Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
AGGIORNAMENTI IN TEMA DI TERAPIE DI DISLIPIDEMIE
Mauro Vannucci V° CONGRESSO NAZIONALE, Riccione Maggio 2015

2
Studi con statine in prevenzione primaria: riduzione eventi ed LDL-col “on trial”
10 y = x – R2 = p = 9 WOSCOPS-P 8 7 WOSCOPS-S 6 5 AFCAPS-P Eventi coronarici (%) AFCAPS-S 4 3 Gli eventi sembrano azzerarsi per un C-LDL di 55 mg/dL ASCOT-P 2 ASCOT-S 1 -1 55 75 95 115 135 155 175 195 C-LDL (mg/dL) O’Keefe et al. JACC, 2004
 AFCAPS-S Gli eventi sembrano. azzerarsi per un. C-LDL di 55 mg/dL. ASCOT-P. 2. ASCOT-S C-LDL (mg/dL) O’Keefe et al. JACC,")
3
Studi con statine in prevenzione secondaria: riduzione eventi ed LDL-col “on trial”
30 y = x – R2 = p = 4S-P 25 20 HPS-P LIPID-P 4S-S Eventi coronarici (%) 15 HPS-S CARE-P LIPID-S Gli eventi sembrano azzerarsi per un C-LDL di 30 mg/dL 10 CARE-S PROVET-IT-AT PROVET-IT-PR 5 30 50 70 90 110 130 150 170 190 210 C-LDL (mg/dL) O’Keefe et al. JACC, 2004
 15. HPS-S. CARE-P. LIPID-S. Gli eventi sembrano. azzerarsi per un. C-LDL di 30 mg/dL. 10. CARE-S. PROVET-IT-AT. PROVET-IT-PR C-LDL (mg/dL) O’Keefe et al. JACC,")
4
Secondary Prevention Primary Prevention THE LOWER THE BETTER
LDL-C achieved mg/dL (mmol/L) WOSCOPS – Placebo AFCAPS - Placebo ASCOT - Placebo AFCAPS - Rx WOSCOPS - Rx ASCOT - Rx 4S - Rx HPS - Placebo LIPID - Rx 4S - Placebo CARE - Rx LIPID - Placebo CARE - Placebo HPS - Rx 5 10 15 20 25 30 40 (1.0) 60 (1.6) 80 (2.1) 100 (2.6) 120 (3.1) 140 (3.6) 160 (4.1) 180 (4.7) Event rate (%) 6 Secondary Prevention Primary Prevention Rx - Statin therapy PRA – pravastatin ATV - atorvastatin 200 (5.2) PROVE-IT - PRA PROVE-IT – ATV TNT – ATV10 TNT – ATV80 THE LOWER THE BETTER Jupiter Ros La riduzione deelle LDL è efficace sia in prevenzione primaria che in prevenzione primaria, ma , ovviamente, nei pazienti in prevenzione secondaria che sono a rischio più elevato il beneficio è maggiore, come ben evidenziato dalla diversa pendanza della retta che esprime la relazione lineare tra livelli di LDL e rischio di eventi. Adattata e modificata da : LaRosa JC et al. N Engl J Med 2005;352:e-version 4
 WOSCOPS – Placebo. AFCAPS - Placebo. ASCOT - Placebo. AFCAPS - Rx. WOSCOPS - Rx. ASCOT - Rx. 4S - Rx. HPS - Placebo. LIPID - Rx. 4S - Placebo. CARE - Rx. LIPID - Placebo. CARE - Placebo. HPS - Rx (1.0) 60. (1.6) 80. (2.1) 100. (2.6) 120. (3.1) 140. (3.6) 160. (4.1) 180. (4.7) Event rate (%) 6. Secondary Prevention. Primary Prevention. Rx - Statin therapy. PRA – pravastatin. ATV - atorvastatin (5.2) PROVE-IT - PRA. PROVE-IT – ATV. TNT – ATV10. TNT – ATV80. THE LOWER. THE BETTER. Jupiter Ros. La riduzione deelle LDL è efficace sia in prevenzione primaria che in prevenzione primaria, ma , ovviamente, nei pazienti in prevenzione secondaria che sono a rischio più elevato il beneficio è maggiore, come ben evidenziato dalla diversa pendanza della retta che esprime la relazione lineare tra livelli di LDL e rischio di eventi. Adattata e modificata da : LaRosa JC et al. N Engl J Med 2005;352:e-version. 4.")
5
Aderenza terapeutica: il fattore di rischio occulto
Furio Colivicchi, Maurizio G. Abrignani, Massimo Santini In uno studio condotto nell’ASL di Treviso dal 1994 al 2003 su oltre soggetti che avevano ricevuto una prescrizione di statina, il tasso di interruzione è stato del 50% nel primo anno. Nel Lazio abbiamo osservato un elevato tasso di interruzione del trattamento con statine che va dal 25% nei primi 3 mesi dalla dimissione dopo una sindrome coronarica acuta, al 40% dopo 1 anno da un ictus27, al 50% entro 1 anno dalla prima prescrizione in una popolazione di diabetici afferenti a strutture ambulatoriali. G Ital Cardiol 2010

