Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
CHE COS’È LA CHEMIOTERAPIA ?

2
La chemioterapia è una branca della farmacoterapia che si riferisce all’uso di farmaci con lo scopo di uccidere organismi estranei patogeni presenti nel paziente (o almeno di inibirne la crescita)
")
3
QUALI SONO I BERSAGLI DELLA CHEMIOTERAPIA ?

4
batteri virus e funghi parassiti cellule tumorali

5
BASI DELLA SELETTIVITÀ D’AZIONE
DEI CHEMIOTERAPICI Bersagli esclusivi, presenti unicamente nell’organismo patogeno, (o nella cellula patologica) Bersagli selettivi, presenti sia nell’ospite sia nell’organismo patogeno, ma con caratteristiche farmacologiche differenti Bersagli comuni, presenti sia nell’ospite sia nell’organismo patogeno, ma essenziali solo per quest’ultimo
 Bersagli selettivi, presenti sia nell’ospite sia nell’organismo patogeno, ma con caratteristiche farmacologiche differenti. Bersagli comuni, presenti sia nell’ospite sia nell’organismo patogeno, ma essenziali solo per quest’ultimo.")
6
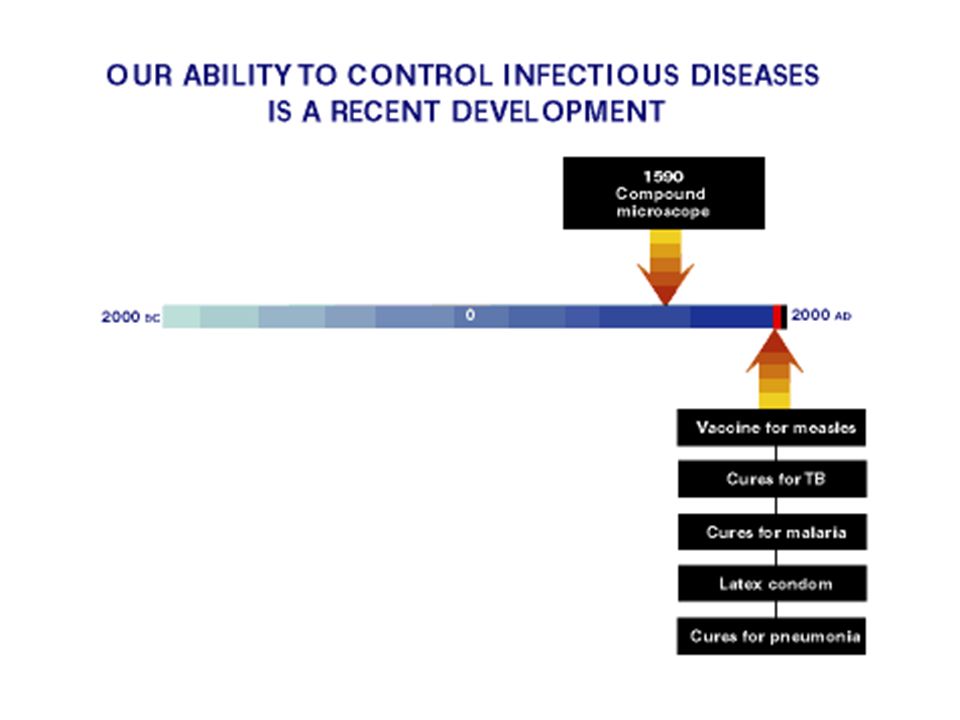
PREVENIRE È SEMPRE MEGLIO CHE CURARE

7
Semmelweis nel 1847 introdusse nel suo reparto di ostetricia la pratica del lavaggio delle mani con cloruro di calcio, riducendo drasticamente la mortalità da febbre puerperale

9
gli ANTISETTICI sono sostanze chimiche troppo tossiche per l’uso sistemico, ma sufficientemente poco tossiche per l’uso topico Alcooli Clorexidina Tintura di iodio Perossido di idrogeno Nel 1967/8 Joseph Lister, basandosi sugli studi di Pasteur, introdusse la pratica della disinfezione delle ferite, chirurgiche e accidentali, con acido fenico, riducendo drasticamente il numero di amputazioni e la letalità dovuta a sepsi.

