione con Fisiologica 0.9% -Insulina: dose iniziale i.m o e.v. (monitorare accuratamente i valori glicemici, poiché la reidratazione può contribuire significativamente alla riduzione dell’iperglicemia). -Potassio: controlli frequenti ed eventuale somministrazione.
. -Potassio: controlli frequenti ed eventuale somministrazione.")
54
DELLA SINDROME IPEROSMOLARE
COMPLICANZE DELLA SINDROME IPEROSMOLARE IPERGLICEMICA -elevata mortalità -edema cerebrale -tromboembolismi -necrosi tubulare acuta -infarto del miocardio

55
DIAGNOSI DIFFERENZIALE DI COMPLICANZE DEL DIABETE
LABORATORIO DELLE COMPLICANZE DEL DIABETE Chetoacidosico Iperosmolare plasma Glicemia < >600 mg/dl Chetonemia assente Osmolarità < >320 pH < N Bicarbonati < N Na bassa normale-alta Bicarbonati bassi normali urine Glicosuria Chetonuria assente

56
IPOGLICEMIA È l’emergenza più frequente nei soggetti geriatrici
ed è estremamente grave in quanto può essere associata o scatenare eventi cerebrovascolari, infarto del miocardio, coma etc.

57
CAUSE DI IPOGLICEMIA -farmaci:insulina, sulfonilurea, alcol
-disfunzione d’organo: renale, epatico, cardiovascolare, sistema nervoso centrale ed autonomico, sepsi, gastrointestinale -anoressia, fattori sociali -neoplasie

58
SINTOMI E SEGNI -ansietà, irrequiettezza -palpitazioni, tremore
-senso di fame, sudorazione -astenia, difficoltà alla concentrazione, stordimento -sonnolenza, alterazione dello stato di coscienza (confusione, coma) -manifestazioni convulsive, segni neurologici focali -alterazione della termoregolazione (ipotermia, ipertermia)
 -manifestazioni convulsive, segni neurologici focali. -alterazione della termoregolazione (ipotermia, ipertermia)")
59
MANIFESTAZIONI CLINICHE
Cute: pallida PAO: nella norma Fc: tachicardia (bradicardia in fase avanzata) respiro: iperpnea (bradipnea in fase avanzata) occhio: pupille midriasi (miosi in fase avanzata) EON: ipertono muscolare, ROT nella norma, Babinsky talora presente
 respiro: iperpnea (bradipnea in fase avanzata) occhio: pupille midriasi (miosi in fase avanzata) EON: ipertono muscolare, ROT nella norma, Babinsky talora presente.")
60
TRATTAMENTO IPOGLICEMIA
Se il paziente è cosciente: -somministrare g glucosio per os (latte zuccherato) Se il paziente è incosciente: -somministrare 25 g glucosio e.v. in bolo seguiti da infusione continua di glucosata (5 o 10% a seconda della gravità dell’ipoglicemia). Eventuale ulteriore bolo di 25 g di glucosio in caso dopo 10 minuti il paziente sia ancora incosciente.
 Se il paziente è incosciente: -somministrare 25 g glucosio e.v. in bolo seguiti da. infusione continua di glucosata (5 o 10% a seconda della gravità. dell’ipoglicemia). Eventuale ulteriore bolo di 25 g di glucosio in caso. dopo 10 minuti il paziente sia ancora incosciente.")
62
American Diabetes Association 2007

63
Correlazione tra HbA1c e livello medio di glicemia plasmatica
Ripetuta almeno due/anno in pazienti in buon controllo glico-metab, negli altri 4 volte American Diabetes Association 2007

64
Lowering HbA1c Reduces Risk of Complications*
Retinopathy -5 -6 p=0.63 Cataract extraction -10 Microvascular complications -15 -16 p=0.052 Reduction in Risk (%) -20 Albuminuria at 12 years -21 p=0.015 -25 -24 p=0.046 -25 p=0.009 MI -30 Fatal myocardial infarction -35 -34 p= -40 *Percent risk reduction for 0.9% decrease in HbA1c UKPDS. Lancet 1998; 352:837
 -20. Albuminuria at. 12 years p= p= p= MI Fatal myocardial. infarction p= *Percent risk reduction for. 0.9% decrease in HbA1c. UKPDS. Lancet 1998; 352:837.")
66
Treatment of Type 2 Diabetes
Diagnosis Therapeutic Lifestyle Change Monotherapy This algorithm represents the logical progression of treatment for a patient diagnosed with type 2 diabetes. However, there are some exceptions. For example, there are some instances in which a patient presents with acute hyperglycemia that must be temporarily controlled with insulin. In addition, women with gestational diabetes must utilize diet or insulin therapy to control the disease, since all oral diabetes medications are contraindicated during pregnancy. Finally, it is important for the physician and patient to agree on a therapy based on the needs of the patient and the patient's comfort level with available treatment options. Combination Therapy - Oral Drugs Only Combination Therapy – Oral Drugs with Insulin

67
Riduzione dell’incidenza di diabete di tipo 2 con interventi sullo stile di vita o con metformina Diabetes Prevention Program Research Group NEJM 346:393, 2002 -31% -58% DPP. Le modificazioni dello stile di vita riducono l’incidenza di diabete del 58 % e lla metformina del 31 %. In soggetti a rischio.

68
Glucose tolerance after weight loss fifhteen month follow-up
baseline 1 m 5 m 15 m 20 40 60 80 100 120 140 baseline 1 m 5 m 15 m 300 600 900 Body weight Body weight ∑ glucose ∑ glucose baseline 1 m 5 m 15 m 200 400 600 ∑ insulin ∑ insulin Glucose tolerance after weight loss fifhteen month follow-up Bosello et al, 1978

69
Metabolic Improvements of Weight Loss: 1 yr treatment
Before > 13,6 6,9- 13,6 2,4 - 6,8 0 - 2,3 gained RBW % HbA1 (%) Glucose (mg/dl) Insulin (mU/ml) Tg (mg/dl) HDL-Ch 159 121* 143* 152* 157° 164* 9,7 7,1* 8,7* 9,8 10,4 10,6§ 190 109* 162° 185 197 217§ 20 2,9* 10,5§ 11,8§ 14,6 14,9 195 87* 155° 165§ 175 204 28,2 48,8* 41,3 40,3 38,4 39,7 * < 0, ° < 0, § < 0,05 Wing et al, 1987
 Glucose. (mg/dl) Insulin. (mU/ml) Tg (mg/dl) HDL-Ch * 143* 152* 157° 164* 9,7. 7,1* 8,7* 9,8. 10,4. 10,6§ * 162° § 20. 2,9* 10,5§ 11,8§ 14,6. 14, * 155° 165§ ,2. 48,8* 41,3. 40,3. 38,4. 39,7. * < 0,001 - ° < 0,01 - § < 0,05. Wing et al,")
70
Changes in HbA1 as a function of weight loss
after 1 year program < 5% 6 -14% >15% -2,5 -2 -1,5 -1 -0,5 NS NS % % p < 0,0005 p < 0,0005 Wing at al, 1994 p < 0,0001 Wing at al, 1994 p < 0,0001 Weight loss Weight loss

