Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Indicazioni al Trattamento Locale delle Metastasi
HOT TOPICS Controversie Oncologiche Indicazioni al Trattamento Locale delle Metastasi Roberto Sabbatini Azienda Ospedaliero Universitaria di Modena Policlicnico di Modena Scuola di UrOncologia Tumore del rene Roma maggio 2014

2
Non raccomandata al di fuori di studi clinici
ESMO (Giugno 2012) NCCN (Gennaio 2013) EAU (Marzo 2013) AIOM (Luglio 2013) Terapia Adiuvante Non raccomandata al di fuori di studi clinici Nefrectomia in presenza di metastasi Solo se buon PS e grosso T. Oppure nei pazienti sintomatici Solo se anche le metastasi sono resecabili, buon PS (limitata ai casi a basso rischio) Sempre dove è possibile, prima del trattamento medico (Grado B) Resezione delle Metastasi Solo se: metastasi solitarie o multiple polmonari, lungo IL, buon PS, in risposta dopo terapia. Sempre se metastasi resecabili e buon PS Sempre se metastasi resecabili Courtesy of R. Passalacqua
 NCCN. (Gennaio 2013) EAU. (Marzo 2013) AIOM. (Luglio 2013) Terapia Adiuvante. Non raccomandata al di fuori di studi clinici. Nefrectomia. in presenza. di metastasi. Solo se buon PS e grosso T. Oppure nei pazienti sintomatici. Solo se anche le metastasi sono resecabili, buon PS (limitata ai casi a basso rischio) Sempre dove è possibile, prima del trattamento medico (Grado B) Resezione. delle. Metastasi. Solo se: metastasi solitarie o multiple polmonari, lungo IL, buon PS, in risposta dopo terapia. Sempre se metastasi resecabili e buon PS. Sempre se metastasi resecabili. Courtesy of R. Passalacqua.")
3
RCC: metastasectomy as independent prognostic variable
Median OS: 78 m. Median OS: 5 m. Eggener, J Urol 2008 Thomas, Curr Urol Rep 2009 Breau, Curr Opin Urol 2010

4
3711 pts Median OS overall: 17-41 m. Resected median OS: 44-55 m.
Breau, Curr Opin Urol 2010

5
Prognostic Factors of Patients With Metastatic Renal Cell Carcinoma With Removed Metastases: A Multicenter Study of 556 Patients Median OS 80 m. Patients with 3 or 4 of these adverse prognostic factors had a worse prognosis. Naito, Urology 2013

6
Patients with only resected lung metastases have a longer survival
Lung only mets 887 pts nephrectomy 1976 – 2006 R0 predictive for CSS also for >3 mets and synchronous or asynchronous mets Non Lung mets Alt, Cancer 2011

7
417 pts (1986 – 2001) M1 lung (92 metastasectomy)
50% 1 or 2 mets; 37% > 5 mets. 63 pts (68%) R0 Incomplete resection strongest risk factor for OS (5 yrs OS : 8% vs 45%) RISK FACTORS Larger nodule size Increasing n° of N+ Preoperative 1-second forced expiratory volume (FEV1) Shorter DFI (resected pts) If FEV1 is 60% to 70% of predicted normal, long-term survival decreases by about 33%. Conclusions Because pulmonary metastasectomy for renal cell carcinoma is safe, survival depends on complete resection of pulmonary disease and adequate pulmonary reserve. Linfonodi regionali inclusi in “en block resection” .A novel finding was that lower preoperative FEV1 is an important risk factor for mortality. This might be the first time this variable has been examined. Because a quarter of our patients had an anatomic pulmonary resection as part of their therapy, spirometry was a standard component of preoperative evaluation. Although the relation is continuous, if a patient has three or fewer nodules identified on preoperative CT, chance of complete resection exceeds 80%; conversely, if more than six nodules are seen on CT, chance of incomplete resection is 80% or higher. However, if FEV1 is 60% to 70% of predicted normal, long-term survival was decreased by about 33%. Murty, Ann Thorac Surg 2005
 R0. Incomplete resection strongest risk factor for OS (5 yrs OS : 8% vs 45%) RISK FACTORS. Larger nodule size. Increasing n° of N+ Preoperative 1-second forced expiratory volume (FEV1) Shorter DFI (resected pts) If FEV1 is 60% to 70% of predicted normal, long-term survival decreases by about 33%. Conclusions. Because pulmonary metastasectomy for. renal cell carcinoma is safe, survival depends on complete resection of pulmonary disease and adequate pulmonary reserve. Linfonodi regionali inclusi in en block resection .A novel finding was that lower preoperative FEV1 is an important risk factor for mortality. This might be the first time this variable has been examined. Because a quarter of our patients had an anatomic pulmonary resection as part. of their therapy, spirometry was a standard component of preoperative evaluation. Although the relation is continuous, if a patient has three. or fewer nodules identified on preoperative CT, chance of complete resection exceeds 80%; conversely, if more than six nodules are seen on CT, chance of incomplete resection is 80% or higher. However, if FEV1 is 60% to 70% of predicted normal, long-term survival was decreased by about 33%. Murty, Ann Thorac Surg")
8
Lung metastasis conclusions
good long-term results after metastasectomy low morbidity and long-term efficacy pulmonary surgery with systematic lymph node dissection is indicated