10
i DISINFETTANTI sono sostanze chimiche anti-infettive la cui tossicità è tale da conbsentirne l’applicazione solamente a superficie inanimate Aldeidi (formaldeide, glutaraldeide) Ipoclorito di sodio (candeggina)
 Ipoclorito di sodio (candeggina)")
12
gli ANTIBIOTICI sono composti isolati da organismi viventi in grado di uccidere, o di inibire la crescita di, altri organismi

13
SERENDIPITY: "One sometimes finds what one is not looking for.“
the faculty of making providential discoveries by accident (from its possession by the characters in the Persian fairy tale The three princes of Serendip) "One sometimes finds what one is not looking for.“ Sir Alexander Fleming
 One sometimes finds what one is not looking for. Sir Alexander Fleming.")
16
EFFETTI AVVERSI DEI CHEMIOTERAPICI ANTIBATTERICI
REAZIONI ALLERGICHE EFFETTI BIOLOGICI TOSSICITÀ A CARICO DI: rene orecchio (coclea e/o organi vestibolari) ossa e denti muscolatura respiratoria
 ossa e denti. muscolatura respiratoria.")
17
Figure 2 | Antibacterial drug targets
Figure 2 | Antibacterial drug targets. There are five main antibacterial drug targets in bacteria: cell-wall synthesis, DNA gyrase, metabolic enzymes, DNA-directed RNA polymerase and protein synthesis. The figure shows the antimicrobial agents that are directed against each of these targets. In the case of protein synthesis, aminoglycosides and tetracyclines inhibit 30S RNA, and macrolides, chloramphenicol and clindamycin inhibit 50S RNA. mRNA, messenger RNA.

18
i chemioterapici ad azione BATTERICIDA sono in grado di uccidere il microrganismo patogeno
esempi: penicilline aminoglicosidi fluorochinoloni

19
i chemioterapici ad azione BATTERIOSTATICA sono in grado di arrestare la crescita del microrganismo patogeno esempi: sulfamidici tetracicline macrolidi

20
LA DISTINZIONE TRA CHEMIOTERAPICI AD AZIONE BATTERICIDA
E CHEMIOTERAPICI AD AZIONE BATTERIOSTATICA NON È UN CONCETTO ASSOLUTO

21
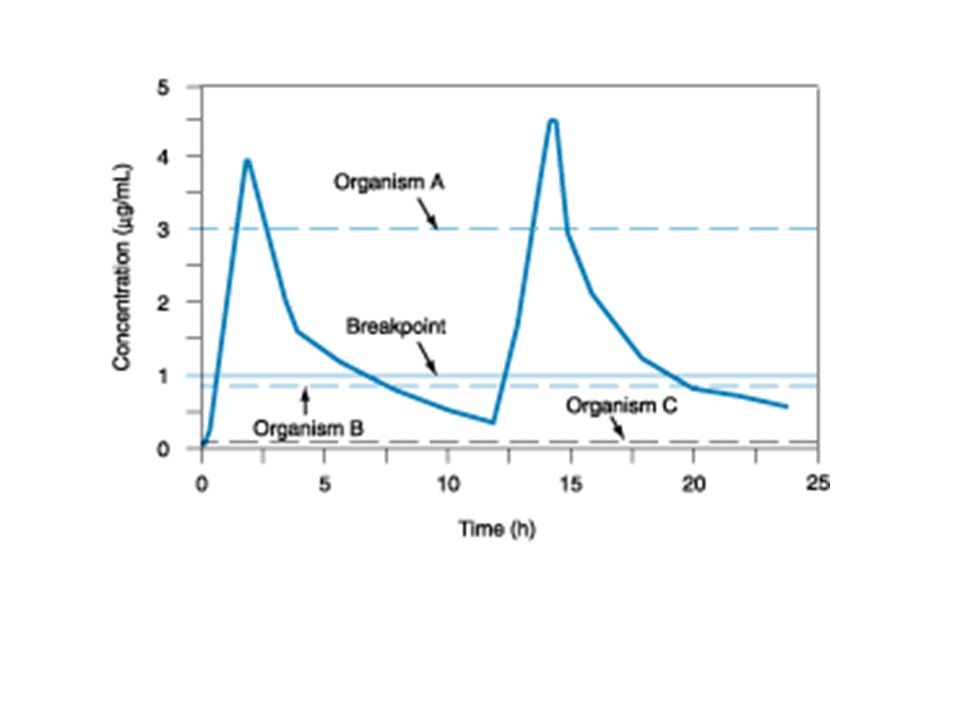
MIC MBC I FARMACI ANTIMICROBICI SONO CARATTERIZZATI DA minima
concentrazione inibente minima concentrazione battericida