71
Recommended Nutrient Content of a Weight-Reducing Diet
Saturated fatty acids Polyunsaturated fatty acids Monounsaturated fatty acids Protein 15% 8%-10% Fat <30% Carbohydrate >55% <10% <15% Recommended nutrient content of a weight-reducing diet Dietary guidelines proposed by the National Institutes of Health [1] recommend a 500 kcal/d deficit for overweight persons (BMI kg/m2) who have obesity-related complications, and for persons with class I obesity (BMI kg/m2). This energy deficit will result in approximately a 1-lb (0.45 kg) weight loss per week and about a 10% weight reduction at 6 months. A kcal/d deficit is recommended for those with class II (BMI kg/m2) or class III (BMI 40 kg/m2) obesity, which will produce about a 1- to 2-lb weight loss per week and a 10% weight loss at 6 months. The recommended macronutrient composition for a low-calorie weight loss diet is shown in this figure and includes 55% or more of daily calories from carbohydrates, 15% from protein, and 30% or less from fat. In addition, specific recommendations are made regarding the composition of fat ingestion: total energy intake should be comprised of 8%-10% calories from saturated fat, 10% or less calories from polyunsaturated fats, and 15% or less calories from monounsaturated fats. Daily cholesterol intake should not exceed 300 mg/d, and daily fiber intake should be between g/d. National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The Evidence Report. Obes Res. 1998;6(suppl 2):51S-209S. Calories: kcal/d reduction Cholesterol: <300 mg/d Fiber: g/d Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults– The Evidence Report. Obes Res. 1998;6 (suppl 2).
 who have obesity-related complications, and for persons with class I obesity (BMI kg/m2). This energy deficit will result in approximately a 1-lb (0.45 kg) weight loss per week and about a 10% weight reduction at 6 months. A kcal/d deficit is recommended for those with class II (BMI kg/m2) or class III (BMI 40 kg/m2) obesity, which will produce about a 1- to 2-lb weight loss per week and a 10% weight loss at 6 months. The recommended macronutrient composition for a low-calorie weight loss diet is shown in this figure and includes 55% or more of daily calories from carbohydrates, 15% from protein, and 30% or less from fat. In addition, specific recommendations are made regarding the composition of fat ingestion: total energy intake should be comprised of 8%-10% calories from saturated fat, 10% or less calories from polyunsaturated fats, and 15% or less calories from monounsaturated fats. Daily cholesterol intake should not exceed 300 mg/d, and daily fiber intake should be between g/d. National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The Evidence Report. Obes Res. 1998;6(suppl 2):51S-209S. Calories: kcal/d reduction. Cholesterol: <300 mg/d. Fiber: g/d. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults– The Evidence Report. Obes Res. 1998;6 (suppl 2).")
72
Blood Glucose Concentrations After Ingesting High and Low Glycemic Index Foods
New potatoes* Kidney beans* Blood Glucose (mg/dL) Blood glucose concentrations after ingesting high and low glycemic index foods Glycemic index refers to the increase in blood glucose that occurs after consumption of a food containing a standard amount of carbohydrate. The index represents the comparison of a tested food to a standard amount (50 g) of glucose. This figure illustrates the differences in blood glucose concentrations that are achieved after ingesting a food that has a high glycemic index (new potatoes) and a food that has a low glycemic index (kidney beans). The index number is the area under the blood glucose concentration curve during the 2 hours after food ingestion and represents the rate of digestion and absorption of the carbohydrate present in the food being evaluated. Glucose has the highest glycemic index and is rated at Low-glycemic-index foods have a glycemic index less than 55. Most refined grain products and potatoes have a high glycemic index, whereas most fruits, legumes, and non-starchy vegetables have a low glycemic index. However, the “true” glycemic index of a specific food that is ingested as part of a meal can be altered by several factors, such as the method of preparation and the effect of concomitantly ingested foods on intestinal motility. For example, a high-glycemic index food may cause a mild increase in blood glucose concentration if gastric emptying is slowed by simultaneous fat ingestion. A low-glycemic-index diet has been proposed as a treatment for obesity because it may affect hunger by specific effects on postprandial pancreatic hormone secretion [3]. The results of one randomized controlled trial, conducted in 14 overweight adolescents, found a reduced glycemic index diet caused weight loss, while a low fat diet caused weight gain (2). However, additional randomized controlled trials conducted in a larger number of subjects are needed to evaluate the potential efficacy of a low-glycemic diet as a therapy for obesity. Jenkins DJ, Wolever TM, Jenkins AL. Starchy foods and glycemic index. Diabetes care 1988;11: Anderson JW, Geil PB. Nutritional management of diabetes. In: Shils ME, Olson JA, Shike M, eds. Modern Nutrition in Health and Disease. 8th ed. Philadelphia, PA: Lea & Febiger; 1994: Ludwig DS, Majzoub JA, Al-Zahrani A, et al. High glycemic index foods, overeating, and obesity. Pediatrics 1999;103: Ebbeling CB, Leidig MM, Sinclair KB, Hangen JP, Ludwig DS: A reduced-glycemic load diet in the treatment of adolescent obesity. Arch Pediatr Adolesc.Med 2003;157: Spieth LE, Harnish JD, Lenders CM, et al. A low-glycemic index diet in the treatment of pediatric obesity. Arch Pediatr Adolesc Med 2000;154: Time (min) 30 60 90 120 *containing 50 g glucose Adapted from: Anderson et al. Modern Nutrition in Health and Disease; 2001:1269.
 Blood glucose concentrations after ingesting high and low glycemic index foods. Glycemic index refers to the increase in blood glucose that occurs after consumption of a food containing a standard amount of carbohydrate. The index represents the comparison of a tested food to a standard amount (50 g) of glucose. This figure illustrates the differences in blood glucose concentrations that are achieved after ingesting a food that has a high glycemic index (new potatoes) and a food that has a low glycemic index (kidney beans). The index number is the area under the blood glucose concentration curve during the 2 hours after food ingestion and represents the rate of digestion and absorption of the carbohydrate present in the food being evaluated. Glucose has the highest glycemic index and is rated at 100. Low-glycemic-index foods have a glycemic index less than 55. Most refined grain products and potatoes have a high glycemic index, whereas most fruits, legumes, and non-starchy vegetables have a low glycemic index. However, the true glycemic index of a specific food that is ingested as part of a meal can be altered by several factors, such as the method of preparation and the effect of concomitantly ingested foods on intestinal motility. For example, a high-glycemic index food may cause a mild increase in blood glucose concentration if gastric emptying is slowed by simultaneous fat ingestion. A low-glycemic-index diet has been proposed as a treatment for obesity because it may affect hunger by specific effects on postprandial pancreatic hormone secretion [3]. The results of one randomized controlled trial, conducted in 14 overweight adolescents, found a reduced glycemic index diet caused weight loss, while a low fat diet caused weight gain (2). However, additional randomized controlled trials conducted in a larger number of subjects are needed to evaluate the potential efficacy of a low-glycemic diet as a therapy for obesity. Jenkins DJ, Wolever TM, Jenkins AL. Starchy foods and glycemic index. Diabetes care 1988;11: Anderson JW, Geil PB. Nutritional management of diabetes. In: Shils ME, Olson JA, Shike M, eds. Modern Nutrition in Health and Disease. 8th ed. Philadelphia, PA: Lea & Febiger; 1994: Ludwig DS, Majzoub JA, Al-Zahrani A, et al. High glycemic index foods, overeating, and obesity. Pediatrics 1999;103: Ebbeling CB, Leidig MM, Sinclair KB, Hangen JP, Ludwig DS: A reduced-glycemic load diet in the treatment of adolescent obesity. Arch Pediatr Adolesc.Med 2003;157: Spieth LE, Harnish JD, Lenders CM, et al. A low-glycemic index diet in the treatment of pediatric obesity. Arch Pediatr Adolesc Med 2000;154: Time (min) *containing 50 g glucose. Adapted from: Anderson et al. Modern Nutrition. in Health and Disease; 2001:1269.")
73
Diabete e Life style Sospensione del fumo
Valutare regolarmente il livello di attività fisica e informare il paziente sui benefici di attività fisica regolare Sospensione del fumo American Diabetes Association 2007

