Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Il monitoraggio della NIV
M Vitacca Divisione di Pneumologia Fondazione S.Maugeri Lumezzane (BS) Italy
 Italy.")
2
LA NIV può fallire ! Carlucci A. AJRCCM 2001;163:874

3
Perchè fallisce la NIV ? Perchè si sbaglia paziente
Perchè non si rispettono le controindicazioni Perchè si sbaglio maschera Perchè si sbaglio modalità di ventilazione Perchè si sbaglio il settaggio Perchè il paziente non supporta più la NIV Perchè non miglioranono i gas Perchè vi è cattiva interazione con il ventilatore Perchè dà un senso di falsa sicurezza

4
Il paziente giusto

5
FATTORI PREDITTIVI PER IL FALLIMENTO DELLA NIV
IN SOGGETTI CON INSUFFICIENZA RESPIRATORIA. A) Ipossiemici Ipercapnici Età Basso punteggio del livello di dipendenza misurato con scala ADL (activity daily life) Iperglicemia Presenza di polmonite come causa di insufficienza respiratoria acuta (IRA) Alto punteggio di gravità prognostica (alto APACHE II score all’ ammissione) Paziente incosciente, non collaborante Severa ipercapnia (paCO2 > 90 mmHg) Severa acidosi (pH a < 7.10) Mancanza di miglioramento (entro 1-2 h) degli scambi gassosi, frequenza cardiaca e respiratoria Paziente ipersecretivo Presenza di encefalopatia Intolleranza alla VMN Perdite di flusso dalla maschera Caduta della pressione arteriosa
 Ipossiemici Ipercapnici. Età. Basso punteggio del livello di dipendenza misurato con scala ADL (activity daily life) Iperglicemia. Presenza di polmonite come causa di insufficienza respiratoria acuta (IRA) Alto punteggio di gravità prognostica (alto APACHE II score all’ ammissione) Paziente incosciente, non collaborante. Severa ipercapnia (paCO2 > 90 mmHg) Severa acidosi (pH a < 7.10) Mancanza di miglioramento (entro 1-2 h) degli scambi gassosi, frequenza cardiaca e respiratoria. Paziente ipersecretivo. Presenza di encefalopatia. Intolleranza alla VMN. Perdite di flusso dalla maschera. Caduta della pressione arteriosa.")
6
FATTORI PREDITTIVI PER IL FALLIMENTO DELLA NIV
IN SOGGETTI CON INSUFFICIENZA RESPIRATORIA. B) Ipossiemici Normocapnici Età Alto punteggio di gravità prognostica (alto SAPS II score all’ ammissione) ARDS e polmonite come causa del ricovero Edema polmonare cardiogeno senza risposta alla terapia medica Mancato miglioramento della ossigenazione dopo VMN (1-2 h) Paziente ipersecretivo Presenza di encefalopatia Intolleranza alla VMN
 Ipossiemici Normocapnici. Età. Alto punteggio di gravità prognostica. (alto SAPS II score all’ ammissione) ARDS e polmonite come causa del ricovero. Edema polmonare cardiogeno senza risposta alla terapia medica. Mancato miglioramento della ossigenazione dopo VMN (1-2 h) Paziente ipersecretivo. Presenza di encefalopatia. Intolleranza alla VMN.")
7
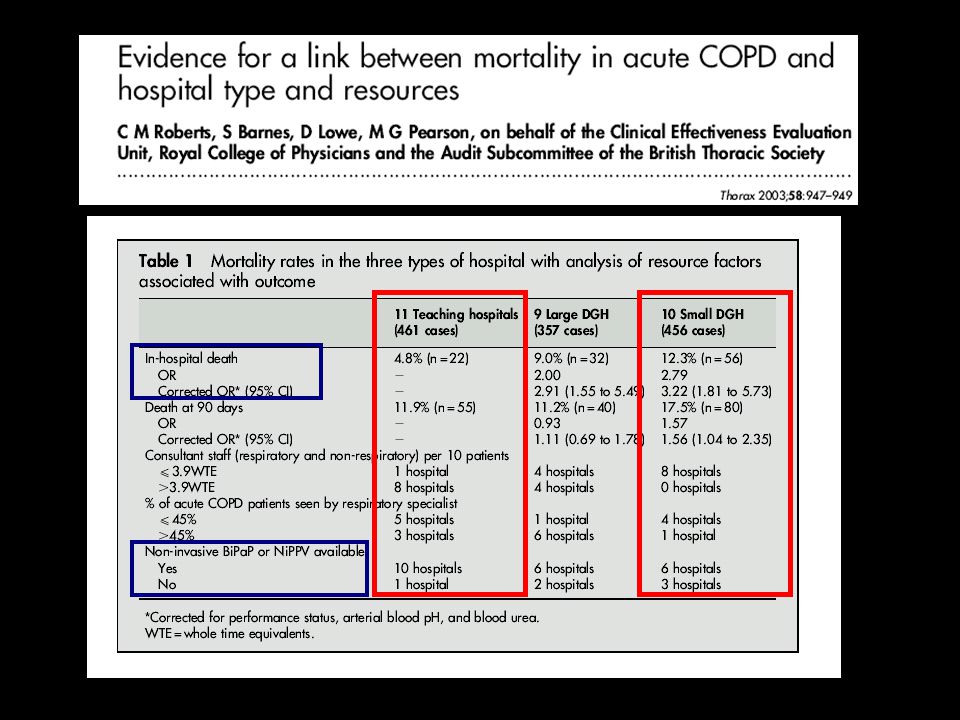
Variables associated with in hospital NIV failure (n=22/120)
Cero esistono condizioni particolari o complicanze che possono incidere sulla probabilità di successo o insuccesso della NIV. Queste sono in particolare condizioni legate al paziente