22
chemioterapici ad azione battericida CONCENTRAZIONE - DIPENDENTE

23
chemioterapici ad azione battericida CONCENTRAZIONE - DIPENDENTE

24
chemioterapici ad azione battericida TEMPO - DIPENDENTE

25
chemioterapici ad azione battericida TEMPO - DIPENDENTE

28
MECCANISMI DI TRASMISSIONE DELLA RESISTENZA NEI BATTERI
TRASMISSIONE VERTICALE Geni che codificano per bersagli mutati e/o trasportatori vengono trasmessi alle cellule figlie

29
MECCANISMI DI TRASMISSIONE DELLA RESISTENZA NEI BATTERI
1 CONIUGAZIONE 2 TRASFORMAZIONE 3 TRASDUZIONE Drug resistance genes can be spread from one bacterium to another through various mechanisms such as plasmids, bacteriophages, naked DNA or transposons. Some transposons contain integrons—more complex transposons that contain a site for integrating different antibiotic resistance genes and other gene cassettes in tandem for expression from a single promoter91. Originally discovered among Gram-negative bacteria, integrons have been since located in Gram-positive commensal flora—a newly found reservoir of these unique genetic elements92. A model of resistance gene spread is the tet(M) tetracycline resistance gene, which is commonly located on the transposon Tn916 (ref. 93). It has been found in Gram-positive and Gram-negative bacteria, aerobic and anaerobic bacteria, and in all environmental and biological niches94. Chromosomal genes can be also transferred: they are acquired by one bacterium through the uptake of naked DNA released from another microorganism. This transfer process, called transformation, created penicillin-resistant S. pneumoniae through the acquisition of genes from the naturally occurring, penicillin-resistant commensal Streptococcus viridans and the formation of mosaic, penicillin-insensitive, penicillin-binding proteins95, 96. Similar exchanges have helped to generate quinolone-resistant strains of S. pneumoniae through the production of a mutant drug-resistant gyrase97. Other organisms that are easily capable of integrating naked chromosomal DNA are H. influenzae and A. baumanii. The pneumococci have shown that the chromosomal location of the resistance determinant is not a safeguard against its spread. Bacteria themselves are mobile and can easily travel from person to person and between countries. Resistant pneumococci in Iceland and in the United States have been shown to be the progeny of strains that initially appeared in Spain85. Thus, countries and citizens worldwide have become part of a global microbial ecology, sharing and spreading the consequences of antimicrobial resistance.
 tetracycline resistance gene, which is commonly located on the transposon Tn916 (ref. 93). It has been found in Gram-positive and Gram-negative bacteria, aerobic and anaerobic bacteria, and in all environmental and biological niches94. Chromosomal genes can be also transferred: they are acquired by one bacterium through the uptake of naked DNA released from another microorganism. This transfer process, called transformation, created penicillin-resistant S. pneumoniae through the acquisition of genes from the naturally occurring, penicillin-resistant commensal Streptococcus viridans and the formation of mosaic, penicillin-insensitive, penicillin-binding proteins95, 96. Similar exchanges have helped to generate quinolone-resistant strains of S. pneumoniae through the production of a mutant drug-resistant gyrase97. Other organisms that are easily capable of integrating naked chromosomal DNA are H. influenzae and A. baumanii. The pneumococci have shown that the chromosomal location of the resistance determinant is not a safeguard against its spread. Bacteria themselves are mobile and can easily travel from person to person and between countries. Resistant pneumococci in Iceland and in the United States have been shown to be the progeny of strains that initially appeared in Spain85. Thus, countries and citizens worldwide have become part of a global microbial ecology, sharing and spreading the consequences of antimicrobial resistance.")
30
L’USO IMPROPRIO DEI CHEMIOTERAPICI PUÒ
FACILITARE LO SVILUPPO DI RESISTENZA DOSAGGIO INSUFFICIENTE INSUFFICIENTE DURATA DELLA TERAPIA