74
Diabetes as a CHD Risk Equivalent
10-year risk for CHD 20% High mortality with established CHD High mortality with acute MI High mortality post acute MI

75
Three Categories of Risk that Modify LDL-Cholesterol Goals
Risk Category CHD and CHD risk equivalents Multiple (2+) risk factors Zero to one risk factor LDL Goal (mg/dL) <100 <130 <160
 risk factors. Zero to one risk factor. LDL Goal (mg/dL) <100. <130. <160.")
76
Diabete ed IPERTENSIONE
Controllo PA ad ogni visita Goal PA ≤ 130/80 mmHg, Se PA sistolica e diastolica intervento sullo stile di vita per 3 mesi. Se goal non raggiunto terapia farmacologica. Se PA > 140/90: terapia farmacologica Controllo della funzionalità renale e della ionemia entro 1-2 settimane dall’inizio del trattamento antiipertensivo con l’utilizzo di ACE-inibitori, sartanici, diuretici dell’ansa o tiazidici. Diabetes Care, 2007 American Diabetes Association 2007

77
Diabete e anti-aggregazione
terapia con aspirina ( mg/die) in prevenzione secondaria nei pazienti diabetici con CVD terapia con aspirina ( mg/die) in prevenzione primaria in Pazienti con diabete tipo 2 e tipo 1 con età > 40 anni e aumentato rischio CVD (familiarità, altri fatt di rischio, fumo, albuminuria) considera la terapia con aspirina in pazienti diabetici con età tra anni in presenza di altri fattori di rischio CVD Non prescrivere terapia con aspirina in soggetti diabetici con età < 30 anni Diabetes Care, 2007 American Diabetes Association 2007
 in prevenzione secondaria nei pazienti diabetici con CVD. terapia con aspirina ( mg/die) in prevenzione primaria in Pazienti con diabete tipo 2 e tipo 1 con età > 40 anni e aumentato rischio CVD (familiarità, altri fatt di rischio, fumo, albuminuria) considera la terapia con aspirina in pazienti diabetici con età tra anni in presenza di altri fattori di rischio CVD. Non prescrivere terapia con aspirina in soggetti diabetici con età < 30 anni. Diabetes Care, American Diabetes Association")
78
Oral Medications to Treat Type 2 Diabetes

79
Major Classes of Medications
1. Drugs that sensitize the body to insulin and/or control hepatic glucose production 2. Drugs that stimulate the pancreas to make more insulin 3. Drugs that slow the absorption of starches Thiazolidinediones Biguanides Sulfonylureas Meglitinides Alpha-glucosidase inhibitors There are five major classes of oral diabetes medications: thiazolidinediones, biguanides, sulfonylureas, meglitinides, and alpha-glucosidase inhibitors. These five classes of medication operate in essentially three different ways. Thiazolidinediones and biguanides decrease glucose production in the liver and increase insulin sensitivity in peripheral body tissues. Sulfonylureas and meglitinides stimulate the pancreatic beta cells to make more insulin. Finally, alpha-glucosidase inhibitors slow the absorption of starches in the gut, reducing the amount of glucose that enters the bloodstream.

80
Efficacy of Monotherapy with Oral Diabetes Agents
There are a number of antihyperglycemic agents available for patients with type 2 diabetes. With the exception of the alpha-glucosidase inhibitors, most of the drug classes share a similar level of efficacy. Drug therapy decisions must take into consideration patient conditions which may contraindicate the use of the drug, any adverse effects as well as any beneficial effects such as weight loss, and patient and physician preferences. In addition to taking antihyperglycemic agents, all patients with type 2 diabetes should be encouraged to maintain a healthy lifestyle by exercising and following an appropriate diet. Additional medications may also be required to treat conditions such as hypertension or dyslipidemia. DeFronzo Annals of Internal Medicine 1999;131: Nathan N Engl J Med 2002; 347:

81
Biguanides Biguanides decrease hepatic glucose production and increase insulin-mediated peripheral glucose uptake. Efficacy Decrease fasting plasma glucose mg/dl ( mmol/L) Reduce A1C % Other Effects Diarrhea and abdominal discomfort Lactic acidosis if improperly prescribed Cause small decrease in LDL cholesterol level and triglycerides No specific effect on blood pressure No weight gain, with possible modest weight loss Contraindicated in patients with impaired renal function (Serum Cr > 1.4 mg/dL for women, or 1.5 mg/dL for men) Medications in this Class: metformin (Glucophage), metformin hydrochloride extended release (Glucophage XR) The mechanism of action of metformin is not entirely understood, but it's predominant effect is to suppress hepatic glucose production and to enhance insulin sensitivity in peripheral tissues (primarily muscle). It is unclear if insulin sensitivity occurs by metformin binding to cell receptors,which leads to an increase in glucose transporter expression, or whether insulin sensitivity is simply a secondary effect of the suppressed glucose production. Metformin's ability to lower A1C and decrease fasting plasma glucose is similar to that of sulfonylurea drugs. However, the UKPDS showed that those who received metformin had less hypoglycemia and weight gain than those who received sulfonylureas. Metformin must be avoided in patients with renal impairments, as those patients are at higher risk of experiencing lactic acidosis. However, metformin is an effective monotherapy and may be an ideal drug for overweight patients since it does not cause weight gain and has been seen to cause modest amounts of weight loss when first administered. Diarrhea and abdominal discomfort can be alleviated by changes in diet and slow increases in metformin dosage.
 Reduce A1C % Other Effects. Diarrhea and abdominal discomfort. Lactic acidosis if improperly prescribed. Cause small decrease in LDL cholesterol level and triglycerides. No specific effect on blood pressure. No weight gain, with possible modest weight loss. Contraindicated in patients with impaired renal function (Serum Cr > 1.4 mg/dL for women, or 1.5 mg/dL for men) Medications in this Class: metformin (Glucophage), metformin hydrochloride extended release (Glucophage XR) The mechanism of action of metformin is not entirely understood, but it s predominant effect is to suppress hepatic glucose production and to enhance insulin sensitivity in peripheral tissues (primarily muscle). It is unclear if insulin sensitivity occurs by metformin binding to cell receptors,which leads to an increase in glucose transporter expression, or whether insulin sensitivity is simply a secondary effect of the suppressed glucose production. Metformin s ability to lower A1C and decrease fasting plasma glucose is similar to that of sulfonylurea drugs. However, the UKPDS showed that those who received metformin had less hypoglycemia and weight gain than those who received sulfonylureas. Metformin must be avoided in patients with renal impairments, as those patients are at higher risk of experiencing lactic acidosis. However, metformin is an effective monotherapy and may be an ideal drug for overweight patients since it does not cause weight gain and has been seen to cause modest amounts of weight loss when first administered. Diarrhea and abdominal discomfort can be alleviated by changes in diet and slow increases in metformin dosage.")
82
Metformin : dosage data
AACE Diabetes Guidelines, Endocr Pract. 2002