6
Dati del registro SIMG - Health Search – J Cardiovasc Med 2009
Riduzione progressiva della persistenza dei trattamenti farmacologici raccomandati dalle linee guida durante il follow-up in pazienti con pregresso IMA Dati del registro SIMG - Health Search – J Cardiovasc Med 2009

7
Cause di interruzione della terapia con statine riferite dai pazienti
Effetti collaterali riferiti Dispepsia (52%) Astenia (18%) Cefalea (17%) Mialgie (11%) Incremento asintomatico delle transaminasi (1%) Incremento asintomatico del CK totale (1%) Assenza di reazioni avverse maggiori “Troppe pastiglie” Colivicchi F, et al. Stroke 2007; 38:
 Astenia (18%) Cefalea (17%) Mialgie (11%) Incremento asintomatico delle transaminasi (1%) Incremento asintomatico del CK totale (1%) Assenza di reazioni avverse maggiori. Troppe pastiglie Colivicchi F, et al. Stroke 2007; 38:")
8
L’aderenza alla terapia con statine tende a ridursi nel tempo: dati della ASL di Ravenna
Poluzzi E et al. Br J Clin Pharm 2007; 63:

9
Association between switching and MACEs
Colivicchi F, et al. Int J Cardiology 2011; 152:56-60

10
Recent Coronary IVUS Progression Trials
-1.2 -0.6 0.6 1.2 1.8 50 60 70 80 90 100 110 120 Median Change In Percent Atheroma Volume (%) Mean Low-Density Lipoprotein Cholesterol (mg/dL) REVERSAL pravastatin atorvastatin CAMELOT placebo A-Plus ACTIVATE ASTEROID rosuvastatin r2= 0.95 p<0.001 Nissen S. JAMA 2006
 Mean Low-Density Lipoprotein Cholesterol (mg/dL) REVERSAL. pravastatin. atorvastatin. CAMELOT. placebo. A-Plus. ACTIVATE. ASTEROID. rosuvastatin. r2= p< Nissen S. JAMA")
11
Efficacy and safety of statin treatment for cardiovascular disease:
a network meta-analysis of patients from 76 randomized trials Statin therapy reduced: All-cause mortality (RR 0.90) Cardiovascular disease mortality (RR 0.80) Fatal myocardial infarction (RR 0.82) Non-fatal MI (RR 0.74) Revascularization (RR 0.76) Fatal and non-fatal strokes (RR 0.86) E.J. MILLS et al, Q J Med 2011
 Cardiovascular disease mortality (RR 0.80) Fatal myocardial infarction (RR 0.82) Non-fatal MI (RR 0.74) Revascularization (RR 0.76) Fatal and non-fatal strokes (RR 0.86) E.J. MILLS et al, Q J Med")
12
Efficacy and safety of statin treatment for cardiovascular disease:
a network meta-analysis of patients from 76 randomized trials E.J. MILLS et al, Q J Med 2011