31
Figure 4 | Prolonged chemotherapy can lead to an enhanced rate of emergence of resistance to antibacterial agents. a | Most multiplying bacteria are killed by bactericidal antibiotics, such as penicillin. b | Surviving bacteria that are not killed can, over a period of days, produce resistant clones, which are then selected by the antimicrobial agent. This results in the resistant clone becoming predominant.

32
L’USO IMPROPRIO DEI CHEMIOTERAPICI PUÒ
FACILITARE LO SVILUPPO DI RESISTENZA DOSAGGIO INSUFFICIENTE INSUFFICIENTE DURATA DELLA TERAPIA INTERVALLI TRA LE DOSI INAPPROPRIATI SCELTA INAPPROPRIATA DELL’ANTIBIOTICO RICORSO ALLA SOLA CHEMIOTERAPIA IN INFEZIONI CON COMPLICANZE USO DI ANTIBIOTICI NELL’ALLEVAMENTO DEL BESTIAME

33
Manca: antibiotici nell’allevamento come fattore di resistenza Azione battericida e batteriostatica come criterio per l’uso di chemioterapici in associazione

34
1a 1 Meccanismi che riducono l’accesso del farmaco al bersaglio 1b 1c 2a 2b 2 Alterazioni quali- e/o quantitative del bersaglio Figure 3 | Mechanisms of genetic resistance to antimicrobial agents. Bacteria have developed, or will develop, genetic resistance to all known antimicrobial agents that are now in the marketplace. The five main mechanisms that bacteria use to resist antibacterial drugs are shown in the figure. a | The site of action (enzyme, ribosome or cell-wall precursor) can be altered. For example, acquiring a plasmid or transposon that codes for a resistant dihydrofolate reductase confers trimethoprim resistance to bacteria52. b | The inhibited steps can be by-passed. c | Bacteria can reduce the intracellular concentration of the antimicrobial agent, either by reducing membrane permeability, for example, as shown by Pseudomonas aeruginosa53, or by active efflux of the agent54. d | They can inactivate the drug. For example, some bacteria produce -lactamase, which destroys the penicillin -lactam ring50, 51 (Fig. 1). e | The target enzyme can be overproduced by the bacteria. 3 Meccanismi a valle dell’interazione con il bersaglio
 can be altered. For example, acquiring a plasmid or transposon that codes for a resistant dihydrofolate reductase confers trimethoprim resistance to bacteria52. b | The inhibited steps can be by-passed. c | Bacteria can reduce the intracellular concentration of the antimicrobial agent, either by reducing membrane permeability, for example, as shown by Pseudomonas aeruginosa53, or by active efflux of the agent54. d | They can inactivate the drug. For example, some bacteria produce -lactamase, which destroys the penicillin -lactam ring50, 51 (Fig. 1). e | The target enzyme can be overproduced by the bacteria. 3. Meccanismi a valle dell’interazione con il bersaglio.")
35
Resistance mechanisms vary
Resistance mechanisms vary. Some are directed at the antibiotic itself: enzymes such as -lactamases destroy penicillins and cephalosporins, and modifying enzymes inactivate chloramphenicol and aminoglycosides such as streptomycin and gentamicin. Others target how the drug is transported; for example, an active efflux of drug mediates resistance to the tetracyclines, chloramphenicol and the fluoroquinolones98, 99. A third type of mechanism (not shown) alters the intracellular target of the drug—for example, the ribosome, metabolic enzymes or proteins involved in DNA replication or cell wall synthesis—making the drug unable to inhibit a vital function in the microbial cell. The same kind of drug resistance mechanism can be specified by many different genes. For example, the -lactamases now number in the hundreds and more than 20 different resistance determinants mediate an efflux of tetracyclines100. In addition, more than one type of mechanism may provide resistance to the same antibiotic; for example, tetracycline resistance can be effected by either efflux or ribosome protection101. Although most fluoroquinolone resistance stems from chromosomal mutations in the gyrase target or from drug efflux, a plasmid-mediated resistance to fluoroquinolones has been recently described102. Since being recognized, it has been found among clinical strains of E. coli and K. pneumoniae 103. Multidrug resistance can be specified by chromosomal genes for regulatory proteins such as MarA and SoxS. These proteins promote drug resistance by controlling the expression of other chromosomal genes, such as those involved in drug efflux61.