83
Thiazolidinediones Thiazolidinediones decrease insulin resistance by making muscle and adipose cells more sensitive to insulin. They also suppress hepatic glucose production. Efficacy Decrease fasting plasma glucose ~35-40 mg/dl ( mmol/L) Reduce A1C ~ % 6 weeks for maximum effect Other Effects Weight gain, edema Hypoglycemia (if taken with insulin or agents that stimulate insulin release) Contraindicated in patients with abnormal liver function or CHF Improves HDL cholesterol and plasma triglycerides; usually LDL neutral Medications in this Class: pioglitazone (Actos), rosiglitazone (Avandia), [troglitazone (Rezulin) - taken off market due to liver toxicity] Thiazolidinediones (TZDs) enhance insulin sensitivity in muscle and adipose tissue by binding to cell receptors,which leads to an increase in glucose transporter expression. TZDs encourage beta cells to respond more efficiently by lowering the amount of glucose and free fatty acids in the bloodstream, both of which are known to be detrimental to insulin secretion. Finally, these drugs reduce glucose production in the liver. Clinical trials indicate that pioglitazone and rosiglitazone are slightly more effective at reducing A1C ( % reduction) than troglitazone (1.1% reduction). Some of the beneficial side effects of thiazolidinediones include an increase in HDL cholesterol and reduction of triglyceride concentrations. This class of drugs has also been shown to lower blood pressure and decrease vascular inflammation in vitro. There are clinical studies underway to further examine the cardiovascular benefit to TZDs. Some adverse effects of TZDs include weight gain, a potential increase in LDL cholesterol levels, and a possible increase in alanine aminotransferase levels (ALT). Because of the risk of weight gain, edema, and increased LDL cholesterol, thiazolidinediones are contraindicated in patients with advanced forms of congestive heart failure. Due to reported cases of liver failure and liver toxicity caused by the increase in ALT levels, TZDs are contraindicated in patients with abnormal liver function. TZDs are the most expensive of the oral antidiabetic agents.
 Reduce A1C ~ % 6 weeks for maximum effect. Other Effects. Weight gain, edema. Hypoglycemia (if taken with insulin or agents that stimulate insulin release) Contraindicated in patients with abnormal liver function or CHF. Improves HDL cholesterol and plasma triglycerides; usually LDL neutral. Medications in this Class: pioglitazone (Actos), rosiglitazone (Avandia), [troglitazone (Rezulin) - taken off market due to liver toxicity] Thiazolidinediones (TZDs) enhance insulin sensitivity in muscle and adipose tissue by binding to cell receptors,which leads to an increase in glucose transporter expression. TZDs encourage beta cells to respond more efficiently by lowering the amount of glucose and free fatty acids in the bloodstream, both of which are known to be detrimental to insulin secretion. Finally, these drugs reduce glucose production in the liver. Clinical trials indicate that pioglitazone and rosiglitazone are slightly more effective at reducing A1C ( % reduction) than troglitazone (1.1% reduction). Some of the beneficial side effects of thiazolidinediones include an increase in HDL cholesterol and reduction of triglyceride concentrations. This class of drugs has also been shown to lower blood pressure and decrease vascular inflammation in vitro. There are clinical studies underway to further examine the cardiovascular benefit to TZDs. Some adverse effects of TZDs include weight gain, a potential increase in LDL cholesterol levels, and a possible increase in alanine aminotransferase levels (ALT). Because of the risk of weight gain, edema, and increased LDL cholesterol, thiazolidinediones are contraindicated in patients with advanced forms of congestive heart failure. Due to reported cases of liver failure and liver toxicity caused by the increase in ALT levels, TZDs are contraindicated in patients with abnormal liver function. TZDs are the most expensive of the oral antidiabetic agents.")
84
Thiazolidinediones Pioglitazone Rosiglitazone Controindicazioni
Dose: mg/die, 1 somministrazione/die, anche in presenza di IRC (fino a GFR di 4 ml/m), Rosiglitazone Dose: mg/die, 1-2 somministrazioni/die, anche in presenza di IRC (fino a GFR di 30 ml/m) Controindicazioni transaminasi > 2.5 la norma Insufficienza epatica Insufficienza cardiaca (classe NYHA I-IV)
, Rosiglitazone. Dose: 4-8 mg/die, 1-2 somministrazioni/die, anche in presenza di IRC (fino a GFR di 30 ml/m) Controindicazioni. transaminasi > 2.5 la norma. Insufficienza epatica. Insufficienza cardiaca (classe NYHA I-IV)")
85
Thiazolidinediones : dosage data
AACE Diabetes Guidelines, Endocr Pract. 2002

86
Sulfonylureas Sulfonylureas increase endogenous insulin secretion
Efficacy Decrease fasting plasma glucose mg/dl ( mmol/L) Reduce A1C by % Other Effects Hypoglycemia Weight gain No specific effect on plasma lipids or blood pressure Generally the least expensive class of medication Medications in this Class: First generation sulfonylureas: chlorpropamide (Diabinese), Glibenclamide (Euglucon) Second generation sulfonylureas: gliclazide (Diamicron), glimepiride (Amaryl, Solosa), glipizide (Minidiabe) Sulfonylureas (SUs) increase insulin secretion by binding to receptors on the surface of pancreatic beta cells, triggering a series of reactions which leads to insulin secretion. Because SUs cause circulating insulin levels to increase, there is a risk of hypoglycemia. There is also some concern that increased insulin levels are associated with cardiovascular disease, however the UKPDS did not show a relationship between increased mortality and SU administration. Finally, there is concern that SUs will exhaust beta cell function by increasing insulin secretion. However, the decline in beta cell function is more likely caused by the disease itself, and not the use of SUs. First generation sulfonylureas are just as efficacious as the second generation drugs, however the second generation may be more potent and safer than first. When diet and exercise fail, SUs are an effective monotherapy.
 Reduce A1C by % Other Effects. Hypoglycemia. Weight gain. No specific effect on plasma lipids or blood pressure. Generally the least expensive class of medication. Medications in this Class: First generation sulfonylureas: chlorpropamide (Diabinese), Glibenclamide (Euglucon) Second generation sulfonylureas: gliclazide (Diamicron), glimepiride (Amaryl, Solosa), glipizide (Minidiabe) Sulfonylureas (SUs) increase insulin secretion by binding to receptors on the surface of pancreatic beta cells, triggering a series of reactions which leads to insulin secretion. Because SUs cause circulating insulin levels to increase, there is a risk of hypoglycemia. There is also some concern that increased insulin levels are associated with cardiovascular disease, however the UKPDS did not show a relationship between increased mortality and SU administration. Finally, there is concern that SUs will exhaust beta cell function by increasing insulin secretion. However, the decline in beta cell function is more likely caused by the disease itself, and not the use of SUs. First generation sulfonylureas are just as efficacious as the second generation drugs, however the second generation may be more potent and safer than first. When diet and exercise fail, SUs are an effective monotherapy.")
87
Commonly used Sulfonylureas: dosage data
Gliclazide 30 mg ril modificato 80 mg 1-2 die AACE Diabetes Guidelines, Endocr Pract. 2002