14
Target della terapia con statine
Linee Guida ESC 2012 Target della terapia con statine Target LDL-C Rischio molto alto < 70 mg/dL(1.8 mmol/L) oppure, se il target non si riesce a raggiungere, riduzione ≥ 50% del LDL-C rispetto al basale Rischio alto < 100 mg/dL (2.5 mmol/L) Rischio moderato < 115 mg/dL (3.0 mmol/L) Presenza di almeno un fattore di rischio rilevante (per esempio dislipidemie familiari severe) Diabete mellito (tipo 1 o tipo 2) ma senza fattori di rischio CV concomitante o danno d’organo IRC moderata (GFRe 30–59 mL/min/1.73 m2) Calcolo del rischio a 10-anni SCORE ≥ 5% e < 10% per patologia cardiaca fatale ACS - CAD documentata – MCV documentata SCORE > 10% La strategia del trattamento con statine con obiettivi di LDL diversi secondo i livelli di rischio CV è “figlia culturale” di queste considerazioni , ed è la syrategia adottata nelle LLGG europee e nella stessa nota 13 italiana. 14
 oppure, se il target non si riesce a raggiungere, riduzione ≥ 50% del LDL-C rispetto al basale. Rischio alto. < 100 mg/dL (2.5 mmol/L) Rischio moderato. < 115 mg/dL (3.0 mmol/L) Presenza di almeno un fattore di rischio rilevante (per esempio dislipidemie familiari severe) Diabete mellito (tipo 1 o tipo 2) ma senza fattori di rischio CV concomitante o danno d’organo. IRC moderata (GFRe 30–59 mL/min/1.73 m2) Calcolo del rischio a 10-anni SCORE ≥ 5% e < 10% per patologia cardiaca fatale. ACS - CAD documentata – MCV documentata. SCORE > 10% La strategia del trattamento con statine con obiettivi di LDL diversi secondo i livelli di rischio CV è figlia culturale di queste considerazioni , ed è la syrategia adottata nelle LLGG europee e nella stessa nota 13 italiana. 14.")
16
Recommendations for treatment targets for LDL-C
Class Level In patients at VERY HIGH CV risk (established CVD, type 2 diabetes, type 1 diabetes with target organ damage, moderate to severe CKD or a SCORE level ≥ 10%) the LDL-C goal is < 1.8 mmol/L (less than ~ 70 mg/dL) and/or ≥ 50% LDL-C reduction when target level cannot be reached. I A In patients at HIGH CV risk (markedly elevated single risk factors, a SCORE level ≥ 5 to < 10%) an LDL-C goal < 2.5 mmol/L (less than ~ 100 mg/dL) should be considered. IIa In subjects at MODERATE risk (SCORE level > 1 to ≤ 5%) an LDL-C goal < 3.0 mmol/L (less than ~ 115 mg/dL) should be considered. C La riduzione di LDL-C necessaria per il raggiungimento del target spesso in questa categoria di pazienti è ≥ 50 % aClass of recommendation. bLevel of evidence. cReferences. CKD = chronic kidney disease; CV = cardiovascular; CVD = cardiovascular disease; LDL-C = low-density lipoprotein-cholesterol. European Heart Journal (2011) 32, 1769–1818
 the LDL-C goal is < 1.8 mmol/L (less than ~ 70 mg/dL) and/or ≥ 50% LDL-C reduction when target level cannot be reached. I. A. In patients at HIGH CV risk (markedly elevated single risk factors, a SCORE level ≥ 5 to < 10%) an LDL-C goal < 2.5 mmol/L (less than ~ 100 mg/dL) should be considered. IIa. In subjects at MODERATE risk (SCORE level > 1 to ≤ 5%) an LDL-C goal < 3.0 mmol/L (less than ~ 115 mg/dL) should be considered. C. La riduzione di LDL-C necessaria per il raggiungimento del. target spesso in questa categoria di pazienti è ≥ 50 % aClass of recommendation. bLevel of evidence. cReferences. CKD = chronic kidney disease; CV = cardiovascular; CVD = cardiovascular disease; LDL-C = low-density lipoprotein-cholesterol. European Heart Journal (2011) 32, 1769–1818.")
17
Recommendations for treatment of dyslipidaemia
in the elderly Recommendations Class Level Treatment with statins is recommended for elderly patients with established CVD in the same way as for younger patients. I B Since elderly people often have comorbidities and have altered pharmacokinetics, it is recommended to start lipid-lowering medication at a low doe and then titrate with caution to achieve target lipid levels which are the same as in the younger subjects. C Statin therapy may be considered in elderly subjects free of CVD, particularly in the presence of at least of at least one other CV risk factor besides age. IIb

18
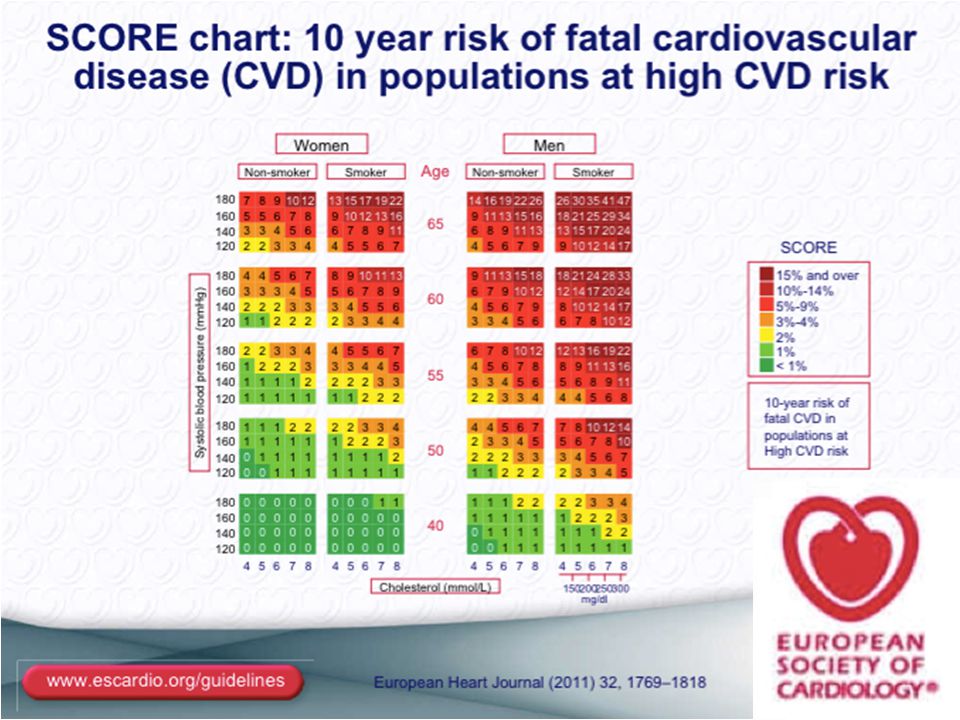
Preventive cardiology efforts begin with assessment of
Preventive cardiology efforts begin with assessment of cardiovascular disease risk Recommendation to begin with a global risk assessment using the Pooled Cohort Equations to estimate 10-year ASCVD Risk (other risk assessment algorithms include the European SCORE, PROCAM, or Framingham scores)
")
19
What’s New in the Cholesterol Guideline?
Focus on ASCVD reduction: 4 Statin Benefit Groups New Perspective on LDL-C and/or Non-HDL-C Treatment Goals Emphasis on the Clinician-Patient Risk Discussion Global Risk Assessment for Primary Prevention Safety Recommendations Critical questions addressed the evidence for LDL-C and non-HDL-C goals primary and secondary prevention and the evidence for reduction in ASCVD events in relation to cholesterol lowering drugs available

