Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Ulss 12 veneziana: percorsi dello Stroke
estuario terraferma centro storico

2
Stroke (ictus) cerebrale Che cos’è
Stroke (ictus) cerebrale Che cos’è? È un improvviso danno di una parte del cervello e può essere provocato da una ischemia (chiusura di una arteria da trombosi locale o da embolia) o da una emorragia (rottura di una arteria)
 cerebrale Che cos’è È un improvviso danno di una parte del cervello e può essere provocato da una ischemia (chiusura di una arteria da trombosi locale o da embolia) o da una emorragia (rottura di una arteria)")
3
Incidenza di evento cerebrovascolare nel Veneto (DGR 4453 del 28. 12
212/ abitanti nei maschi 226/ abitanti nelle femmine Media del Veneto (219/ abitanti) dati del 1999 Ricoveri annui per Stroke Venezia Centro Storico: 250 Popolazione Venezia centro storico ed estuario presunta: abitanti ma…
 dati del Ricoveri annui per Stroke. Venezia Centro Storico: 250. Popolazione Venezia centro storico ed estuario presunta: abitanti ma…")
4
(residenti, turisti, lavoratori)
Popolazione media a Venezia Centro Storico oggi (dati forniti dal Comune di Venezia) persone (residenti, turisti, lavoratori)
 persone. (residenti, turisti, lavoratori)")
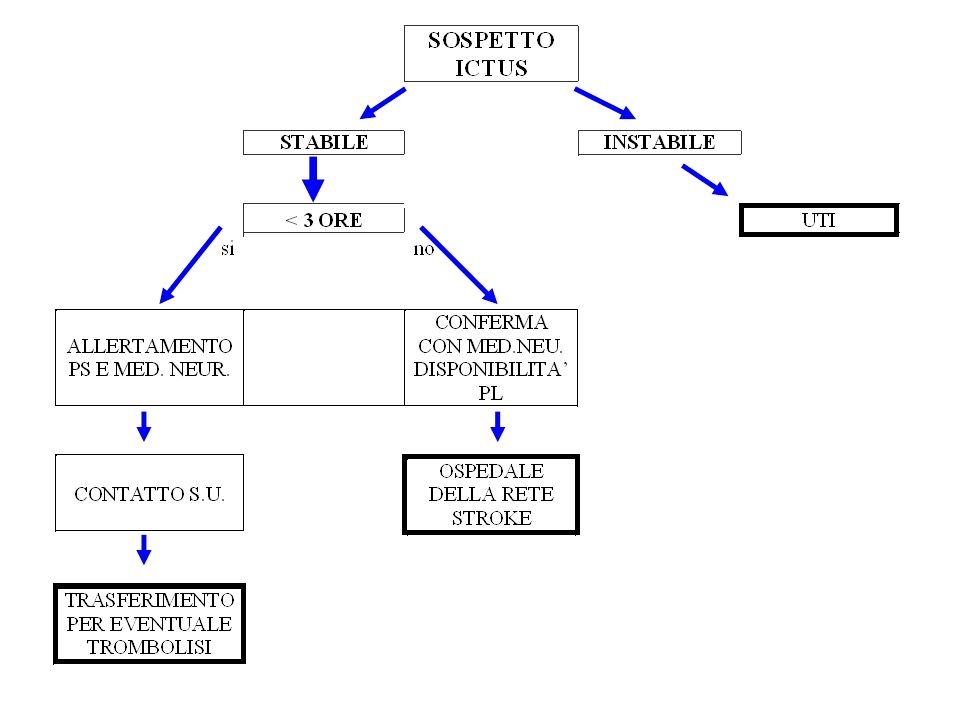
5
Gestione della richiesta di soccorso da parte dell’operatore di centrale in caso di sospetto ictus
Alterazioni della mimica facciale Deficit motori degli arti superiori e/o inferiori Alterazioni del linguaggio Tempo preciso di insorgenza dei sintomi

7
Rete anti ictus unità ictus II livello: Mestre, Padova, Rovigo, Treviso, Verona B.T., Vicenza, unità ictus I livello: Verona B.R., Legnago, Negrar e Peschiera. Bassano, Arzignano e Thiene. Monselice , Camposampiero e Cittadella. Venezia, Portogruaro e Mirano. Belluno e Feltre. Conegliano Aree dedicate: Bussolengo e San Bonifacio. Piove di Sacco,Camposanpiero e Cittadella. Adria, Dolo, Castelfranco, Montebelluna

8
Early Treatment Remains Essential
The effect size (OR 1.4) in the 3-4.5h is confirmed by ECASS III, and the confidence intervals will significantly narrow in the new pooled analysis, however, the differnce in effect size compared with early treatment (OR 2.8) remains Time Interval from onset of symptoms to treatment initiation [min] Adjusted odds ratio 1.5h OR 2.8 3h OR 1.5 4.5h OR 1.4 6h OR 1.2 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 60 120 180 240 300 360 The investigators of NINDS, ECASS and ATLANTIS have combined their data for a pooled analysis. This analysis was presented for the first time in 2002 and has now been published. This is the first analysis to look at effects of timing on outcome. The interesting findings are that the outcome in patients treated early (in the first 90 minutes) is extremely improved. There is not such a difference between the second and the third 90-minute interval. However, beyond 4.5 hours the effect may no longer be evident. Certainly statistical significance is lost although this may be simply a reflection of lack of statistical power to detect a benefit beyond 4.5 hours. The time interval to treatment was divided into 90-minute intervals (0–90, 91–180, 181–270, 271–360) and the ratio of patients with a favourable outcome (mRS 0–1, NIHSSS 0–1, BI 95–100) was analysed in 2779 patients. There was a significant correlation of outcome with time from symptom onset. The odds ratios for the favourable outcome were 2.81, 1.55, 1.4 and 1.15 respectively with the last OR missing statistical significance. The lower confidence interval intersects with 1.0 at 285 minutes after symptom onset.20 OR, odds ratio Hacke et al. Lancet 2004; 363: 768–74 8 8
 in the 3-4.5h is confirmed by ECASS III, and the confidence intervals will significantly narrow in the new pooled analysis, however, the differnce in effect size compared with early treatment (OR 2.8) remains. Time Interval from onset of symptoms to treatment initiation [min] Adjusted odds ratio. 1.5h. OR h. OR h. OR h. OR The investigators of NINDS, ECASS and ATLANTIS have combined their data for a pooled analysis. This analysis was presented for the first time in 2002 and has now been published. This is the first analysis to look at effects of timing on outcome. The interesting findings are that the outcome in patients treated early (in the first 90 minutes) is extremely improved. There is not such a difference between the second and the third 90-minute interval. However, beyond 4.5 hours the effect may no longer be evident. Certainly statistical significance is lost although this may be simply a reflection of lack of statistical power to detect a benefit beyond 4.5 hours. The time interval to treatment was divided into 90-minute intervals (0–90, 91–180, 181–270, 271–360) and the ratio of patients with a favourable outcome (mRS 0–1, NIHSSS 0–1, BI 95–100) was analysed in 2779 patients. There was a significant correlation of outcome with time from symptom onset. The odds ratios for the favourable outcome were 2.81, 1.55, 1.4 and 1.15 respectively with the last OR missing statistical significance. The lower confidence interval intersects with 1.0 at 285 minutes after symptom onset.20. OR, odds ratio. Hacke et al. Lancet 2004; 363: 768–")
9
NEURORADIOLOGIA INTERVENTISTICA

Presentazioni simili