Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Fisiopatologia comune e terapia dei LUTS/IPB e DE Vincenzo Gentile Sapienza Università di Roma

3
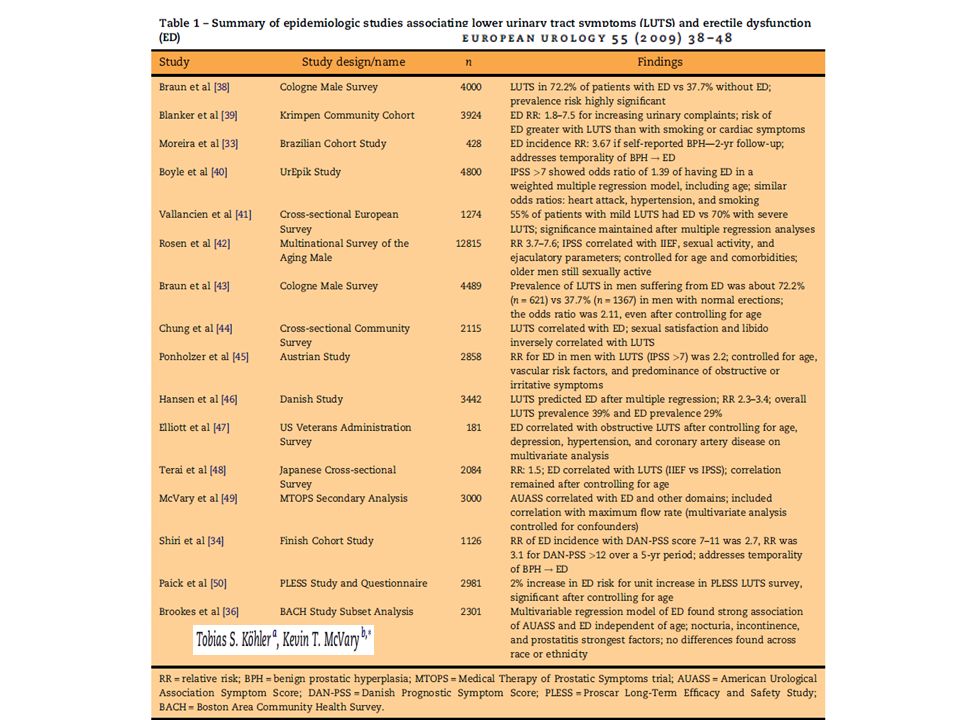
Indagine su 14.000 soggetti di sesso maschile di età compresa fra 50 e 80 anni in USA, UK, Francia, Germania, Italia, Spagna e Paesi Bassi sulle correlazioni fra Sintomi delle Basse Vie Urinarie e Disfunzioni Sessuali Board scientifico:P. Rosen, M. o'Leary, J. Altwein, F. Giuliano, R. Kirby, E Meuleman Associazione BPH-LUTS e Disfunzioni Sessuali

4
Uk 1812 Never Mild Moderate Severe Base : campione totale - + 100 75 50 25 0 Tot.C 12815 Tot.EU 10900 USA 1915 Fr 1896 Ger 2012 It 1772 Nl 2103 Sp 1305 % I-PSS>0 908990 9186928592 101110 9148158 59605665625461 252327212325261924 667467557 I-PSS>0 + + - MSAM - 7 Circa il 90% degli over 50 soffre di LUTS

5
Gravità di LUTS (IPSS) e DE (DAN-PSS-Sex): MSAM-7 Survey Rosen et al, Eur Urol 2003
 e DE (DAN-PSS-Sex): MSAM-7 Survey Rosen et al, Eur Urol 2003")
6
E’ ampiamente riconosciuta una associazione significativa tra LUTS e disfunzioni sessuali “ “Paz con LUTS moderati o gravi dovrebbero essere indagati rutinariamente sulla loro funzione erettile ed eiaculatoria, e a questo riguardo dovrebbero essere informati sui potenziali effetti in queste aree del trattamento” Leliefeld et al, BJU Int, 2002ALF-ONE St., Vallencien et al, J Urol, 2003 UrEpik St, Boyle et al, BJU Int, 2003MTOPS St., McConnell et al, N Eng J M, 2003 MSAM-7,Rosen et al, Eur Urol 2003 La gravità dei LUTS è risultata (analisi di regressione logistica) un predittore indipendente di problemi sia erettili che eiaculatori In particolare:
 un predittore indipendente di problemi sia erettili che eiaculatori In particolare:")
7
ED° (n=853) No ED° (n=3581) Diabetes20.2%3.2% Hypertension32.0%13.6% Pelvicsurgery18.8%2.4% LUTS72.2%37.7% Smoker29.6%34.6% Regularalcohol37.5%42.4% °Erectile dysfunction Braun M et al. Int J Impot Res 2000; 12: 305-311 Cologne Survey LUTS & Sexual Dysfunction

