Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Summary of variations in RBC shape (poikilocytosis)
")
2
Microcitosi Macrocitosi Tear-drop cell Cellula nucleata Target cell
Frammentazione Macrocitosi Tear-drop cell Cellula nucleata Target cell Normal

3
Anemia sideropenica grave
Globuli rossi microcitici e ipocromici più piccoli del nucleo di un linfocita + anisocitosi + poikilocitosi

4
Macrocitosi (macro-ovalociti)
Globuli rossi più grandi di un linfocita, ricchi in emoglobina

5
Howell-Jolly bodies. In the absence of a functional spleen, nuclear remnants are not culled from the red cells and remain as small homogeneously staining inclusions

6
Red cell changes in myelofibrosis.
The left panel shows a teardrop-shaped cell. The right panel shows a nucleated red cell. These forms are seen in myelofibrosis

7
Target cells Tipiche nella talassemia e in epatopatie

8
Red cell fragmentation.
Red cells may become fragmented in the presence of foreign bodies in the circulation, such as mechanical heart valves, or in the setting of thermal injury

9
Echinociti The red cells in uremia may acquire numerous regularly spaced, small, spiny projections. Such cells, called burr cells or echinocytes, are readily distinguishable from irregularly spiculated acanthocytes

10
Cellule a sperone - Acantociti
Spur cells are recognized as distorted red cells containing several irregularly distributed thornlike projections. Cells with this morphologic abnormality are also called acanthocytes

11
Reticolociti Methylene blue stain demonstrates residual RNA in newly made red cells POLICROMASIA: reticolociti rilasciati precocemente dal midollo

12
Diagnosis of anemia Reticulocyte count gives an indication of the level of the bone marrow activity. Done by staining a peripheral blood smear with new methylene blue to help visualize remaining ribosomes. The number of reticulocytes/1000 RBC is counted and reported as a %. At birth the normal range is 1.8-8% The normal range in an adult (i.e. in an individual with no anemia) is %. Note that this % is not normal for anemia where the bone marrow should be working harder and throwing out more reticulocytes per day. In anemia the reticulocyte count should be elevated above the normal values.
 is %. Note that this % is not normal for anemia where the bone marrow should be working harder and throwing out more reticulocytes per day. In anemia the reticulocyte count should be elevated above the normal values.")
13
The critical elements of erythropoiesis
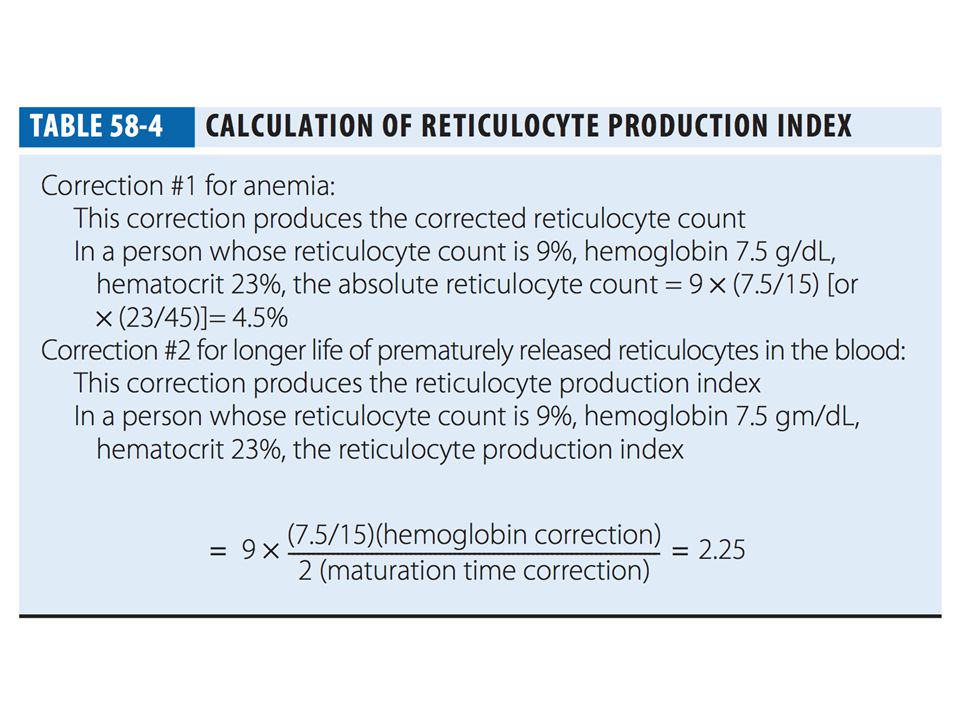
L'indice di produzione dei reticolociti è una misura indiretta di una appropriata EPO production, iron availability, the proliferative capacity of the bone marrow, and effective maturation of red cell precursors