9
The presence of bone metastases has been associated with poor outcome
pts treated with SU N: N: 1059 (30% bone mets) Median OS 23.4 months Multivariate analysis of PFS and OS identified independent predictors: Ethnic origin, ECOG PS, including ethnic origin, time from diagnosis to treatment, prior cytokine use, HB. LDH, corrected Ca, neutrophils, PLTS and bone metastases (OS only). OS: 19.5 vs 38.5 months Predictive Factors: bone mets + PS Hoffman, J Urol 2008 Woodward, Bone 2011 Beuselinck, Ann Oncol 2011 Motzer, BJC 2013
 Median OS 23.4 months Multivariate analysis of PFS and OS identified independent predictors: Ethnic origin, ECOG PS, including ethnic origin, time from diagnosis to treatment, prior cytokine use, HB. LDH, corrected Ca, neutrophils, PLTS and bone metastases (OS only). OS: 19.5 vs 38.5 months. Predictive Factors: bone mets + PS. Hoffman, J Urol Woodward, Bone Beuselinck, Ann Oncol Motzer, BJC")
10
Radical Surgery Can Lead to Durable Long Term Responses
Retrospective analysis n=101 pts operatively treated for skeletal mets ( ) Predictors of longer survival •Age younger than 65 •No fractures •Negative margins Fottner A et al., BMC musculoskeletal Dis 2010
 Predictors of longer survival. •Age younger than 65. •No fractures. •Negative margins. Fottner A et al., BMC musculoskeletal Dis")
11
Development of anti-resorptive agents have revolutionized the management of bone disease
RCC-subgroup analysis of a large randomized, placebo-controlled trial demonstrated significant benefits for ZA when compared to placebo 2,3 773 pts (46 RCC) 1 bone mets ECOG 2 352 days 1.Lipton , Clin Cancer Res 2004; 2.Lipton , Cancer 2003 3.Rosen , JCO 2003; 4. Saad, BJU Int 2005
 1 bone mets. ECOG days. 1.Lipton , Clin Cancer Res 2004; 2.Lipton , Cancer Rosen , JCO 2003; 4. Saad, BJU Int")
12
Denosumab: Efficacy Overview
Dmab 120 mg SC* + placebo IV infusion q 4 wk Denosumab: Efficacy Overview ZOL 4 mg IV + placebo SC injection q 4 wk 155 RCC pts Breast cancer1,2 OST and MM2,3 Prostate cancer2,4 Dmab ZOL N 1,026 1,020 886 890 950 951 Pts with on-study SRE, % 30.7 36.5 31.4 36.3 35.9 40.6 SRE breakdown, % RT Path Fx Surgery SCC 2.7 Median time to SRE, mo NR 26.4 20.5 16.3 20.7 17.1 HR P (non-inf.) P (superior.) 0.82 < 0.84 < 0.82 < .001 (0.0002) .008 Abbreviations: Dmab, denosumab; HR, hazard ratio; Path Fx, pathologic fracture; RT, radiotherapy; SCC, spinal cord compression; SRE, skeletal-related event; ZOL, zoledronic acid. 1. Stopeck AT, et al. JCO. 2010;28(35): ; 2. Xgeva™ (denosumab) injection, for subcutaneous use [package insert]. Thousand Oaks, CA. Amgen Inc. 2010; 3. Henry D, et al. ECCO-ESMO 2009, abstract 20LBA; 4. Fizazi K, et al ASCO 2010, abstract LBA4507.
 P (superior.) 0.82 < < < .001 (0.0002) Abbreviations: Dmab, denosumab; HR, hazard ratio; Path Fx, pathologic fracture; RT, radiotherapy; SCC, spinal cord compression; SRE, skeletal-related event; ZOL, zoledronic acid. 1. Stopeck AT, et al. JCO. 2010;28(35): ; 2. Xgeva™ (denosumab) injection, for subcutaneous use [package insert]. Thousand Oaks, CA. Amgen Inc. 2010; 3. Henry D, et al. ECCO-ESMO 2009, abstract 20LBA; 4. Fizazi K, et al. ASCO 2010, abstract LBA4507.")
13
76 pts with bone mets treated with SU or SO (49 BF + TKI - 27 TKI)
Concomitant use of BF and TKI in RCC pts with bone involvement probably improves treatment efficacy Retrospective 76 pts with bone mets treated with SU or SO (49 BF + TKI TKI) CAVEAT!!!!! ONJ 10% Beuselinck BJC 2012
 CAVEAT!!!!! ONJ 10% Beuselinck BJC")
14
Concomitant use of ZA and EVE in RCC: RAZOR study (randomized phase II): PFS
1st line setting – 30 pts randomized 1:1 EVE vs EVE +ZOL EVE + ZOL significantly prolonged PFS and the time to 1st SRE compared with EVE alone (P=0.03 for each) 1.0 0.8 0.6 0.4 0.2 0.0 Survival Probability 1 2 16 6 15 8 20 5 10 Time since randomisation (months) EVE EVE + ZOL + Censored Logrank P=0.0296 PFS mPFS (95% CI) EVE + ZOL: 7.5 mo ( mo) EVE alone: 4.6 mo ( mo) Time to 1st SRE Median time to 1st SRE (95% CI) EVE + ZOL: 9.6 mo ( mo) EVE alone: 5.2 mo ( mo) Broom RJ et al. ASCO-GU Poster #402
 Survival Probability Time since randomisation (months) EVE. EVE + ZOL. + Censored. Logrank P= PFS. mPFS (95% CI) EVE + ZOL: 7.5 mo ( mo) EVE alone: 4.6 mo ( mo) Time to 1st SRE. Median time to 1st SRE (95% CI) EVE + ZOL: 9.6 mo ( mo) EVE alone: 5.2 mo ( mo) Broom RJ et al. ASCO-GU Poster #402.")
15
Caso clinico EM, ♂, 73 anni Ipertensione arteriosa in trattamento farmacologico (Ramipril 5 mg/die) Non altre comorbidità PS 0 Luglio 2005 Dolore lombare non responsivo alla terapia con FANS