8
Patologie croniche più frequenti nella terza età *Zakaria et al, Int Urol Nephrol, 2001 - Disfunzione Erettile (DE) - Depressione - Patologie Cardiovascolari - LUTS/BPH * Sono le 4 principali patologie croniche che impattano negativamente sulla salute degli uomini sopra i 50 anni, secondo il Columbia Male Aging Project * 179.300 nuovi casi all’anno (USA) 179.300 nuovi casi all’anno (USA) 32.000 decessi all’anno (USA) 32.000 decessi all’anno (USA) Inoltre: il TUMORE PROSTATICO ha una prevalenza maggiore nelle fasce di età più avanzata, con: Stanford JL et al. JAMA 2000

9
diabete diabete ipertensioneipertensionefumofumo etàetà Disfunzioneendoteliale Malattia coronarica Malattia coronarica Disfunzione erettile Disfunzione erettile Principali fattori di rischio di Disfunzione Endoteliale

10
McVary KT. Eur Urol, 47:838-845, 2005 4 leading theories for causal association Andersson KE, et al. NeuroUrol Urodyn, 30:292-301, 2011 LUTS/BPH e DE: associazione o causalità?

11
Ipertono adrenergico Obesity-BMI Hyperinsulinemia Age Other factors? Physical inactivity INCREASED SYMPATHETIC TONE BPH BOO, BPH Erectile dysfunction? Hypertension McVary, AUA 2003

12
I SOGGETTI DIABETICI HANNO UN RISCHIO DI DE TRIPLICATO RISPETTO ALLA POPOLAZIONE GENERALE PER LA DE MMAS (Massachussets Male Aging Study 1290 soggetti, 40-70 anni) Popolazione generaleDiabete mellito tipo I e II % Feldman et al J Urol 151: 54, 1994
 Popolazione generaleDiabete mellito tipo I e II % Feldman et al J Urol 151: 54, 1994")
13
Glycemic Variability

14
Erectile Dysfunction in Diabetes Mellitus Lasantha L Malavige J Sex Med 2009; 6:1232-1237

15
Ipertensione Fumo Ipercolesterolemia Diabete Aterosclerosi Stenosi Arteriosa Fibrosi Riduzione della funzione dei nervi e dell’endotelio Insufficienza Arteriosa e mancato rilassamento della muscolatura liscia Ipotesi della riduzione della Ossido Nitrico sintetasi (NOS)/Ossido Nitrico (NO) Riduzione NOS/NO McVary and McKenna. Curr Urol Reports 2004;5:251-257 LUTS/BPH e DE: associazione o causalità?

16
Biologic Link Between BOO and ED? Atherosclerosis-induced chronic ischemia causes bladder and penile fibrosis Tarcan et al, BJU Int, 82 (Suppl 1): 26-33, 1998
: 26-33,")
17
Analisi Biochimiche hanno dimostrato l’attività della NOS nella zona periferica e di transizione nella prostata umana 1 La produzione di NOS/NO è ridotta nella prostata con IPB rispetto alla prostata sana 2,3 Con il progredire dell’ IPB i livelli tissutali di NOS/NO potrebbero ridursi ulteriormente, il che comporta una riduzione del rilassamento del tono prostatico 2,3 Riduzione di NOS influenza la minzione LUTS 1. Burnett AL, et al. Urology 1995;45:435-439. 2. Bloch W, et al. Prostate 1997;33:1-8. 3. Klotz T, et al. Urology 1997;36:316-322. Ipotesi della riduzione della Ossido Nitrico sintetasi (NOS)/Ossido Nitrico (NO)
/Ossido Nitrico (NO).")
18
PDE11 glandular epithelium PDE5 Localizzazione delle PDE nella prostata umana prostatic smooth muscle Loughney K et al. Int J Impot Res. 2005;17(4):320-5.
:")
19
Smooth muscle cells –Vasculature –Bladder –Urethra –Prostate –Corpus cavernosum Striated muscle cells –External urethral sphincter Localization of PDE5-isoenzymes in the Lower Urinary Tract Localization of PDE5-isoenzymes Andersson et al. Neurourol Urodyn 2011;30(3):292-301. PDE5-isoenzymes in the LUT
: PDE5-isoenzymes in the LUT.")
20
PDE5 Inibitori nella IPB: Razionale Il collo vescicale e la prostata hanno innervazione nitrossidergica e contengono PDE5 PDE5 inibitori potenziano l’ effetto rilassante NO-mediato in questi tessuti PDE5 inibitori potrebbero ridurre i sintomi ostruttivi e migliorare il LUTS