88
Alpha-glucosidase Inhibitors
Alpha-glucosidase inhibitors block the enzymes that digest starches in the small intestine Efficacy Decrease peak postprandial glucose mg/dl ( mmol/L) Decrease fasting plasma glucose mg/dl ( mmol/L) Decrease A1C % Other Effects Flatulence or abdominal discomfort No specific effect on lipids or blood pressure No weight gain Contraindicated in patients with inflammatory bowel disease or cirrhosis Medications in this Class: acarbose (Precose), miglitol (Glyset) Alpha-glucosidase inhibitors (AGIs) work by blocking the enzyme in the small intestine that breaks down complex carbohydrates, alpha-glucosidase. By blocking this enzyme these drugs prevent starches from being absorbed into the bloodstream and in doing so lower blood glucose levels. AGIs are the only drug class used to treat type 2 diabetes that does not specifically target the pathology of the disease. Because AGIs work in the digestive tract, they are more effective at lowering postprandial glucose levels than fasting plasma glucose levels. On average, AGIs are less effective at lowering A1c levels than biguanides or sulfonylureas. What makes this class of drug attractive to patients and physicians is it's disassociation with weight gain and hypoglycemia. However, it is known to cause abdominal discomfort and diarrhea. AGIs are also rarely used as monotherapy because of their low efficacy.
 Decrease fasting plasma glucose mg/dl ( mmol/L) Decrease A1C % Other Effects. Flatulence or abdominal discomfort. No specific effect on lipids or blood pressure. No weight gain. Contraindicated in patients with inflammatory bowel disease or cirrhosis. Medications in this Class: acarbose (Precose), miglitol (Glyset) Alpha-glucosidase inhibitors (AGIs) work by blocking the enzyme in the small intestine that breaks down complex carbohydrates, alpha-glucosidase. By blocking this enzyme these drugs prevent starches from being absorbed into the bloodstream and in doing so lower blood glucose levels. AGIs are the only drug class used to treat type 2 diabetes that does not specifically target the pathology of the disease. Because AGIs work in the digestive tract, they are more effective at lowering postprandial glucose levels than fasting plasma glucose levels. On average, AGIs are less effective at lowering A1c levels than biguanides or sulfonylureas. What makes this class of drug attractive to patients and physicians is it s disassociation with weight gain and hypoglycemia. However, it is known to cause abdominal discomfort and diarrhea. AGIs are also rarely used as monotherapy because of their low efficacy.")
89
Alpha-glucosidasi Inhibitors : dosage data
AACE Diabetes Guidelines, Endocr Pract. 2002

90
Meglitinides Meglitinides stimulate insulin secretion (rapidly and for a short duration) in the presence of glucose. Efficacy Decreases peak postprandial glucose Decreases plasma glucose mg/dl ( mmol/L) Reduce A1C % Other Effects Hypoglycemia (although may be less than with sulfonylureas if patient has a variable eating schedule) Weight gain No significant effect on plasma lipid levels Safe at higher levels of serum Cr than sulfonylureas Medications in this Class: repaglinide (Novonorm), nateglinide (Starlix) Vanno somministrati 30 min prima dei pasti The mechanism of action of repaglinide is similar to that of the sulfonylurea drugs: binding to beta cell receptors to stimulate insulin secretion. The major difference between the two drug classes is that meglitinides are shorter-acting, and are most effective when taken after meals in the presence of glucose. Adverse effects include weight gain and hypoglycemia. An additional drawback to this drug is the dosing schedule since it must be taken with meals.
 Reduce A1C % Other Effects. Hypoglycemia (although may be less than with sulfonylureas if patient has a variable eating schedule) Weight gain. No significant effect on plasma lipid levels. Safe at higher levels of serum Cr than sulfonylureas. Medications in this Class: repaglinide (Novonorm), nateglinide (Starlix) Vanno somministrati 30 min prima dei pasti. The mechanism of action of repaglinide is similar to that of the sulfonylurea drugs: binding to beta cell receptors to stimulate insulin secretion. The major difference between the two drug classes is that meglitinides are shorter-acting, and are most effective when taken after meals in the presence of glucose. Adverse effects include weight gain and hypoglycemia. An additional drawback to this drug is the dosing schedule since it must be taken with meals.")
91
Quando prescrivere l’insulina
Mancato raggiungimento di valori target di glicemia (a digiuno e/o postprandiali) e di HbA1c nonostante terapia con antidiabetici orali (monoterapia o terapia di associazione) Presenza di grave sintomatologia (specialmente al momento della diagnosi) o in presenza di chetoacidosi diabetica JAMA 2007
 e di HbA1c nonostante terapia con antidiabetici orali (monoterapia o terapia di associazione) Presenza di grave sintomatologia (specialmente al momento della diagnosi) o in presenza di chetoacidosi diabetica. JAMA")
92
Hirsch IB, 2005

93
Hirsch IB, 2005

94
Algorithm for the metabolic management of type 2 diabetes
ADA/EASD Consensus Statement Tier 1: Well-validated core therapies At diagnosis: Lifestyle + Metformin Lifestyle + Metformin + Basal insulin Lifestyle + Metformin + Intensive insulin Lifestyle + Metformin + Sulfonylureaa STEP 1 STEP 2 STEP 3 Tier 2: Less well-validated therapies Lifestyle + Metformin + Pioglitazone Lifestyle + Metformin + Pioglitazone Sulfonylureaa -glucosidase inhibitors (e.g. acarbose) – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2 Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2 Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2 Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. No hypoglycemia Oedema/CHF Bone loss Lifestyle + Metformin + GLP-1 agonistb Lifestyle + Metformin + Basal insulin No hypoglycemia Weight loss Nausea/vomiting aOther than glibenclamide or chlorpropamide bInsufficient clinical use to be confident regarding safety Nathan et al. Diabetes Care 31:1-11, 2008
 – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2. Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2. Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2. Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2. 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. No hypoglycemia. Oedema/CHF. Bone loss. Lifestyle + Metformin. + GLP-1 agonistb. Lifestyle + Metformin. + Basal insulin. No hypoglycemia. Weight loss. Nausea/vomiting. aOther than glibenclamide or chlorpropamide. bInsufficient clinical use to be confident regarding safety. Nathan et al. Diabetes Care 31:1-11,")
96
Aspetti peculiari nelle gestione
del paziente diabetico anziano

97
In Anamnesi Patologica Remota
Paziente di sesso femminile di 75 anni, pensionata, vedova, ex contabile, attiva nel volontariato. Ipertesa, ipercolesterolemica, osteoporotica In Anamnesi Patologica Remota Diabete mellito tipo 2 (riscontro determinato dalla presenza di disuria e vaginite) da 10 anni Nessuna complicanza macro e micro-vascolare apparente Caso clinico-2 Durso SC, JAMA, 2006
 da 10 anni. Nessuna complicanza macro e micro-vascolare apparente. Caso clinico-2. Durso SC, JAMA,")
98
Attuale controllo glico-metabolico e terapia in atto
Glicemia 130 mg/dl (7.2 mmol/L), HbA1C 7.9% Fin dall’esordio counseling su stile di vita Automonitoraggio stick glicemici Da due anni trattamento con insulina, ASA, ace-inibitori, atorvastatina, calcio, vit D e bifosfonati Caso clinico-2 Durso SC, JAMA, 2006
, HbA1C 7.9% Fin dall’esordio counseling su stile di vita. Automonitoraggio stick glicemici. Da due anni trattamento con insulina, ASA, ace-inibitori, atorvastatina, calcio, vit D e bifosfonati. Caso clinico-2. Durso SC, JAMA,")
99
La signora presenta: PAO: 136/84 mmHg
BMI 24 Kg/m² (era 28.4) , W=78 cm (era 86) Colesterolo totale= 185 mg/dl (4.8 mmol/L), LDL-Ch= 110 mg/dl (2.8 mmol/L), HDL-Ch 50 mg/dl (0.8 mmol/L), trigliceridi 120 mg/dl (1.4 mmol/L), creatinina 1.2 mg/dl Funzionalità renale ed esame oftalmologico. Micro-aneurismi ed emorragie. Cammina 4 km die ed esegue esercizi di resistenza indipendente in ADL e IADL. MMSE: 30/30 Caso clinico-2 Durso SC, JAMA, 2006
 , W=78 cm (era 86) Colesterolo totale= 185 mg/dl (4.8 mmol/L), LDL-Ch= 110 mg/dl (2.8 mmol/L), HDL-Ch 50 mg/dl (0.8 mmol/L), trigliceridi 120 mg/dl (1.4 mmol/L), creatinina 1.2 mg/dl. Funzionalità renale ed esame oftalmologico. Micro-aneurismi ed emorragie. Cammina 4 km die ed esegue esercizi di resistenza. indipendente in ADL e IADL. MMSE: 30/30. Caso clinico-2. Durso SC, JAMA,")
100
In Anamnesi Patologica Remota
Paziente di sesso femminile di 75 anni, pensionata, casalinga, vedova, vive con il figlio Ipertesa, IMA, scompenso cardiaco classe NYHA III, decadimento cognitivo iniziale In Anamnesi Patologica Remota Diabete mellito tipo 2 da 5 anni Incontinenza urinaria Ansia e depressione Caso clinico-3 Durso SC, JAMA, 2006

