Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
3° CIACC – Congresso Interassociativo di Cardiologia Clinica”
Valutazione del diabetico nella fase precoce della malattia: quale iter diagnostico, quali provvedimenti

2
Caso clinico -Uomo, 56 anni, BMI 29, vita attiva.
-FRCV: ipertensione arteriosa di grado moderato, DMNID noto da 2 anni circa. -Terapia in corso: Lisinopril 20 mg/die, Metformina 500 x2/die. Non ASA né statina. -Anamnesi cardiologica muta. Asintomatico. -Screening: Periodici controlli diabetologici. Ultima Hb glicata 7,1% Glicemia capillare al domicilio circa 130 mg/dl a digiuno e mg/dl post-prandiali. Giunge a visita presso DH Diabetologico Ultimo controllo cardiologico un anno fa, con ECG normale. Mai praticato ecocardio e/o test provocativi.

3
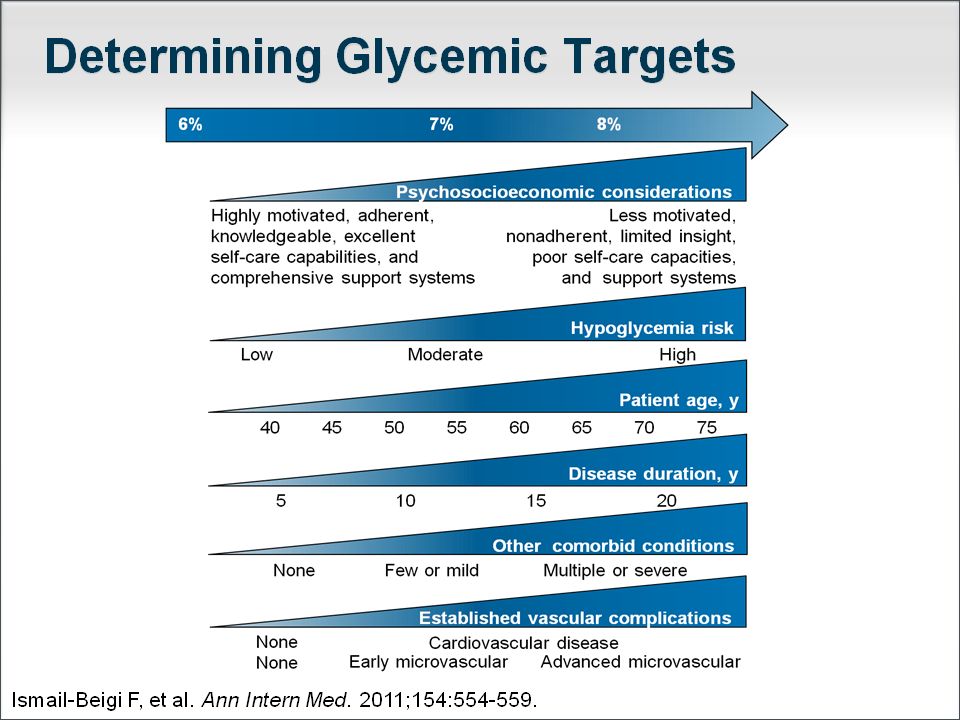
OSSERVAZIONI Durata malattia
Glicemia a digiuno e post-prandiale, HbA1C Laboratorio incompleto Valutazione clinico-strumentale Terapia