16
Luglio 2005 Rx rachide: ampia osteolisi del soma di L1, crollo di L2.
TC rachide DL: osteolisi del soma di L1 e L2. Cuneizzazione di L2. Tessuto neoformato che impronta il sacco durale. RM rachide DL: bombatura del muro posteriore di L1 e L2 con tessuto neoformato che impronta il sacco durale.

17
Luglio 2005 Laminectomia decompressiva e stabilizzazione D11-L4 previa embolizzazione Istologia compatibile con metastasi di carcinoma renale a cellule chiare Radioterapia sul rachide D11-L4 30 Gy totali (3 Gy per frazione)
")
18
Radiotherapy for bone mets
Re-treatment rates to same painful site 8% following 30 Gy in 10 fractions 20% following a single 8 Gy fractio Convenience of single fraction treatment Patient Caregiver There is no evidence to suggest that a single 8 Gy fraction provides inferior pain relief to a more prolonged course of treatment in painful spine

19
2003 Meta-analysis of reported randomized trials shows no significant difference in complete and overall pain relief between single and multifraction palliative RT for bone metastases. 16 studies: 5455 pts

20
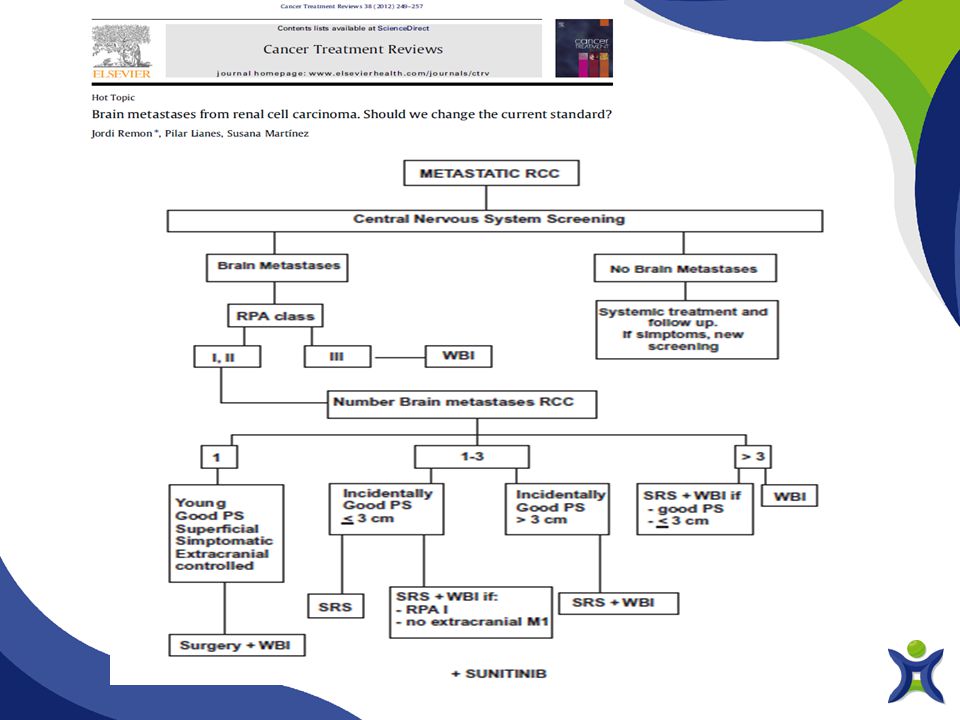
Brain metastases The presence of brain metastases is a particularly important consideration when selecting treatment Patients with brain metastases are often excluded from clinical trials due to their poor prognoses2-4 Brain metastases occur in 4-17% of patients with RCC5 RCC with brain metastases has been associated with a median survival of 7 months3,4 Untreated brain metastases have a survival of around 3.2 months Risk of developing spontaneous intracranial bleeding 1. Flanigan RC, et al. Curr Treat Options Oncol 2. Gay PC, et al. J Neurooncol 3. Decker DA, et al. J Clin Oncol 4. Culine S, et al. Cancer 5.Doh LS, et al. Oncology 20

21
EU Sorafenib: 3/1155 pts (28 brain mets) 0.3%
16.7% EAP EU Sorafenib: 3/1155 pts (28 brain mets) 0.3% US Sorafenib: pts (50 brain mets) 0% Global compassionate use Sunitinib: 2341 (182 brain mets) <1% Uncontrolled hypertension could probably justify the particularly high rate of intracerebral hemorrhage Shutz, Lancet 2009 Porta, Eur Urol 2008
 0.3% US Sorafenib: 2502 pts (50 brain mets) 0% Global compassionate use. Sunitinib: 2341 (182 brain mets) <1% Uncontrolled hypertension could probably justify the particularly high rate of intracerebral hemorrhage. Shutz, Lancet Porta, Eur Urol")