20
WHAT’S SIMILAR TO ATP III?
Emphasis on lifestyle measures as crucial Focus on treatment of LDL cholesterol (LDL-C) Greatest intensity of treatment for patients at highest risk Preference for statins over other medications lowering LDL-C (although this is greater in the new ACC/AHA Guideline)
 Greatest intensity of treatment for patients at highest risk. Preference for statins over other medications lowering LDL-C (although this is greater in the new ACC/AHA Guideline)")
21
4 STATIN BENEFIT GROUPS Clinical ASCVD
LDL–C >190 mg/dL, Age >21 years Primary prevention – Diabetes: Age years, LDL–C mg/dL Primary prevention - No Diabetes ≥ 7,5% 10-year ASCVD risk, Age years, LDL–C mg/dL, These identified statin benefit groups to not imply that other groups (e.g., those outside the specified age ranges) will not benefit and should not be treated
 will not benefit and should not be treated.")
22
INDIVIDUALS NOT IN A STATIN BENEFIT GROUP
In those for whom a risk decision is uncertain: These factors may inform clinical decision making: Family history of premature ASCVD Elevated lifetime risk of ASCVD LDL–C ≥160 mg/dL hs-CRP ≥2.0 mg/L Coronary artery calcium (CAC) score ≥300 Agaston units Ankle brachial index (ABI)<0.9 Their use still requires discussion between clinician and patient 22
 score ≥300 Agaston units. Ankle brachial index (ABI)<0.9. Their use still requires discussion between clinician and patient. 22.")
23
Summary of Statin Initiation Recommendations to Reduce ASCVD Risk (Revised Figure)
")
24
Summary of Statin Initiation Recommendations to Reduce ASCVD Risk (Revised Figure)
*The Pooled Cohort Equations can be used to estimate 10-year ASCVD risk in individuals with and without diabetes. A downloadable spreadsheet enabling estimation of 10-year and lifetime risk for ASCVD and a web-based calculator are available at and The calculator should be used to inform decision making in primary prevention patients not on a statin. †Consider moderate-intensity statin as more appropriate in low-risk individuals. ‡For those in whom a risk assessment is uncertain, factors such as primary LDL–C >160 mg/dL or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, lifetime risk of ASCVD, CAC score ≥300 Agatston units, or ≥75 percentile for age, sex, and ethnicity (For additional information, see ABI <0.9, or hs-CRP >2 mg/L. Additional factors that may aid in individual risk assessment may be identified in the future. §1) Potential ASCVD risk reduction benefits (e.g., absolute risk reduction from moderate- or high-intensity statin therapy can be approximated by using the estimated 10-year ASCVD risk and the relative risk reduction of ~30% for moderate-intensity statin or ~45% for high-intensity statin therapy. 2) Potential adverse effects. The excess risk of diabetes is the main consideration in ~0.1 excess case per 100 individuals treated with a moderate-intensity statin for 1 year and ~0.3 excess cases per 100 individuals treated with a high-intensity statin treated patients for 1 year. Note: a case of diabetes is not considered equivalent to a fatal or nonfatal MI or stroke. Both statin-treated and placebo-treated participants experienced the same rate of muscle symptoms. The actual rate of statin-related muscle symptoms in the clinical population is unclear. Muscle symptoms attributed to statin should be evaluated in as Table 8, Safety Rec 8. 24
 Potential ASCVD risk reduction benefits (e.g., absolute risk reduction from moderate- or high-intensity statin therapy can be approximated by using the estimated 10-year ASCVD risk and the relative risk reduction of ~30% for moderate-intensity statin or ~45% for high-intensity statin therapy. 2) Potential adverse effects. The excess risk of diabetes is the main consideration in ~0.1 excess case per 100 individuals treated with a moderate-intensity statin for 1 year and ~0.3 excess cases per 100 individuals treated with a high-intensity statin treated patients for 1 year. Note: a case of diabetes is not considered equivalent to a fatal or nonfatal MI or stroke. Both statin-treated and placebo-treated participants experienced the same rate of muscle symptoms. The actual rate of statin-related muscle symptoms in the clinical population is unclear. Muscle symptoms attributed to statin should be evaluated in as Table 8, Safety Rec")
25
Ray KK et al. Eur Heart J 2014