101
La signora presenta: PAO: 154/92 mmHg BMI 30 Kg/m², W=95 cm
Colesterolo totale= 225 mg/dl (5.8 mmol/L), LDL- Ch= 130 mg/dl (3.4 mmol/L), HDL-Ch 45 mg/dl (1.2 mmol/L), trigliceridi 250 mg/dl, creatinina 1.5 mg/dl esame oftlmologico nella norma difficoltà nella deambulazione e instabilità nella marcia indipendente in ADL. Necessita di aiuto nelle IADL. MMSE: 23/30 Caso clinico-3 Durso SC, JAMA, 2006
, LDL- Ch= 130 mg/dl (3.4 mmol/L), HDL-Ch 45 mg/dl (1.2 mmol/L), trigliceridi 250 mg/dl, creatinina 1.5 mg/dl. esame oftlmologico nella norma. difficoltà nella deambulazione e instabilità nella marcia. indipendente in ADL. Necessita di aiuto nelle IADL. MMSE: 23/30. Caso clinico-3. Durso SC, JAMA,")
102
Attuale controllo glico-metabolico e terapia in atto
Glicemia 170 mg/dl (9.4 mmol/L), HbA1C 10% fin dall’esordio counseling su stile di vita Da due anni trattamento con Glyburide , ace-inibitori, atorvastatina, ASA, calcio, vit D, furosemide Caso clinico-3 Durso SC, JAMA, 2006
, HbA1C 10% fin dall’esordio counseling su stile di vita. Da due anni trattamento con Glyburide , ace-inibitori, atorvastatina, ASA, calcio, vit D, furosemide. Caso clinico-3. Durso SC, JAMA,")
103
Finland Diabetologia 29:611,1986 Australia Med. J. Aus. 143:436,1985
NHANES II Diabetes 36:523,1987 U. K. Diab. Med. 3:338,1986 Finland Diabetologia 29:611,1986 Australia Med. J. Aus. 143:436,1985 % popolazione 50 40 30 20 10 20-44 45-54 55-64 65-74 >80 65-84 >65 >75 età I G T Diabete mellito

104
DIABETES RISK FACTORS IN AGEING
Decreased physical activity INSULIN RESISTANCE Increased adiposity Impaired adaptation No insulin Progression to IGTand type 2 diabetes Age effects on insulin action Medication DECREASED INSULIN SECRETION Genetics Coexisting illness Age effects on Beta cells Chang AM, Am J Physiol Endocrinol Metab 2003

105
Meneilly , J Clin Endocrinol Metab 84: 1938–1943, 1999
INSULIN RELEASE DURING GLUCOSE STIMULUS IN THE ELDERLY Meneilly , J Clin Endocrinol Metab 84: 1938–1943, 1999

106
INSULIN ACTION AND AGE Ferrannini et al. Diabetes 45: 947-953, 1996
mmol kg-1min-1

107
Clinical and Functional Eterogeneity of Elderly T2DM
Older individuals may have developed diabetes years earlier and may have significant complications Newly diagnosed may have had years of undiagnosed diabetes with resultant complications or may have few complications from the disease Older adults with diabetes may be frail and have other underlying chronic conditions, substantial diabetes-related comorbidity, or limited physical or cognitive functioning Older individuals with diabetes have little comorbidity and are active Life expectancies are highly variable for this population, but often longer than clinicians realize -glucosidase inhibitors (e.g. acarbose) – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2 Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2 Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2 Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. American Diabetes Association: Standards of Medical Care in Diabetes—2008; Diabetes Care 31:S12-S54, 2008
 – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2. Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2. Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2. Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2. 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. American Diabetes Association: Standards of Medical Care in Diabetes—2008; Diabetes Care 31:S12-S54,")
108
Diabete e Problematiche Geriatriche
Valutare nel paziente anziano diabetico la presenza di: Polifarmacoterapia Depressione Decadimento cognitivo Incontinenza urinaria Cadute accidentali f. Dolore Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003

109
Diabete ed Intervento Comportamentale
Valutare regolarmente il livello di attività fisica e informare il paziente sui benefici di attività fisica regolare. Valutare le abitudini alimentari, iniziare trattamento dietologico ed informare il paziente sui benefici della riduzione del peso corporeo (IA). 2. Sospensione del fumo (IIA). Bisogna fornire ai pazienti diabetici, ai familiari e/o ai caregivers le seguenti informazioni sulla ipo- o iper-glicemia (IA): i. Fattori precipitanti. ii. Prevenzione. iii. Sintomi. iv. Trattamento. v. Quando si deve contattare il medico. 4. Ogni volta che si prescrive un nuovo farmaco, informare il paziente o il caregiver sull’utilità, modalità d’assunzione, effetti collaterali comuni e reazioni avverse (IIIA) Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003
. 2. Sospensione del fumo (IIA). Bisogna fornire ai pazienti diabetici, ai familiari e/o ai caregivers le seguenti informazioni sulla ipo- o iper-glicemia (IA): i. Fattori precipitanti. ii. Prevenzione. iii. Sintomi. iv. Trattamento. v. Quando si deve contattare il medico. 4. Ogni volta che si prescrive un nuovo farmaco, informare il paziente o il caregiver sull’utilità, modalità d’assunzione, effetti collaterali comuni e reazioni avverse (IIIA) Guidelines for improving the Care of the Older Person with Diabetes Mellitus. JAGS,")
110
Diabete e CONTROLLO GLICEMICO
Come per i giovani adulti, per i pazienti anziani, il valore dell’Hb-glicata < 7%, indica un buon controllo glicemico. Pazienti con scarso controllo glicemico, l’Hb-glicata deve essere controllata almeno ogni 6 mesi . Per i pazienti con valori di Hb-glicata stabili da anni il controllo può essere eseguito ogni 12 mesi (IIIB). 2. L’uso di metformina è controindicato nei pazienti diabetici con aumentati livelli di creatinina sierica (uomini ≥ 1.5 mg/dl, donne ≥ 1.4 mg/dl) o con ridotti valori della clearance di creatinina (IIB), per evitare l’acidosi metabolica. Nei pazienti anziani che assumono metformina, il valore della creatinina sierica deve essere controllato ogni 12 mesi. Nei pazienti con età superiore a 80 anni o con ridotta massa muscolare bisogna monitorare la clearance della creatinina. Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003
. 2. L’uso di metformina è controindicato nei pazienti diabetici con aumentati livelli di creatinina sierica (uomini ≥ 1.5 mg/dl, donne ≥ 1.4 mg/dl) o con ridotti valori della clearance di creatinina (IIB), per evitare l’acidosi metabolica. Nei pazienti anziani che assumono metformina, il valore della creatinina sierica deve essere controllato ogni 12 mesi. Nei pazienti con età superiore a 80 anni o con ridotta massa muscolare bisogna monitorare la clearance della creatinina. Guidelines for improving the Care of the Older Person with Diabetes Mellitus. JAGS,")
111
Diabete e CONTROLLO GLICEMICO
Per i pazienti anziani, il valore dell’Hb-glicata < 8%, può essere<accettato quando la spettanza di vita è < 5 anni Il frequente auto-monitoraggio della glicemia riduce il rischio di ipoglicemia 2. Gli anziani più a rischio di ipoglicemia sono quelli più fragili Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003