4
La clinica: glicemia a digiuno, post-prandiale, HbA1c e rischio cv
HR per primo evento cv: follow up 5 anni (0.43– 4.26) Postprandial Blood Glucose Is a Stronger Predictor of Cardiovascular Events Than Fasting Blood Glucose in Type 2 Diabetes Mellitus, Particularly in Women: Lessons from the San Luigi Gonzaga Diabetes Study F. Cavalot, A. Petrelli, M. Traversa, K. Bonomo, E. Fiora, M. Conti, G. Anfossi, G. Costa, and M. Trovati Diabetes Unit, Department of Clinical and Biological Sciences, University of Turin, San Luigi Gonzaga Hospital (F.C., M.Tra., K.B., E.F., M.C., G.A., M.Tro.), and Department of Public Health, University of Turin (A.P., G.C.), 10043 Orbassano, Turin, Italy Objective: The influence of postprandial blood glucose on diabetes complications is intensively debated. We aimed to evaluate the predictive role of both fasting and postprandial blood glucose on cardiovascular events in type 2 diabetes and the influence of gender. Methods: In a population of 529 (284 men and 245 women) consecutive type 2 diabetic patients attending our diabetes clinic, we evaluated the relationships, corrected for cardiovascular risk factors and type of treatment, between cardiovascular events in a 5-yr follow-up and baseline values of hemoglobin A1c (HbA1c) and blood glucose measured: 1) after an overnight fast, 2) after breakfast, 3) after lunch, and 4) before dinner. Continuous variables were categorized into tertiles. Results: We recorded cardiovascular events in 77 subjects: 54 of 284 men (19%) and 23 of 245 women (9.4%). Univariate analysis indicated that cardiovascular events were associated with increasing age, longer diabetes duration, and higher HbA1c and fibrinogen in men, and higher systolic blood pressure, albumin excretion rate, HbA1c, and all blood glucose values in women. Smoking was more frequent in subjects with events. When all blood glucose values and HbA1c were introduced simultaneously in the models, only blood glucose after lunch predicted cardiovascular events, with hazard ratio of the third tertile vs. the first and the second tertiles greater in women (5.54; confidence interval, 1.45–21.20) than in men (2.12; confidence interval, 1.04–4.32; P 0.01). Conclusions: Postprandial, but not fasting, blood glucose is an independent risk factor for cardiovascular events in type 2 diabetes, with a stronger predictive power in women than in men, suggesting that more attention should be paid to postprandial hyperglycemia, particularly in women. (J Clin Endocrinol Metab 91: 813–819, 2006) Cavalot F J Clin Endocrinol Metab 2006; 91: 813–819 4
 Postprandial Blood Glucose Is a Stronger Predictor of Cardiovascular Events Than Fasting Blood Glucose in Type 2 Diabetes Mellitus, Particularly in Women: Lessons from the San Luigi Gonzaga Diabetes Study. F. Cavalot, A. Petrelli, M. Traversa, K. Bonomo, E. Fiora, M. Conti, G. Anfossi, G. Costa, and M. Trovati. Diabetes Unit, Department of Clinical and Biological Sciences, University of Turin, San Luigi Gonzaga Hospital (F.C., M.Tra., K.B., E.F., M.C., G.A., M.Tro.), and Department of Public Health, University of Turin (A.P., G.C.), Orbassano, Turin, Italy. Objective: The influence of postprandial blood glucose on diabetes. complications is intensively debated. We aimed to evaluate the predictive. role of both fasting and postprandial blood glucose on cardiovascular. events in type 2 diabetes and the influence of gender. Methods: In a population of 529 (284 men and 245 women) consecutive. type 2 diabetic patients attending our diabetes clinic, we evaluated. the relationships, corrected for cardiovascular risk factors and. type of treatment, between cardiovascular events in a 5-yr follow-up. and baseline values of hemoglobin A1c (HbA1c) and blood glucose. measured: 1) after an overnight fast, 2) after breakfast, 3) after lunch, and 4) before dinner. Continuous variables were categorized into. tertiles. Results: We recorded cardiovascular events in 77 subjects: 54 of 284. men (19%) and 23 of 245 women (9.4%). Univariate analysis indicated. that cardiovascular events were associated with increasing age, longer diabetes duration, and higher HbA1c and fibrinogen in men, and higher systolic blood pressure, albumin excretion rate, HbA1c, and all blood glucose values in women. Smoking was more frequent. in subjects with events. When all blood glucose values and HbA1c. were introduced simultaneously in the models, only blood glucose. after lunch predicted cardiovascular events, with hazard ratio of the. third tertile vs. the first and the second tertiles greater in women. (5.54; confidence interval, 1.45–21.20) than in men (2.12; confidence. interval, 1.04–4.32; P 0.01). Conclusions: Postprandial, but not fasting, blood glucose is an independent. risk factor for cardiovascular events in type 2 diabetes, with a stronger predictive power in women than in men, suggesting. that more attention should be paid to postprandial hyperglycemia, particularly in women. (J Clin Endocrinol Metab 91: 813–819, 2006) Cavalot F J Clin Endocrinol Metab 2006; 91: 813–")
5
Hb A1c vs glicemia a digiuno e post prandiale
Monnier L, Lapinski H, Collette C. Diabetes Care. 2003; 26:

