Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Nuove prospettive nel campo della Resincronizzazione Cardiaca (CRT)
Tullio Agricola Ospedale Spirito Santo Pescara

2
Prevalenza dei ritardi di conduzione inter- o intraventricolari nei pts con scompenso
Popolazione con scompenso in generale1,2 Popolazione con scompenso moderato o severo 3,4,5 IVCD 15% IVCD >30% IVCD >30% IVCD 15% Approximately 15% of all heart failure patients have an inter- or intraventricular conduction delay (QRS > 120 msec)1-2. Over 30% of moderate to severe heart failure patients have a prolonged QRS. The prevalence of conduction defects increases with severity of heart failure.3-5 Shenkman and colleagues found the factors associated with prolonged QRS included: Older age, Male gender, Caucasian race, Lower EF, Higher LVESD 1 Havranek EP, Masoudi FA, Westfall KA, Wolfe P, Ordin DL, Krumholz HM. Spectrum of heart failure in older patients: Results from the National Heart Failure Project. Am Heart J 2002;143: 2 Shenkman HJ, McKinnon JE, Khandelwal AK, et al. Determinants of QRS Prolongation in a Generalized Heart Failure Population: Findings from the Conquest Study [Abstract 2993]. Circulation 2000;102(18 Suppl II) 3 Schoeller R, Andersen D, Buttner P, Oezcelik K, Vey G, Schroder R. First-or second-degree atrioventricular block as a risk factor in idiopathic dilated cardiomyopathy. Am J Cardiol 1993;71: 4 Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development & prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation 1997; 95: 5 Farwell D, Patel NR, Hall A, Ralph S, Sulke AN. How many people with heart failure are appropriate for biventricular resynchronization? Eur Heart J 2000;21: 1 Havranek E, Masoudi F, Westfall K, et al. Am Heart J 2002;143: 2 Shenkman H, McKinnon J, Khandelwal A, et al. Circulation 2000;102(18 Suppl II): abstract 2293 3 Schoeller R, Andersen D, Buttner P, et al. Am J Cardiol. 1993;71: 4 Aaronson K, Schwartz J, Chen T, et al. Circulation 1997;95: 5 Farwell D, Patel N, Hall A, et al. Eur Heart J 2000;21: September 2001
1-2. Over 30% of moderate to severe heart failure patients have a prolonged QRS. The prevalence of conduction defects increases with severity of heart failure.3-5 Shenkman and colleagues found the factors associated with prolonged QRS included: Older age, Male gender, Caucasian race, Lower EF, Higher LVESD 1 Havranek EP, Masoudi FA, Westfall KA, Wolfe P, Ordin DL, Krumholz HM. Spectrum of heart failure in older patients: Results from the National Heart Failure Project. Am Heart J 2002;143: Shenkman HJ, McKinnon JE, Khandelwal AK, et al. Determinants of QRS Prolongation in a Generalized Heart Failure Population: Findings from the Conquest Study [Abstract 2993]. Circulation 2000;102(18 Suppl II) 3 Schoeller R, Andersen D, Buttner P, Oezcelik K, Vey G, Schroder R. First-or second-degree atrioventricular block as a risk factor in idiopathic dilated cardiomyopathy. Am J Cardiol 1993;71: Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development & prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation 1997; 95: Farwell D, Patel NR, Hall A, Ralph S, Sulke AN. How many people with heart failure are appropriate for biventricular resynchronization Eur Heart J 2000;21: Havranek E, Masoudi F, Westfall K, et al. Am Heart J 2002;143: Shenkman H, McKinnon J, Khandelwal A, et al. Circulation 2000;102(18 Suppl II): abstract Schoeller R, Andersen D, Buttner P, et al. Am J Cardiol. 1993;71: Aaronson K, Schwartz J, Chen T, et al. Circulation 1997;95: Farwell D, Patel N, Hall A, et al. Eur Heart J 2000;21: September")
3
Conseguenze Cliniche della Dissincronia Ventricolare
Movimento anormale della parete del setto interventricolare1 Ridotto dP/dt3 Tempo di riempimento diastolico ridotto1,2 Durata prolungata del rigurgito mitralico (MR)1,2 Key Messages: Ventricular dysynchrony has been associated with paradoxical septal wall motion, reduced LV pressure, prolonged mitral regurgitation duration, and reduced diastolic filling times in studies comparing patients with left bundle branch block with normals or with comparable patients without LBBB. Animation Filename: “4-chamber.avi”. The animation can be started by positioning the mouse-cursor over the image and clicking once. To stop or restart the animation video at anytime, click once on the image. Using simultaneous ECG, phonocardiogram, radionuclide ventriculograms, and 2D and M-mode echoes, Grines et al studied 18 patients with LBBB (and no other underlying cardiac disease) compared with 10 normals. In LBBB patients she found significant delays in LV systolic and diastolic events, reduced diastolic filling times, abnormal interventricular septal wall motion, and a loss of septal contribution to global ejection fraction. [Grines C, Bashore T, Boudoulas H, et al. Functional abnormalities in isolated left bundle branch block: the effect of interventricular asynchrony. Circulation 1989;79: ]. Xiao et al (1991) in a study of 52 pts with DCM, 12 of whom had LBBB, found that those with LBBB had prolonged MR and shortened LV filling time. [ Xiao Lee C, Gibson D. effect of left bundle branch block on diastolic function in dilated cardiomyopathy. Br Heart J 1991;66: ] Xiao et al (1992) studied 50 DCM patients with functional MR, finding a positive correlation between QRS duration and MR duration, and negative correlation between QRS duration and the peak rate of rise in LV pressure. [Xiao H, Brecker S, Gibson D. Effects of abnormal activation on the time course of left ventricular pressure pulse in dilated cardiomyopathy. Br Heart J 1992;68: ]. Click to Start/Stop 1 Grines CL, Bashore TM, Boudoulas H, et al. Circulation 1989;79: 2 Xiao, HB, Lee CH, Gibson DG. Br Heart J 1991;66: 3 Xiao HB, Brecker SJD, Gibson DG. Br Heart J 1992;68: September 2001
1,2. Key Messages: Ventricular dysynchrony has been associated with paradoxical septal wall motion, reduced LV pressure, prolonged mitral regurgitation duration, and reduced diastolic filling times in studies comparing patients with left bundle branch block with normals or with comparable patients without LBBB. Animation Filename: 4-chamber.avi . The animation can be started by positioning the mouse-cursor over the image and clicking once. To stop or restart the animation video at anytime, click once on the image. Using simultaneous ECG, phonocardiogram, radionuclide ventriculograms, and 2D and M-mode echoes, Grines et al studied 18 patients with LBBB (and no other underlying cardiac disease) compared with 10 normals. In LBBB patients she found significant delays in LV systolic and diastolic events, reduced diastolic filling times, abnormal interventricular septal wall motion, and a loss of septal contribution to global ejection fraction. [Grines C, Bashore T, Boudoulas H, et al. Functional abnormalities in isolated left bundle branch block: the effect of interventricular asynchrony. Circulation 1989;79: ]. Xiao et al (1991) in a study of 52 pts with DCM, 12 of whom had LBBB, found that those with LBBB had prolonged MR and shortened LV filling time. [ Xiao Lee C, Gibson D. effect of left bundle branch block on diastolic function in dilated cardiomyopathy. Br Heart J 1991;66: ] Xiao et al (1992) studied 50 DCM patients with functional MR, finding a positive correlation between QRS duration and MR duration, and negative correlation between QRS duration and the peak rate of rise in LV pressure. [Xiao H, Brecker S, Gibson D. Effects of abnormal activation on the time course of left ventricular pressure pulse in dilated cardiomyopathy. Br Heart J 1992;68: ]. Click to Start/Stop. 1 Grines CL, Bashore TM, Boudoulas H, et al. Circulation 1989;79: Xiao, HB, Lee CH, Gibson DG. Br Heart J 1991;66: Xiao HB, Brecker SJD, Gibson DG. Br Heart J 1992;68: September")