8
High percentage of failures Late resolution
Be carefull ! NON INVASIVE RESPIRATORY SUPPORT IN HYPOXIEMIC ACUTE RESPIRATORY FAILURE ? High percentage of failures Late resolution Difficult “invasive” diagnostic procedures (BAL, Brush) Risk to delay ETI Take care of: Accurate selection of the patients: - PaO2/FiO2 > 150 mmHg, - Lobar densities at chest X- Ray or CT - Absence of hemodynamic shock (BE > -2.5 mEq/L) Empiric Antibiotic Treatment (Protocols !) Non invasive fast diagnostic tests (Urinary antigens, etc.) Hemocoltures Don’t push to hard (stop NIV if PaO2/FiO2< 150 at 1-2 hrs)
 Risk to delay ETI. Take care of: Accurate selection of the patients: - PaO2/FiO2 > 150 mmHg, - Lobar densities at chest X- Ray or CT. - Absence of hemodynamic shock (BE > -2.5 mEq/L) Empiric Antibiotic Treatment (Protocols !) Non invasive fast diagnostic tests (Urinary antigens, etc.) Hemocoltures. Don’t push to hard (stop NIV if PaO2/FiO2< 150 at 1-2 hrs)")
9
Predictors of failure of noninvasive ventilation in acute hypoxiemic patients
100 NIV Efficiency (%) 50 ACPE COPD ARF Antonelli ICM 2001 Pelosi Eur Emerg J 2000
 50. ACPE. COPD. ARF. Antonelli ICM Pelosi Eur Emerg J")
11
Il training adeguato

12
Reasons for low use of NIV in acute hospitals: US survey
No. of responses 20 10 Equipment not appropriate Poor previous experience Hospital staff inadequately trained Physicians lack of experience Other Maheshwari v et al Chest 2006:129:

14
H admissions pts from NIV to EI
Am J Respir Crit Care Med Vol 185, Iss. 2, pp 152–159, Jan 15, 2012 H admissions pts from NIV to EI N° pts NIV deaths

15
NIV and EI EI NIV no EI No support
Am J Respir Crit Care Med Vol 185, Iss. 2, pp 152–159, Jan 15, 2012 NIV and EI EI NIV no EI No support