14
CLASSIFICAZIONE INIZIALE DELLA
ANEMIA

16
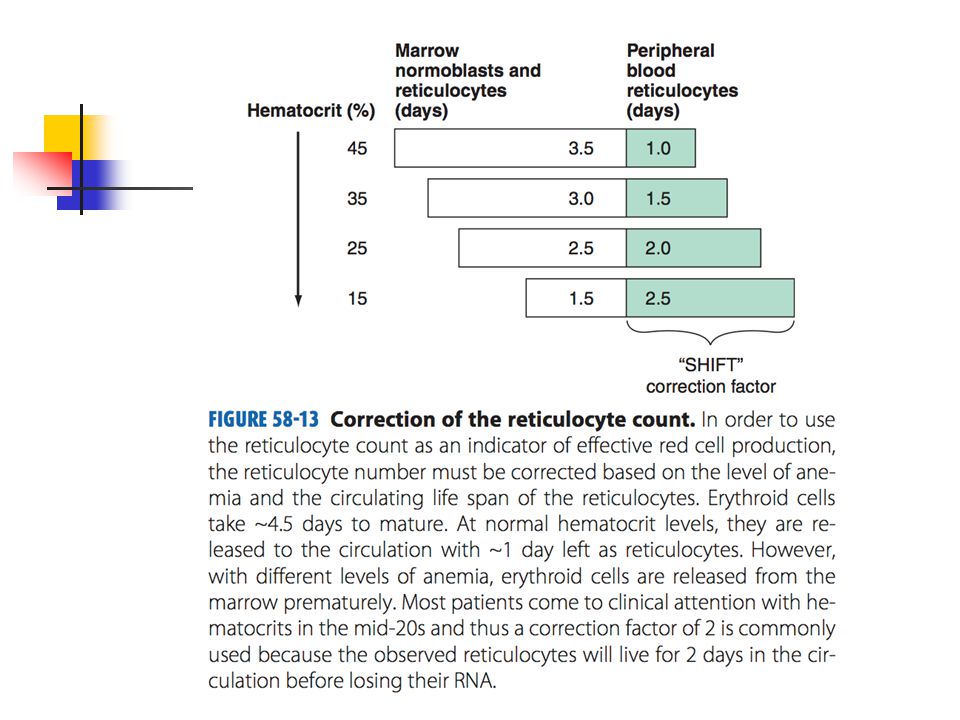
Diagnosis of anemia To get a better indication of what is really going on, a corrected reticulocyte count is done. Prima correzione. La conta dei reticolociti è corretta sul valore dell'ematocrito. As an anemia gets more severe, i reticolociti vengono rilasciati prematuramente. Queste cellule più giovani impiegano più di 24 hours to mature (shift reticulocyte – macrocita policromatofilo). The reticulocyte production index (RPI) is a truer indication of the real bone marrow activity. Se EPO aumenta e il midollo è OK following onset of anemia, ti devi aspettare 2-3 volte più reticolociti
. The reticulocyte production index (RPI) is a truer indication of the real bone marrow activity. Se EPO aumenta e il midollo è OK following onset of anemia, ti devi aspettare 2-3 volte più reticolociti.")
19
funzionale della anemia
Classificazione funzionale della anemia CBC, reticolociti Index < 2.5 Index > 2.5 Definition and classification of anemia Initial classification of anemia Classifying an anemia according to the functional defect in red cell production helps organize the subsequent use of laboratory studies. The three major classes of anemia are: 1) marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1. hypoproliferative anemia or maturation disorder. Diminuita sopravvivenza dei globuli rossi hemolysis is most likely
 marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1. hypoproliferative anemia or maturation disorder. Diminuita sopravvivenza dei globuli rossi. hemolysis is most likely.")
20
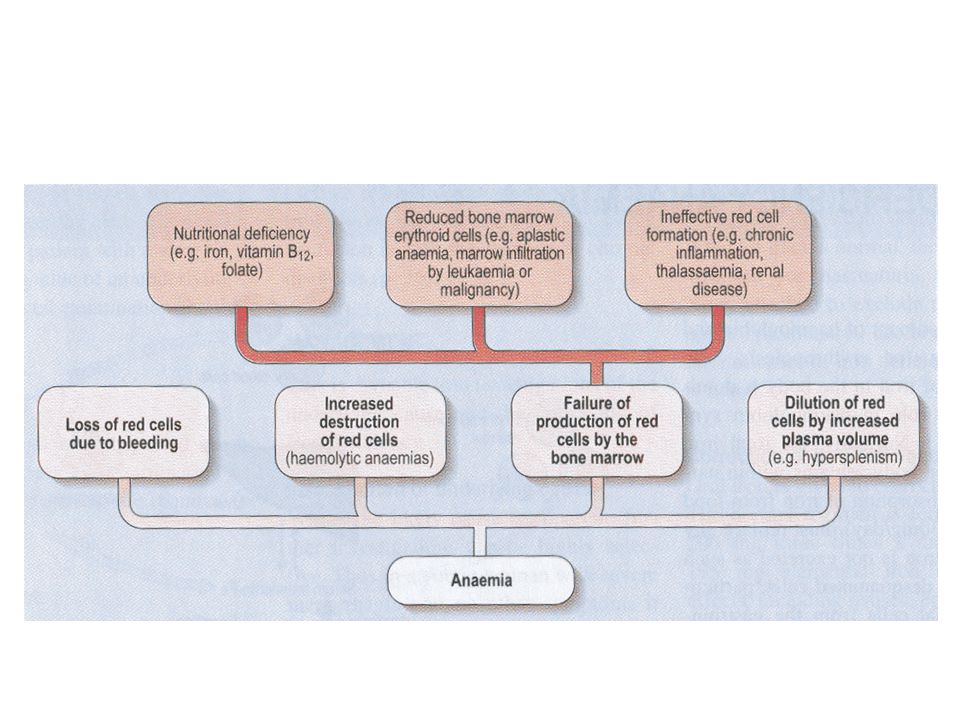
Classificazione in base alla produttività del midollo
Una ridotta presenza nel sangue dei globuli rossi può essere dovuta a: ridotta sintesi perdita di sangue eliminazione dal circolo più veloce del processo di sintesi (anemia emolitica) Si ha sintesi ridotta nei casi di: ridotta capacità generativa da parte del midollo osseo assenza dei fattori essenziali alla maturazione cellulare