26
FIRE and Forget….. the patient !!
L’impatto della strategia ACC/AHA dovrebbe essere considerato alla luce del gran numero di soggetti nella popolazione che sarebbero destinati al trattamento con statine per tutta la vita a partire dall’età di 40 anni Per la popolazione europea si continua a raccomandare l’utilizzo delle tabelle SCORE o di tabelle nazionali calibrate sullo SCORE. La riduzione del rischio in generale deve essere personalizzata per ogni paziente, e questa pratica può essere più specifica se vengono definiti degli obiettivi. FIRE and Forget….. the patient !!

27
The results of the EUROASPIRE III survey show that despite the clear evidence of the benefits of lipid-lowering treatment in secondary prevention, many coronary patients with dyslipidaemia are still inadequately treated and a significant number of patients on lipid-lowering therapy is still not reaching the treatment goals. Almost half of all coronary patients did not reach the LDL-C goal of 2.5 mmol/L and about the same percentage did not reach the total cholesterol goal of 4.5 mmol/L Atherosclerosis 2013

28
Conoscendo la riduzione percentuale necessaria per raggiungere il target terapeutico, è possibile individuare quale opzione terapeutica consente di ottenerla.

35
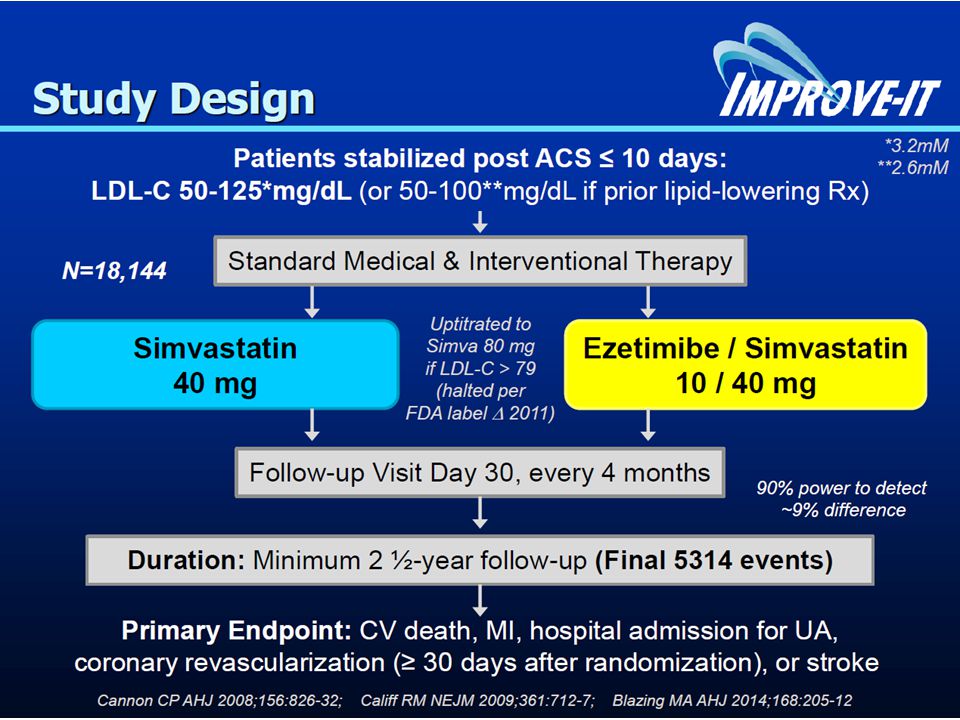
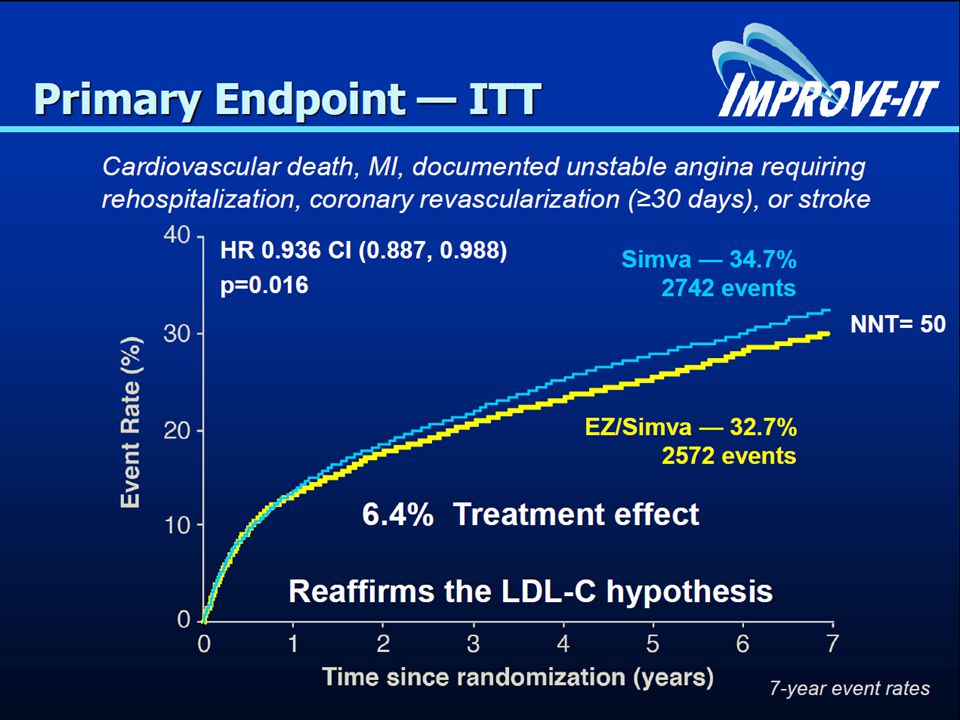
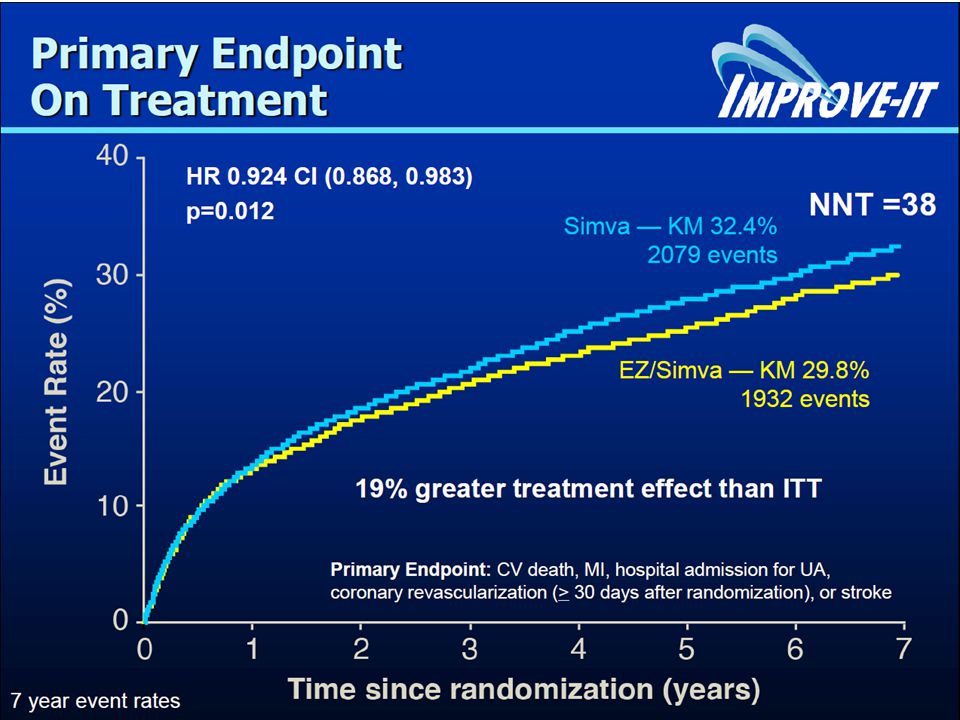
CONCLUSIONS IMPROVE-IT: First trial demonstrating incremental clinical benefit when adding a non-statin agent (ezetimibe) to statin therapy: YES: Non-statin lowering LDL-C with ezetimibe reduces cardiovascular events YES: Even Lower is Even Better (achieved mean LDL-C 53 vs. 70 mg/dL at 1 year) YES: Confirms ezetimibe safety profile Reaffirms the LDL hypothesis, that reducing LDL-C prevents cardiovascular events Results could be considered for future guidelines 35