6
LA GLICEMIA MEDIA NON BASTA

8
Eff ects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in high-risk individuals: a randomised controlled trial The Lancet November 23, 2011 DOI: /S (11)
")
9
Eff ects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in high-risk individuals: a randomised controlled trial The Lancet November 23, 2011 DOI: /S (11)
")
10
Retinopathy Predicts Cardiovascular Mortality in Type 2 Diabetic Men and Women
Diabetes Care 30:292–299, 2007 These associations were independent of current smoking, hypertension, total cholesterol, HDL cholesterol, glycemic control of diabetes, duration of diabetes, and proteinuria.

11
ANNUAL TRANSITION RATES THROUGH THE STAGES OF NEPHROPATHY AND TO DEATH FROM ANY CAUSE
No nephropathy 1.4% 2.0% Microalbuminuria 3.0% 2.8% Macroalbuminuria 4.6% 2.3% ESRD 19.2% UKPDS 64: Kidney International 2003 11

13
ECG: RS normofrequente, segni di IVS con anomalie aspecifiche della fase di recupero in sede laterale, non presenti al tracciato precedente.

14
Il paziente non esegue Angio TAC coronarica.
CONSULENZA CARDIOLOGICA: richiesta di approfondimenti diagnostici: Ecocardiogramma e Angio TAC coronarica. ECOCARDIOGRAMMA: lieve ipertrofia parietale di tipo concentrico del Vsx con conservata funzione sistolica globale e regionale. Lieve IM da fibrosi dei lembi. Lieve dilatazione atriale sx. Valvola aortica ed aorta ascendente nei limiti. Sezioni destre nei limiti. Nulla al pericardio. Il paziente non esegue Angio TAC coronarica. ECG DA SFORZO AL CICLOERGOMETRO: test sottomassimale (75% FC max) interrotto per fatica muscolare e blanda oppressione precordiale, prontamente regredita in recupero. Lieve sottoST (circa 1 mm ascendente) in V5-V6 all’acme dello sforzo e in R1. Non arimie. Test dubbio per segni e sintomi di ischemia inducibile.
 interrotto per fatica muscolare e blanda oppressione precordiale, prontamente regredita in recupero. Lieve sottoST (circa 1 mm ascendente) in V5-V6 all’acme dello sforzo e in R1. Non arimie. Test dubbio per segni e sintomi di ischemia inducibile.")
15
OSSERVAZIONI Refertazione ecocardiografica
Angio TC coronarica/Calcium score Test provocativo dopo ECG da sforzo

16
Probabilità elevata di ischemia silente
Consensus SID-ANMCO-AMD-SIC 2010

17
MIOCARDIOSCINTIGRAFIA PERFUSIONALE A RIPOSO E DA SFORZO AL CICLOERGOMETRO:
test sottomassimale (78% FC max) interrotto per fatica muscolare e lieve dispnea. SottoST 1 mm ascendente in V5-V6 all’acme dello sforzo. Immagini di ipoperfusione reversibile a livello di parete inferiore.
 interrotto per fatica muscolare e lieve dispnea. SottoST 1 mm ascendente in V5-V6 all’acme dello sforzo. Immagini di ipoperfusione reversibile a livello di parete inferiore.")
18
Visto l’esito dubbio dei test provocativi, la dubbia sintomatologia e la presenza di 2 fattori di rischio, il paziente è stato posto in terapia con ASA e statina ed inviato a coronarografia.

19
OSSERVAZIONI Interpretazione del test di imaging Coronarografia si/no?

20
CORONAROGRAFIA:

21
CORONAROGRAFIA:

22
Quando la coronarografia?
Consensus SID-ANMCO-AMD-SIC 2010

23
Lesione subcritica del 60% della coronaria destra, non emodinamicamente significativa alla valutazione FFR Indicazione a terapia medica e follow up

24
Probabilità elevata di ischemia silente
Consensus SID-ANMCO-AMD-SIC 2010

Presentazioni simili


 ha smesso nel Impiegato. Diabete mellito tipo 2 noto dal 1993, in trattamento con ipoglicemizzanti.>")




 N. Pazienti in Dialisi (2002: 308.910)>")







 Area Prevenzione ANMCO>")

 sottoposto a CABG.>")