112
Factors influencing targets
and OHA choice Life expectancy <5 yrs Functional and cognitive impairment Life-limiting comorbidities Polytherapy Diabetic complications Long life expectancy Active Good functional status Otherwise healthy Few therapies No comorbidities No complications -glucosidase inhibitors (e.g. acarbose) – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2 Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2 Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2 Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. HbA1c = 8% HbA1c < 7% Most OHA contraindicated All OHA recommended American Geriatrics Society: Guidelines for improving the care of the older person with diabetes mellitus; J Am Geriatr Soc 2003; 51:S265–S280
 – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2. Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2. Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2. Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2. 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. HbA1c = 8% HbA1c < 7% Most OHA contraindicated. All OHA recommended. American Geriatrics Society: Guidelines for improving the care of the older person with diabetes mellitus; J Am Geriatr Soc 2003; 51:S265–S280.")
113
Diabete ed IPERTENSIONE
PA ≤ 140/80 mmHg, se tollerata dal paziente non necessita terapia farmacologica (IA). La riduzione della PA deve essere graduale (IIIA). Con il trattamento farmacologico e con l’intervento comportamentale sui fattori di rischio, la PA deve essere ridotta in: -tre mesi, se PAS è tra mmHg e PAD tra mmHg - un mese se PAS > 160, PAD > 100 e. Controllo della funzionalità renale e della ionemia entro 1-2 settimane dall’inizio del trattamento antiipertensivo con l’utilizzo di ACE-inibitori, sartanici, diuretici dell’ansa o tiazidici. Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003
. La riduzione della PA deve essere graduale (IIIA). Con il trattamento farmacologico e con l’intervento comportamentale sui fattori di rischio, la PA deve essere ridotta in: -tre mesi, se PAS è tra mmHg e PAD tra mmHg. - un mese se PAS > 160, PAD > 100. e. Controllo della funzionalità renale e della ionemia entro 1-2 settimane dall’inizio del trattamento antiipertensivo con l’utilizzo di ACE-inibitori, sartanici, diuretici dell’ansa o tiazidici. Guidelines for improving the Care of the Older Person with Diabetes Mellitus. JAGS,")
114
Diabete e LIPIDI (1) Nei pazienti diabetici, bisogna monitorare ed eventualmente correggere i valori lipidici (IA): a. LDL ≤ 100mg/dl: bisogna monitorare i valori lipidici ogni 2 anni b. LDL tra mg/dl: i. raccomandare attività fisica e terapia dietetetica ii. monitorare i valori lipidici almeno ogni anno iii. Se LDL ≥ 100 mg/dl dopo 6 mesi di terapia dietetica, valutare terapia farmacologica c. LDL ≥ 130 mg/dl: i. iniziare terapia farmacologica, dietetica ed attività fisica. ii. controllare i valori lipidici almeno ogni 12 mesi iii. monitorare la risposta alla terapia Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003

115
Diabete e LIPIDI (2) Diabete e ASPIRINA
TG ≥ 150 mg/dl: iniziare terapia dietetica e valutare terapia con fibrati. Nei pazienti trattati con statine o fibrati, bisogna monitorare gli enzimi epatici all’inizio della terapia, ogni anno o al cambiamento della terapia farmacologica (IIIB). Diabete e ASPIRINA 1. Pazienti anziani diabetici (che non assumono nessuna terapia anticoagulante e senza controindicazioni all’assunzione di aspirina) dovrebbero assumere giornalmente aspirina ( mg/ die) (IB).
. Diabete e ASPIRINA. 1. Pazienti anziani diabetici (che non assumono nessuna terapia anticoagulante e senza controindicazioni all’assunzione di aspirina) dovrebbero assumere giornalmente aspirina ( mg/ die) (IB).")
116
Diabete e OCCHIO Bisogna eseguire l’esame del fondo dell’occhio in pazienti con recente insorgenza di DM (IB). Persone a basso rischio di oculopatia: fondo dell’occhio ogni 2 anni (IIB). Persone ad alto rischio di oculopatia: fondo dell’occhio almeno ogni anno - segni di retinopatia, glaucoma o cataratta -Hb-glicata ≥ 8%, -DM tipo 1 -PA ≥ 140/80 mmHg Alto rischio di oculopatia
. Persone ad alto rischio di oculopatia: fondo dell’occhio almeno ogni anno. - segni di retinopatia, glaucoma o cataratta. -Hb-glicata ≥ 8%, -DM tipo 1. -PA ≥ 140/80 mmHg. Alto rischio di oculopatia.")
117
Diabete e PIEDI Diabete e NEFROPATIA
Pazienti anziani diabetici devono effettuare visita annuale per controllare integrità della cute e in caso di presenza di deformità ossee, perdità di sensibilità o diminuita perfusione vascolaretali controlli devono essere più frequenti (IIIA). Diabete e NEFROPATIA Bisogna eseguire il test per dosare la presenza di microalbuminuria in pazienti con recente diagnosi di diabete mellito. Tale test va ripetuto annualmente (IIIA).
. Diabete e NEFROPATIA. Bisogna eseguire il test per dosare la presenza di microalbuminuria in pazienti con recente diagnosi di diabete mellito. Tale test va ripetuto annualmente (IIIA).")
118
I. Diabete e Problematiche Geriatriche
Valutare nel paziente anziano diabetico la presenza di: Polifarmacoterapia Depressione Decadimento cognitivo Incontinenza urinaria Cadute accidentali f. Dolore Guidelines for improving the Care of the Older Person with Diabetes Mellitus JAGS, 2003