 Si ha sintesi ridotta nei casi di: ridotta capacità generativa da parte del midollo osseo. assenza dei fattori essenziali alla maturazione cellulare.")
21
funzionale della anemia
Classificazione funzionale della anemia CBC, reticolociti Index < 2.5 Difetti di maturazione dei globuli rossi Difetti di produttività del midollo Definition and classification of anemia Initial classification of anemia Classifying an anemia according to the functional defect in red cell production helps organize the subsequent use of laboratory studies. The three major classes of anemia are: 1) marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1.
 marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1.")
22
funzionale della anemia
Classificazione funzionale della anemia CBC, reticolociti Index < 2.5 Index > = 2.5 Definition and classification of anemia Initial classification of anemia Classifying an anemia according to the functional defect in red cell production helps organize the subsequent use of laboratory studies. The three major classes of anemia are: 1) marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1. Emorragia (=) Emolisi (>) Diminuita sopravvivenza dei globuli rossi
 marrow production defects (hypoproliferation), (2) red cell maturation defeects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. Fig A hypoproliferative anemia is typically seen with a low reticulocyte production index toghether with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocie production index that is accompanied by either macrocitic or microcitic red cell indices. Increazsed red blood cell distruction secondary to emolisis results in increase in the reticulòocite production index to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch pointt of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erithroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have rithroid hyperplasia and a M/E ratio < 1:1. Emorragia (=) Emolisi (>) Diminuita sopravvivenza dei globuli rossi.")
23
Classificazione in base alla morfologia del globulo rosso
normocitica, microcitica e macrocitica normocromica, ipercromica e ipocromica Anisocitosi poichilocitosi