 alters the intracellular target of the drug—for example, the ribosome, metabolic enzymes or proteins involved in DNA replication or cell wall synthesis—making the drug unable to inhibit a vital function in the microbial cell. The same kind of drug resistance mechanism can be specified by many different genes. For example, the -lactamases now number in the hundreds and more than 20 different resistance determinants mediate an efflux of tetracyclines100. In addition, more than one type of mechanism may provide resistance to the same antibiotic; for example, tetracycline resistance can be effected by either efflux or ribosome protection101. Although most fluoroquinolone resistance stems from chromosomal mutations in the gyrase target or from drug efflux, a plasmid-mediated resistance to fluoroquinolones has been recently described102. Since being recognized, it has been found among clinical strains of E. coli and K. pneumoniae 103. Multidrug resistance can be specified by chromosomal genes for regulatory proteins such as MarA and SoxS. These proteins promote drug resistance by controlling the expression of other chromosomal genes, such as those involved in drug efflux61.")
36
There are five families of multidrug-resistance efflux pumps: the ATP-binding cassette (ABC) superfamily, the major facilitator superfamily (MFS), the multidrug and toxic-compound extrusion (MATE) family, the small multidrug resistance (SMR) family and the resistance nodulation division (RND) family. A diagrammatic representation of the structure and membrane location of efflux pumps from each of these families is shown. Common examples of the individual proteins that form each class of efflux pump are indicated. Antibiotic substrates and examples of other substrates are also listed for each class of efflux pump. Multidrug-resistance efflux pumps expressed by Gram-negative bacteria usually have several components, and the outer-membrane protein is typically TolC. Pi, inorganic phosphate.

37
Multidrug resistance mechanisms associated with porin modification
Multidrug resistance mechanisms associated with porin modification. Shows the various resistance mechanisms that are associated with porin modification. The β-lactam molecules and porin trimers are represented by blue circles and pink cylinders, respectively. The thickness of the straight arrows reflects the level of β-lactam penetration through porin channels. The curved arrows illustrate the uptake failure that occurs with: a change (decrease) in the level of porin expression; an exchange in the type of porin that is expressed (restricted-channel porin); and mutation or modification that impairs the functional properties of a porin channel (mutated porin). The effect of pore-blocking molecules (black circles) is shown at the bottom of the figure.
 in the level of porin expression; an. exchange in the type of porin that is expressed (restricted-channel porin); and mutation or modification that impairs the functional properties of a porin channel (mutated porin). The effect of pore-blocking molecules (black circles) is shown at the. bottom of the figure.")
38
Figure 5 | Non-multiplying bacteria
Figure 5 | Non-multiplying bacteria. a | Bacteria can exist in two states — multiplying and non-multiplying. Most infections contain both multiplying and non-multiplying organisms. During a course of antimicrobial agents to treat an infection, all the multiplying bacteria are quickly killed, leaving a pool of non-multiplying organisms that survive. When the levels of antimicrobial agent fall between doses, the non-multiplying bacteria 'spin off' multiplying ones, which are then killed by the next dose of the drug.