4
Epidemiology, Prognosis, and Pathophysiology of Heart Failure
In the EuroHeart Failure survey, 36% of those who had LV function assessed had an LVEF ≤ 35% and, of these, 41% had a QRS duration ≥120 ms; 7% had RBBB, 34% had LBBB or other intraventricular conduction delay (IVCD) and 17% had QRS ≥150 ms In the Italian Network on CHF (IN-CHF) registry, 1391 patients (25%) had complete LBBB, 336 (6%) had complete RBBB and 339 (6%) had other forms of IVCD. The annual incidence of LBBB is about 10% in ambulatory patients with left ventricular systolic dysfunction (LVSD) and chronic HF 2013 ESCGuidelines on cardiac pacing and cardiac resynchronization therapy
 and 17% had QRS ≥150 ms. In the Italian Network on CHF (IN-CHF) registry, 1391 patients (25%) had complete LBBB, 336 (6%) had complete RBBB and 339 (6%) had other forms of IVCD. The annual incidence of LBBB is about 10% in ambulatory patients with left ventricular systolic dysfunction (LVSD) and chronic HF ESCGuidelines on cardiac pacing and cardiac resynchronization therapy.")
5
Normal Heart The activation sequence in the normal heart (Top) and with left bundle branch block (LBBB) conduction defect (Bottom) is presented; the anterior wall of the ventricle is flipped open and placed (cavity en face) on the right. The activation sequence is represented by the time scale color bar; the activation spreads in a wave front, with each colored zone representing successive 10 to 20 ms. During normal conduction, activation begins within both the left ventricular (LV) and right ventricular endocardium but in LBBB, activation begins only in the right ventricle and proceeds through the septum before reaching the LV endocardium. The line of activation sequence block in the anterior wall in LBBB is shown by a dashed line (between substantially different time zones). The normal electromechanical activation sequence of the LV develops from a close interaction of the specialized conduction system with the myocyte architecture. Nearly the entire LV endocardial layer is directly activated within approximately 40 ms by Purkinje cells (Fig. 1) (1). The epicardial layer, which is void of Purkinje cells, experiences delayed activation through cell-to-cell propagation of electrical activity. LBBB J Am Coll Cardiol Img. 2013;6(8): doi: /j.jcmg
 and with left bundle branch block (LBBB) conduction defect (Bottom) is presented; the anterior wall of the ventricle is flipped open and placed (cavity en face) on the right. The activation sequence is represented by the time scale color bar; the activation spreads in a wave front, with each colored zone representing successive 10 to 20 ms. During normal conduction, activation begins within both the left ventricular (LV) and right ventricular endocardium but in LBBB, activation begins only in the right ventricle and proceeds through the septum before reaching the LV endocardium. The line of activation sequence block in the anterior wall in LBBB is shown by a dashed line (between substantially different time zones). The normal electromechanical activation sequence of the LV develops from a close interaction of the specialized conduction system with the myocyte architecture. Nearly the entire LV endocardial layer is directly activated within approximately 40 ms by Purkinje cells (Fig. 1) (1). The epicardial layer, which is void of Purkinje cells, experiences delayed activation through cell-to-cell propagation of electrical activity. LBBB. J Am Coll Cardiol Img. 2013;6(8): doi: /j.jcmg")
6
Posizionamento del catetere ventricolare sinistro
1. Vena cardiaca Laterale (marginale) 2. Vena cardiaca Postero-laterale 3. Vena cardiaca Posteriore 4. Vena cardiaca Media 5. Vena cardiaca Grande 1 5 2 3 4
 2. Vena cardiaca Postero-laterale. 3. Vena cardiaca Posteriore. 4. Vena cardiaca Media. 5. Vena cardiaca Grande")
7
La Stimolazione Biventricolare (CRT)
")
8
Modificazione del complesso QRS con la stimolazione biventricolare
Spontaneo CRT September 2001

9
Effetto della CRT sulla funzione cardiaca
Movimento anormale della parete del setto interventricolare1 Ridotto dP/dt3 Tempo di riempimento diastolico ridotto1,2 Durata prolungata del rigurgito mitralico (MR)1,2 Key Messages: Ventricular dysynchrony has been associated with paradoxical septal wall motion, reduced LV pressure, prolonged mitral regurgitation duration, and reduced diastolic filling times in studies comparing patients with left bundle branch block with normals or with comparable patients without LBBB. Animation Filename: “4-chamber.avi”. The animation can be started by positioning the mouse-cursor over the image and clicking once. To stop or restart the animation video at anytime, click once on the image. Using simultaneous ECG, phonocardiogram, radionuclide ventriculograms, and 2D and M-mode echoes, Grines et al studied 18 patients with LBBB (and no other underlying cardiac disease) compared with 10 normals. In LBBB patients she found significant delays in LV systolic and diastolic events, reduced diastolic filling times, abnormal interventricular septal wall motion, and a loss of septal contribution to global ejection fraction. [Grines C, Bashore T, Boudoulas H, et al. Functional abnormalities in isolated left bundle branch block: the effect of interventricular asynchrony. Circulation 1989;79: ]. Xiao et al (1991) in a study of 52 pts with DCM, 12 of whom had LBBB, found that those with LBBB had prolonged MR and shortened LV filling time. [ Xiao Lee C, Gibson D. effect of left bundle branch block on diastolic function in dilated cardiomyopathy. Br Heart J 1991;66: ] Xiao et al (1992) studied 50 DCM patients with functional MR, finding a positive correlation between QRS duration and MR duration, and negative correlation between QRS duration and the peak rate of rise in LV pressure. [Xiao H, Brecker S, Gibson D. Effects of abnormal activation on the time course of left ventricular pressure pulse in dilated cardiomyopathy. Br Heart J 1992;68: ]. Click to Start/Stop 1 Grines CL, Bashore TM, Boudoulas H, et al. Circulation 1989;79: 2 Xiao, HB, Lee CH, Gibson DG. Br Heart J 1991;66: 3 Xiao HB, Brecker SJD, Gibson DG. Br Heart J 1992;68: September 2001