24
macrocitosi microcitosi ipercromici ipocromici

25
M/E >3:1 M/E 1:1

26
Bone marrow examination
Aspirate Needle biopsy Particolarmente diagnostico per mielofibrosis, red cell maturation defect, infiltrative disease M/E ratio (ratio of WBC to nucleated RBC, n.v. M/E >3:1 iperproliferazione mieloide: neutrofili in infezione) M/E 2-3:1 hypoproliferative anemia Reticulocyte PI <2 NO erythroid hyperplasia < 1:1 Malattia emolitica Reticulocyte PI >3 YES erythroid hyperplasia Normally 20-40% developing erythroblasts in marrow contain IRON ---> sideroblasti BONE MARROW EXAMINATION A bone marrow aspirate and smear or a needle biopsy can be useful in the evaluation of some patients with anemia. Marrow examination can diagnose primary marrow disorders such as myelofibrosis, a red cell maturation defect, or an infiltrative disease. The increase or decrease of one cell lineage (myeloid vs. erythroid) compared to another is obtained by a differential count of nucleated cells in a bone marrow smear [the myeloid/erythroid (M/E) ratio]. Either the marrow smear or biopsy can be stained for the presence of iron stores or iron in developing red cells. The storage iron is in the form of ferritin or hemosiderin. Ferritin granules can normally be seen under oil immersion in 20–40% of developing erythroblasts. Such cells are called sideroblasts.
 M/E 2-3:1. hypoproliferative anemia. Reticulocyte PI <2. NO erythroid hyperplasia. < 1:1. Malattia emolitica. Reticulocyte PI >3. YES erythroid hyperplasia. Normally 20-40% developing erythroblasts in marrow contain IRON ---> sideroblasti. BONE MARROW EXAMINATION. A bone marrow aspirate and smear or a needle biopsy can be useful in the evaluation of some patients with anemia. Marrow examination can diagnose primary marrow disorders such as myelofibrosis, a red cell maturation defect, or an infiltrative disease. The increase or decrease of one cell lineage (myeloid vs. erythroid) compared to another is obtained by a differential count of nucleated cells in a bone marrow smear [the myeloid/erythroid (M/E) ratio]. Either the marrow smear or biopsy can be stained for the presence of iron stores or iron in developing red cells. The storage iron is in the form of ferritin or hemosiderin. Ferritin granules can normally be seen under oil immersion in 20–40% of developing erythroblasts. Such cells are called sideroblasts.")
27
funzionale della anemia
Classificazione funzionale della anemia CBC, reticolociti Index PR < 2.5 Index PR > = 2.5 Morfologia globulo rosso Emolisi (>) emorragia (=) Definition and classification of anemia Initial classification of anemia Classifying an anemia according to the functional defect in red cell production helps organize the subsequent use of laboratory studies. The three major classes of anemia are: 1) marrow production defects (hypoproliferation), (2) red cell maturation defects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. A hypoproliferative anemia is typically seen with a low reticulocyte production index together with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocite production index that is accompanied by either macrocitic or microcitic red cell indices. Increased