21
Tadalafil Once Daily for the Treatment of LUTS/BPH

22
428 men entered: 44 centers in US, and Canada Screening/ Washout Period Placebo Run-in Period Tadalafil 5 mg QD, N = 427 Open-label Extension (OLE) Period 3 0 Week Visit -8 12 -4 4 412 6/7 a 8 5 16 8 51 11 64 12 24 9 38 10 Placebo-controlled Treatment Period Tadalafil 5 mg QD N = 83 Placebo QD N = 92 Tadalafil 2.5 mg QD N = 96 Tadalafil 10 mg QD N = 85 Tadalafil 20 mg QD N = 71 Baseline & Randomization This12-month extension trial was an extension of the dose-finding study a A total of 428 patients elected to continue for an additional 52 weeks in the open-label extension; 427 received treatment and 299 (69.9%) completed the open-label extension 1.Roehrborn et al. J Urol 2008;180(4):1228-34. 2.Donatucci et al. BJU Int 2011;107(7):1110-6. 12 Months Extension Trial:Study Design 1,2
: Donatucci et al. BJU Int 2011;107(7): Months Extension Trial:Study Design 1,2.")
23
Placebo → 5 mg 5 mg → 5 mg OLE to Endpoint Change (LOCF, n = 416) mean (SD) -2.2 (5.3) 0.2 (5.4) Visit 3 6 8 9 1011 12 Week Mean Total IPSS Placebo- controlled, double- blind period Open-label extension, all on 5 mg Long-term once daily treatment with 5 mg tadalafil was effective in maintaining reduction in LUTS/BPH 1.Donatucci et al. BJU Int 2011;107(7):1110-6. 2.Data on file, Eli Lilly and Company. This12-month extension trial was an extension of the dose-finding study 12 Months Extension Trial:Study Design 1,2
: Data on file, Eli Lilly and Company. This12-month extension trial was an extension of the dose-finding study 12 Months Extension Trial:Study Design 1,2.")
24
***p .001 IPSS and IIEF-EF: Coprimary objectives SEP Q3: Key secondary objective 12-week Endpoint LS Mean Change (ANCOVA, LOCF) IPSSIIEF-EFSEP Q3 Baseline 18.2- 18.5 15.7- 16.6 36.3- 42.7 Placebo-3.81.812.0 Tadalafil 2.5 mg-4.65.2***24.6*** Tadalafil 5 mg-6.1***6.5***31.7*** Only the dose of 5 mg Tadalafil once daily showed an improvement in both ED as well as LUTS/BPH Egerdie et al. J Sex Med 2011;9(1):271-81. LUTS/BPH and ED Comorbidity Study: Results
: LUTS/BPH and ED Comorbidity Study: Results.")
25
Placebo Lead-in Period Screening/ Washout Period Treatment Period Placebo QD, N = 172 Tadalafil 5 mg QD, N = 171 Tamsulosin 0.4 mg QD, N = 168 No Study Drug Placebo QD Baseline & Randomization Visit -8 1 2 -4 3 0 5 4 6 812 7 Week 4 1 511 men randomized Germany, Italy, France, Austria, Netherlands, Belgium, Greece, Poland, Australia, Mexico, Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: Study Design Oelke et al. Eur Urol 2012;61(5):917-25.
:")
26
Baseline Week1 # Week 4 Week 12 (EP) *p<.05 vs. placebo (ANCOVA) # Values based on modified IPSS Total IPSS LS Mean Change from Baseline (LOCF) IPSS 1 Q max 1 IIEF-EF 2 Baseline 16.8- 17.4 9.4- 10.5 14.0- 16.1 Placebo- 4.21.22.1 Tadalafil 5 mg- 6.3*2.4*6.0* Tamsulosin 0.4 mg- 5.7*2.2*1.7 12-week endpoint LS mean change (ANCOVA, LOCF) * * * * * * -4.2 -5.7 -6.3 The LS mean change in total IPSS was statistically significant compared to placebo, as well as similar for both tadalafil and tamsulosin, already at Week 1 and through Week 12 The LS mean change in IIEF-EF in sexually active men with ED was significant for tadalafil, but not for tamsulosin 1.Oelke et al. Eur Urol 2012;61(5):917-25. 2.Giuliano et al. Eur Urol Suppl 2012;11(2):e705(Abstract). Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: IPSS Change from Baseline
 # Values based on modified IPSS Total IPSS LS Mean Change from Baseline (LOCF) IPSS 1 Q max 1 IIEF-EF 2 Baseline Placebo Tadalafil 5 mg- 6.3*2.4*6.0* Tamsulosin 0.4 mg- 5.7*2.2* week endpoint LS mean change (ANCOVA, LOCF) * * * * * * The LS mean change in total IPSS was statistically significant compared to placebo, as well as similar for both tadalafil and tamsulosin, already at Week 1 and through Week 12 The LS mean change in IIEF-EF in sexually active men with ED was significant for tadalafil, but not for tamsulosin 1.Oelke et al. Eur Urol 2012;61(5): Giuliano et al. Eur Urol Suppl 2012;11(2):e705(Abstract). Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: IPSS Change from Baseline.")
27
p =.009 p =.014 mL/s Oelke et al. Eur Urol 2012;61(5):917-25. Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: Q max Change from Baseline