 YES: Confirms ezetimibe safety profile. Reaffirms the LDL hypothesis, that reducing LDL-C prevents cardiovascular events. Results could be considered for future guidelines. 35.")
36
Target Stili di vita Tipo e dose di statina Aderenza Inerzia
Terapeutica Target Aderenza Stili di vita Tipo e dose di statina Le cause di questo fenomeno sono diverse : La mancata adesione agli stili di vita da parte del paziente che non considera dieta ed attività fisica come una terapia La mancata aderenza alla terapia o la breve persistenza in terapia La inappropriatezza prescrittiva con shift a statine meno potenti e/o rimodulazioni inappropriate della dose La discontinuità assistenziale con mancato uso delle LDL come guida alla terapia L’ inerzia terapaeutica per la quale non si modifica la terapia per motivazioni varie (strategia di attesa, poco è meglio di niente, paura di effetti collaterali) Appropriatezza Prescrittiva Continuità Assistenziale 36
 Appropriatezza. Prescrittiva. Continuità. Assistenziale. 36.")
37
G Ital Cardiol 2015;16(1):44-51
:44-51")
43
DEFINE Determining the EFficacy and Tolerability of CEPT INhibition with AnacEtrapib Safety of Anacetrapib in Patients with or at Risk for Coronary Heart Disease Christopher P. Cannon, MD, Sukrut Shah, PhD, RPh, Hayes M. Dansky, MD, Michael Davidson, MD, Eliot A. Brinton, MD, Antonio M. Gotto, Jr., MD, DPhil, Michael Stepanavage, MS, Sherry Xueyu Liu, MS, Patrice Gibbons, MS, Tanya B. Ashraf, BA, Jennifer Zafarino, MS, Yale Mitchel, MD, Philip Barter, MD, PhD, for the DEFINE Investigators