red blood cell destruction secondary to hemolysis results in increase in the reticulocite production index (index PR) to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch point of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erythroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have erythroid hyperplasia and a M/E ratio < 1:1. Normocitico Normocromico (indice PR + basso) Iperplasia eritroide NO Microcitico o Macrocitico (indice PR + alto) Iperplasia eritroide SI Diminuita sopravvivenza dei globuli rossi Difetti di maturazione dei globuli rossi Difetti di produttività del midollo
 emorragia (=) Definition and classification of anemia. Initial classification of anemia. Classifying an anemia according to the functional defect in red cell production helps organize the subsequent use of laboratory studies. The three major classes of anemia are: 1) marrow production defects (hypoproliferation), (2) red cell maturation defects (ineffective erythropoiesis), and (3) decreased red cell survival (blood loss/hemolysis). This functional classification of anemia then guides the selection of specific clinical and laboratory studies designed to complete the differential diagnosis and to plan appropriate therapy. A hypoproliferative anemia is typically seen with a low reticulocyte production index together with a little or no change in red cell morphology (normocitic, normochromic anemia). Maturation disorders typically have a slight to moderately elevated reticulocite production index that is accompanied by either macrocitic or microcitic red cell indices. Increased red blood cell destruction secondary to hemolysis results in increase in the reticulocite production index (index PR) to at least three times normal, provided sufficient iron is available for hemoglobin synthesis. Hemorragic anemia does not tipically result in production indicies of more than 2.5 times normal because of the limitations placed on expansion of the erithroid marrow by iron availability. In the first branch point of the classification of anemia, a reticulocite production index > 2.5 indicates that hemolisis is most likely. A reticulocyte production index > 2 indicates either a hypoproliferative anemia or maturation disorder. The latter two possibilities can often be distinguished by the red cell indices, by examination of the periopheral blood smear or by a marrow examination. If the red cell indeces are normal, the anemia is almost certainly hypoproliferative in nature. Maturation disorders are characterized by ineffective red cell production and a low reticulocite production index. Bizarre red cell shapes - macrocytes or hypochromic microcites - are seen on the periferal smear. With a hypoproliferative anemia, no erythroid hyperplasia is noted in the marrow, whereas patients with ineffective red cell production have erythroid hyperplasia and a M/E ratio < 1:1. Normocitico. Normocromico. (indice PR + basso) Iperplasia eritroide NO. Microcitico o. Macrocitico. (indice PR + alto) Iperplasia eritroide SI. Diminuita sopravvivenza dei globuli rossi. Difetti di maturazione dei globuli rossi. Difetti di produttività del midollo.")
28
Anemie ipoproliferative