1,2. Key Messages: Ventricular dysynchrony has been associated with paradoxical septal wall motion, reduced LV pressure, prolonged mitral regurgitation duration, and reduced diastolic filling times in studies comparing patients with left bundle branch block with normals or with comparable patients without LBBB. Animation Filename: 4-chamber.avi . The animation can be started by positioning the mouse-cursor over the image and clicking once. To stop or restart the animation video at anytime, click once on the image. Using simultaneous ECG, phonocardiogram, radionuclide ventriculograms, and 2D and M-mode echoes, Grines et al studied 18 patients with LBBB (and no other underlying cardiac disease) compared with 10 normals. In LBBB patients she found significant delays in LV systolic and diastolic events, reduced diastolic filling times, abnormal interventricular septal wall motion, and a loss of septal contribution to global ejection fraction. [Grines C, Bashore T, Boudoulas H, et al. Functional abnormalities in isolated left bundle branch block: the effect of interventricular asynchrony. Circulation 1989;79: ]. Xiao et al (1991) in a study of 52 pts with DCM, 12 of whom had LBBB, found that those with LBBB had prolonged MR and shortened LV filling time. [ Xiao Lee C, Gibson D. effect of left bundle branch block on diastolic function in dilated cardiomyopathy. Br Heart J 1991;66: ] Xiao et al (1992) studied 50 DCM patients with functional MR, finding a positive correlation between QRS duration and MR duration, and negative correlation between QRS duration and the peak rate of rise in LV pressure. [Xiao H, Brecker S, Gibson D. Effects of abnormal activation on the time course of left ventricular pressure pulse in dilated cardiomyopathy. Br Heart J 1992;68: ]. Click to Start/Stop. 1 Grines CL, Bashore TM, Boudoulas H, et al. Circulation 1989;79: Xiao, HB, Lee CH, Gibson DG. Br Heart J 1991;66: Xiao HB, Brecker SJD, Gibson DG. Br Heart J 1992;68: September")
10
Effetto della CRT sulla funzione cardiaca
Ottimizzazione intervallo AV Riduce il rigurgito mitralico1,2,3 Aumenta il tempo di riempimento diastolico Migliora il dP/dt del ventricolo sinistro Diastolic mitral regurgitation occurs with wide QRS as a result of delayed left ventricular activation and late initiation of the left lateral papillary muscle. Pre-emptive activation of the lateral wall of the left ventricle may lead to early activation of the papillary muscles and decreased mitral regurgitation. Video Filename: “mitral-regurg.avi” The animation can be started by positioning the mouse-cursor over the image and clicking once. To stop or restart the animation video at anytime, click once on the image. Nishimura RA, et al. Mechanism of hemodynamic improvement by dual chamber pacing for severe left ventricular dysfunction: an acute doppler and catheterization hemodynamic study. J Am Coll Cardiol 1995;25: pts with left ventricular systolic dysfunction (mean EF 19%, 7 ischemic, 8 idiopathic) studied acutely during AV sequential pacing at various AV intervals (60, 100,120, 140, 180, 240 ms). 4 had LBBB, 1 had RBBB, 2 were paced. Measured SBP, LA pressure, Tau, CO (thermodilution), diastolic filling period, LVEDP. Identified 8 pts with PR intervals > 200 ms who had improvement with optimal AV delay vs. baseline in CO, LVEDP, diastolic filling duration, and abolished diastolic MR. In remaining 7 pts, with normal AV conduction at rest, CO decreased during pacing and diastolic filling period did not change. Walker S, et al. Left ventricular remodeling with chronic biventricular pacing. Europace 2000;I (supplement D): abstract 212/5 21 HF pts with mean QRS of 171 ms. Echo study at baseline, after 3 months of BiV pacing, and immediately no pacing. MR area (cm2) was significantly improved with CR versus baseline (5.9±5.5 vs. 7.1±5.4, p<0.05), but there was no difference after 3 months of no CR (7.6±6.5) versus baseline. Brecker SJD, et al. Effects of dual chamber pacing with short atrioventricular delay in dilated cardiomyopathy. Lancet 1992;340: Acute study in 12 pts with DCM and LV or RV filling times < 200 ms due to MR or TR. 4 with permanent pacemaker. Of other 8 pts, 5 with PR interval > 200 ms, 5 with QRS > 120 ms, 4 with both. LV fill time = RR-MR duration. Measured HR, MR & TR durations, LV & RV filling times (= RR-MR or TR duration), and CO (by echo). Measurements at various AV intervals. Shortest AV delay was 6 ms in non pacemaker pts and 31 ms in PM pts. Best outcomes reported at shortest AV intervals. Increases in CO and exercise duration. 1 Nishimura et al. J Am Coll Cardiol. 1995; 25:281. 2 Walker et al. Europace 2000;I(suppl D): abstract 212/5. 3 Brecker et al. Lancet. 1992;340:1308. September 2001
 studied acutely during AV sequential pacing at various AV intervals (60, 100,120, 140, 180, 240 ms). 4 had LBBB, 1 had RBBB, 2 were paced. Measured SBP, LA pressure, Tau, CO (thermodilution), diastolic filling period, LVEDP. Identified 8 pts with PR intervals > 200 ms who had improvement with optimal AV delay vs. baseline in CO, LVEDP, diastolic filling duration, and abolished diastolic MR. In remaining 7 pts, with normal AV conduction at rest, CO decreased during pacing and diastolic filling period did not change. Walker S, et al. Left ventricular remodeling with chronic biventricular pacing. Europace 2000;I (supplement D): abstract 212/5. 21 HF pts with mean QRS of 171 ms. Echo study at baseline, after 3 months of BiV pacing, and immediately no pacing. MR area (cm2) was significantly improved with CR versus baseline (5.9±5.5 vs. 7.1±5.4, p<0.05), but there was no difference after 3 months of no CR (7.6±6.5) versus baseline. Brecker SJD, et al. Effects of dual chamber pacing with short atrioventricular delay in dilated cardiomyopathy. Lancet 1992;340: Acute study in 12 pts with DCM and LV or RV filling times < 200 ms due to MR or TR. 4 with permanent pacemaker. Of other 8 pts, 5 with PR interval > 200 ms, 5 with QRS > 120 ms, 4 with both. LV fill time = RR-MR duration. Measured HR, MR & TR durations, LV & RV filling times (= RR-MR or TR duration), and CO (by echo). Measurements at various AV intervals. Shortest AV delay was 6 ms in non pacemaker pts and 31 ms in PM pts. Best outcomes reported at shortest AV intervals. Increases in CO and exercise duration. 1 Nishimura et al. J Am Coll Cardiol. 1995; 25: Walker et al. Europace 2000;I(suppl D): abstract 212/5. 3 Brecker et al. Lancet. 1992;340:1308. September")
11