44
Effects on LDL-C and HDL-C
DEFINE Determining the EFficacy and Tolerability of CEPT INhibition with AnacEtrapib Effects on LDL-C and HDL-C HDL-C Study Week Baseline Wk 6 Wk 12 Wk 18 Wk 24 Wk 30 Wk 46 Wk 62 Wk 76 HDL-C (mg/dL) (SE) 20 40 60 80 100 120 Anacetrapib Placebo Anacetrapib n = 776 757 718 687 647 607 572 543 Placebo n = 766 761 741 744 736 711 691 666 LDL-C LDL-C (mg/dL) (SE) 804 771 716 646 604 568 540 803 759 743 735 -39.8% (p<0.001) +138.1% (p<0.001) The point estimates are for wk 24
 (SE) Anacetrapib. Placebo. Anacetrapib n = Placebo n = LDL-C. LDL-C (mg/dL) (SE) % (p<0.001) % (p<0.001) The point estimates are for wk 24.")
45
Anacetrapib treatment had robust effects on HDL-C, LDL-C, non HDL-C and Lp(a) with sustained effects over 18 months. Anacetrapib had an acceptable side-effect profile with no effects on blood pressure, electrolytes or aldosterone. Within the power of the study, anacetrapib did not exhibit adverse cardiovascular effects seen with a prior CETP inhibitor The long term safety and efficacy of anacetrapib will now be tested in a large clinical outcomes trial. Cannon CP et al. N Engl J Med 2010;363 (19) online 11/17/2010
 online 11/17/2010.")
46
30,000 patients with occlusive arterial disease in North America, Europe and Asia
Background LDL-lowering with atorvastatin Randomized to anacetrapib 100 mg vs. placebo Scheduled follow-up: 4 years Primary outcome: Coronary death, myocardial infarction or coronary revascularization

47
Lipid effects with dalcetrapib
18/04/2017 Lipid effects with dalcetrapib *p<0.0001 35 30 %change from baseline 25 20 *p<0.01 D 24 weeks D 48 weeks 15 Placebo 10 *p=0.002 5 Treatment with dalcetrapib led to significant increases in plasma HDL cholesterol levels (by 33%) and apolipoprotein A-I (by 11-16%) at weeks 24 and 48, together with about 50% reduction in CETP activity (54% at 24 weeks and 57% at 48 weeks, p< at each time point). There was negligible effect on LDL cholesterol levels. Reference 1. Stein EA, Stroes ESG, Steiner G et al. Am J Cardiol 2009;104:82-91 Dalcetrapib 900 mg/day -5 HDL-C LDL-C ApoA-I * D 48 weeks vs. placebo Stein EA et al. Eur Heart J 2010;31(4):480-8 47
 and apolipoprotein A-I (by 11-16%) at weeks 24 and 48, together with about 50% reduction in CETP activity (54% at 24 weeks and 57% at 48 weeks, p< at each time point). There was negligible effect on LDL cholesterol levels. Reference. 1. Stein EA, Stroes ESG, Steiner G et al. Am J Cardiol 2009;104: Dalcetrapib. 900 mg/day. -5. HDL-C. LDL-C. ApoA-I. * D 48 weeks vs. placebo Stein EA et al. Eur Heart J 2010;31(4):")
48
Dalcetrapib Phase IIb Trial HDL-C Increase at Week 12
* *P < vs placebo * Change From Baseline (%) * Dalcetrapib in some of the early phase trials has shown increases in HDL, again, somewhere in the 30% to 35% range. The 600 milligram is the dose that is currently under evaluation in clinical outcome studies. Key points: There was evidence of a dose-response relationship for HDL-C–raising with dalcetrapib up to 600 mg, after which it reached a plateau. At week 12, dalcetrapib 600 mg had raised HDL-C by 31% from baseline (P<0.0001). Background: The phase IIb study randomized patients aged 18–75 years with low or average HDL-C to receive placebo, dalcetrapib 300, 600 or 900 mg in addition to pravastatin 400 mg for 12 weeks. NOTE: Dalcetrapib 600 mg is the dose used in phase III. placebo n = 73 dalcetrapib 300 mg n = 75 dalcetrapib 600 mg n = 67 dalcetrapib 900 mg n = 72 NOTE: Dalcetrapib 600 mg is the dose used in phase III Stein EA. Am J Cardiol. 2009;104:82-91 48
 * Dalcetrapib in some of the early phase trials has shown increases in HDL, again, somewhere in the 30% to 35% range. The 600 milligram is the dose that is currently under evaluation in clinical outcome studies. Key points: There was evidence of a dose-response relationship for HDL-C–raising with dalcetrapib up to 600 mg, after which it reached a plateau. At week 12, dalcetrapib 600 mg had raised HDL-C by 31% from baseline (P<0.0001). Background: The phase IIb study randomized patients aged 18–75 years with low or average HDL-C to receive placebo, dalcetrapib 300, 600 or 900 mg in addition to pravastatin 400 mg for 12 weeks. NOTE: Dalcetrapib 600 mg is the dose used in phase III. placebo n = 73. dalcetrapib 300 mg n = 75. dalcetrapib 600 mg n = 67. dalcetrapib 900 mg n = 72. NOTE: Dalcetrapib 600 mg is the dose used in phase III. Stein EA. Am J Cardiol. 2009;104:")
49
CEPT Residual CV risk remains problematic despite statin- mediated LDL-C reduction Low HDL-C is an independent risk factor for CHD Most clinical trial and observational data suggest that raising HDL-C may reduce CVD HDL particles are very heterogeneous in composition and function, not all HDL may be anti-atherogenic Many new HDL-C raising treatments are in development CETP inhibitors greatly raise HDL-C levels, but their effect on HDL function and clinical outcomes remains in question