29
Hypoproliferative anemias (75% anemie)
Insufficienza midollare: il midollo eritroide non produce a sufficienza, produzione da ridotta a nulla Cause principali: Sideropenia lieve/moderata (+++) Infiammazione (+++) Danno al midollo Infiltrazione/fibrosi Aplasia Ridotta stimolazione (EPO) Soppressione da citochine infiammatorie (i.e. IL-1) malattia metabolica (ipotiroidismo) Insufficienza renale Hypoproliferative anemias At least 75% of all cases of anemia are hypoproliferative in nature. A hypoproliferative anemia reflects absolute or relative marrow failure in which the erythroid marrow has not proliferated appropriately for the degree of anemia. The majority of hypoproliferative anemias are due to mild or moderate iron deficiency or inflammation. A hypoproliferative anemia can result from marrow damage, iron deficiency, or inadeguate EPO stimulation. The last may reflect impaired renal function, suppression of EPO production by inflammatory cytokines such as IL 1 , or reduced tissue needs for oxygen from metabolic disease such as hypotiroidism. Only occasionally is the marrow unable to produce red cells at a normal rate, and this is most prevalent in patients with renal failure. In general hypoproliferative anemias are characterized by normocytic, normochromic red cells, although microcytic hypochromic cells may be observed with mild iron deficiency or long standing chronic inflammatory disease.
 Infiammazione (+++) Danno al midollo. Infiltrazione/fibrosi. Aplasia. Ridotta stimolazione (EPO) Soppressione da citochine infiammatorie (i.e. IL-1) malattia metabolica (ipotiroidismo) Insufficienza renale. Hypoproliferative anemias. At least 75% of all cases of anemia are hypoproliferative in nature. A hypoproliferative anemia reflects absolute or relative marrow failure in which the erythroid marrow has not proliferated appropriately for the degree of anemia. The majority of hypoproliferative anemias are due to mild or moderate iron deficiency or inflammation. A hypoproliferative anemia can result from marrow damage, iron deficiency, or inadeguate EPO stimulation. The last may reflect impaired renal function, suppression of EPO production by inflammatory cytokines such as IL 1 , or reduced tissue needs for oxygen from metabolic disease such as hypotiroidism. Only occasionally is the marrow unable to produce red cells at a normal rate, and this is most prevalent in patients with renal failure. In general hypoproliferative anemias are characterized by normocytic, normochromic red cells, although microcytic hypochromic cells may be observed with mild iron deficiency or long standing chronic inflammatory disease.")
30
Come si distinguono le varie forme di anemia ipoproliferativa ?
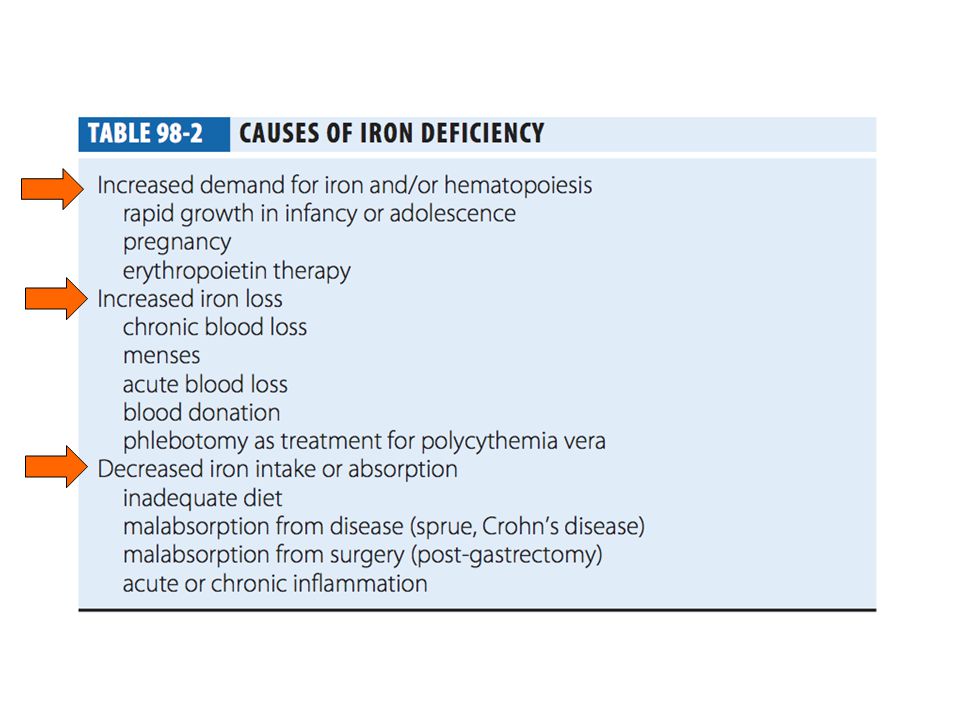
key laboratory tests serum iron TIBC evaluation of renal and thyroid function marrow biopsy o ago-aspirato (to detect marrow damage or infiltrative disease) serum ferritin (to assess iron stores) iron staining of marrow (to assess pattern of distribution) Hypoproliferative anemias The key laboratory tests in distiguishing between the various forms of hypoproliferative anemia include the serum iron and iron-binding capacity, evaluation of renal and thiroid function, a marrow biopsy or aspirate to detect marrow damage or infiltrative disease, and serum ferritin to assess iron stores. Occasionally, an iron stain of the marrow will be needed to determine the pattern of iron distribution.