6MWT, 6-min walk test; CARE-HF, Cardiac Resynchronization-Heart Failure; COMPANION, Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure; HF, heart failure; LV, left ventricular; LVEDD, left ventricular end-diastolic dimension; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; MADITCRT, Multicenter Automatic Defibrillator Implantation Trial–Cardiac Resynchronization Therapy; MIRACLE, Multicenter InSync Randomized Clinical Evaluation; MIRACLE ICD, Multicenter InSync Implantable Cardioverter Defibrillator trial; MR, mitral regurgitation; MUSTIC, Multisite Simulation in Cardiomyopathies; NYHA, New York Heart Association; PATH-CHF, Pacing Therapies in Congestive Heart Failure trial; QOL, quality-of-life score; RAFT, Resynchronization-Defibrillation for Ambulatory Heart Failure; REVERSE, Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction; VO2, volume of oxygen Over the last 2 years, several landmark studies that included less symptomatic patients have been published. The first, the REVERSE trial, enrolled 610 patients in NYHA class I or II with a QRS120 ms and LVEF40%. All patients received a CRT device (with or without defibrillator) and were randomly assigned to active CRT or to control. The primary analysis was carried out after 12 months of follow-up, with the European population (n=262) remaining in the trial and further analyzed after 24 months. REVERSE used a clinical composite endpoint, scoring patients as worsened, unchanged, or improved. As it is difficult to show clinical improvements in NYHA class I patients, the criterion for success was predefined as the proportion of patient worsening only. This primary endpoint was not met at 12 months despite a significant difference in favor of CRT in the distribution of patients who worsened, remained unchanged, or improved; CRT also reduced the risk of death or HF hospitalizations at 12 and at 24 months with a 53% reduction (P=.03) at 12 months and 62% (P=.0003) at 24 months. Both LV function and remodeling improved significantly with CRT. Although there was a nonsignificant trend toward lower all-cause mortality with active treatment, the trial was not powered to show differences in all-cause death in this population where mortality rates were low. Very similar results were reported by the larger (n=1820) MADIT-CRT trial.39 Included patients had NYHA class I or II HF, LVEF30% and QRS130 ms. Patients were randomized in a 3:2 ratio to receive CRT and defibrillator or a defibrillator alone. Although physicians were not blinded to treatment assignments, the members of the assessment committee were unaware of such assignments. During an average follow-up of 2.4 years, CRT reduced the risk of the primary endpoint of all-cause death or nonfatal HF events by 34% (P=.001), although there was no reduction in all-cause death alone. As in REVERSE, CRT improved LV function significantly at 12 months. Although mortality was not significantly reduced in either study, the consistency of the other clinically relevant findings and the improvements in LV function argue for benefits of CRT in NYHA class II patients. A subanalysis of MADIT-CRT showed the benefits from CRT were driven by those patients with QRS interval>150 ms and LBBB.40 Some evidence of possible benefit on all-cause mortality or hospitalization for HF in these healthier patients (21.5% of the study population was in class I or II) was provided by a post hoc analysis of the CARE-HF study, which showed that the outcome of these patients was similar to those in the overall trial population.41 Definitive evidence was provided by the RAFT study,42 a multicenter, double-blind, randomized study that enrolled 1798 patients to either implantable cardioverter-defibrillator (ICD) or ICD with CRT. The inclusion criteria were NYHA class II (80%) or III, LVEF30% and QRS120 ms or paced QRS200 ms. The primary endpoint was death from any cause or HF leading to hospitalization. There was a reduction of the relative risk for all cause death of 25% in patients with CRT-D compared with those with ICD only. The risk of cardiovascular death and hospitalization for HF were also significantly reduced. Similar to MADIT-CRT, a greater benefit was found in patients with QRS150 ms. These findings led to the last update in 2010 of the European guidelines43 for device therapy in HF, which indicate the CRT for patients in NYHA class II, LVEF 35%, sinus rhythm, and a QRS width of150 ms (recommendation class I, level of evidence A) (Figure).
 and were randomly assigned to active CRT or to control. The primary analysis was carried out after 12 months of follow-up, with the European population (n=262) remaining in the trial and further analyzed after 24 months. REVERSE used a clinical composite endpoint, scoring patients as worsened, unchanged, or improved. As it is difficult to show clinical improvements in NYHA class I patients, the criterion for success was predefined as the proportion of patient worsening only. This primary endpoint was not met at 12 months despite a significant difference in favor of CRT in the distribution of patients who worsened, remained unchanged, or improved; CRT also reduced the risk of death or HF hospitalizations at 12 and at 24 months with a 53% reduction (P=.03) at 12 months and 62% (P=.0003) at 24 months. Both LV function and remodeling improved significantly with CRT. Although there was a nonsignificant trend toward lower all-cause mortality with active treatment, the trial was not powered to show differences in all-cause death in. this population where mortality rates were low. Very similar results were reported by the larger (n=1820) MADIT-CRT trial.39 Included patients had NYHA class I or II HF, LVEF30% and QRS130 ms. Patients were randomized in a 3:2 ratio to receive CRT and defibrillator or a defibrillator alone. Although physicians were not blinded to treatment assignments, the members of the assessment committee were unaware of such assignments. During an average follow-up of 2.4 years, CRT reduced the risk of the primary endpoint of all-cause death or nonfatal HF events by 34% (P=.001), although there was no reduction in all-cause death alone. As in REVERSE, CRT improved LV function significantly at 12 months. Although mortality was not significantly reduced in either study, the consistency of the other clinically relevant findings and the improvements in LV function argue for benefits of CRT in NYHA class II patients. A subanalysis of MADIT-CRT showed the benefits from CRT were driven by those patients with QRS interval>150 ms and LBBB.40 Some evidence of possible benefit on all-cause mortality or hospitalization for HF in these healthier patients (21.5% of the study population was in class I or II) was provided by a post hoc analysis of the CARE-HF study, which showed that the outcome of these patients was similar to those in the overall trial population.41 Definitive evidence was provided by the RAFT study,42 a multicenter, double-blind, randomized study that enrolled 1798 patients to either implantable cardioverter-defibrillator. (ICD) or ICD with CRT. The inclusion criteria were NYHA class II (80%) or III, LVEF30% and QRS120 ms or paced QRS200 ms. The primary endpoint was death from any cause or HF leading to hospitalization. There was a reduction of the relative risk for all cause death of 25% in patients with CRT-D compared with those with ICD only. The risk of cardiovascular death and hospitalization for HF were also significantly reduced. Similar to MADIT-CRT, a greater benefit was found in patients with QRS150 ms. These findings led to the last update in 2010 of the European guidelines43 for device therapy in HF, which indicate the CRT for patients in NYHA class II, LVEF 35%, sinus rhythm, and a QRS width of150 ms (recommendation class I, level of evidence A) (Figure).")