50
Revisiting the HDL Hypothesis
Residual CVD risk exists despite intense statin monotherapy Low HDL-C predicts high CVD risk; high HDL-C is protective Existing HDL raising therapies have inconsistent effects Investigational drugs to raise HDL-C and reduce CVD risk CETP inhibitors PPAR agonists, APO A1 agonists, delipidating agents, etc. But clinical trials have not yet proven that: HDL is a causal factor vs biomarker of risk Raising HDL-C reduces CVD risk

51
Don’t give up on HDL, researchers plead
At a session on the subject, Dr Alan Tall (Columbia University, New York) summarized the situation: "The HDL hypothesis is certainly under attack. And there have been a lot of setbacks. But we mustn't throw the baby out with the bathwater. I think we need a new, modified HDL hypothesis." Hughs S, Jun, 2012
 summarized the situation: The HDL hypothesis is certainly under attack. And there have been a lot of setbacks. But we mustn t throw the baby out with the bathwater. I think we need a new, modified HDL hypothesis. Hughs S, Jun,")
52
Increased risk of diabetes with statin treatment is associated with impaired insulin sensitivity and insulin secretion: a 6 year follow-up study of the METSIM cohort Cederberg H(1), Stančáková A, Yaluri N, Modi S, Kuusisto J, Laakso M. Diabetologia May; 58(5):
:")
53
STATINS AND DIABETES RISK
1) Meta-analysis of 170,255 patients from 76 randomized clinical trials show overall a 9% increased risk for development of incident diabetes among statin users (Sattar, Lancet 2010) 2) Increased risk of diabetes only seen in those with multiple risk factors; obesity, elevated triglycerides, glucose, and hypertension are more strongly related than statins to development of diabetes 3) Many persons on statins have pre-diabetes to begin with; statins may accelerate the progression to diabetes, but on average diabetes occurs 5 weeks later in those on placebo. 4) For every case of diabetes associated with statin use, approximately 5-9 cardiovascular events are prevented 5) Most experts contend the benefits outweigh the risks regarding increases in glucose / A1c.
 Meta-analysis of 170,255 patients from 76 randomized clinical trials show overall a 9% increased risk for development of incident diabetes among statin users (Sattar, Lancet 2010) 2) Increased risk of diabetes only seen in those with multiple risk factors; obesity, elevated triglycerides, glucose, and hypertension are more strongly related than statins to development of diabetes. 3) Many persons on statins have pre-diabetes to begin with; statins may accelerate the progression to diabetes, but on average diabetes occurs 5 weeks later in those on placebo. 4) For every case of diabetes associated with statin use, approximately 5-9 cardiovascular events are prevented. 5) Most experts contend the benefits outweigh the risks regarding increases in glucose / A1c.")
54
Statins and diabetes risk: how real is it and what are the mechanisms
Statins and diabetes risk: how real is it and what are the mechanisms? Jennifer G. Robinson Statins are associated with a modest excess risk of type 2 diabetes mellitus in individuals at risk for diabetes. Multiple mechanisms have been proposed for statin-associated diabetes, primarily related to increased insulin resistance and decreased insulin secretion. Diabetes is diagnosed on average 2–4 months earlier in statin-treated patients compared with untreated patients, and is therefore unlikely to have any more adverse consequences in the long term than diabetes occurring in patients who did not receive statins. The cardiovascular risk reduction benefits far outweigh the potential for adverse effects in all but the very lowest risk individuals. Curr Opin Lipidol Jun;26(3):228-35
:")
Presentazioni simili






>")



 sottoposto a CABG.>")