 serum ferritin (to assess iron stores) iron staining of marrow (to assess pattern of distribution) Hypoproliferative anemias. The key laboratory tests in distiguishing between the various forms of hypoproliferative anemia include the serum iron and iron-binding capacity, evaluation of renal and thiroid function, a marrow biopsy or aspirate to detect marrow damage or infiltrative disease, and serum ferritin to assess iron stores. Occasionally, an iron stain of the marrow will be needed to determine the pattern of iron distribution.")
31
I diversi gradi della sideropenia
II-III fase (Hb Htc ) Moderata anemia = stadio ipoproliferativo Anemia severa = stadio iperproliferativo del midollo ------> Ineffective maturation MCHC e MCV diminuiscono. in caso di grave anemia, danno epiteliale causato da deplezione degli enzimi che utilizzano ferro Per quanto riguarda la sideropenia, essa evolve attraverso una serie continua di fasi in cui osserviamo una distribuzione differenziale delle alterazioni degli indici legati al ferro. Osserva dapprima come cambiano i livelli del ferro nei depositi rispetto alla massa dell'eritrone. Appena i primi cominciano ad accusare una riduzione significativa della quantità di ferro accumulata, vediamo una riduzione dei livelli di ferritina sierica mentre i livelli di transferrina aumentano. Nella II fase questi indici peggiorano e comincia anche a vedersi una riduzione del ferro sierico e una diminuizione della transferrina legata al Fe. Diminuiscono i sideroblasti del midollo e aumentano i livelli di protoporfirina. L'ultima fase è quella iperproliferativa (per compensazione ?) talchè noi vediamo la presenza in circolo di forme microcitiche e ipocromiche mentre tutti gli altri indici giungono ai livelli più estremi di alterazione.
 Moderata anemia = stadio ipoproliferativo. Anemia severa = stadio iperproliferativo del midollo > Ineffective maturation. MCHC e MCV diminuiscono. in caso di grave anemia, danno epiteliale causato da deplezione degli enzimi che utilizzano ferro. Per quanto riguarda la sideropenia, essa evolve attraverso una serie continua di fasi in cui osserviamo una distribuzione differenziale delle alterazioni degli indici legati al ferro. Osserva dapprima come cambiano i livelli del ferro nei depositi rispetto alla massa dell eritrone. Appena i primi cominciano ad accusare una riduzione significativa della quantità di ferro accumulata, vediamo una riduzione dei livelli di ferritina sierica mentre i livelli di transferrina aumentano. Nella II fase questi indici peggiorano e comincia anche a vedersi una riduzione del ferro sierico e una diminuizione della transferrina legata al Fe. Diminuiscono i sideroblasti del midollo e aumentano i livelli di protoporfirina. L ultima fase è quella iperproliferativa (per compensazione ) talchè noi vediamo la presenza in circolo di forme microcitiche e ipocromiche mentre tutti gli altri indici giungono ai livelli più estremi di alterazione.")
33
IRON DEFICIENCY ANEMIA
ANEMIA OF INFLAMMATORY DISEASE HCT MODERATE TO MARKED ANEMIA MILD TO MODERATE ANEMIA MCV MILD TO MODERATELY LOW NORMAL TO MILDLY LOW MCHC NORMAL TO MARKEDLY LOW NORMAL RDW MILD TO MODERATE INCREASE NORMAL TO MILDLY DECREASED RETICULOCYTE COUNT LOW TO MARKED INCREASE LOW SERUM IRON NORMAL TO LOW TIBC NORMAL TO INCREASED NORMAL TO DECREASED SERUM FERRITIN DECREASED BONE MARROW IRON DECREASED TO ABSENT