12
2013 ESCGuidelines on cardiac pacing and cardiac resynchronization therapy

13
29% 18% BACKGROUND The Multicenter Automatic Defibrillator Implantation Trial with Cardiac Resynchronization Therapy (MADIT-CRT) showed that early intervention with cardiac-resynchronization therapy with a defibrillator (CRT-D) in patients with an electrocardiographic pattern showing left bundle-branch block was associated with a significant reduction in heart-failure events over a median follow-up of 2.4 years, as compared with defibrillator therapy alone. METHODS We evaluated the effect of CRT-D on long-term survival in the MADIT-CRT population. Post-trial follow-up over a median period of 5.6 years was assessed among all 1691 surviving patients (phase 1) and subsequently among 854 patients who were enrolled in post-trial registries (phase 2). All reported analyses were performed on an intention-to-treat basis. RESULTS At 7 years of follow-up after initial enrollment, the cumulative rate of death from any cause among patients with left bundle-branch block was 18% among patients randomly assigned to CRT-D, as compared with 29% among those randomly assigned to defibrillator therapy alone (adjusted hazard ratio in the CRT-D group, 0.59; 95% confidence interval [CI], 0.43 to 0.80; P<0.001). The long-term survival benefit of CRT-D in patients with left bundle-branch block did not differ significantly according to sex, cause of cardiomyopathy, or QRS duration. In contrast, CRT-D was not associated with any clinical benefit and possibly with harm in patients without left bundlebranch block (adjusted hazard ratio for death from any cause, 1.57; 95% CI, 1.03 to 2.39; P = 0.04; P<0.001 for interaction of treatment with QRS morphologic findings). CONCLUSIONS Our findings indicate that in patients with mild heart-failure symptoms, left ventricular dysfunction, and left bundle-branch block, early intervention with CRT-D was associated with a significant long-term survival benefit. (Funded by Boston Scientific; ClinicalTrials.gov numbers, NCT , NCT , and NCT )
 showed that early intervention with cardiac-resynchronization therapy with a defibrillator (CRT-D) in patients with an electrocardiographic pattern showing left bundle-branch block was associated with a significant reduction in heart-failure events over a median follow-up of 2.4 years, as compared with defibrillator therapy alone. METHODS. We evaluated the effect of CRT-D on long-term survival in the MADIT-CRT population. Post-trial follow-up over a median period of 5.6 years was assessed among all 1691 surviving patients (phase 1) and subsequently among 854 patients who were enrolled in post-trial registries (phase 2). All reported analyses were performed on an intention-to-treat basis. RESULTS. At 7 years of follow-up after initial enrollment, the cumulative rate of death from any cause among patients with left bundle-branch block was 18% among patients randomly assigned to CRT-D, as compared with 29% among those randomly assigned to defibrillator therapy alone (adjusted hazard ratio in the CRT-D group, 0.59; 95% confidence interval [CI], 0.43 to 0.80; P<0.001). The long-term survival benefit of CRT-D in patients with left bundle-branch block did not differ significantly according to sex, cause of cardiomyopathy, or QRS duration. In contrast, CRT-D was not associated. with any clinical benefit and possibly with harm in patients without left bundlebranch block (adjusted hazard ratio for death from any cause, 1.57; 95% CI, 1.03 to 2.39; P = 0.04; P<0.001 for interaction of treatment with QRS morphologic findings). CONCLUSIONS. Our findings indicate that in patients with mild heart-failure symptoms, left ventricular dysfunction, and left bundle-branch block, early intervention with CRT-D was associated with a significant long-term survival benefit. (Funded by Boston Scientific; ClinicalTrials.gov numbers, NCT , NCT , and NCT )")
14
La Stimolazione Biventricolare (CRT)
Stimolazione biventricolare è indicata nei pazienti con disfunzione ventricolare sinistra e dissincronia ventricolare (BBSX) Posizionamento di elettrocatetere per il ventricolo sinistro attraverso una vena tributaria del seno coronarico (laterale o postero-laterale) Insuccesso dovuto a: anatomia del CS e dei suoi rami, instabilità dei cateteri, soglie elevate, stimolazione diaframmatica,etc Elevata morbidità e mortalità dell’approccio chirurgico Non responder >30% dei pazienti
 Posizionamento di elettrocatetere per il ventricolo sinistro attraverso una vena tributaria del seno coronarico (laterale o postero-laterale) Insuccesso dovuto a: anatomia del CS e dei suoi rami, instabilità dei cateteri, soglie elevate, stimolazione diaframmatica,etc. Elevata morbidità e mortalità dell’approccio chirurgico. Non responder >30% dei pazienti.")
16
Figure 1. Methods, indicating the position of pacing leads and multielectrode arrays.
Figure 1. Methods, indicating the position of pacing leads and multielectrode arrays. Each gray dot denotes an epicardial electrode, each arrow an endocardial electrode. Ant indicates anterior; Lat, lateral; and Post, posterior. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.

17
Figure 2. Three-dimensional reconstruction of electrical activation times in the RV and LV, as measured with epicardial and endocardial electrodes (see Figure 1). Figure 2. Three-dimensional reconstruction of electrical activation times in the RV and LV, as measured with epicardial and endocardial electrodes (see Figure 1). LV pacing site was the midlateral wall (center of the red area in the BiV-epi and LV-epi panels). Color bar indicates time scale in milliseconds. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.
. LV pacing site was the midlateral wall (center of the red area in the BiV-epi and LV-epi panels). Color bar indicates time scale in milliseconds. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.")