16
Controlla gli effetti collaterali

17
Pressure sores

18
80-100% Air Leaks

20
Controlla se la NIV funziona

21
Monitoring Tools Physical examination
(Clinical status, respiratory rate, heart rate, dyspnoea score, secretion clearance) ABG ECG and non-invasive BP Questionnaires Compliance Side effects (skin integrity, GI, nasal symptoms) Endpoints Diurnal gas exchanges Sleep quality Compliance, tolerance End-of night gas exchanges Techniques Oximetry Expiratory capnography Transcut. capnography Ventilator software Ventilatory settings, FiO2, leak CXR, screening bloods etc. Polysomnography Endpoints Desaturation Hypoventilation Leaks Apneas Bradypnea Patient-ventilator asynchronies Sleep quality
 ABG. ECG and non-invasive BP. Questionnaires. Compliance. Side effects (skin integrity, GI, nasal symptoms) Endpoints. Diurnal gas exchanges. Sleep quality. Compliance, tolerance. End-of night gas exchanges. Techniques. Oximetry. Expiratory capnography. Transcut. capnography. Ventilator software. Ventilatory settings, FiO2, leak. CXR, screening bloods etc. Polysomnography. Endpoints. Desaturation. Hypoventilation. Leaks. Apneas. Bradypnea. Patient-ventilator asynchronies. Sleep quality.")
22
A proposito di fallimento della NIV mi è piaciuta particolarmente questa tabella tratta da un lavoro del gruppo di Elliott pubblicata su thorax nel 2001 che tiene conto sostanzialmente di 2 parametri predittori del fallimento o dell’efficacia della NIV: pH e frequenza respiratoria (RR). Dato un pH iniziale di 7.30 se a 4 h di distanza a parità di valore di pH anche la RR è invariata i il rischio di fallimento è invariato rispetto al punto iniziale, mentre aumenta o si riduce proporzionalmente in caso rispettivamente di aumento o riduzione della RR di circa 0.5 punti per ogni quattro atti respiratori. Diverso è se il pH si riduce ulteriormente dopo 4 h per cui anche a parità di RR il rischio di fallimento aumenta e ulteriormente aumenta per ogni auemtno della RR.

23
Percentage of patients who fail NIV
Eur Respir J 2005; 25: 100 – 75 % % % 24 -0 % Percentage of patients who fail NIV

24
Percentage of patients who fail NIV
Eur Respir J 2005; 25: 100 – 75 % % % 24 -0 % Percentage of patients who fail NIV

25
< 150 after 1hr NPPV

26
Controlla l’interazione con la NIV

27
Patient brain Physician brain Pmus Paw
Dyssynchrony, Asyncrony, mismatch between patient and ventilator With ERS courtesy 27

28
Apparently there is nothing wrong on what you see on the ventilator
With S. Nava courtesy

29
But if you could see the neural activity of the patient…..
With S. Nava courtesy

30
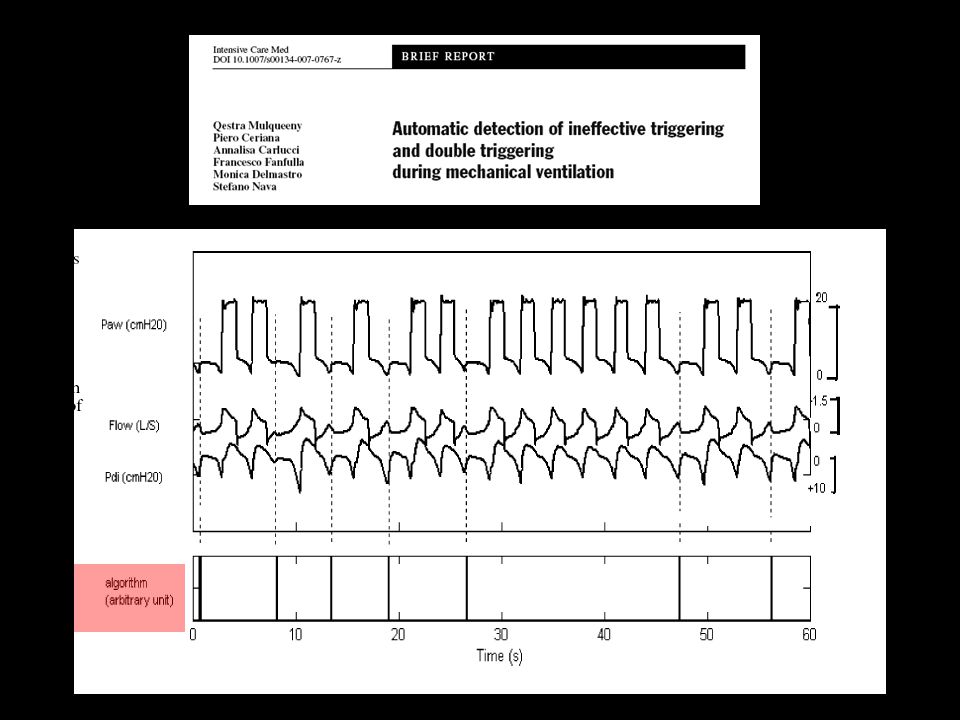
INEFFECTIVE EFFORT PHENOMENON
Flow (L/s) Airway Pressure (cmH20) Time (s) Increase in flow Decrease in pressure Patient’s inspiratory time With S. Nava courtesy Ventilator inspiratory time Nava et al. Intensive Care Med. 1995;21:871-9 Why ineffective efforts ?
 Airway Pressure (cmH20) Time (s) Increase in flow. Decrease in pressure. Patient’s inspiratory time. With S. Nava courtesy. Ventilator inspiratory time. Nava et al. Intensive Care Med. 1995;21: Why ineffective efforts")
31
Sforzi inefficaci Pao Pes 25 20 Ineffective effort