34
cronica Gli stati patologici cronici che instaurano il processo di flogosi cronica conducono tutti alla attivazione della risposta mono-macrofagica. Tutti questi stati patologici hanno una componente immunitaria, ad es. le infezioni o i tumori o le malattie autoimmuni. Il sistema immunitario e quello monomacrofagico è attivato, da qui la risposta immunitaria da una parte e quella mono-macrofagica dall'altra. Tale risposta consiste: a) attivazione di linfociti T CD3+ che a loro volta mantengono il monocita attivo. Le due cellule si attivano reciprocamente attraverso la presentazione dell' antigene. I linfociti T attivati producono IFN-gamma. I monociti attivati producono IL-1 IL-6 e TNF-alfa e IL-10. IFN-gamma insieme a TNF-alfa e IL-1 inibiscono la produzione di eritropoietina da parte del rene e quindi hanno una azione inibitoria indiretta sulla attività midollare ma anche direttamente. IFN-gamma inoltre da una parte stimola il trasportatore di metalli divalenti del macrofago del sistema RE (quello che si occupa della degradazione e fagocitosi degli eritrociti senescenti) e dall' altra inibisce la ferroportina incrementando l' accumulo di Fe nella cellula. IL-1, IL-6 e IL-10 inoltre incrementano la produzione di ferritina nel macrofago del RE. Pare che anche il recettore per la transferrina sia aumentato contribuendo all' accumulo di ferro nella cellula. Nella infiammazione un po' tutta la attività del macrofago del sistema RE risulta aumentata. La IL-6 in aggiunta agisce anche sul fegato stimolando la produzione di epcidina che bloccando la ferroportina notoriamente fa diminuire il riassorbimento del Fe a livello del duodeno e aumentare l' accumulo di Fe a livello del macrofago del sistema RE tramite la inibizione della ferroportina. la ridotta disponibilità di Fe contribuisce alla fine a inibire la eritropoiesi e quindi a instaurare la anemia.
 attivazione di linfociti T CD3+ che a loro volta mantengono il monocita attivo. Le due cellule si attivano reciprocamente attraverso la presentazione dell antigene. I linfociti T attivati producono IFN-gamma. I monociti attivati producono IL-1 IL-6 e TNF-alfa e IL-10. IFN-gamma insieme a TNF-alfa e IL-1 inibiscono la produzione di eritropoietina da parte del rene e quindi hanno una azione inibitoria indiretta sulla attività midollare ma anche direttamente. IFN-gamma inoltre da una parte stimola il trasportatore di metalli divalenti del macrofago del sistema RE (quello che si occupa della degradazione e fagocitosi degli eritrociti senescenti) e dall altra inibisce la ferroportina incrementando l accumulo di Fe nella cellula. IL-1, IL-6 e IL-10 inoltre incrementano la produzione di ferritina nel macrofago del RE. Pare che anche il recettore per la transferrina sia aumentato contribuendo all accumulo di ferro nella cellula. Nella infiammazione un po tutta la attività del macrofago del sistema RE risulta aumentata. La IL-6 in aggiunta agisce anche sul fegato stimolando la produzione di epcidina che bloccando la ferroportina notoriamente fa diminuire il riassorbimento del Fe a livello del duodeno e aumentare l accumulo di Fe a livello del macrofago del sistema RE tramite la inibizione della ferroportina. la ridotta disponibilità di Fe contribuisce alla fine a inibire la eritropoiesi e quindi a instaurare la anemia.")
Presentazioni simili


.>")







>")





>")


, Ladetto CANALE A Giorno Ora Docente ARGOMENTO Boccadoro Introduzione.>")