28
Tadalafil 5 mg once daily and tamsulosin 0.4 mg once daily resulted in significant improvement in IPSS Significant increases in peak urinary flow (Q max ) compared with placebo were observed in both the tadalafil and tamsulosin groups Only tadalafil improved LUTS/BPH-related quality of life, treatment satisfaction, and erectile dysfunction The adverse event profile was similar to that in previous reports of once daily tadalafil use in men with BPH or men with ED Oelke et al. Eur Urol 2012;61(5):917-25. Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: Conclusions
: Tadalafil vs. Placebo and Tamsulosin vs. Placebo An Active Control Trial: Conclusions.")
29
Conclusioni: once daily tadalafil was more efficacious in treating both ED and LUTS than on-demand dosing. The side effects were insignificant for both dosing schedules. Conclusioni: the association of tamsulosin/tadalafil reduces detrusor pressure at maximum flow without changing the maximum flow rate during micturition and significantly improves lower urinary tract symptoms compared with the isolated use of tamsulosin. 2012

30
Conclusioni: tadalafil enhances cGMP accumulation and potentiates prostate relaxation, tadalafil combined with tamsulosin results in enhanced inhibition of neurogenic contractions of human peripheral prostate (HPP) and human bladder neck (HBN) Conclusioni: tadalafil once daily represents an effective and well tolerated medical treatment for Asian men presenting with LUTS suggestive of BPH. 2012
31
I PDE5i potrebbero agire rilassando la muscolatura liscia della vescica ?

32
PDE5i NO

33
NO cGMP 1)Hedlund P et al. Nitric oxide/cGMP-mediated effects in the outflow region of the lower urinary tract - is there a basis for pharmacological targeting of cGMP? (2005) World J Urol 23: 362–367 2) Oger S et al. Signalling pathways involved in sildenafil-induced relaxation of human bladder dome smooth muscle. Br J Pharmacol. 2010 Jul;160(5):1135-43. ←cGMP←NO (2) (1)
 World J Urol 23: 362–367 2) Oger S et al. Signalling pathways involved in sildenafil-induced relaxation of human bladder dome smooth muscle. Br J Pharmacol Jul;160(5): ←cGMP←NO (2) (1).")
34
Spontaneous contractions Afferent firing Storage LUTS CBS CSE L-Cysteine H2SH2S LUTS improvement PDE5i

35
LUTS ED L-Cys ↓ H 2 S NO ↓ cGMP

Presentazioni simili