32
Un eccesso di supporto Con la cortesia del dott. Polese

33
Totale desincronizzazione durante PSV
Con la cortesia del dott. Polese

34
Totale desincronizzazione durante PSV (perdite)
Con la cortesia del dott. Polese

35
Flow cycling OFF with leaks without compensation
n-PCV n-PSV Calderini et al. Intensive Care Med 1999; 25:

37
Vent. rate = 12 b/min Fr = 33 b/min Flow (l/sec) Paw (cmH2O)
Pes (cmH2O) 5 sec Time (sec) Triggering delay= Ineffective effort Georgopoulos et al. Intensive Care Med 2006
 5 sec. Time (sec) Triggering delay= Ineffective effort. Georgopoulos et al. Intensive Care Med")
38
Paw (cmH2O) Flow (l/sec) Pes (cmH2O) Time (sec) Autotriggering
1) Low threshold for triggering 2) Dirt circuit 3) leaks Flow (l/sec) Pes (cmH2O) Time (sec) With ERS courtesy 38
 Low threshold for triggering. 2) Dirt circuit. 3) leaks. Flow (l/sec) Pes (cmH2O) Time (sec) With ERS courtesy. 38.")
39
Flow Paw Pga Pes Pdi Expiratory asynchrony
Flow, airway pressure (Paw), gastric pressure (Pga), esophageal pressure (Pes) and transdiaphragmatic pressure (Pdi) in a patient ventilated with pressure support. Observe the flow and Paw distortion early in expiration caused by continuing contraction of inspiratoty muscles (see Pdi). This type of expiratory asynchrony is due to premature opening of exhalation valve. Expiratory asynchrony With ERS courtesy 39
, gastric pressure (Pga), esophageal pressure (Pes) and transdiaphragmatic pressure (Pdi) in a patient ventilated with pressure support. Observe the flow and Paw distortion early in expiration caused by continuing contraction of inspiratoty muscles (see Pdi). This type of expiratory asynchrony is due to premature opening of exhalation valve. Expiratory asynchrony. With ERS courtesy. 39.")
40
Paw 3 6 Paw 8 Periodic breathing is a sign of excessive assist
3 6 Paw 8 Meza et al. J Appl Physiol 1998;85:1928

42
Controlla il setting diurno e notturno

43
The rising time during pressure support
Prinianakis et al. Eur Respir J 2004

44
Bosma et al. Crit Care Med 2007;35:1048

45
A CORRECT SETTING IS IMPERATIVE !

46
Results 64 patients were included. 21 exacerbations were detected and medically confirmed. The risk of exacerbation was increased when RR (OR 5.6, 95% CI 1.4 to 22.4) and %Trigg (OR 4.0, 95% CI 1.1 to 14.5) were considered as ‘high value’ on ≥2 days out of five.
 and %Trigg (OR 4.0, 95% CI 1.1 to 14.5) were considered as ‘high value’ on. ≥2 days out of five.")
47
A good monitoring 1. on ventilators:
Good screen with VERY clear traces Algorythm able to depict the presence of asynchrony and warn the clinicians 2. Non-invasive monitoring of gas exchange during NIV 3. sleep architecture monitoring

48
Safety first: Respect indications Strong training and education programs Safe staffing levels Rolling programme of staff training and protocols Correct ventilator titration Continous monitoring during time Suitable alarms Stop NIV if fails Ability to intubate & transfer pts to ICU

49
Correct pt interface nurses monitoring Location MT NIV success

Presentazioni simili






>")











 Consigliere Onorario della FADOI Emilia Romagna.>")