119
Primary aims for the care of the older adult with diabetes
1. Elimination of symptoms of uncontrolled hyperglycemia and avoiding treatment related hypoglycemia 2. Individualization of care, taking into account the patient’s longevity, personalized glucose goals, financial resources, and life situation 3. Attention to nonglycemic risk factors that contribute to cardiovascular mortalitiy, namely blood pressure, dyslipidemia, tobacco use, and physical inactivity -glucosidase inhibitors (e.g. acarbose) – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2 Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2 Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2 Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. American Diabetes Association: Standards of Medical Care in Diabetes—2008; Diabetes Care 31:S12-S54, 2008
 – delay digestion and absorption of carbohydrates in the gastrointestinal tract.1,2. Sulfonylureas and meglitinides – stimulate insulin secretion from the pancreas.1,2. Biguanides (e.g. metformin) – suppress liver glucose output, enhance insulin sensitivity in the liver and stimulate insulin-mediated glucose disposal. They do not stimulate insulin secretion.1,2. Thiazolidinediones – decrease insulin resistance in fat, muscle and liver. In addition, they improve estimates of -cell function.1,2. 1Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl. 1):S32–S40. 2Nattrass M & Bailey CJ. Baillieres Best Pract Res Clin Endocrinol Metab 1999; 13:309–329. American Diabetes Association: Standards of Medical Care in Diabetes—2008; Diabetes Care 31:S12-S54,")
120
Reasons for increased rate of hypoglycemia in elderly diabetics
Decrease in hepatic oxidative enzyme activity Age-related decline in renal function Less protective hormonal CR funtion Loss of symptom recognition (hypoglycemia unawereness) Inadequate education regarding signs and symptoms of hypoglycemia Prevalence of Hypertension in the US The prevalence of hypertension in a representative sample from the National Health and Nutritional Examination Survey (NHANES III, phases 1 and 2) reveals that approximately 25% of the US adult population has hypertension, and the prevalence of hypertension increases sharply with advancing age. NHANES III was a national examination study conducted in the US with the goals of: estimating the prevalence of selected diseases and risk factors; estimating population reference distributions of certain health parameters; documenting and investigating reasons for secular trends in selected diseases and risk factors; contributing to an understanding of disease etiology; and investigating the natural history of selected diseases. The NHANES III sample was selected from 81 counties between 1988 and 1994. Reference: The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157(21):
 Inadequate education regarding signs and symptoms of hypoglycemia. Prevalence of Hypertension in the US. The prevalence of hypertension in a representative sample from the National Health and Nutritional Examination Survey (NHANES III, phases 1 and 2) reveals that approximately 25% of the US adult population has hypertension, and the prevalence of hypertension increases sharply with advancing age. NHANES III was a national examination study conducted in the US with the goals of: estimating the prevalence of selected diseases and risk factors; estimating population reference distributions of certain health parameters; documenting and investigating reasons for secular trends in selected diseases and risk factors; contributing to an understanding of disease etiology; and investigating the natural history of selected diseases. The NHANES III sample was selected from 81 counties between 1988 and Reference: The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157(21):")
121
Disease management: caso clinico 2
Life Expenctancy: vicino al più alto quartile per la sua età (25% donne 75 anni 17 anni, 50% 12 anni, 25% 7 anni o meno) Individualmente interessata alla “medicina preventiva” Screening per sindromi geriatriche: negativa Candidata a: stretto controllo metabolico e pressorio: presenza di retinopatia ulteriore motivazione Target PA < 130/80 , HbA < 7%, lipidi sec ATP III Scarsa preoccupazione per l’ipoglicemia
 Individualmente interessata alla medicina preventiva Screening per sindromi geriatriche: negativa. Candidata a: stretto controllo metabolico e pressorio: presenza di retinopatia ulteriore motivazione. Target PA < 130/80 , HbA < 7%, lipidi sec ATP III. Scarsa preoccupazione per l’ipoglicemia.")
122
Disease management: caso clinico 3
Life Expenctancy: vicino al più basso quartile per la sua età (25% donne 75 anni: 17 anni, 50% 12 anni, 25% 7 anni o meno) Individualmente interessata alla “feel well” e rimanere indipendente Screening per sindromi geriatriche: positiva per deterioramento cognitivo Polifarmacoterapia, Depressione, Incontinenza urinaria Candidata a: terapia anti-depressiva,correzione cauta della PA, moderato controllo dei valori glicemici al fine di ridurre i sintomi da iperglicemia Target, HbA 8 %, Target lipidi secondo ATP III elevata preoccupazione per l’ipoglicemia
 Individualmente interessata alla feel well e rimanere indipendente. Screening per sindromi geriatriche: positiva per deterioramento cognitivo Polifarmacoterapia, Depressione, Incontinenza urinaria. Candidata a: terapia anti-depressiva,correzione cauta della PA, moderato controllo dei valori glicemici al fine di ridurre i sintomi da iperglicemia. Target, HbA 8 %, Target lipidi secondo ATP III. elevata preoccupazione per l’ipoglicemia.")
Presentazioni simili
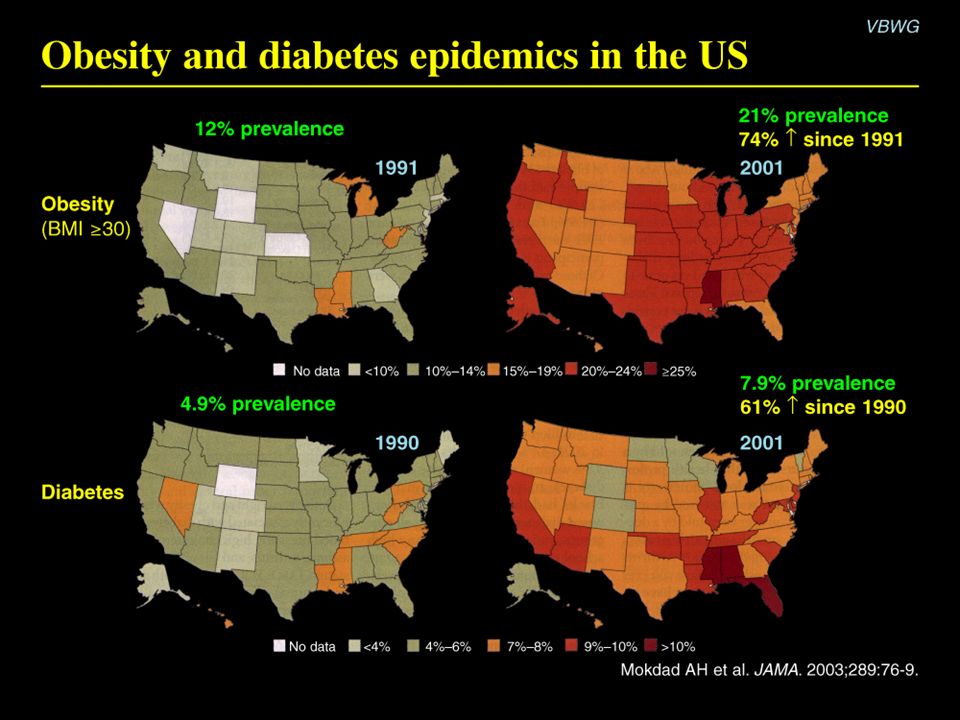
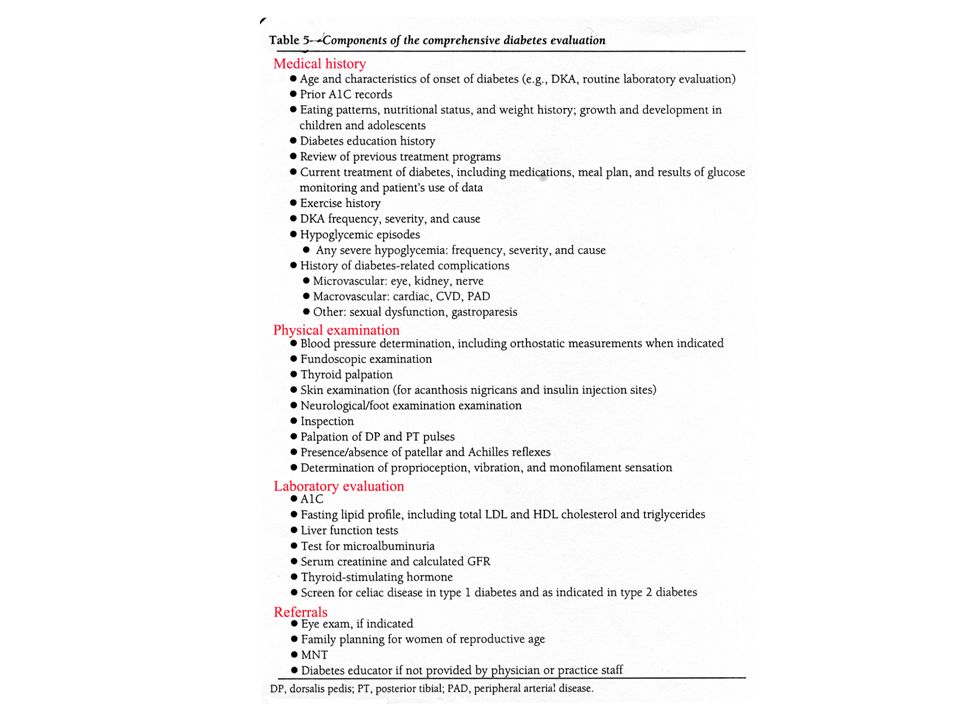







 ha smesso nel Impiegato. Diabete mellito tipo 2 noto dal 1993, in trattamento con ipoglicemizzanti.>")

 pregestazionale>")




 STEATOSI CIRROSI (8-25%) HCC.>")






 Area Prevenzione ANMCO>")