18
Figure 3. Activation time delays (ms) from the lateral to septal wall, from the base to apex and transmurally across the LV wall, as determined during pacing at the basal lateral wall with a short AV interval. Figure 3. Activation time delays (ms) from the lateral to septal wall, from the base to apex and transmurally across the LV wall, as determined during pacing at the basal lateral wall with a short AV interval. Presented are mean values and standard deviations of 8 experiments. *P<0.05 compared with baseline; †P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.
 from the lateral to septal wall, from the base to apex and transmurally across the LV wall, as determined during pacing at the basal lateral wall with a short AV interval. Presented are mean values and standard deviations of 8 experiments. *P<0.05 compared with baseline; †P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.")
19
Figure 4. Percent increase in electrical LV resynchronization (percent reduction in LV activation time) (A) and LVdP/dtmax (B) during ENDO and EPI-BiV pacing compared with baseline atrial pacing in the LBBB heart. Figure 4. Percent increase in electrical LV resynchronization (percent reduction in LV activation time) (A) and LVdP/dtmax (B) during ENDO and EPI-BiV pacing compared with baseline atrial pacing in the LBBB heart. Presented are mean values and standard deviations of 48 paired measurements in 8 experiments. *P<0.05 compared with baseline; #P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.
 (A) and LVdP/dtmax (B) during ENDO and EPI-BiV pacing compared with baseline atrial pacing in the LBBB heart. Presented are mean values and standard deviations of 48 paired measurements in 8 experiments. *P<0.05 compared with baseline; #P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.")
20
Figure 5. Left, Example from a study of pressure-volume diagrams of the LV during ENDO (black) and EPI BiV pacing (gray line) and their related baseline states (broken lines). Figure 5. Left, Example from a study of pressure-volume diagrams of the LV during ENDO (black) and EPI BiV pacing (gray line) and their related baseline states (broken lines). Right, Percent increase of stroke work compared with baseline atrial pacing for all animals and pacing sites. *P<0.05 compared with baseline; #P<0.05 ENDO compared with EPI (all paired analyses). van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.
 and EPI BiV pacing (gray line) and their related baseline states (broken lines). Right, Percent increase of stroke work compared with baseline atrial pacing for all animals and pacing sites. *P<0.05 compared with baseline; #P<0.05 ENDO compared with EPI (all paired analyses). van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.")
21
Figure 8. A, Percent decrease in Tpeak-Tend (left) and percent decrease in dispersion of repolarization during EPI and ENDO-BiV pacing. Figure 8. A, Percent decrease in Tpeak-Tend (left) and percent decrease in dispersion of repolarization during EPI and ENDO-BiV pacing. B, Time differences in repolarization between epicardium and endocardium during BiV pacing. Presented are mean values and standard deviations of 8 experiments. *P<0.05 compared with baseline atrial pacing; #P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.
 and percent decrease in dispersion of repolarization during EPI and ENDO-BiV pacing. B, Time differences in repolarization between epicardium and endocardium during BiV pacing. Presented are mean values and standard deviations of 8 experiments. *P<0.05 compared with baseline atrial pacing; #P<0.05 ENDO compared with EPI. van Deursen C et al. Circ Arrhythm Electrophysiol. 2009;2: Copyright © American Heart Association, Inc. All rights reserved.")
23
Copyright © The American College of Cardiology.
From: Optimizing Hemodynamics in Heart Failure Patients by Systematic Screening of Left Ventricular Pacing Sites: The Lateral Left Ventricular Wall and the Coronary Sinus Are Rarely the Best Sites J Am Coll Cardiol. 2010;55(6): doi: /j.jacc Figure Legend: (A) Predetermined left ventricular (LV) pacing site used during the study. The LV cavity was divided into 9 zones: 4 basal, 4 mid-cavity (inferior, lateral, anterior, and septal aspects), and 1 apex. One site was epicardial in a lateral branch of the coronary sinus (CS), and 1 site was endocardial just facing the CS pacing site. (B) Catheter position during the study. Date of download: 10/5/2014 Copyright © The American College of Cardiology. All rights reserved.
: doi: /j.jacc Figure Legend: (A) Predetermined left ventricular (LV) pacing site used during the study. The LV cavity was divided into 9 zones: 4 basal, 4 mid-cavity (inferior, lateral, anterior, and septal aspects), and 1 apex. One site was epicardial in a lateral branch of the coronary sinus (CS), and 1 site was endocardial just facing the CS pacing site. (B) Catheter position during the study. Date of download: 10/5/2014. Copyright © The American College of Cardiology. All rights reserved.")
24
Copyright © The American College of Cardiology.
From: Optimizing Hemodynamics in Heart Failure Patients by Systematic Screening of Left Ventricular Pacing Sites: The Lateral Left Ventricular Wall and the Coronary Sinus Are Rarely the Best Sites J Am Coll Cardiol. 2010;55(6): doi: /j.jacc The present study demonstrates that acutely: 1) the LV pacing site is a major determinant of the hemodynamic response; 2) major interindividual and intraindividual variations in response to LV pacing are observed; 3) an optimal LV pacing site cannot be defined a priori and is specific to each individual; 4) an individually-based approach to pacing at the best possible location is superior to the other pacing strategies: pacing from within the CS, at the lateral, or at the most delayed wall; 5) endocardial pacing may improve the diastolic function compared with epicardial pacing; and 6) in LV pacing, a long AVD is consistently superior to a short AVD. Figure Legend: Comparison of hemodynamic change when the pacing site is defined by the site associated with the greatest improvement of +dP/dTmax. AV = atrioventricular; CS = coronary sinus; ESP = end-systolic pressure; PP = pulse pressure. Date of download: 10/5/2014 Copyright © The American College of Cardiology. All rights reserved.
: doi: /j.jacc The present study demonstrates that acutely: 1) the LV pacing site is a major determinant of the hemodynamic response; 2) major interindividual and intraindividual variations in response to LV pacing are observed; 3) an optimal LV pacing site cannot be defined a priori and is specific to each individual; 4) an individually-based approach to pacing at the best possible location is superior to the other pacing strategies: pacing from within the CS, at the lateral, or at the most delayed wall; 5) endocardial pacing may improve the diastolic function compared with epicardial pacing; and 6) in LV pacing, a long AVD is consistently superior to a short AVD. Figure Legend: Comparison of hemodynamic change when the pacing site is defined by the site associated with the greatest improvement of +dP/dTmax. AV = atrioventricular; CS = coronary sinus; ESP = end-systolic pressure; PP = pulse pressure. Date of download: 10/5/2014. Copyright © The American College of Cardiology. All rights reserved.")