39
Figure 5 | Non-multiplying bacteria
Figure 5 | Non-multiplying bacteria. . b | Antibiotics, such as penicillin, can kill multiplying bacteria within hours, but are either ineffective or only partially effective against non-multiplying organisms.

40
Figure 7 | Killing non-multiplying bacteria with one-dose therapy
Figure 7 | Killing non-multiplying bacteria with one-dose therapy. a | In a patient with a bacterial infectious disease, such as pneumonia, both multiplying and non-multiplying bacteria are present. The antimicrobial agent kills the multiplying bacteria but does not kill the non-multiplying ones. When the level of the drug dips between doses, metabolism in the surviving non-multiplying bacteria spurts into activity, and some start to multiply. The next dose of antimicrobial agent, which raises the level of drug, kills these multiplying organisms. The number of bacteria in the non-multiplying pool gradually declines, but enough survive to repeat the cycle many times. If antimicrobial treatment is stopped too early, non-multiplying bacteria can start to multiply again, which leads to reactivation of infectious disease. Eventually, when the non-multiplying pool is either eliminated or can be mopped up by the immune system, the patient is cured. However, prolonged treatment with antimicrobial agents, particularly with suboptimal concentrations or in the presence of partially resistant bacteria, leads to resistance in the commensal bacteria of the bowel, mucosa and skin. Over the period of chemotherapy, these resistant bacteria increase in number, and can be transmitted to other people, or cause disease with a resistant organism in the parent host.

41
Figure 7 | Killing non-multiplying bacteria with one-dose therapy
Figure 7 | Killing non-multiplying bacteria with one-dose therapy. b | Drug discovery that is aimed at this non-multiplying population should result in shorter periods of chemotherapy, perhaps one dose. This should lead to a lower level of resistance in the commensal flora and could prolong the effective life of new antimicrobial agents. A drug that could kill the non-multiplying bacteria should lead to an overall improvement in the rate of emergence of resistance, not only because it should reduce chromosomal resistance in clinically latent bacteria, but also because it should improve patient compliance.

42
Five stages of biofilm development
Five stages of biofilm development. Biofilm maturation is a complex developmental process that involves several stages, each with unique characteristics that should be considered when designing strategies for biofilm treatment with antibiotics. Each stage of development in the diagram is paired with a photomicrograph of a developing Pseudomonas aeruginosa biofilm. All photomicrographs are shown at the same scale. Modified with permission from Ref. 58 © (2002) American Society for Microbiology. Please close this window to return to the main article.
 American Society for Microbiology. Please close this window to return to the main article.")
43
Schematic showing three examples of possible points of entry into the body for infectious biofilms; catheter, hip replacement, and periodontal disease. Arrows show how the biofilm (green) might be disseminated around the body, either by single cells or clumps of protected emboli, using the example of native or artificial heart valve infective endocarditis as a common central location for embolization. Sporadic detachment could lead to cycles
 might be disseminated around the body, either by single cells or clumps of protected emboli, using the example of native or artificial heart valve infective endocarditis as a common central location for embolization. Sporadic detachment could lead to cycles.")
45
Metabolic activity in a biofilm mirocolony
Metabolic activity in a biofilm mirocolony. Metabolic activity in a biofilm cell cluster is a function of depth within the biofilm and is influenced by nutrient transport. Cells at the edges of a microcolony at the bulk liquid interface are the most active. Cells deep within the microcolony can potentially remain dormant and provide a nucleus for regrowth following antibiotic treatment.