22
A multi-institutional retrospective database of 3.940 pts
Months 14.8 11.3 7.3 3.3

23
Results: local control: 90%
166 RCC patients with brain metastases treated with SRS at the Cleveland Clinic between 1996 and 2010. Results: local control: 90% In 38% of patients there were additional distant CNS metastases at a median of 12.8 months . The median TTP (either local or distant) 9.9 m. Seastone, Clinical Genitourinary Cancer 2013
 9.9 m. Seastone, Clinical Genitourinary Cancer")
24
Targeted agents appear to improve overall survival and local control in patients with brain metastases from RCC treated with GKS. Median OS for pts treated with targeted agents (n = 24 vs 37) was 16.6 vs 7.2 mos Freedom from local failure at 1 year: 93% vs 60% Multivariate analysis the use of targeted agents was the only factor that predicted for improved survival. 61 pts 20 Gy Cochran, J Neurosurg 2012
 was 16.6 vs 7.2 mos. Freedom from local failure at 1 year: 93% vs 60% Multivariate analysis the use of targeted agents was the only factor that predicted for improved survival. 61 pts. 20 Gy. Cochran, J Neurosurg")
25
Treatment with TKI agents reduces the incidence of brain metastasis in mRCC
OS 338 pts: 154 TKI, 184 no : 25 vs 12.1 mos Brain mets incidence 5-year actuarial rate of brain mets: 40% vs 17%, (P < .001). TKI treatment lower incidence of brain mets in Cox multivariate analysis Lung mets increased the risk of brain mets Verma, Cancer 2011
. TKI treatment lower incidence of brain mets in Cox multivariate analysis. Lung mets increased the risk of brain mets. Verma, Cancer")
27
Conclusions Patients with metastatic renal cell carcinoma should be considered for multimodal therapy A proportion of patients will achieve long-term survival with aggressive surgical resection In the treatment of lung metastases, metastasectomy has a low morbidity and long-term efficacy Sunitinib appeared more effective than sorafenib in delaying mean time to progression or onset of bone lesions Concomitant use of antiresorptive agents and TKI or mTOR inhibitors probably improves efficacy of bone targeted therapy Local treatments are in use to control symptoms in brain mets despite the low radiosensity TKIs seems to be effective in the control of brain mets without high risk of bleeding

Presentazioni simili













>")