25
Vantaggi della LVEP Potenziale accesso a tutte le regioni del ventricolo sinistro Propagazione più rapida dell’impulso elettrico nell’endocardio con altrettanto più rapida ripolarizzazione Più fisiologica stimolazione del VS con preservazione dell’attivazione transmurale e della sequenza di ripolarizzazione Possibilità di un migliore controllo degli indici di contrattilità La CRT classica presenta più del 30% di non responder. Nelle limitate casistiche con LVEP i risultati sono migliori. Ciò permette: scelta del sito non obbligata dall’anatomia, miglioramento quindi delle soglie di stimolazione, minore incidenza di stimolazione diaframmatica, minore possibilità di dislocazione dei cateteri grazie al fissaggio attivo (come lo è stato per i cateteri a vite nel ventricolo destro), possibilità di monitorare la funzione cardiaca con sensori applicati ai cateteri. e 3) La stimolazione endocardica appare più fisiologica e sembra essere meno aritmogena di quella epicardica, lo shift della stimolazione da endocardica ad epicardica, nella CRT convenzionale, aumenta la dispersione transmurale e la ripolarizzazione e la durata del QT, aumentando il rischio di torsione di punta,
, possibilità di monitorare la funzione cardiaca con sensori applicati ai cateteri. e 3) La stimolazione endocardica appare più fisiologica e sembra essere meno aritmogena di quella epicardica, lo shift della stimolazione da endocardica ad epicardica, nella CRT convenzionale, aumenta la dispersione transmurale e la ripolarizzazione e la durata del QT, aumentando il rischio di torsione di punta,")
29
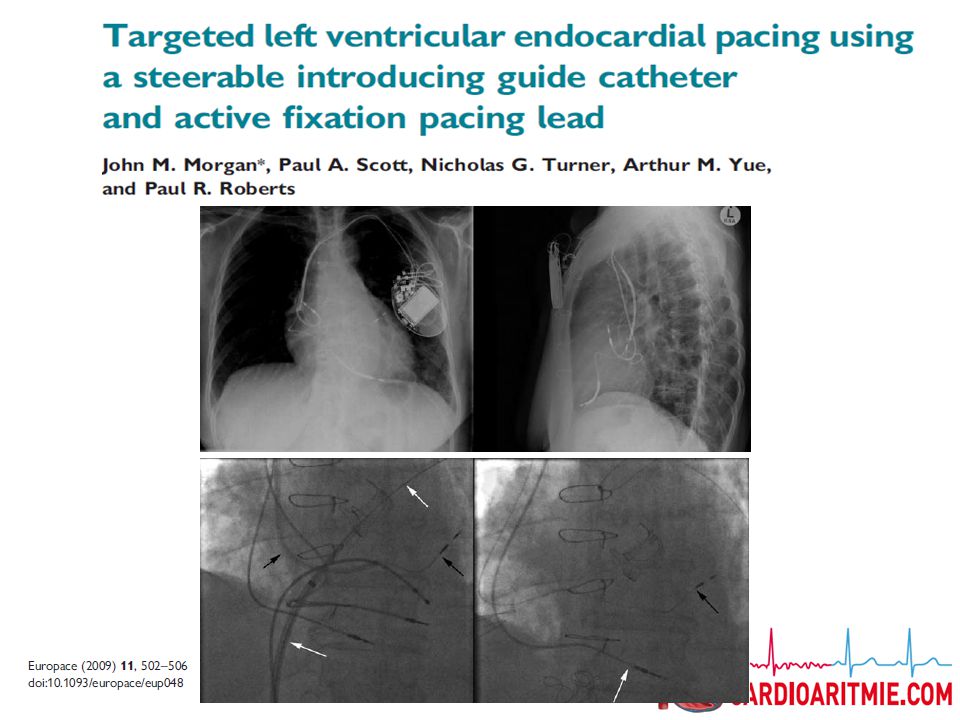
From: Left Ventricular Endocardial Stimulation for Severe Heart Failure
J Am Coll Cardiol. 2010;56(10): doi: /j.jacc Fluoroscopic views from a recipient of an atriobiventricular cardiac resynchronization therapy system, with the left ventricular endocardial lead implanted transseptally. (A) The septum was punctured with a needle preformed to reach the fossa ovalis. The proximal segment of a guidewire was then placed in the left atrium. (B) A sheath was introduced into the left atrium along the guidewire, and the stimulation lead was advanced through the sheath.
: doi: /j.jacc Fluoroscopic views from a recipient of an atriobiventricular cardiac resynchronization therapy system, with the left ventricular endocardial lead implanted transseptally. (A) The septum was punctured with a needle preformed to reach the fossa ovalis. The proximal segment of a guidewire was then placed in the left atrium. (B) A sheath was introduced into the left atrium along the guidewire, and the stimulation lead was advanced through the sheath.")
30
Svantaggi della LVEP Complicanze tromboemboliche
Complicanze legate all’eparina durante la procedura Interazione con la valvola mitrale Rischi di eventuale estrazione

31
From: Left Ventricular Endocardial Stimulation for Severe Heart Failure
J Am Coll Cardiol. 2010;56(10): doi: /j.jacc Transseptal passage of a left ventricular endocardial lead (arrow) and absence of adhesion at the level of the mitral valve (green star), in a cardiac resynchronization therapy recipient who died suddenly from a ventricular tachyarrhythmia.
: doi: /j.jacc Transseptal passage of a left ventricular endocardial lead (arrow) and absence of adhesion at the level of the mitral valve (green star), in a cardiac resynchronization therapy recipient who died suddenly from a ventricular tachyarrhythmia.")