46
Biofilm resistance to anibiotic addition
Biofilm resistance to anibiotic addition. Treatment of biofilms with antibiotics often results in incomplete killing, allowing unaffected bacteria to act as a nucleus for the spread of infection following the withdrawal of antibiotic therapy.

47
FIGURE 4 | Biofilm drug resistance
FIGURE 4 | Biofilm drug resistance. The figure shows a model of biofilm resistance to killing based on persister survival. Initial treatment with antibiotic kills normal cells (coloured green) in both planktonic and biofilm populations. The immune system kills planktonic persisters (coloured pink), but the biofilm persister cells (coloured pink) are protected from the host defences by the exopolymer matrix. After the antibiotic concentration is reduced, persisters resuscitate and repopulate the biofilm and the infection relapses. Modified with permission from Ref 51 © (2001) American Society for Microbiology.
 in both planktonic and biofilm populations. The immune system kills planktonic persisters (coloured pink), but the biofilm persister cells (coloured pink) are protected from the host defences by the exopolymer matrix. After the antibiotic concentration is reduced, persisters resuscitate and repopulate the biofilm and the infection relapses. Modified with permission from Ref 51 © (2001) American Society for Microbiology.")
48
CONSIDERAZIONI NELLA SCELTA DI UNA TERAPIA ANTIBIOTICA
FATTORI RELATIVI AL BATTERIO identità del patogeno (spesso non nota all’inizio della terapia) sensibilità del patogeno
 sensibilità del patogeno.")
49
CONSIDERAZIONI NELLA SCELTA DI UNA TERAPIA ANTIBIOTICA
FATTORI RELATIVI AL PAZIENTE sito dell’infezione allergie funzionalità epatica e renale neutropenia funzione digerente malattie concomitanti e relative terapie gravidanza

50
CONSIDERAZIONI NELLA SCELTA DI UNA TERAPIA ANTIBIOTICA
FATTORI RELATIVI AL FARMACO attività sul patogeno (spesso non nota all’inizio della terapia) accessibilità al sito dell’infezione possibili interazioni con altri farmaci vie di somministrazione frequenza del dosaggio gusto stabilità a diverse temperature costo
 accessibilità al sito dell’infezione. possibili interazioni con altri farmaci. vie di somministrazione. frequenza del dosaggio. gusto. stabilità a diverse temperature. costo.")
51
RAZIONALE PER L’USO DI COMBINAZIONI DI CHEMIOTERAPICI
TERAPIA EMPIRICA DI INFEZIONI A GENESI IGNOTA TRATTAMENTO DI INFEZIONI POLIMICROBICHE AUMENTO DELL’ATTIVITÀ ANTIBATTERICA NEL TRATTAMENTO DI INFEZIONI SPECIFICHE PREVENZIONE DELL’EMERGENZA DI MICRORGANISMI RESISTENTI

52
POSSIBILI LIVELLI DI INTERAZIONE TRA FARMACI
Interazione chimica Interazione farmacocinetica Interazione farmacodinamica attività farmacologica tossicità resistenza

53
TIME-KILL CURVES Ore dopo l’inoculo

54
USO DI COMBINAZIONI DI CHEMIOTERAPICI ASPETTI QUANTITATIVI

55
DELL’USO COMBINATO DEI CHEMIOTERAPICI
POSSIBILI SVANTAGGI DELL’USO COMBINATO DEI CHEMIOTERAPICI AUMENTO DEI COSTI DELLA TERAPIA DIMINUZIONE DELLA COMPLIANCE DEL PAZIENTE RISCHIO DI AUMENTATA TOSSICITÀ RISCHIO DI INTERAZIONI ANTAGONISTICHE SELEZIONE DI MICRORGANISMI MULTIRESISTENTI

56
PROFILASSI DELLE INFEZIONI CON AGENTI ANTIMICROBICI
PROTEZIONE NEI CONFRONTI DI MICRORGANISMI SPECIFICI PAZIENTI IMMUNOCOMPROMESSI PAZIENTI SOTTOPOSTI A PROCEDURE CHIRURGICHE

Presentazioni simili