32
Tecniche di Impianto Approccio Transettale Ventricolare
Approccio Transaortico

35
ALSYNC: LV Endocardial Pacing Could Help in CRT Nonresponse
In a 138-patients not suitable for or not responder to traditional CRT Safety and efficacy study of LV endocardial-lead CRT 16 centers in Europe and two in Canada About two-thirds of the group showed some kind of functional or reverse-remodeling response characteristic of standard CRT over at least six months of follow-up. The system evaluated in the ALSYNC study is not available for investigational or commercial use in the United States. Some heart failure patients are not suitable for, or do not respond to, traditional CRT because of limitations associated with implanting a lead, or thin wire, in veins on the outside of the left ventricle; these limitations may include unique patient anatomy orsuboptimal lead placement. As a potential alternative for these patients, the system evaluated in the study implants a lead placed inside the left ventricle by crossing the atrial septum, the wall that divides the two top chambers of the heart. "There is a significant need for a new way to pace the left ventricle in patients unable to receive the clinical benefits of standard CRT therapy, and this study suggests left ventricular endocardial pacing is a feasible option," said Prof. Morgan, lead investigator of the ALSYNC study. "These findings will elevate this new approach from something that is investigational to one that is closer to the mainstream." The ALSYNC study, the first of its kind to evaluate the safety and performance of a new delivery system and left ventricular endocardial (LVE) pacing lead for CRT implantation, included 138 patients at 18 centers in Europe and Canada, all of whom were indicated for CRT but were unable to receive a conventional system or did not respond to the therapy at least six months post-implant. LVE pacing was successful in 118 out of 133 (89 percent) implant attempts. The ALSYNC study assessed the safety and performance of the system and implant procedure. The primary objective was to demonstrate that the complication rates were less than 30 percent at six months in patients with an implant attempt. The objective was met with an observed rate of 17.7 percent (upper confidence bound 24.2 percent), which is comparable to the complication rates of conventional CRT implants. "As the leader in CRT, we are committed to continued innovations in heart failure treatment and bringing renewed hope to the many patients who have previously had limited options," said David Steinhaus, M.D., vice president and general manager, heart failure, and medical director for the Cardiac Rhythm Disease Management business at Medtronic. In collaboration with leading clinicians, researchers and scientists worldwide, Medtronic offers the broadest range of innovative medical technology for the interventional and surgical treatment of cardiovascular disease and cardiac arrhythmias. The company strives to offer products and services that deliver clinical and economic value to healthcare consumers and providers around the world. Prof John Morgan (Southampton University Hospitals Trust, UK) Heart Rhythm Society 2014 Scientific Sessions
 pacing lead for CRT implantation, included 138 patients at 18 centers in Europe and Canada, all of whom were indicated for CRT but were unable to receive a conventional system or did not respond to the therapy at least six months post-implant. LVE pacing was successful in 118 out of 133 (89 percent) implant attempts. The ALSYNC study assessed the safety and performance of the system and implant procedure. The primary objective was to demonstrate that the complication rates were less than 30 percent at six months in patients with an implant attempt. The objective was met with an observed rate of 17.7 percent (upper confidence bound 24.2 percent), which is comparable to the complication rates of conventional CRT implants. As the leader in CRT, we are committed to continued innovations in heart failure treatment and bringing renewed hope to the many patients who have previously had limited options, said David Steinhaus, M.D., vice president and general manager, heart failure, and medical director for the Cardiac Rhythm Disease Management business at Medtronic. In collaboration with leading clinicians, researchers and scientists worldwide, Medtronic offers the broadest range of innovative medical technology for the interventional and surgical treatment of cardiovascular disease and cardiac arrhythmias. The company strives to offer products and services that deliver clinical and economic value to healthcare consumers and providers around the world. Prof John Morgan (Southampton University Hospitals Trust, UK) Heart Rhythm Society 2014 Scientific Sessions.")
36
Rates of Achieving Functional, Reverse-Remodeling Improvements in ALSYNC
End Points All Patients (%) Patients With Prior Failed CRT Implant (%) Patients With Prior CRT Nonresponse (%) LVESV >15% improvement 55 57 47 LVEF >5-point improvement 64 65 61 NYHA class >1 class improvement 60 63 52 Mitral regurgitation >1 class improvement 33 29 43 The study enrolled 138 patients with indications for CRT and included 40% with ischemic cardiomyopathy, 50% with atrial fibrillation, 78% with a failed prior attempt to engage a CRT system, and 22% with prior successful CRT-device implantation but no response within six months. About 75% were initially in NYHA functional class 3 or 4. Successful CRT pacing with the LV endocardial lead system was achieved in 89% of attempted cases, Morgan reported. By the six-month follow-up, 60% of patients showed improved in NYHA class and 55% showed an improvement in LV end-systolic volume of at least 15%. Complications in the first six months included some related to anticoagulation, such as implantation-site hematoma, but also some infections, one aortic puncture at transfemoral implantation, one case of intraventricular thrombosis, two strokes, four cases of transient ischemic attack (TIA), and 10 deaths—only one, from a pneumothorax, that was related to the device implantation. Morgan said "this is a safe procedure in the right hands." ALSYNC suggests that "we are not exposing these patients to any significantly greater risk with the actual implant procedure itself," and there is "no unexpected adverse complication rate that bothers us about this procedure in clinical terms." He emphasized that the procedure's safety depended on using the right tools, which included conventional equipment except for an investigational transseptal lead delivery system (Medtronic) designed specifically for the procedure. It could be an option, he said, for about 30% of patients with CRT indications, those with obstacles to the standard technique. "It may be that, even in those patients who respond to conventional CRT, there are subgroups in whom the response may be even greater if they had this type of pacing approach." LVESV=left ventricular end-systolic volume LVEF=left ventricular ejection fraction
 Patients With Prior Failed CRT Implant (%) Patients With Prior CRT Nonresponse (%) LVESV >15% improvement LVEF >5-point improvement NYHA class >1 class improvement Mitral regurgitation >1 class improvement The study enrolled 138 patients with indications for CRT and included 40% with ischemic cardiomyopathy, 50% with atrial fibrillation, 78% with a failed prior attempt to engage a CRT system, and 22% with prior successful CRT-device implantation but no response within six months. About 75% were initially in NYHA functional class 3 or 4. Successful CRT pacing with the LV endocardial lead system was achieved in 89% of attempted cases, Morgan reported. By the six-month follow-up, 60% of patients showed improved in NYHA class and 55% showed an improvement in LV end-systolic volume of at least 15%. Complications in the first six months included some related to anticoagulation, such as implantation-site hematoma, but also some infections, one aortic puncture at transfemoral implantation, one case of intraventricular thrombosis, two strokes, four cases of transient ischemic attack (TIA), and 10 deaths—only one, from a pneumothorax, that was related to the device implantation. Morgan said this is a safe procedure in the right hands. ALSYNC suggests that we are not exposing these patients to any significantly greater risk with the actual implant procedure itself, and there is no unexpected adverse complication rate that bothers us about this procedure in clinical terms. He emphasized that the procedure s safety depended on using the right tools, which included conventional equipment except for an investigational transseptal lead delivery system (Medtronic) designed specifically for the procedure. It could be an option, he said, for about 30% of patients with CRT indications, those with obstacles to the standard technique. It may be that, even in those patients who respond to conventional CRT, there are subgroups in whom the response may be even greater if they had this type of pacing approach. LVESV=left ventricular end-systolic volume. LVEF=left ventricular ejection fraction.")
40
CONCLUSIONI Studi sperimentali su modelli animali ed umani hanno dimostrato il beneficio emodinamico della stimolazione endocardica LV rispetto a quella epicardica nei pazienti candidati alla CRT I pazienti candidati alla stimolazione LV endo sono i non responders o coloro nei quali è fallito il tentativo di impianto di un catetere epicardico in maniera convenzionale. Esistono diversi modi per ottenere una stimolazione endocardica del ventricolo sinistro, specialmente se la tecnologia leadless diventasse disponibile

Presentazioni simili








>")




>")








